
Abstract
Background:
Rotator cuff repair (RCR) often fails because of poor tendon-bone interface (TBI) healing. Nerve growth factor (NGF) has been shown to regulate tenocyte function and promote regeneration, but it lacks sufficient systematic research, limiting its clinical translation.
Purpose:
To evaluate the therapeutic efficacy of NGF-encoding plasmid (pNGF) for TBI healing in a rat acute rotator cuff tear (RCT) model, delivered via nanosphere-hydrogel (NP-GEL) composites.
Study Design:
Controlled laboratory study.
Methods:
We performed physicochemical characterization of pNGF-loaded NP-GEL (morphology, particle size/zeta potential, and in vitro pNGF release) and assessed rat tenocyte responses (proliferation, migration, and protein expression) in vitro. For in vivo studies, 42 Sprague-Dawley rats were randomized into 3 groups after bilateral acute RCT model establishment: RCR alone (control group), RCR combined with local empty plasmid-loaded NP-GEL composites (pEmpty@NP/GEL group), and RCR combined with local pNGF-loaded NP-GEL composites (pNGF@NP/GEL group). Rats were euthanized at 4 and 8 weeks postoperatively (n = 7 rats per time point, 14 shoulders/group). At 4 weeks, 8 shoulders/group were allocated to biomechanical testing, and 6 shoulders/group to histologic analysis. At 8 weeks, 8 shoulders/group underwent pain threshold and gait analysis before biomechanical testing, while 6 shoulders/group underwent micro-computed tomography imaging before histologic analysis.
Results:
In vitro, pNGF@NP/GEL exhibited pH-responsive sustained release (88% at pH 5, 76% at pH 7 over 28 days), and pNGF maximized primary tenocyte proliferation/migration (peak effect at 2.5 μg pNGF). In vivo, the pNGF@NP/GEL group showed superior TBI healing: higher biomechanical strength (maximum load: 32.7 ± 4.9 N vs 25.5 ± 5.2 N in pEmpty@NP/GEL; P = .026 vs 21.6 ± 5.1 N in control; P < .001 at 8 weeks), improved bone microarchitecture (higher bone mineral density at 8 weeks; P < .001), better histologic repair (Modified Histomorphometric Scoring System: 31.3 ± 2.1 vs 25 ± 1 in pEmpty@NP/GEL; P = .015 vs 22.67 ± 2.31 in control; P = .003 at 8 weeks), optimized collagen I/III ratio, and enhanced functional recovery, with only mild neurotrophin-3 upregulation and increased heterotopic ossification (HO) although not in clinically concerning regions.
Conclusion:
NGF gene delivery effectively enhances TBI healing in a rat model of acute RCT histologically, structurally, and functionally via NP-GEL composites, accompanied by mild upregulation of NT-3 and increased HO, although not in clinically concerning regions. Thus, this strategy holds translational potential to improve the clinical outcomes of RCTs.
Clinical Relevance:
The NGF has translational potential to improve clinical outcomes in RCTs.
Rotator cuff repair (RCR) remains plagued by inadequate tendon-bone interface (TBI) healing, associated with 10% to 40% retear rates, persistent chronic pain, and suboptimal functional recovery.17,18 The TBI—a specialized transitional structure comprising tendon, noncalcified fibrocartilage, calcified fibrocartilage, and bone—depends on coordinated tenocyte proliferation, collagen synthesis/remodeling, neurovascular ingrowth, and inflammation modulation for regeneration.27,33 However, these key processes are often dysregulated clinically, leading to compromised healing outcomes.
Nerve growth factor (NGF), the prototypical member of the neurotrophin family, is a multifunctional cytokine with well-established roles in neural development, survival, and repair.3,26 It exerts biological effects primarily through binding to its high-affinity receptor tropomyosin receptor kinase A (TrkA) and low-affinity receptor p75 neurotrophin receptor, triggering downstream signaling cascades, such as the phosphoinositide 3-kinase–Akt and mitogen-activated protein kinase/extracellular signal-regulated kinase pathways, which regulate cell proliferation, differentiation, and survival.19,31 Beyond its neurotrophic functions, a spectrum of preclinical studies has uncovered NGF's pleiotropic bioactivities in musculoskeletal tissue repair, 15 making it a promising therapeutic agent for TBI healing. Relevant experiments have confirmed that NGF activates TrkA signaling to enhance the proliferation and migration of tendon sheath progenitor cells and tenocytes, directly boosting the activity of cell populations responsible for extracellular matrix (ECM) deposition. 4 For collagen remodeling—a critical determinant of mechanical integrity—growing evidence has shown that NGF promotes the expression of type I collagen (the primary structural component of mature tendons and bone) and suppresses that of immature type III collagen, favoring the development of dense, well-organized collagen fiber networks. 2 In inflammatory regulation, NGF drives macrophage polarization toward M2 prohealing phenotypes, mitigating excessive inflammation that impairs TBI regeneration. 37 Furthermore, NGF-dependent TrkA signaling drives skeletal sensory nerve ingrowth and angiogenesis, restoring nutrient supply and sensory innervation—two factors indispensable for TBI stability.4,8 Notably, elevated endogenous NGF levels have been observed in rotator cuff tear (RCT) models, and its depletion impairs repair processes, validating its physiological necessity for tendon-bone regeneration. 22
Extensive orthopedic research has validated NGF as a key regulator in musculoskeletal disorders, mediating fracture healing, inflammatory modulation, and pain regulation. 31 In the shoulder, NGF is implicated in shoulder pain, subacromial bursitis, synovial inflammation, tendinopathy, adhesive capsulitis, and rotator cuff repair. 32 Notably, phase III clinical trials of systemic anti-NGF monoclonal antibodies (Tanezumab, Fasinumab, Fulranumab) were terminated because of rapid joint degeneration in patients with osteoarthritis. 1 These failures highlight the significant risks of systemic NGF modulation and strongly support the need for localized, controlled NGF delivery—precisely the core innovation of our NP-GEL system.
Despite these potentials, NGF's clinical translation is limited by its ultra-short in vivo half-life (minutes to hours), requiring repeated administration, and off-target hyperalgesia from nonlocalized delivery. 12 To address these limitations, a novel hybrid delivery system for localized delivery of NGF-encoding plasmids (pNGF) was used, composed of biodegradable poly(lactic-co-glycolic acid) nanospheres (NP) (a Food and Drug Administration [FDA]-approved material that protects pNGF from degradation) and hyaluronic acid (HA) hydrogel (GEL) (an ECM-mimetic scaffold that immobilizes NP to prevent diffusion).7,20
This study aimed to evaluate the effects of the pNGF on rat tenocyte responses in vitro and TBI healing in a rat acute RCT model in vivo. We hypothesized that sustained pNGF release from the NP-GEL composites would enhance rotator cuff healing in a rat acute RCT model.
