
Abstract
Background:
Anterior cruciate ligament (ACL) tears often coincide with variable extents of cartilage lesions, which typically worsen clinical symptoms and increase osteoarthritis risk. Alterations in the metabolic profile may be informative for the response of the ACL-injured knee to cartilage lesions.
Purpose:
To determine the effect of the severity of cartilage lesions on synovial fluid metabolism of patients with ACL tears by (1) identifying characteristic metabolites and key metabolic pathways and (2) analyzing the associations between these biomarkers and patient-reported outcome measures (PROMs).
Study Design:
Cross-sectional study; Level of evidence, 4.
Methods:
Synovial fluid was extracted from 39 patients with ACL tears and various severity of cartilage lesions. According to the Outerbridge classification system, patients were divided into high- and low-grade cartilage lesion groups. The metabolic profiles of the synovial fluid were evaluated by ultraperformance liquid chromatography–mass spectrometry, and the differences between the groups were calculated. Pearson correlation analysis examined the correlation between metabolic differences and PROMs.
Results:
A total of 34 metabolites showed differences between the groups, mainly involved in 9 key pathways. Among them, oleoylethanolamide, 13-hydroxyoctadecadienoic acid, glucose, and 5-hydroxylysine are implicated in Lysholm and International Knee Documentation Committee scores.
Conclusion:
The severity of cartilage injury has a significant metabolic effect on the synovial fluid of knees with ACL tears, which correlates with PROMs and may provide new insights into the pathogenesis of osteoarthritis.
Registration:
ChiCTR220061779 (Chinese Clinical Trial Registry).
Anterior cruciate ligament (ACL) tears are common lower extremity injuries, often accompanied by meniscal tears, cartilage lesions, or bone contusions. 38 ACL reconstruction (ACLR) restores knee stability, with previous studies showing that 16% to 46% of patients have concomitant cartilage lesions at the time of surgery. 5 High-grade cartilage lesions (H-GCLs), in particular, increase the risk of osteoarthritis (OA) 25 and adversely affect knee performance and return to sport even after ACLR.4,11,23 Current treatments for cartilage lesions with ACLR, such as microfracture, osteochondral allografts, and autologous chondrocyte implantation, improve knee function but struggle to match outcomes of isolated ACL tears, especially with severe cartilage damage.9,14,18,33 Unclear molecular mechanisms linking ACL and cartilage injuries hinder the development of better treatments, and managing concomitant cartilage lesions during ACLR remains a challenge.
Previous studies suggested that levels of inflammatory cytokines, including interleukin 1β (IL-1β), IL-1ra, and tumor necrosis factor α in the synovial fluid, could reflect the extent of cartilage lesions in ACL-deficient knees 22 and predict clinical outcomes after ACLR by biological or chemical assays such as enzyme-linked immunosorbent assay.1,36 While these assays target biomarkers that are disease-specific candidates precisely, omics analysis is a discovery-oriented technique that permits the detection of truly novel biomarkers. 31 A recent proteomic profile analysis found that combined injuries or other factors, such as meniscal tears, 6 bone bruising, 6 and joint hematosis, 8 produce multiple perturbations in the intra-articular environment of the knee in patients with ACL tears, which are by no means limited to inflammatory factors.
So far, few studies have reported the metabolic changes of synovial fluid in patients with ACL injury under the influence of different degrees of cartilage lesions. On this basis, we hypothesized that the severity of cartilage damage not only affects the inflammatory response but may affect other aspects of metabolic characteristics in patients with ACL tears. To comprehensively analyze these metabolic differences, we employed principal component analysis and pathway mapping. Principal component analysis is a widely used statistical method that reduces the complexity of large data sets by identifying patterns and grouping similar metabolic profiles. This technique allows us to detect major metabolic variations between patient groups in an unbiased manner. Pathway mapping, however, contextualizes these metabolic changes by linking them to established biochemical pathways, helping to uncover the potential biological mechanisms underlying different severities of cartilage injury. These approaches, although well established in metabolomics research, are less commonly used in orthopaedic clinical studies; therefore, we provide this background to ensure clarity for a broad readership. This study aimed to investigate the effect of the cartilage lesion grade on the metabolism of patients with ACL injuries to discover new biomarkers and the relationship between these biomarkers and patient-reported outcome measures (PROMs).
Methods
Participants
This study was approved by the research institutional review board (202203) and registered in the Chinese Clinical Trial Registry (ChiCTR2200061779). A total of 39 synovial fluid samples were collected after obtaining informed consent from each patient. The samples were processed under the ethical standards established by the Office for the Protection of Human Research to ensure the highest standards of ethical conduct. Patients aged 18 to 50 years were eligible to participate in this study if they were diagnosed with acute ACL tears based on history, physical examination, and magnetic resonance imaging. A clearly defined inclusion criterion required ACLR surgery within 6 weeks (≤42 days) of injury. Synovial fluid samples were aspirated intraoperatively at the time of ACLR surgery. Because all patients underwent surgery within this standardized time frame, the potential influence of time from injury to aspiration on metabolic profiles was minimized. The participants were excluded if they exhibited multiple ligamentous laxity, concomitant ligamentous injuries, gout or other metabolic arthropathies, and a history of knee surgery.
Clinical Characteristics, Performance, and Cartilage-Related Conditions
Preoperative collection of basic patient information was performed: name, sex, age, body mass index (BMI), and duration of injury. Several scales available for evaluating the clinical functioning of the knee were applied: visual analog scale, Lysholm score, International Knee Documentation Committee (IKDC) score, and Tegner activity scale. All PROMs were collected within 2 days before the synovial fluid aspiration to ensure temporal alignment with biomarker sampling for valid correlative analyses.
Two senior surgeons independently determined cartilage conditions on each injured knee during the same procedure of ACLR. Cartilage lesions were graded I to IV per the Outerbridge system, which reflects the depth and size of macroscopic cartilage lesions in the joint. Patients with grade 0 (normal cartilage) were not included in this study, as our focus was on the metabolic effect of cartilage injury. Cartilage lesions were assessed on 6 articular surfaces: patella, femoral trochanter, lateral femoral condyle, medial femoral condyle, lateral tibial plateau, and medial tibial plateau. The grade and amount of cartilage lesions were recorded. The consistency of the results was calculated with a weighted κ of 0.933, with 3 cases of disagreement. These 3 cases were rediscussed by both doctors to achieve consistent and appropriate grading. Grade I was classified as a low-grade cartilage lesion (L-GCL), and grades II to IV with morphologic changes on the cartilage surface were classified as H-GCLs, similar to the classifications of Yoshida et al. 47 While many cartilage repair studies classify grades I and II as low-grade lesions, we categorized grade II as high grade based on its metabolic characteristics rather than structural severity. Outerbridge grade II lesions involve cartilage surface fissuring or fragmentation, which has been shown to induce metabolic changes comparable to more advanced lesions. Recent metabolomics studies suggest that even moderate cartilage damage (grade II) triggers biochemical alterations similar to grades III and IV, particularly in inflammatory and lipid metabolism pathways. Given our study’s focus on synovial fluid metabolic profiles, we opted to classify grade II as high grade to reflect its biochemical significance rather than purely its structural classification. 8 When multiple cartilage lesions were present in the same knee, grouping was performed according to the highest grade of cartilage lesions.
Collection, Storage, and Handling of Synovial Fluid
An approximately 1-mL sample of synovial fluid was aspirated (not necessarily the maximum available volume) under sterile conditions in the operating theater from each knee of patients who met the inclusion and exclusion criteria. All patients had sufficient synovial fluid available for aspiration, and there were no cases where fluid could not be collected. As a result, no patients were excluded for insufficient fluid volume, and joint lavage was not performed to obtain samples. There was no iatrogenic infection at the time of aspiration. Each sample was sent to the laboratory within 30 minutes and centrifuged at 10,000 rpm for 10 minutes at 4°C. The supernatant was aspirated in the thread cryotube and frozen in liquid nitrogen for 15 minutes. Each sample was then kept at −80°C for subsequent analysis. A series of standardized processes were employed to process the samples before liquid chromatography–mass spectrometry detection, including thawing, centrifugation, concentration drying, and filtration (a full description is in the Appendix, available in the online version of this article). In addition, quality control samples were taken by mixing 10 µL of each sample to ascertain the quality of the data.
Exclusion Criteria
Patients with Outerbridge grade 0 (normal cartilage) were not included in this study, as the primary focus was on metabolic alterations associated with cartilage lesions.
Liquid Chromatography–Mass Spectrometry Analysis
Synovial fluid samples from patients with ACL injuries in the L-GCL and H-GCL groups were subjected to liquid chromatography analysis on a Vanquish UHPLC system (Thermo Fisher Scientific) and chromatography completion on an ACQUITY UPLC HSST3 (Waters). 48 A Q Exactive HF-X (Thermo Fisher Scientific) equipped with an electrospray ionization ion source was used for mass spectrometry (MS) detection of metabolites. Detailed metabolite analyses of the samples were carried out using MS1 and MS/MS simultaneous acquisition. 41
Data Processing and Analysis
An efficient data-processing method was employed to obtain a comprehensive understanding of the metabolic characteristics of knee synovial fluid in patients with ACL tears in the L-GCL and H-GCL groups (a full description is in the Appendix, available online). Principal component analysis and orthogonal partial least squares discriminant analysis (OPLS-DA) models were built by Ropls software 37 to determine the metabolic differences between the groups. In addition, permutation tests were performed to determine if the established models were overfitting. Variables contributing to the classification were identified by calculating the P value (Student t test or Wilcoxon rank sum test), variable importance in projection (VIP) generated by OPLS-DA, and fold change. To reduce false positives in multiple comparisons, the false discovery rate (FDR) was controlled at 0.2 using the Benjamini-Hochberg procedure. P < .05, FDR <0.2, and VIP >1 were used as thresholds for selecting significant metabolites, which are widely accepted criteria in metabolomics studies.30,44 P < .05 ensures statistical significance in univariate analysis. FDR <0.2, rather than the more conservative <0.05 used in genomics, is considered appropriate in metabolomics owing to higher biological variability. VIP >1 is a standard threshold in partial least squares discriminant analysis and OPLS-DA models to identify metabolites contributing significantly to group separation. 43 Pathway analysis of differential metabolites was performed using MetaboAnalyst, 45 with the identified metabolites mapped to the KEGG pathway to elucidate higher-level systemic functions in biological processes. The FDR was controlled at 0.2 using the Benjamini-Hochberg procedure. P < .05, FDR <0.2, and VIP >1 were considered statistically significant metabolites. Pathway analysis of differential metabolites was performed using MetaboAnalyst. The identified metabolites were mapped to the KEGG pathway to elucidate higher-level systemic functions in biological areas.
Volcano plots were used to visualize differential metabolites. Significantly upregulated and downregulated metabolites were marked in red and blue, respectively, while gray dots represented detected but nonsignificant metabolites. This color-coding approach is widely used in metabolomics research for clear differentiation of significant and nonsignificant metabolites, ensuring consistency with published studies. Log2 fold change was applied to ensure a symmetric representation of upregulated and downregulated metabolites, while –log10 P values were used to enhance the visualization of significance levels, making more statistically significant metabolites appear higher in the plot. These transformations are standard in metabolomics studies for improved interpretability.
Clinical data were statistically analyzed with SPSS 23.0 software (IBM). Quantitative data were given as mean and standard deviation, while qualitative data were given as the number of cases. After data normality was tested by the Shapiro-Wilk test, differences between groups were compared through the independent samples t test or Wilcoxon rank sum test. Correlation tests were carried out using Pearson correlation analysis. Based on the observed effect size (Cohen d = 0.8) in key metabolic comparisons and an α level of 0.05, our study achieved a statistical power of 81%, indicating a low probability (<20%) of type II errors (false negatives). Power analysis was conducted using G*Power 3.1 software.
Results
Characteristics of Patients
Thirty-nine patients with ACL tears were included in this study and divided into the L-GCL and H-GCL groups. Among these, 15 patients (7 male, 8 female) were in the L-GCL group with a respective mean age and BMI of 34.28 ± 4.36 and 23.95 ± 3.73. The H-GCL group had 24 patients (13 male, 11 female) with a mean age and BMI of 32.73 ± 8.38 and 25.65 ± 3.64. There was no statistical difference between the groups in terms of age, sex, height, weight, BMI, or time to injury (Table 1).