Methods
Study Design
All experimental procedures were approved by the Animal Experiment Ethics Committee of Nantong University (Ethics Approval No.: S20210227-002). Two sets of experiments were performed. In vitro experiments: (1) physicochemical characterization of the composites—including morphology, particle size/zeta potential, and in vitro pNGF release kinetics; (2) biological responses of tenocytes isolated from 4-week-old male Sprague-Dawley rats, with proliferation, migration, and protein expression analyzed. In vivo experiments: 42 eight-week-old male Sprague-Dawley rats with a mean weight of 300 g were randomly divided into 3 groups after establishing a bilateral acute RCT model: RCR alone (control group), RCR combined with local empty plasmid-loaded NP-GEL composites (pEmpty@NP/GEL group), and RCR combined with local pNGF-loaded NP-GEL composites (pNGF@NP/GEL group). Postsurgical assessments were conducted at 4 and 8 weeks. Specifically, at 4 weeks, 8 shoulders per group were allocated to biomechanical testing, and 6 to histologic analysis. At 8 weeks, 8 shoulders per group underwent pain threshold testing and gait analysis before biomechanical testing, while 6 shoulders per group received micro-computed tomography (CT) imaging before histologic analysis. No specimens were excluded due to infection, fixation failure, or technical errors, ensuring full utilization of the allocated samples. These assessments were designed to evaluate tissue regeneration, structural integrity, and functional recovery (Figure 1).
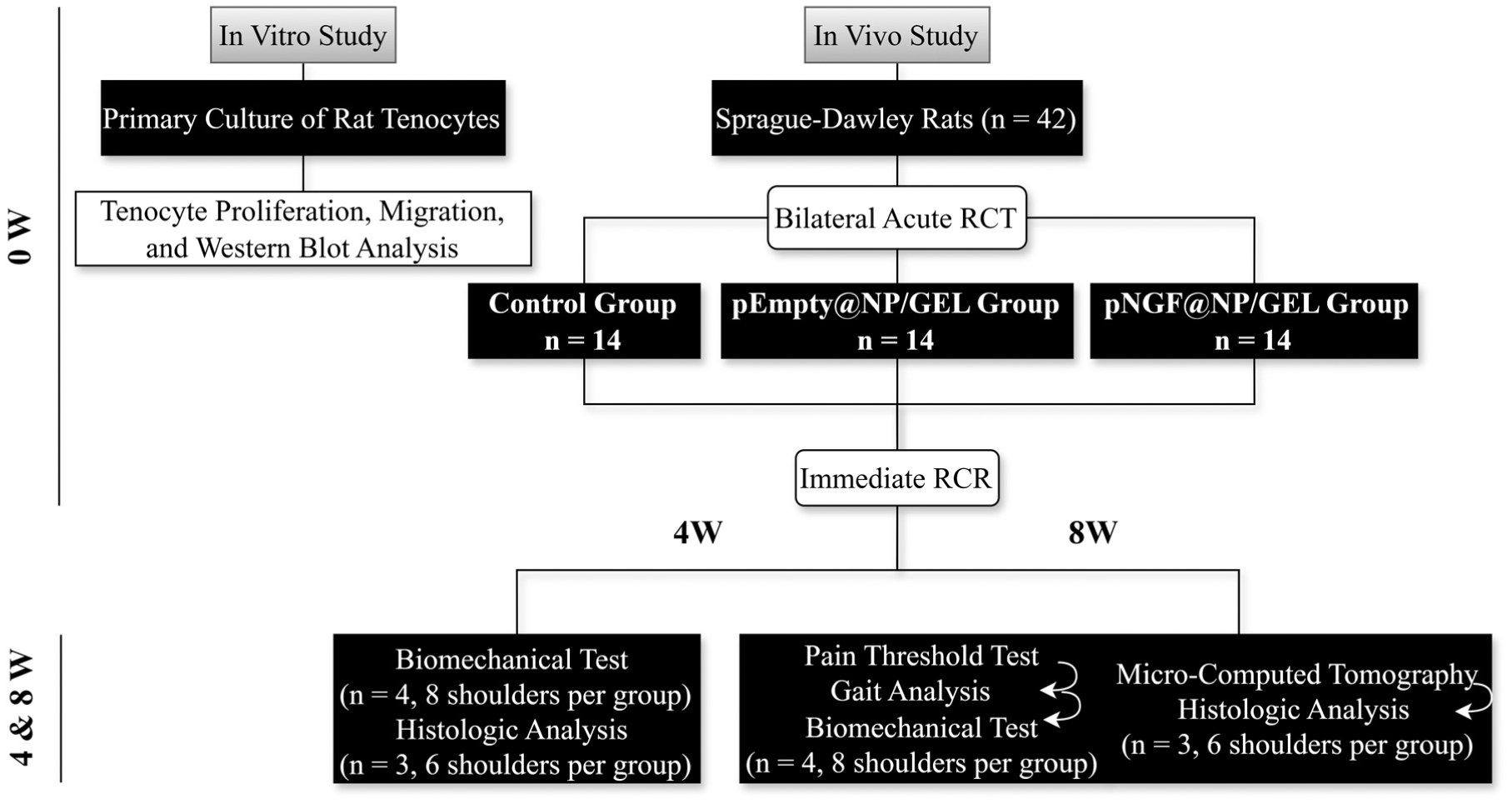
Flowchart illustrating the study design. NGF, nerve growth factor; pEmpty@NP/GEL, empty plasmid-loaded nanosphere-hydrogel composites; pNGF@NP/GEL, NGF-encoding plasmid-loaded nanosphere-hydrogel composites; RCR, rotator cuff repair; RCR, rotator cuff repair.
In Vitro Release Characteristics of pNGF@NP/GEL
In vitro release profiles of pNGF@NP/GEL were evaluated at pH 5 and 7 to assess the system's stability and sustained-release performance in acidic tissue microenvironments. Total pNGF concentration was first quantified via spectrophotometry at 260 nm (designated as n). For release assays, 300 μL pNGF@NP/GEL (5 μg pNGF total) was added to tubes, followed by 200 μL phosphate-buffered saline (PBS) buffer (pH 5 or 7). Tubes were incubated at 37°C in a shaking incubator for release monitoring.
From day 1, supernatants were collected at predetermined time points (1, 3, 5, 7, 10, 14, 21, 28 days) and replenished with equal volumes of matching pH PBS. Collected supernatants were centrifuged (13,000 rpm, 10 min) to remove impurities/nanospheres, and pNGF concentration was measured at 260 nm (designated as np, p = sampling day) for cumulative release calculation. Data were calibrated against a standard curve for accuracy and reproducibility, with pH 5 and 7 release profiles plotted for comparison. All experiments were performed in triplicate. The formula for calculating the in vitro release amount of pNGF@NP/GEL is as follows:
Proliferation of Rat Tenocytes
Cell Counting Kit-8 (CCK-8) assays (Beyotime Biotechnology) were performed in 96-well plates at 24 and 48 hours posttransfection to evaluate rat tenocyte proliferation across different pNGF doses. At each time point, the medium was aspirated and replaced with 100 μL of fresh medium containing 10 μL of CCK-8 solution. After 2 hours of incubation, the optical density was measured at 450 nm with a spectrophotometer.
Migration of Rat Tenocytes
Tenocyte migration was evaluated using a scratch assay. At 24 hours posttransfection, uniform scratches were created perpendicular to the horizontal axis of 6-well plates using sterile 200 μL pipette tips. Wells were rinsed twice with PBS to remove detached tenocytes, and fresh complete medium was added. Scratch regions were imaged at 0, 24, and 48 hours postscratching using an inverted phase-contrast microscope (Olympus). The migration rate was quantified with ImageJ software (National Institutes of Health) as [(initial scratch area - residual scratch area)/initial scratch area] × 100%.