Distribution of Baseline Characteristics Between the L-GCL and H-GCL Groups a
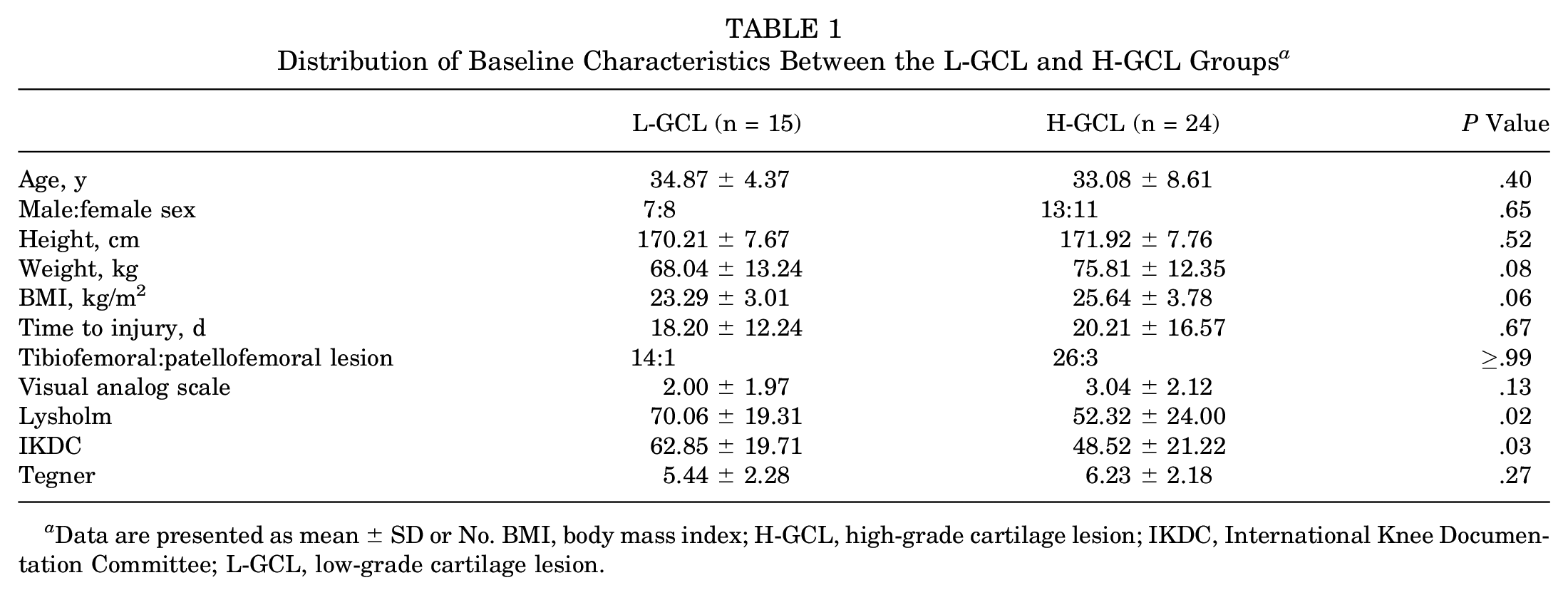
Data are presented as mean ± SD or No. BMI, body mass index; H-GCL, high-grade cartilage lesion; IKDC, International Knee Documentation Committee; L-GCL, low-grade cartilage lesion.
Metabolomic Differences Between the Groups
In the comparison of metabolite levels, 34 metabolites were significantly different between the L-GCL and H-GCL groups by P < .05 (t test), VIP >1.0 (OPLS-DA model), and FDR <0.2 (Appendix Table A1, available online). Among them, 15 were upregulated and 19 were downregulated at any fold change in the H-GCL group, as shown in the volcano plot (Figure 1). Volcano plots were generated to illustrate the distribution of differential metabolites between groups. Metabolites that were significantly upregulated and downregulated were shown in red and blue, respectively, while gray dots represented detected metabolites that did not meet the significance criteria (P ≥ .05, FDR ≥0.2, or VIP ≤1). These nonsignificant metabolites were included in the visualization to provide a complete metabolic landscape, but they were not considered for pathway analysis.
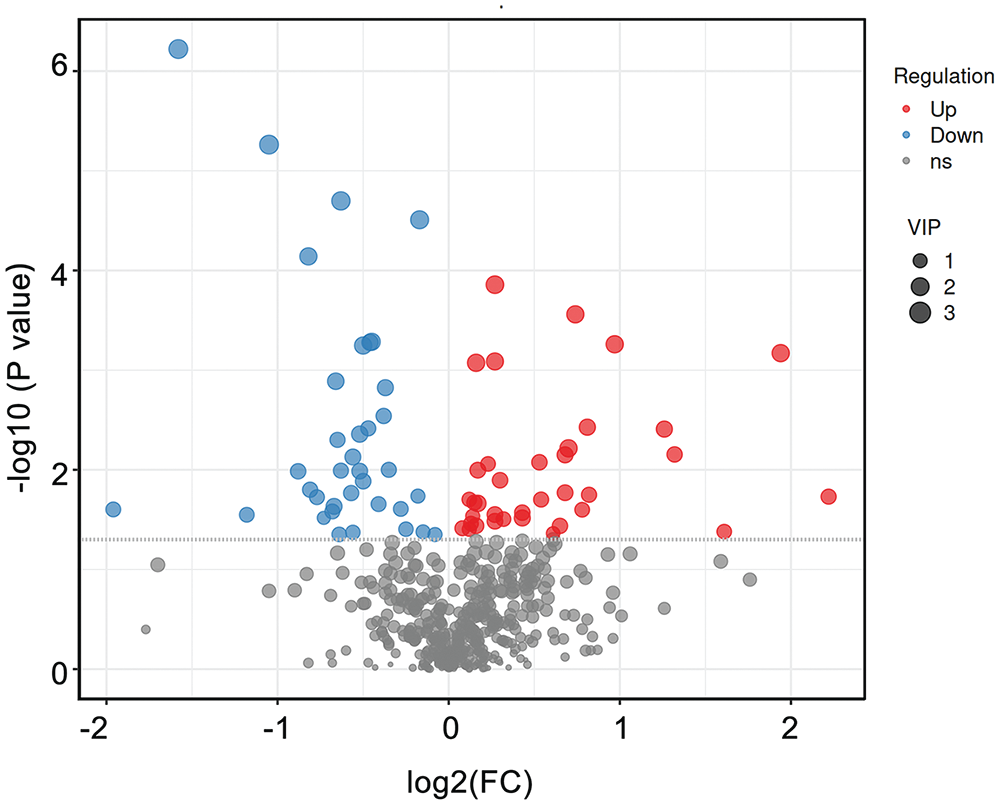
Volcano plot. The x-axis represents the log2 of the fold change between the H-GCL and L-GCL groups for metabolites; the y-axis represents the log10 of the P value. Red dots, upregulated metabolites; blue dots, downregulated metabolites; and gray dots, metabolites detected but not screened for filtering parameters in the H-GCL group. FC, fold change; H-GCL, high-grade cartilage lesion; L-GCL, low-grade cartilage lesion; VIP, variable importance in projection.