Western Blot Analysis for NGF Protein in Rat Tenocytes
At 48 hours posttransfection, tenocytes were lysed on ice for 30 minutes with Radioimmunoprecipitation Assay lysis buffer containing 1% protease inhibitor (Beyotime). Lysates were centrifuged at 12,000 rpm for 15 minutes at 4°C, and the supernatant was collected as the total protein fraction. Protein concentration was quantified using a bicinchoninic acid assay kit (Beyotime). Equal amounts of protein (30 μg per lane) were separated by 10% SDS-PAGE and transferred to polyvinylidene fluoride membranes (Millipore). Membranes were blocked with 5% nonfat milk in Tris-Buffered Saline with Tween-20 (TBST) for 1 hour at room temperature, then incubated with primary antibodies (NGF: 1:1000, Zenbio; β-actin: 1:5000, ABclonal) at 4°C overnight. After three 10-minute TBST washes, membranes were incubated with horseradish peroxidase (HRP)-conjugated secondary antibody (1:5000) for 1 hour at room temperature. Protein bands were visualized via an enhanced chemiluminescence detection kit (Millipore), and band intensity was quantified using ImageJ software. β-actin was used as the internal control for protein normalization.
Animal Model Establishment
All rats were anesthetized with 3% sodium pentobarbital (intraperitoneal injection). Skin was disinfected with 75% ethanol and draped sterilely. A 1.5-cm longitudinal incision was made along the lateral acromial margin; the supraspinatus tendon was exposed via blunt dissection of the deltoid muscle and acromioclavicular joint opening. A 3-mm full-thickness tear was created at the humeral head insertion of the supraspinatus tendon using microscissors. Two 0.4 mm-diameter intramedullary tunnels were drilled, and the tendon was reattached to its insertion site with 5-0 Prolene sutures (Ethicon) via a modified Mason-Allen technique (Figure S5, available in the online version of this article). Based on the results of our preliminary dose-response biomechanical study, which confirmed 2.5 μg pNGF as the optimal dose achieving the highest maximum load to failure and stiffness at the TBI (Figure S6), 200 μL of pNGF@NP/GEL (containing 2.5 μg pNGF) was uniformly applied to the TBI in the pNGF@NP/GEL group after verifying secure tendon fixation. The pEmpty@NP/GEL group received the same volume of composites with 2.5 μg pEmpty. The acromioclavicular joint was repaired with 4-0 Vicryl sutures (Ethicon) using mattress stitches, and the skin incision was closed with 3-0 silk sutures. Postoperatively, rats were housed in specific pathogen-free facilities with daily welfare checks. At 4 and 8 weeks, 7 rats per group were euthanized (14 shoulders/group, bilateral model); 8 shoulders/group were used for biomechanical testing (plus pain/gait analysis at 8 weeks), and 6 for histologic analysis (plus micro-CT at 8 weeks), with no specimens excluded. Specimens were macroscopically scored using the Modified Macroscopic Evaluation System as previously described 34 (Table S1, available online). Two independent observers (Y.Z. and H.F.), blinded to the experimental groups, performed all macroscopic scoring. Any discrepancies in scores were resolved through open discussion until consensus was reached, with a third, senior, blinded observer (F.Z.) consulted if necessary.
Biomechanical Testing
Supraspinatus tendon-humeral complexes were dissected from the scapula for biomechanical testing. The humeral head was fixed in the testing machine's lower jaw, while the supraspinatus tendon was threaded through a perforated metal washer and secured in the upper jaw with nonslip hemostats. Uniaxial tensile testing to failure was conducted with an Instron 3365 universal testing machine (Instron Corp). Maximum load and elongation were automatically recorded using Bluehill 3 software. Stiffness was calculated as the slope of the linear portion of the stress-distance curve.
Micro-CT Analysis
Humeral heads were harvested at 8 weeks postoperatively, fixed in 4% paraformaldehyde for 24 hours, and then transferred to 70% ethanol for preservation before micro-CT scanning. Scanning was performed using a Bruker SkyScan 1276 micro-CT system (Bruker). Three-dimensional reconstruction and analysis of bone microarchitecture parameters were performed using NRecon and CTAn software (both from Bruker).
Gait Analysis
Functional recovery was evaluated at 8 weeks after surgery using the CatWalk XT system (Version 10.6, Noldus Information Technology), a validated automated gait analysis platform widely used in rodent models of musculoskeletal injury. 6 Before testing (dimly lit environment), rats were trained to traverse a 120 × 10 cm glass runway for 3 consecutive days. During testing, rats walked freely along the runway, and their gait was captured by a high-speed camera. The following parameters were analyzed: stand time, swing speed, stride length, mean intensity, and step cycle, as these have been shown to reflect pain-related gait adaptations in rotator cuff and tendon injury models. 29 For each rat, 3 compliant runs with minimal speed variation were acquired; runs with hesitation or interruption were excluded. Paw prints were automatically detected and manually verified to ensure accuracy.
Pain Threshold Testing
The mechanical pain threshold of the affected forelimb was evaluated at 8 weeks after surgery using von Frey filaments (Stoelting). 16 Rats were acclimated for 30 minutes in a transparent acrylic box with a wire mesh floor. Filaments were applied vertically to the forelimb plantar surface (3 applications per filament, 2 s/application, 5 s interval). The minimum force inducing a withdrawal response (licking, shaking, or retracting the forelimb) was defined as the pain threshold. All testing was performed by 2 independent observers (Y.Z. and H.F.) who were fully blinded to group assignments, and any discrepancies in threshold readings were resolved by consensus discussion with a third senior blinded observer (F.Z.).
Histologic Analysis
Supraspinatus tendon-humeral complexes were harvested for histological analysis. Samples were fixed in 4% paraformaldehyde at room temperature for 24 hours, decalcified in 10% thylenediaminetetraacetic acid (pH 7.4) for 4 weeks, gradient ethanol-dehydrated, paraffin-embedded, and sectioned at 5 μm. Sections were stained with hematoxylin-eosin (HE), Masson's trichrome, and Safranin O (Solarbio): HE staining evaluated inflammatory cell infiltration and tenocyte alignment; Masson's trichrome assessed collagen fiber organization; Safranin O quantified cartilage matrix deposition. Specimens were histomorphometrically evaluated using the Modified Histomorphometric Scoring System as previously described 30 (Table S2, available online). Two independent observers (Y.Z. and H.F.), blinded to the experimental group assignments, performed all histomorphometric scoring. Any scoring discrepancies were resolved through open discussion until consensus was reached, with a third, senior, blinded observer (F.Z.) consulted if disagreement persisted.
For immunohistochemistry, sections were deparaffinized, rehydrated, and antigen-retrieved in citrate buffer (pH 6) for 15 minutes. Endogenous peroxidase was blocked with 3% H2O2 for 10 minutes. Sections were incubated with primary antibodies (collagen I [Col I], collagen III [Col III]), NGF, and neurotrophin-3 (NT-3): 1:500; Proteintech) at 4°C overnight, followed by HRP-conjugated secondary antibody for 1 hour at room temperature. Staining was visualized with 3,3’-diaminobenzidine (DAB, Servicebio) and counterstained with hematoxylin. Slides were mounted after staining and observed under a Leica DMR 3000 microscope (Leica), and the positive area ratio was quantified using ImageJ software.
Statistical Analysis
All data were presented as mean ± standard deviation and analyzed using GraphPad Prism Version 10.4 (GraphPad Software). One-way analysis of variance (ANOVA) with the Tukey post hoc test was used for group comparisons with 1 independent variable; 2-way ANOVA with the Dunnett post hoc test was applied for comparisons involving 2 independent variables. Statistical significance was set at P < .05. To verify that the sample size was sufficient to achieve 80% statistical power for the analyses, post hoc power analyses for ANOVA were performed using G*Power software (Universitat Kiel).
Results
Characterization of pNGF@NP/GEL
NP featured a smooth spherical surface with sparse granular structures. GEL exhibited a typical porous network, facilitating cargo loading and mass transport. The morphology of pNGF@NP was also similarly spherical. Both GEL and pNGF@NP/GEL have typical porous structures. (Figure 2A).
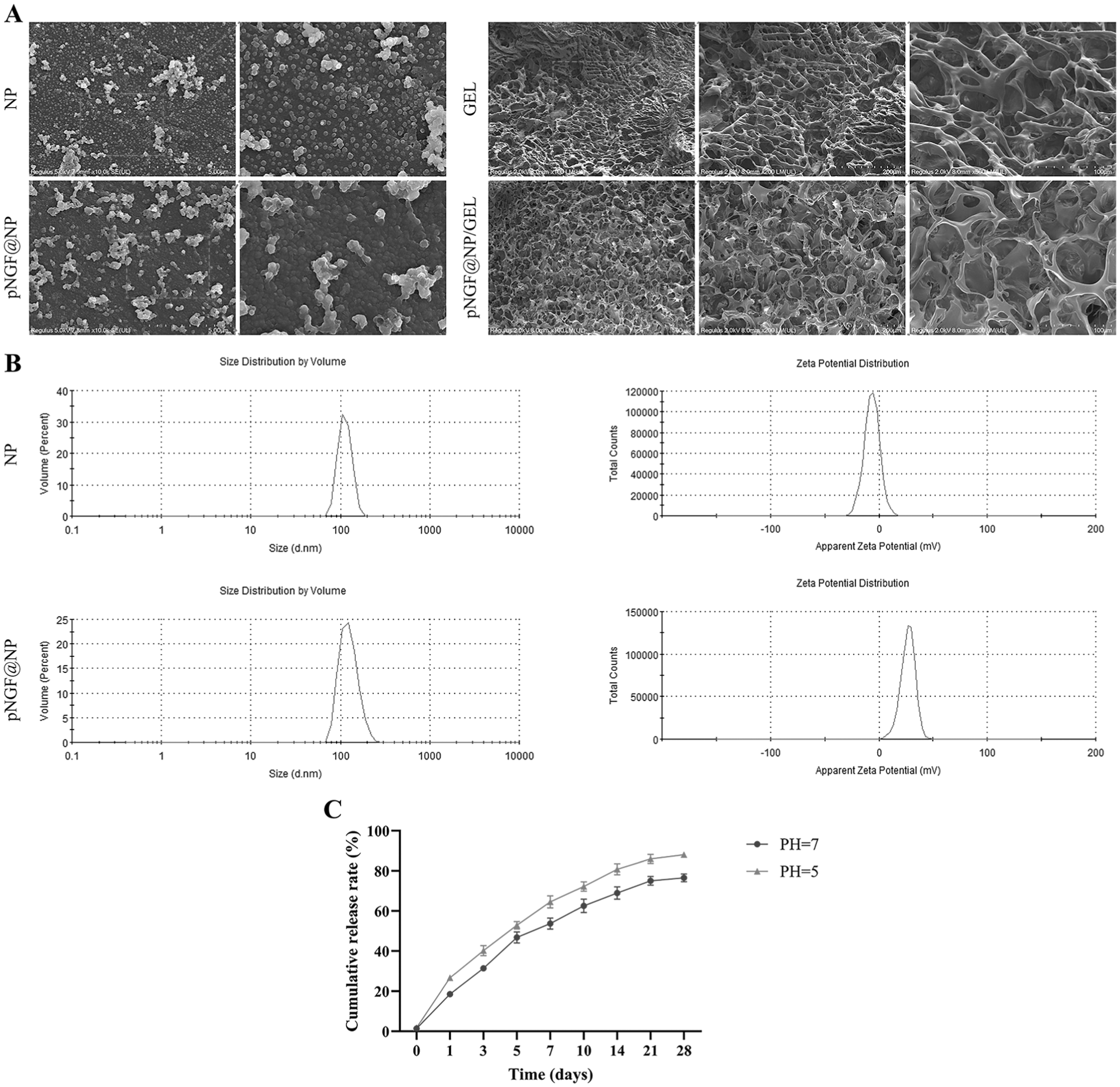
Characterization of the pNGF@NP/GEL delivery system. (A) Scanning electron microscopy (SEM) images of NP, GEL, pNGF@NP, and pNGF@NP/GEL; NP and pNGF@NP showed uniform spherical morphologies, whereas GEL and pNGF@NP/GEL exhibited a porous 3-dimensional network structure favorable for plasmid loading and mass transport. (B) Volume-based particle size distribution and zeta potential of NP and pNGF@NP; NP displayed a peak size of ~102 nm and a zeta potential of ~–5 mV, whereas pNGF@NP showed a slight size increase to ~117 nm and a distinct negative-to-positive charge shift to ~30 mV, confirming successful pNGF loading and surface modification. (C) In vitro cumulative pNGF release profiles from pNGF@NP/GEL in phosphate-buffered saline (PBS) at pH 5 (mimicking the postsurgical inflammatory microenvironment at the injury site) and pH 7 (mimicking normal physiological tissue microenvironment) over 28 days at 37°C; the composite exhibited a pH-responsive sustained-release pattern with an initial mild burst followed by continuous release, achieving a cumulative release rate of ~88% at pH 5 and ~76% at pH 7 at day 28, with higher release efficiency in acidic conditions enabling on-demand pNGF delivery at the inflammatory injury site. Data are presented as mean ± SD. GEL, hydrogel; NGF, nerve growth factor; NP, nanospheres; pNGF@NP/GEL, NGF-encoding plasmid-loaded nanosphere-hydrogel composites; pNGF@NP, NGF-encoding plasmid-loaded nanospheres.
NP and pNGF@NP both exhibited monomodal volume distributions, indicating good monodispersity. Pure NP had a peak particle size of ~102 nm, increasing to ~117 nm for pNGF@NP—this size increment confirmed successful pNGF loading into the NP matrix. For zeta potential, NP showed ~-5 mV, while pNGF@NP exhibited ~30 mV. The negative-to-positive charge shift reflected successful conjugation of positively charged pNGF to NP (Figure 2B).
In Vitro Release Characteristics of pNGF@NP/GEL
Under both pH conditions, pNGF release exhibited an initial burst release followed by sustained release. At 28 days, the cumulative release rate was ~88% at pH 5 (acidic, mimicking the inflammatory microenvironment at the injury site) and ~76% at pH 7 (neutral, mimicking the microenvironment of normal tissues). The higher release efficiency under acidic conditions indicates that the composite system can adapt to the inflammatory microenvironment at the injury site, enabling on-demand enhanced delivery of pNGF (Figure 2C).