Enrichment Analysis
The results of pathway enrichment based on the MetPA database showed that 9 pathways were the most relevant with a P < .05: phenylalanine metabolism, lysine degradation, nonalcoholic fatty liver disease, cAMP signaling pathway, linoleic acid metabolism, insulin signaling pathway, taste transduction, peroxisomal proliferator-activated receptor (PPAR) signaling pathway, and FoxO signaling pathway (Figure 2). These pathways involved amino acid, glucose, and lipid metabolism, with 12 metabolites playing key roles in synovial fluid metabolic changes, especially in different degrees of cartilage lesions (Table 2).
Differential Metabolites in Key Pathways a
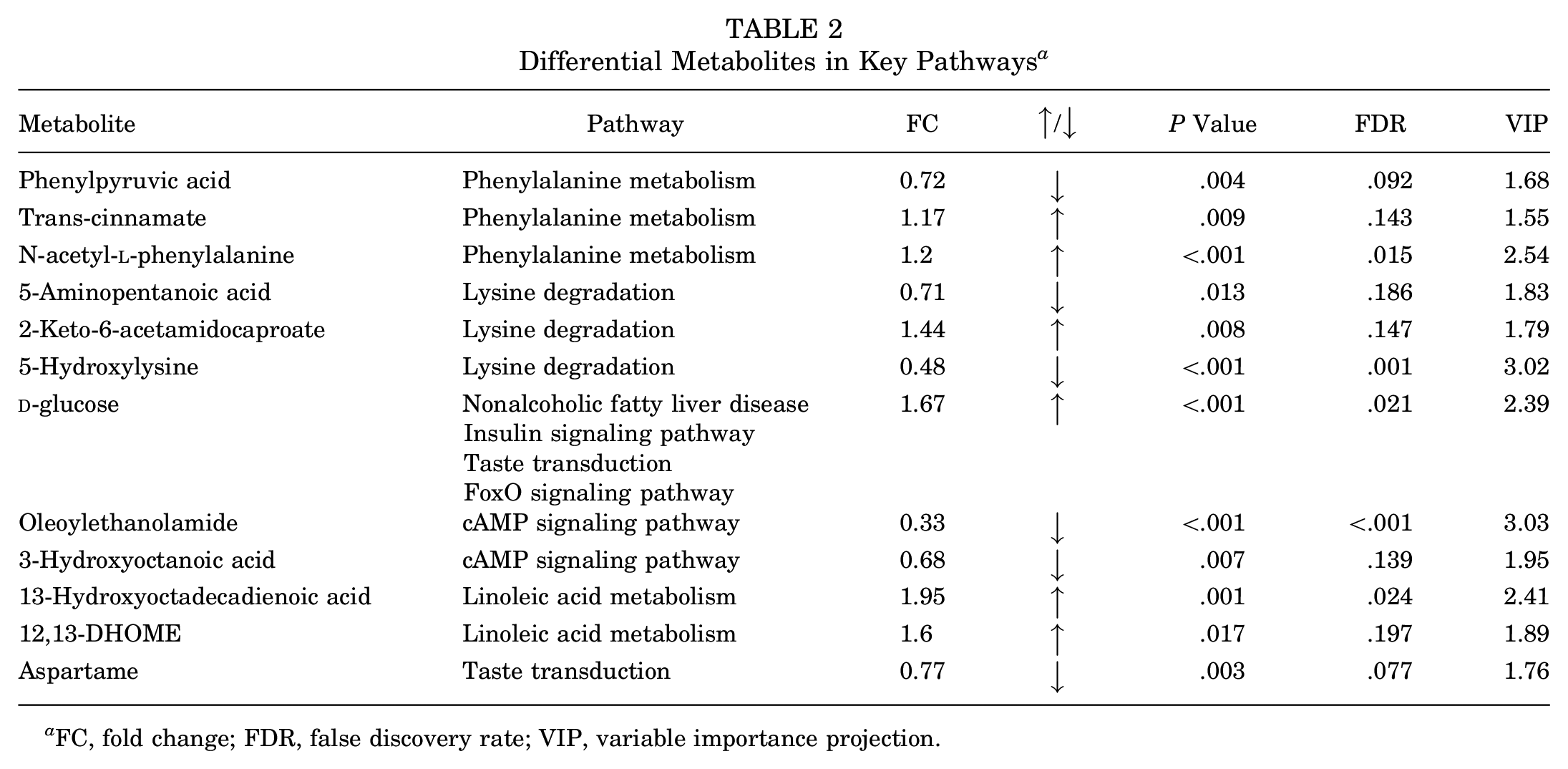
FC, fold change; FDR, false discovery rate; VIP, variable importance projection.