In vitro Rat Tenocyte Responses
At 24 hours, pNGF promoted tenocyte proliferation in a concentration-dependent manner, peaking at 2.5 μg (2.2 ± 0.2 [P < .001] vs the control group: 1.3 ± 0.1); the 5 μg (P < .001) and 10 μg (P = .004) groups remained effective. At 48 hours, all pNGF groups showed sustained proliferation elevation (all P < .001 vs control), with the same concentration-dependent trend (Figure 3C).
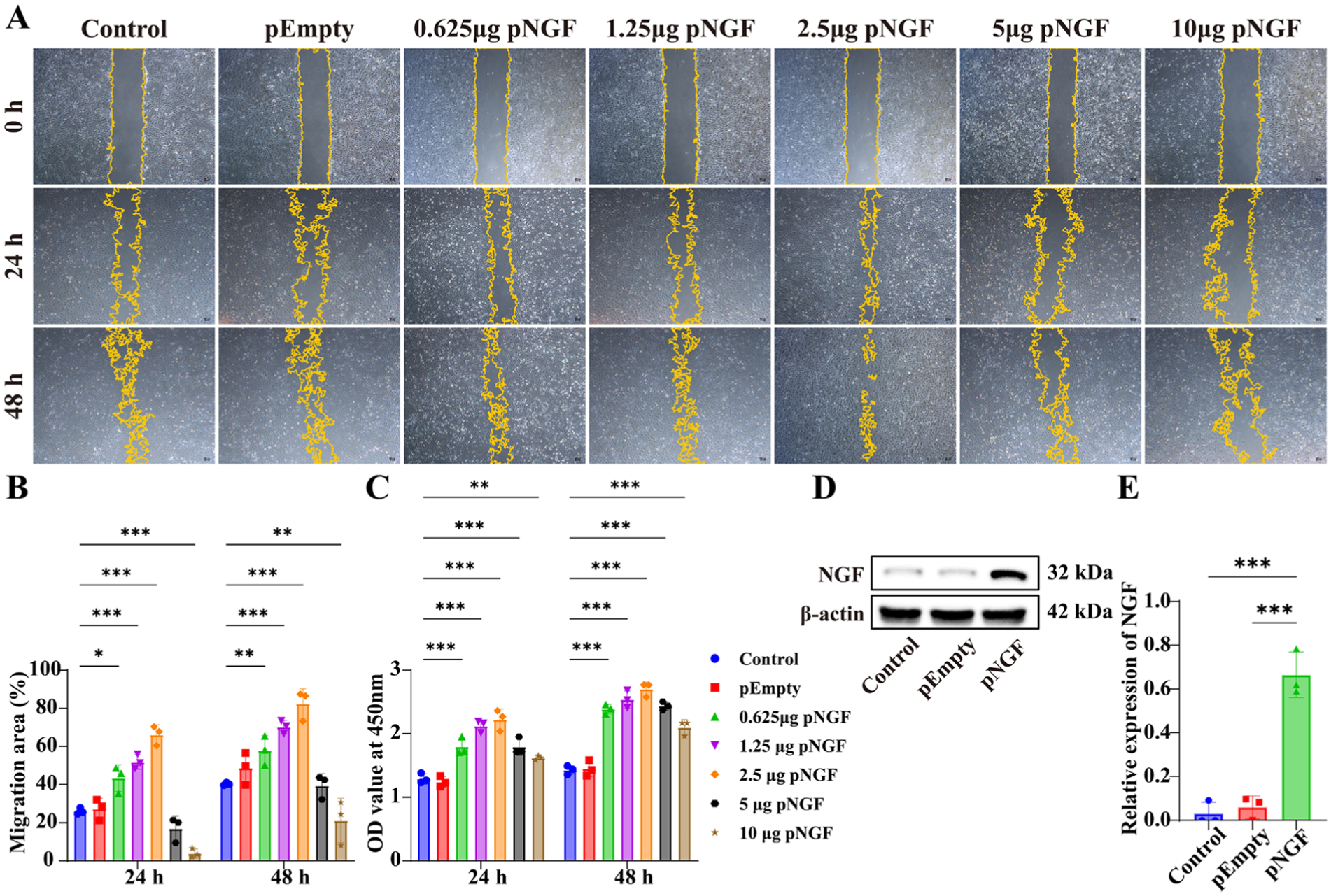
In vitro dose-dependent effects of pNGF on migration, proliferation, and functional NGF protein expression in rat tenocytes. (A) Representative scratch assay images of tenocytes at 0, 24, and 48 hours post-pNGF transfection (gradient doses: 0.625, 1.25, 2.5, 5, 10 μg) with untransfected control and pEmpty groups as controls; scale bar = 100 μm. The 2.5 μg pNGF group exhibited the fastest scratch closure at both 24 and 48 hours, while the 10 μg pNGF group showed significant migration inhibition, demonstrating a biphasic dose-response effect of pNGF on tenocyte migration. (B) Quantification of tenocyte migration area rate at 24 and 48 hours (n = 3), confirming 2.5 μg pNGF as the optimal dose for maximal migratory activity (P < .001 vs control) and significant inhibition at 10 μg (P < .001 vs control). (C) Optical density (OD) values at 450 nm via CCK-8 assay (n = 3) for tenocyte proliferation, showing a dose-dependent promoting effect of pNGF with the peak proliferation at 2.5 μg pNGF at both time points (all pNGF groups P < .001 vs control). (D) Representative western blot images of NGF protein expression at 48 hours posttransfection, with β-actin as the internal loading control. (E) Quantification of relative NGF protein expression (n = 3), verifying that pNGF-transfected tenocytes exhibited significantly higher NGF expression compared with control and pEmpty groups (P < .001), confirming successful functional transfection of pNGF. Data are presented as mean ± SD. *P < .05; **P < .01; ***P < .001. NGF, nerve growth factor; pEmpty, empty plasmid; pNGF, NGF-encoding plasmid.
At 24 and 48 hours, pNGF regulated tenocyte migration in a dose-dependent bidirectional manner: at doses <2.5 μg, the migration ratio increased with dose; at doses >2.5 μg, it decreased. At 24 hours, the migration ratio of the control group was 26% ± 1.7%. The 0.625 μg pNGF group significantly promoted cell migration (P = .010 vs control), with the maximum ratio observed at 2.5 μg (66.2 ± 5.2% [P < .001] vs control). Notably, the 10 μg pNGF group inhibited migration (3.9 ± 2.3% [P < .001] vs control). Consistent with the 24-hour results, the 48-hour data showed that 2.5 μg pNGF retained the strongest promigratory effect (82.4% ± 7.9% [P < .001] vs control), whereas the 10 μg group remained inhibitory (21.1 ± 11.7% [P = .004] vs control) (Figure 3, A and B).
With β-actin as the internal reference control, the pNGF group had a relative NGF protein expression level of 0.664 ± 0.104, which was significantly higher compared with the control group (0.060 ± 0.052; P < .001) and the pEmpty group (0.030 ± 0.053; P < .001). This confirmed the successful transfection and functional expression of pNGF in tenocytes (Figure 3, D and E).