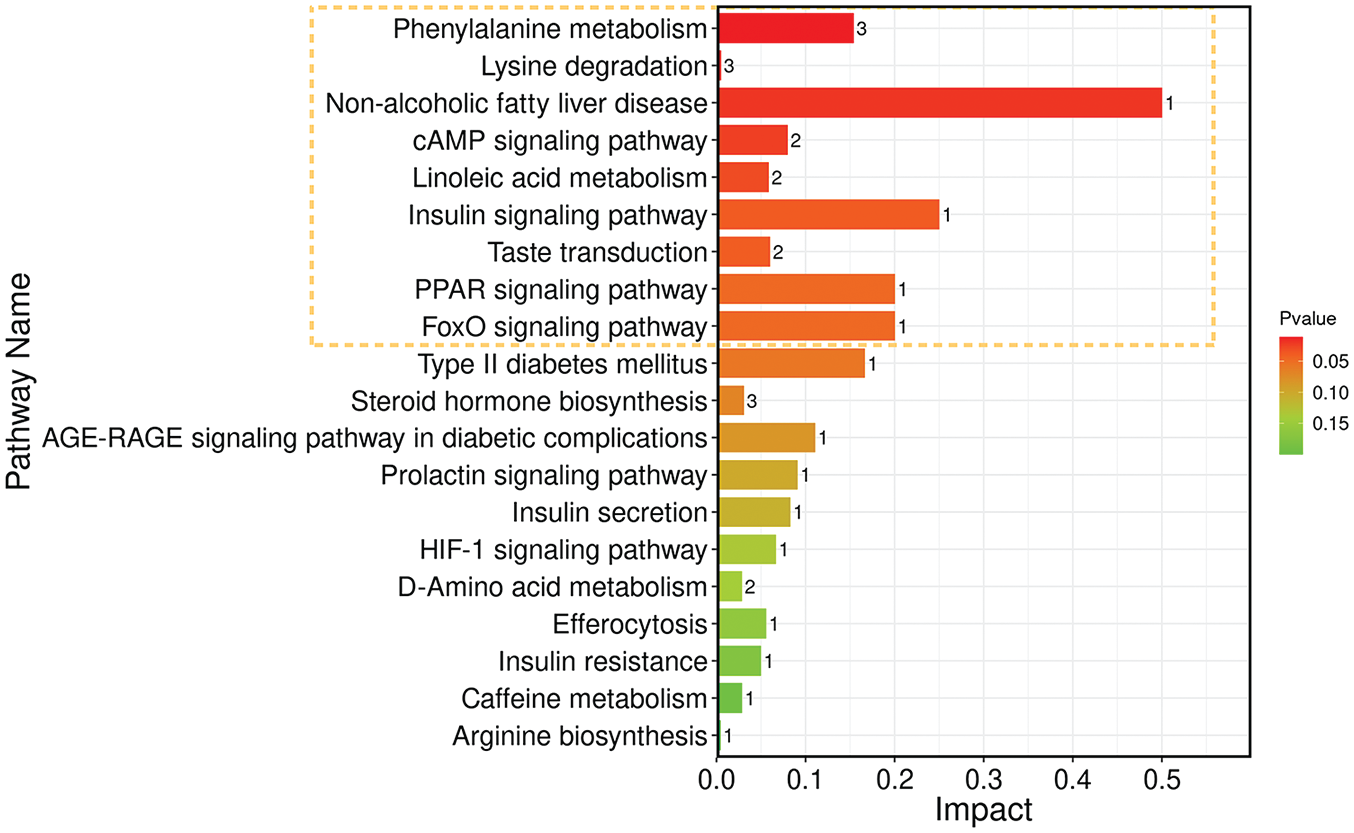
Histogram of metabolic pathway impact factors. The y-axis represents metabolic pathways. The x-axis represents the impact value enriched into different metabolic pathways, reflecting the metabolite contribution detected under the pathway. The color reflects the P value. PPAR, peroxisomal proliferator-activated receptor.
Correlations Between Metabolomic Changes and Knee Performance
In total, 7 metabolites among the top 10 up- and downregulated metabolites were associated with PROMs: oleoylethanolamide (OEA), 5-hydroxylysine (5-Hyl), 5α-dihydroprogesterone (5α-DHP), glucose, 13-hydroxyoctadecadienoic acid (13-HODE), 11b-hydroxyandrost-4-ene-3,17-dione, and selenomethylselenocysteine. The correlation between metabolites and PROMs was reflected on the heat map (Figure 3).
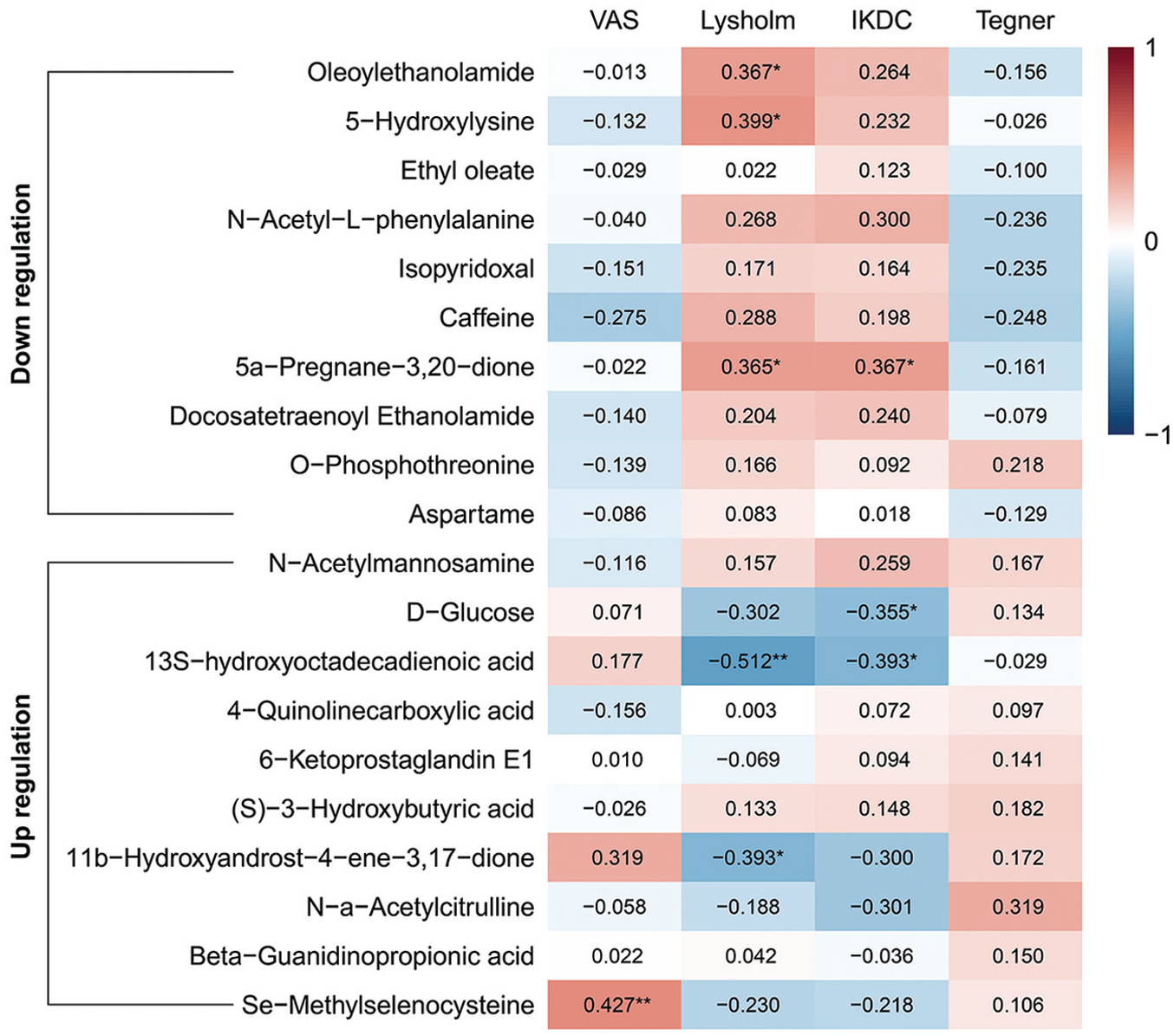
Pearson correlation heat maps of the top 10 up- and downregulated metabolites and patient-reported outcome measures. *P < .05. **P < .01. IKDC, International Knee Documentation Committee; VAS, visual analog scale.
The visual analog scale was positively correlated with selenomethylselenocysteine (R = 0.427; P < .001), which might be related to pain perception. Lysholm was positively correlated with OEA, 5-Hyl, and 5α-DHP (R = 0.367 [P = .025]; R = 0.399 [P = .015]; R = 0.365 [P = .026]). Lysholm had a negative correlation with 13-HODE and 11b-hydroxyandrost-4-ene-3,17-dione (R = −0.512 [P = .001]; R = −0.393 [P = .016]). IKDC scores were positively correlated with 5α-DHP (R = 0.367; P = .025) and negatively correlated with 13-HODE and glucose (R = −0.393 [P = .016]; R = −0.355 [P = .031]). These findings may be involved in the functional status of the knee and the inflammatory response.
Selection of Biomarkers
The Venn diagram showed that 4 metabolites were selected as biomarkers as they were included in the 12 metabolites involved in key pathways and the 7 metabolites associated with PROMs (Figure 4A): OEA, 5-Hyl, 13-HODE, glucose, and 5-Hyl (Table 3). Box plots visualized the relative concentrations of these metabolites between the H-GCL and L-GCL groups (Figure 4, B-E).
Characteristics of Biomarkers a
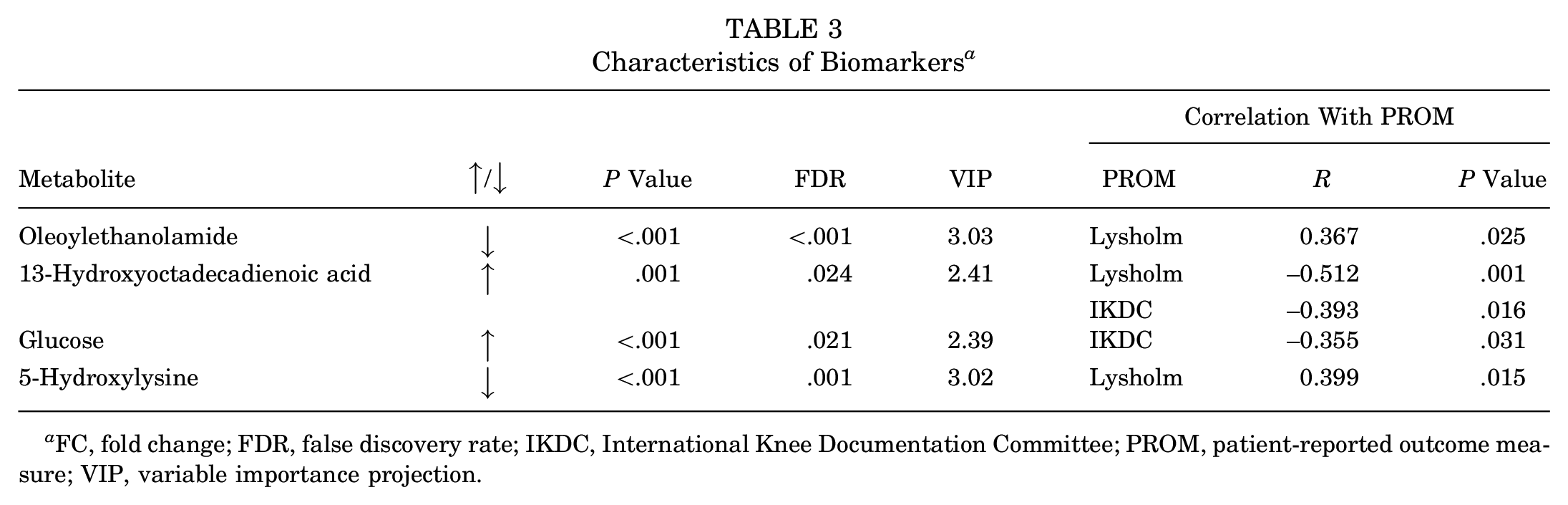
FC, fold change; FDR, false discovery rate; IKDC, International Knee Documentation Committee; PROM, patient-reported outcome measure; VIP, variable importance projection.