Gross Morphological Observation
At 4 and 8 weeks, the pNGF@NP/GEL group exhibited superior TBI compared with the control groups, characterized by reduced exudate and defects as well as a smoother interface. Macroscopic healing scores, with lower scores indicating better healing: 4 weeks: the control group, 11.3 ± 2.7; the pEmpty@NP/GEL group, 9.8 ± 2.2,; the pNGF@NP/GEL group, 6.2 ± 1.8 (control vs pNGF@NP/GEL: P = .004; pEmpty@NP/GEL vs pNGF@NP/GEL: P = .036); 8 weeks: the control group, 8.5 ± 2.7; the pEmpty@NP/GEL group, 7.3 ± 2.7; the pNGF@NP/GEL group, 3.8 ± 1.6 (control vs pNGF@NP/GEL: P = .011) (Figure 4, A-C).
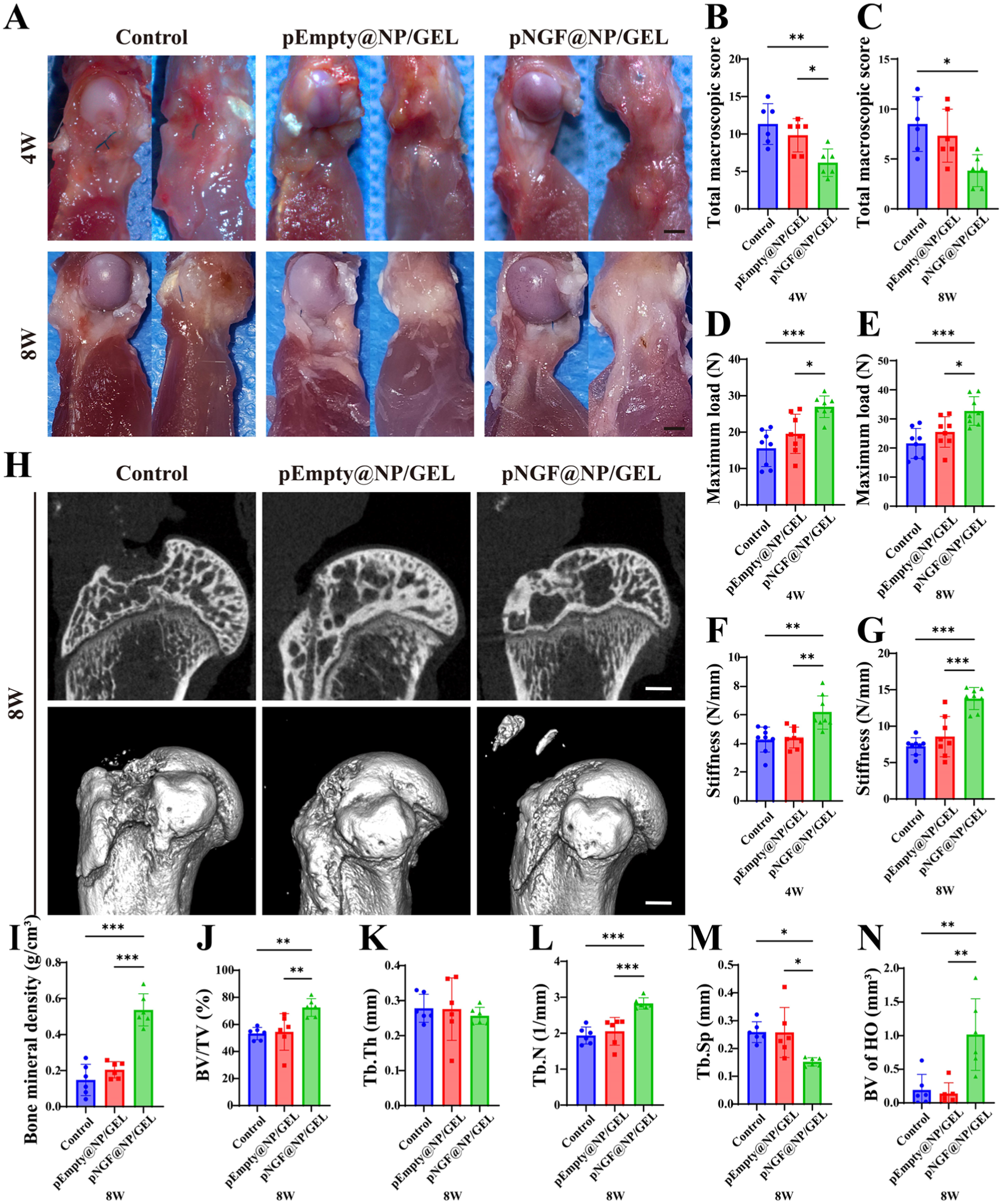
In vivo evaluation of tendon-bone interface healing, biomechanical strength, and bone microarchitectural properties after rotator cuff repair in rats. (A) Gross morphological images of tendon-bone complexes at 4 and 8 weeks; scale bar = 2 mm. The pNGF@NP/GEL group showed a smoother, more integrated interface with fewer defects and reduced exudate than the control groups at both time points. (B, C) Quantification of total macroscopic healing scores (lower scores indicate better healing) at 4 and 8 weeks (n = 6); the pNGF@NP/GEL group had significantly lower scores than the control and pEmpty@NP/GEL groups, indicating superior gross repair. (D, E) Maximum load to failure (N) of tendon-bone complexes at 4 and 8 weeks (n = 8); the pNGF@NP/GEL group exhibited significantly higher maximum load at both time points, with the 8-week value (32.7 ± 4.9 N) being ~51% and ~28% higher than the control and pEmpty@NP/GEL groups, respectively. (F, G) Stiffness (N/mm) of tendon-bone complexes at 4 and 8 weeks (n = 8); the pNGF@NP/GEL group showed markedly elevated stiffness at both time points, with the 8-week value (13.8 ± 1.5 N/mm) being ~90% and ~60% higher than the control and pEmpty@NP/GEL groups, respectively. (H) Representative micro-CT images of tendon-bone complexes at 8 weeks; scale bar = 1 mm. The pNGF@NP/GEL group displayed denser, more continuous trabecular bone at the interface versus sparse, discontinuous trabeculae in control groups. (I-N) Micro-CT quantification of bone microarchitectural parameters at 8 weeks (n = 6): (I) bone mineral density (BMD), (J) bone volume/tissue volume (BV/TV), (K) trabecular number (Tb.N), (L) trabecular thickness (Tb.Th), (M) trabecular separation (Tb.Sp), (N) heterotopic ossification (HO) bone volume (BV). The pNGF@NP/GEL group had significantly higher BMD, BV/TV, Tb.N, BV of HO, and lower Tb.Sp versus control groups. Data are presented as mean ± SD. *P < .05; **P < .01; ***P < .001.
Biomechanical Testing
At 4 weeks, the pNGF@NP/GEL group exhibited a significantly higher maximum load than the control and pEmpty@NP/GEL groups (27 ± 3 N vs 15.6 ± 5.0 N and 19.5 ± 5.4 N; P < .001 and P = .010; post hoc power > 0.8) (Figure 4D). At 8 weeks, the pNGF@NP/GEL group further increased to a significantly higher maximum load than the control and pEmpty@NP/GEL groups (32.7 ± 4.9 N vs 21.6 ± 5.1 N and 25.5 ± 5.3 N, P < .001 and P = .026; post hoc power > 0.8) (Figure 4E).