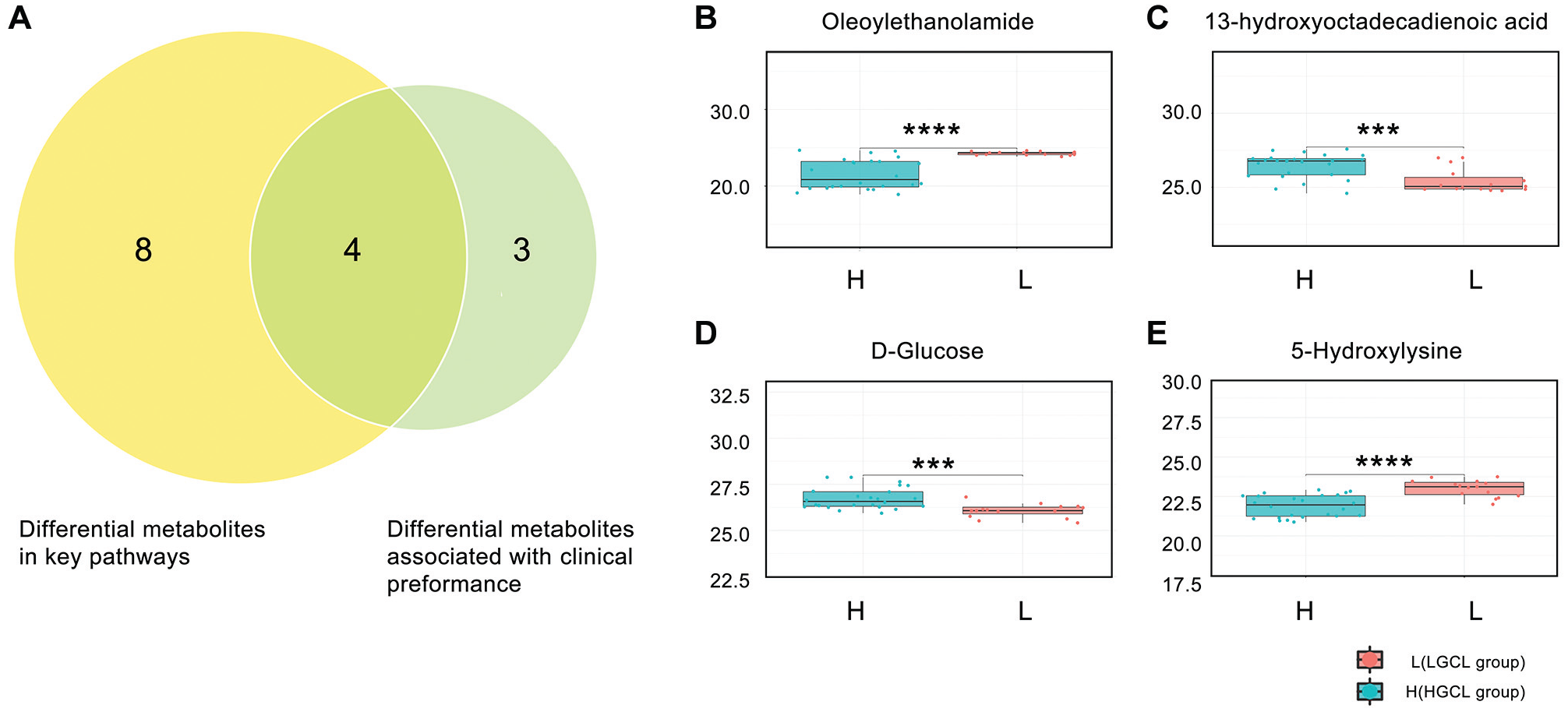
(A) Venn diagram. The overlapping areas represent metabolites involved in key pathways and associated with patient-reported outcome measures. (B-E) The box plots of the biomarkers show the relative concentrations (y-axis) of OEA, 13-HODE, glucose, and 5-Hyl in the L-GCL and H-GCL groups. Data are presented as the mean, minimum, maximum, and range of log2-transformed metabolite signal intensities. ***P < .001. ****P < .0001. H-GCL, high-grade cartilage lesion; L-GCL, low-grade cartilage lesion.
Discussion
The metabolic composition of synovial fluid in ACL-injured knees is correlated with different grades of cartilage lesions. In this study, the standardized inclusion criterion (≤6 weeks from injury to ACLR) ensured that variations in time to aspiration had minimal effect on metabolomic differences. This correlation affects joint health and function, explaining the crosstalk between knee tissues and progression to OA. The inflammatory response plays a critical role in this metabolic shift. Previous studies have demonstrated that acute ACL injury induces an inflammatory surge in synovial fluid, which evolves over time until surgical reconstruction.15,16 This prolonged inflammatory activity may contribute to cartilage matrix degradation and subsequent metabolic alterations as observed in our study. Moreover, early anti-inflammatory treatment after ACL injury has been investigated as a potential strategy to modulate joint homeostasis and improve clinical outcomes. 19 Given that our study identified OEA as a metabolite with anti-inflammatory properties, its downregulation in the H-GCL group may indicate an impaired resolution of inflammation, potentially worsening joint function. Future studies should explore whether targeting metabolic and inflammatory pathways concurrently could enhance ACL rehabilitation strategies. Although conflicting evidence exists regarding how concomitant cartilage lesions affect the clinical outcomes of ACL tears, considerable clinical research showed that high-grade cartilage damage leads to poorer knee function and a higher risk of OA.4,11,23 For instance, high-grade articular cartilage damage in the medial, lateral, or patellofemoral compartment was a specific risk factor for poorer clinical outcomes at 10-year follow-up after ACLR. 34 In another long-term follow-up after ACLR, concomitant cartilage lesions, regardless of grade, increased the risk of OA after 12 years. 40 The findings of Everhart et al 11 indicated that H-GCLs impeded achieving a 90% limb symmetry index in isometric extensor strength at 6 months postoperatively, thus making it difficult to return to sports. The lower Lysholm and IKDC scores in the H-GCL group in this study were similar to previous findings. Moreover, OA was recently considered a whole-joint disease, and the molecular crosstalk articular tissues are the main pathogenesis of OA. 12 Thus, individualized interventions based on different concomitant injuries, such as cartilage injuries, are promising to improve the prognosis and decrease the risk of OA in patients with ACL tears. However, their pathogenic relationship remains unclear. There is limited evidence on how the metabolism features of synovial fluid change among individuals with ACL injuries and cartilage lesions of different severity and how such changes affect PROM outcomes.
In our study, 34 metabolites with differential levels in the H-GCL and L-GCL groups provided new information. Among them, OEA, 13-HODE, glucose, and 5-Hyl are involved in key pathways. Differences in their relative concentration between the groups correlated with poorer Lysholm and IKDC scores. The levels of OEA were reduced by a factor of 2.99 (1/0.33) in the H-GCL group. OEA is a member of the fatty acid ethanolamides, a lipid-derived messenger family that participates in multiple physiologic functions, including regulating pain and inflammation. 28 OEA has been proven to play an antinociceptive and anti-inflammatory role in experimental animal models and humans, primarily but not exclusively via activation of PPAR-α.35,46 In a randomized controlled clinical trial, OEA activated PPAR-α, thereby inhibiting the transcription factor nuclear factor–κB pathway as well as the expression of the proinflammatory factor IL-6 and promoting the expression of the inflammation-protective factor IL-10. 39 Therefore, the significantly reduced OEA in the H-GCL group in this study was associated with worse knee function (lower Lysholm score), possibly attributed to the diminished inhibitory effect of OEA on inflammatory response. In an animal model, OEA attenuated visceral and inflammatory pain through mechanisms unrelated to PPAR-α activation. 35 In addition, OEA modulates lipid metabolism, thereby modulating BMI and obesity, the major risk factors for OA. 3 Given the important physiologic role of OEA, further mechanistic studies of this lipid mediator as a potential therapeutic molecular target for improving the PROMs of the knee joint are warranted.
The level of 13-HODE in synovial fluid was 1.95 times higher in the H-GCL group in this study. 13-HODE, a secondary oxidation product of linoleic acid, 10 has been extensively studied and implicated in a range of inflammatory and degenerative diseases.24,32 High levels of HODEs may affect clinical outcomes by promoting inflammatory responses and sensitization to pain. 42 Our study also found an association between high levels of 13-HODE and poorer clinical outcomes of knee function (lower Lysholm and IKDC scores), which seems to support this conclusion. However, there is conflicting evidence that 13-HODE might have certain anti-inflammatory and cartilage-protective properties.7,24 As a ligand for PPAR-γ, 13-HODE inhibits IL-1β–induced matrix metalloproteinase 1 and 13 expression and type II collagen cleavage in the PPAR-γ pathway, thereby reducing the destruction of cartilage matrix components during OA. Longitudinal studies and quantitative analyses may further validate whether there is a threshold-related dual modulatory effect of 13-HODE on the inflammatory response and cartilage. Although we have not been able to determine the mechanism behind the higher levels of 13-HODE in the H-GCL group, it may have an important effect. Further work is needed to better understand whether and how this kind of lipid metabolite affects the response of the knee joint to injury and whether it may be a therapeutic target.
We found that glucose levels in synovial fluid were 1.67 times higher in the H-GCL group than the L-GCL group. Similar metabolic changes have been observed in recent metabolomic studies of ACL and hemarthrosis. 8 Rosa et al 29 suggested that elevated glucose levels correlate with increased energy demands after joint trauma. There is also evidence that increased glucose levels reflect the upregulation of glucose transporter proteins 1 and 9 by stimulation of inflammation cytokines. 2 This leads to the hypothesis (not supported by the data) that increased glucose levels may be associated with increased energy requirements attributed to the inflammatory response after joint trauma. While the mechanism remains undetermined, the elevated glucose level in the synovial fluid was related to a lower IKDC score, implying that glucose acts negatively in the knee’s response to high-level cartilage damage. Moreover, changes in glucose levels in synovial fluid are an indication of perturbations in energy metabolism that are associated with OA. In the chondrocyte intracellular and extracellular models, higher glucose levels cause changes in transport, induce inflammation and chondrocyte degradation, and thus progress to OA.20,21,27,29 The higher glucose levels in the synovial fluid of patients with more severe cartilage damage in our study may further exacerbate cartilage damage, which may help explain the clinical phenomenon that such combined injuries are more likely to progress to OA.
In the H-GCL group, 5-Hyl levels were downregulated 2.08-fold (1/0.48) in the present study. Hydroxylysine (Hyl) is one of the major components of the α chain of collagen, which forms the hyaline chondrocyte extracellular matrix. The hydroxylation of lysine to Hyl is the process by which collagen forms a more stable structure and is known as posttranslational modification. 13 Although metabolic changes in 5-Hyl have not been reported in related diseases, a multi-omics study 2 found that inflammatory stimulation alters cartilage lysine levels. Meanwhile, in other connective tissue diseases, such as mucopolysaccharidosis 26 and Paget disease, 17 significant changes in the levels of more free Hyl, glycosylated Hyl, and free Hyl/glycosylated Hyl in urine can be regarded as indicators of collagen degradation. Notably, this downregulation of 5-Hyl in our study was associated with poorer clinical outcomes (lower Lysholm and IKDC scores) in the H-GCL group, indicating that 5-Hyl may be a protective factor for cartilage. The current role of 5-Hyl in articular cartilage injury and ACL tears is unclear, and there may be an undefined but important link between changes in cartilage collagen composition and the inflammatory response that requires further investigation.
Our study has several limitations. First, we did not include a control group with ACL injuries of grade 0 (normal cartilage). While our goal was to investigate metabolic alterations associated with cartilage lesions, future studies could explore the metabolic profile of ACL-injured knees without any cartilage damage to provide a more comprehensive comparison. However, this study does reveal the metabolic alterations of combined cartilage damage in the intra-articular environment of patients with ACL injuries. Second, the present study was performed at a single time point—specifically, at the time of ACLR, when synovial fluid was intraoperatively aspirated. All patients underwent ACLR within 6 weeks (≤42 days) of injury, ensuring a standardized sample collection time frame. To determine the prognostic value of these biomarkers, a longitudinal study of patients with ACL tears and cartilage damage could be considered to observe the changes in metabolites over time and their relationship with functional recovery of the knee. Third, given the limited research resources, the sample size of this study is small. To improve the statistical efficacy of the research and the reliability of the conclusion, the follow-up study should consider expanding the sample size to include patients of different ages, genders, and exercise levels. Finally, the synovial fluid of the knee was mainly analyzed between the groups, which can better reflect local metabolic changes. However, samples representing overall metabolic changes, such as blood and urine, can be further explored, and their relationship with the metabolic characteristics of synovial fluid can be contrastively analyzed in future studies for a comprehensive understanding of the overall metabolic status of patients with ACL injury combined with different levels of cartilage injury. Through the development of these follow-up studies, we can better understand the metabolic changes in patients with knee injury and provide a scientific basis for formulating more effective treatment strategies and preventive measures.
Conclusion
Synovial fluid from patients with ACL tears and high-grade cartilage injuries exhibited significant metabolic disturbances, with 15 upregulated and 19 downregulated metabolites. Four metabolites—OEA, 13-HODE, glucose, and 5-Hyl—were identified as biomarkers linked to inflammation, pain sensitization, and cartilage degradation. These findings enhance our understanding of synovial fluid metabolism and its relationship to knee function, offering insights for developing personalized treatment strategies based on injury severity.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465251362493 – Supplemental material for Effect of Cartilage Lesions on the Metabolic Profiles of Synovial Fluid in Patients With Anterior Cruciate Ligament Tears
Supplemental material, sj-pdf-1-ajs-10.1177_03635465251362493 for Effect of Cartilage Lesions on the Metabolic Profiles of Synovial Fluid in Patients With Anterior Cruciate Ligament Tears by Yingqi Zhao, Jingyi Sun, Ting Zhu, Yunjiao Wang, Yi Qian, Feng Gao and Jingbin Zhou in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors sincerely thank all the patients who contributed their time and samples to this research. The authors also wish to acknowledge Professor Xin Xu from Shanghai University of Sport for his technical advice and instrumentation support.
Submitted October 16, 2024; accepted April 28, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.