For stiffness, at 4 weeks, the pNGF@NP/GEL group exhibited a notably higher value than the control and pEmpty@NP/GEL groups (6.2 ± 1.2 N/mm vs 4.3 ± 0.9 N/mm and 4.4 ± 0.7 N/mm, P = .002 and P = .003; post hoc power > 0.8) (Figure 4F). At 8 weeks, the pNGF@NP/GEL group further increased, achieving a notably higher stiffness than the control and pEmpty@NP/GEL groups (13.8 ± 1.5 N/mm vs 7.3 ± 1.2 N/mm and 8.6 ± 2.8 N/mm, P < .001 and P < .001; post hoc power > 0.8) (Figure 4G).
Micro-CT Analysis
At the tendon-bone interface, the pNGF@NP/GEL group exhibited denser, more integrated trabecular bone, whereas the control and pEmpty@NP/GEL groups had sparse, discontinuous trabeculae with obvious repair area defects (Figure 4H).
At 8 weeks, the pNGF@NP/GEL group showed significantly superior bone microarchitecture compared with both the control and pEmpty@NP/GEL groups. Compared with the control group, it exhibited higher bone mineral density (P < .001), bone volume/tissue volume (P = .006), trabecular number (P < .001), bone volume (BV) of heterotopic ossification (HO) (P = .003), and lower trabecular separation (P = .014). Similarly, significant differences with a consistent trend were observed compared with the pEmpty@NP/GEL group (Figure 4I-N).
Gait Analysis
The key gait parameters at 8 weeks revealed significant functional recovery in the pNGF@NP/GEL group versus the control group, characterized by higher left front (LF) mean intensity (P = .003), LF swing speed (P < .001), LF stride length (P = .027), right front (RF) mean intensity (P = .040), RF swing speed (P < .001), RF stride length (P = .035); as well as reduced LF stand time (P = .030), LF step cycle (P < .001), and RF step cycle (P < .001) (Figure 5, B-K).
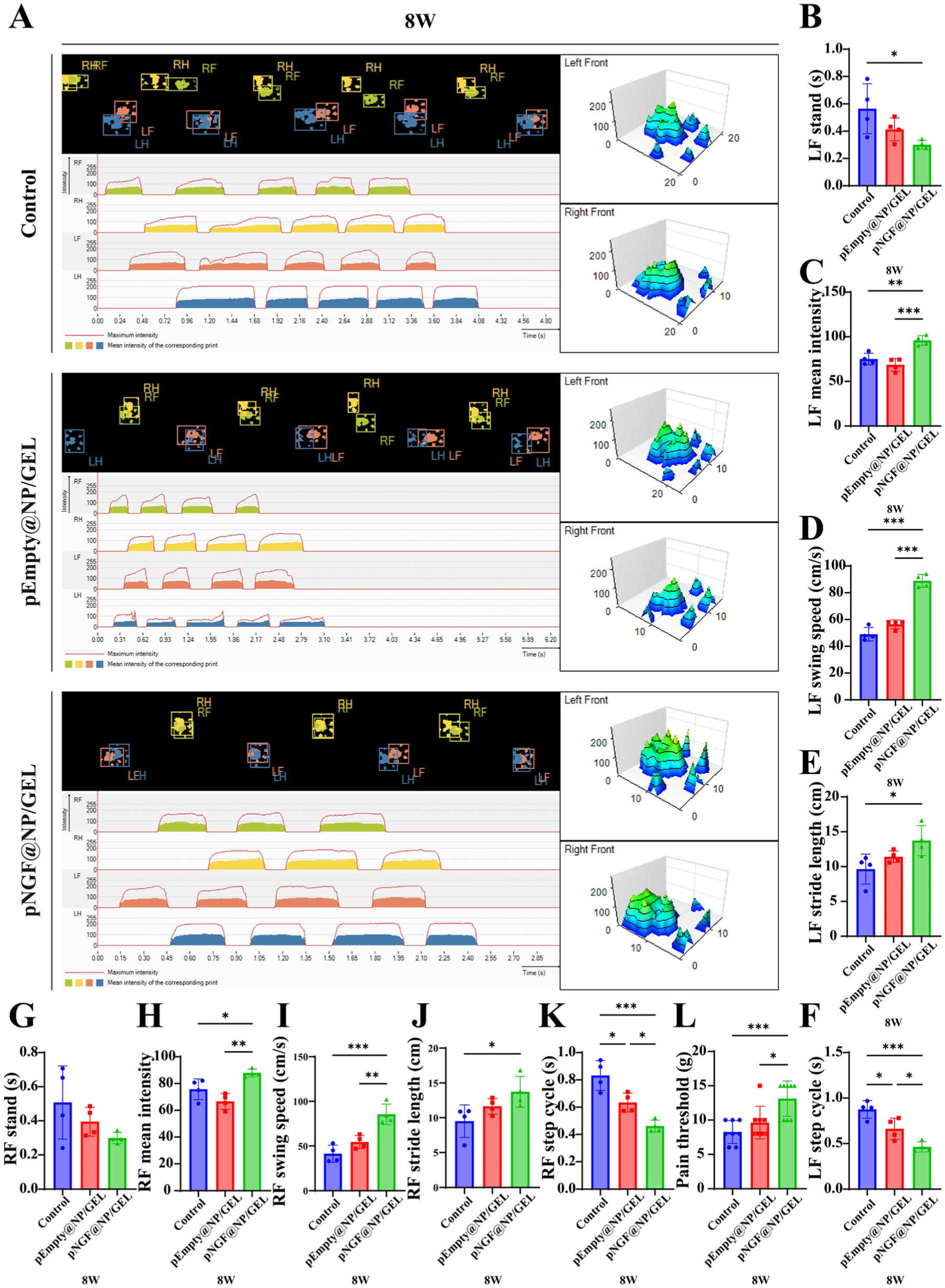
Functional recovery assessment via gait analysis and mechanical pain threshold testing of rats at 8 weeks after rotator cuff repair. (A) Representative CatWalk print views, 2- and 3-dimensional footprint intensity maps at 8 weeks, showing enhanced weight-bearing and gait regularity in the pNGF@NP/GEL group relative to control groups. (B-K) Quantification of key gait parameters (n = 4) for the left front (LF) and right front (RF) paws: (B) stand time, (C) mean intensity, (D) swing speed, (E) stride length, (F) stride cycle (LF); (G) stand time, (H) mean intensity, (I) swing speed, (J) stride length, and (K) stride cycle (RF). The pNGF@NP/GEL group exhibited significantly reduced stand time and stride cycle and increased mean intensity, swing speed and stride length for both forepaws, indicating improved locomotor function and weightbearing capacity. (L) Quantification of mechanical pain threshold (g) of the affected forelimb via von Frey filaments at 8 weeks (n = 8); the pNGF@NP/GEL group had a markedly higher pain threshold (13.1 ± 2.6 g) compared with the control (8.3 ± 1.7 g) and pEmpty@NP/GEL (9.6 ± 2.4 g) groups, reflecting reduced pain sensitivity and improved pain-related functional recovery. Data are presented as mean ± SD. *P < .05; **P < .01; ***P < .001. NGF, nerve growth factor; LF, left front; pEmpty@NP/GEL, empty plasmid-loaded nanosphere-hydrogel composites; pNGF@NP/GEL, NGF-encoding plasmid-loaded nanosphere-hydrogel composites; RF, right front.
Pain Threshold
At 8 weeks, the pain threshold in the pNGF@NP/GEL group was 13.1 ± 2.6 g, which was significantly higher than the control group (8.3 ± 1.7 g; P < .001) and the pEmpty@NP/GEL group (9.6 ± 2.4 g; P = .010) (Figure 5L).
Histologic Analysis
At 4 and 8 weeks, the tendon-bone interface repair quality was evaluated using the Modified Histomorphometric Scoring System (MHSS), and the pNGF@NP/GEL group exhibited significantly higher MHSS total scores compared with the control and pEmpty@NP/GEL groups: at 4 weeks, the pNGF@NP/GEL group scored 19.7 ± 2.1, significantly higher than the control group (13 ± 1, P = .007) and pEmpty@NP/GEL group (14 ± 1.7, P = .014); at 8 weeks, the pNGF@NP/GEL group further increased to 31.3 ± 2.1, maintaining significant advantages over the control group (22.7 ± 2.3, P = .003) and pEmpty@NP/GEL group (25 ± 1, P = .015), collectively indicating superior histomorphometric repair in the pNGF@NP/GEL group across both time points (Figure 6).
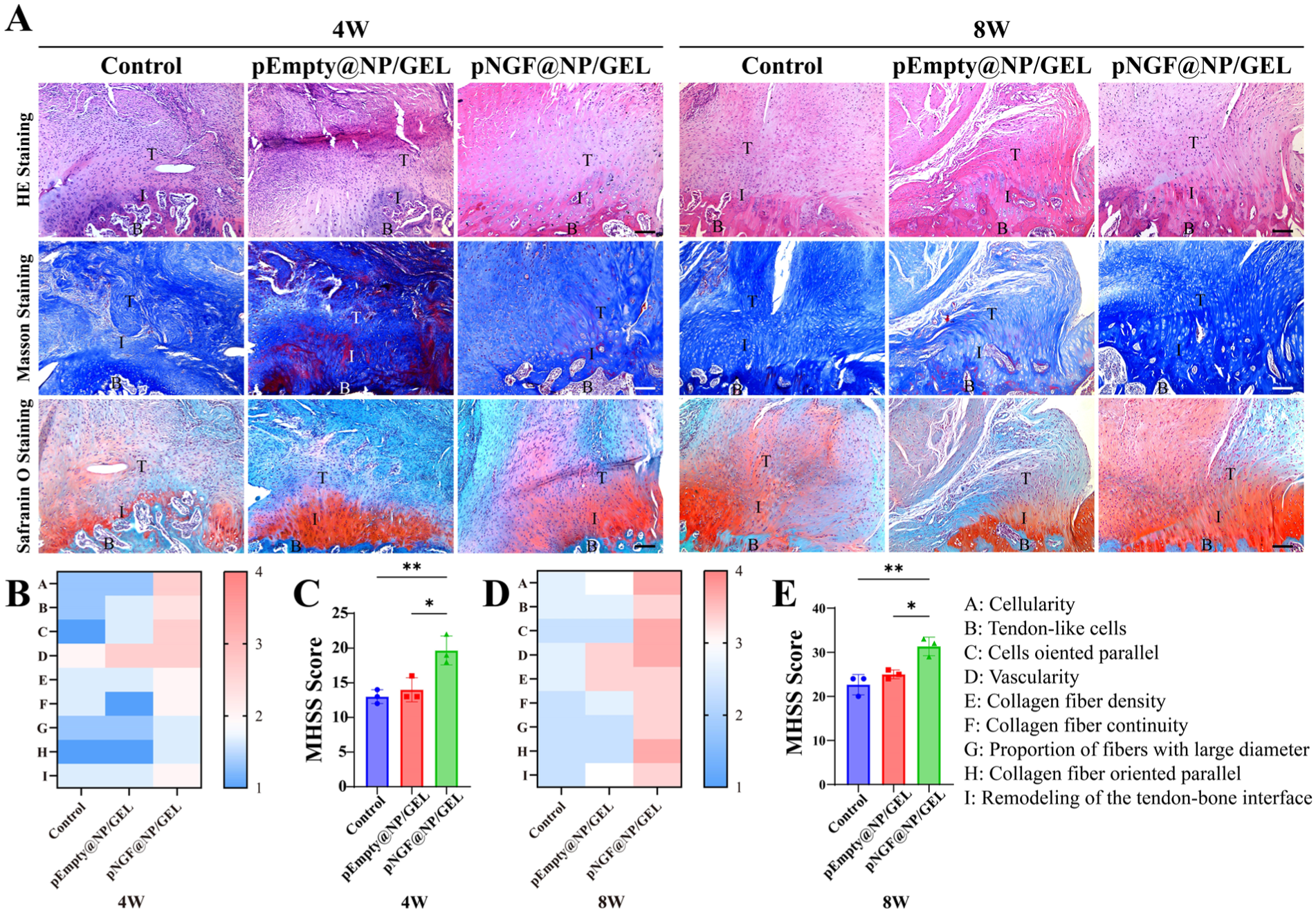
Histologic analysis of tendon-bone interface healing at 4 and 8 weeks after rotator cuff repair in rats. (A) Hematoxylin-eosin (HE), Masson's trichrome, and Safranin O staining of tendon-bone interface tissues at 4 and 8 weeks; scale bar = 100 μm. HE staining showed reduced inflammatory infiltration and aligned tenocytes in the pNGF@NP/GEL group. Masson's trichrome staining revealed a denser, more parallel organization of collagen fibers. Safranin O staining indicated increased cartilage matrix deposition at the interface in the pNGF@NP/GEL group compared with control groups at both time points. (B, D) Heatmaps of histological parameters at 4 and 8 weeks, visually demonstrating superior scoring across all histologic metrics (cellularity, tenocyte proportion, collagen density/orientation, interface remodeling) in the pNGF@NP/GEL group. (C, E) Quantification of Modified Histomorphometric Scoring System (MHSS) scores at 4 and 8 weeks (higher scores indicate better histologic repair, n = 3). The pNGF@NP/GEL group exhibited significantly higher MHSS scores than the control and pEmpty@NP/GEL groups at both time points, confirming superior structural and histological remodeling of the tendon-bone interface. Data are presented as mean ± SD. *P < .05; **P < .01. B, bone; I, interface; NGF, nerve growth factor; pEmpty@NP/GEL, empty plasmid-loaded nanosphere-hydrogel composites; pNGF@NP/GEL, NGF-encoding plasmid-loaded nanosphere-hydrogel composites; T, tendon.
At 4 weeks, the pNGF@NP/GEL group exhibited a significantly higher Col I positive area ratio (5.8% ± 1.7% [P = .017] vs control, 2.1% ± 0.6% [P = .022] vs pEmpty@NP/GEL, 2.4% ± 0.7%) and a lower Col III positive area ratio (2.6% ± 0.8% [P = .006] vs control, 9% ± 2.1% [P = .079] vs pEmpty@NP/GEL, 6% ± 1.5%). This favorable trend persisted at 8 weeks: Col I positive area ratio remained significantly higher (8 ± 1.1 [P = .001] vs control, 2.6 ± 0.9 [P = .003] vs pEmpty@NP/GEL, 3.7 ± 0.8), and Col III positive area ratio remained lower (4.1 ± 1.4 [P = .003] vs control, 14 ± 2.4 [P = .018] vs pEmpty@NP/GEL 10.9 ± 2.3). These results indicate the formation of more mature collagen tissue, as a balanced Col I/Col III ratio favors structural stability of the tendon-bone interface (Figure 7, A, B, C, F, G).
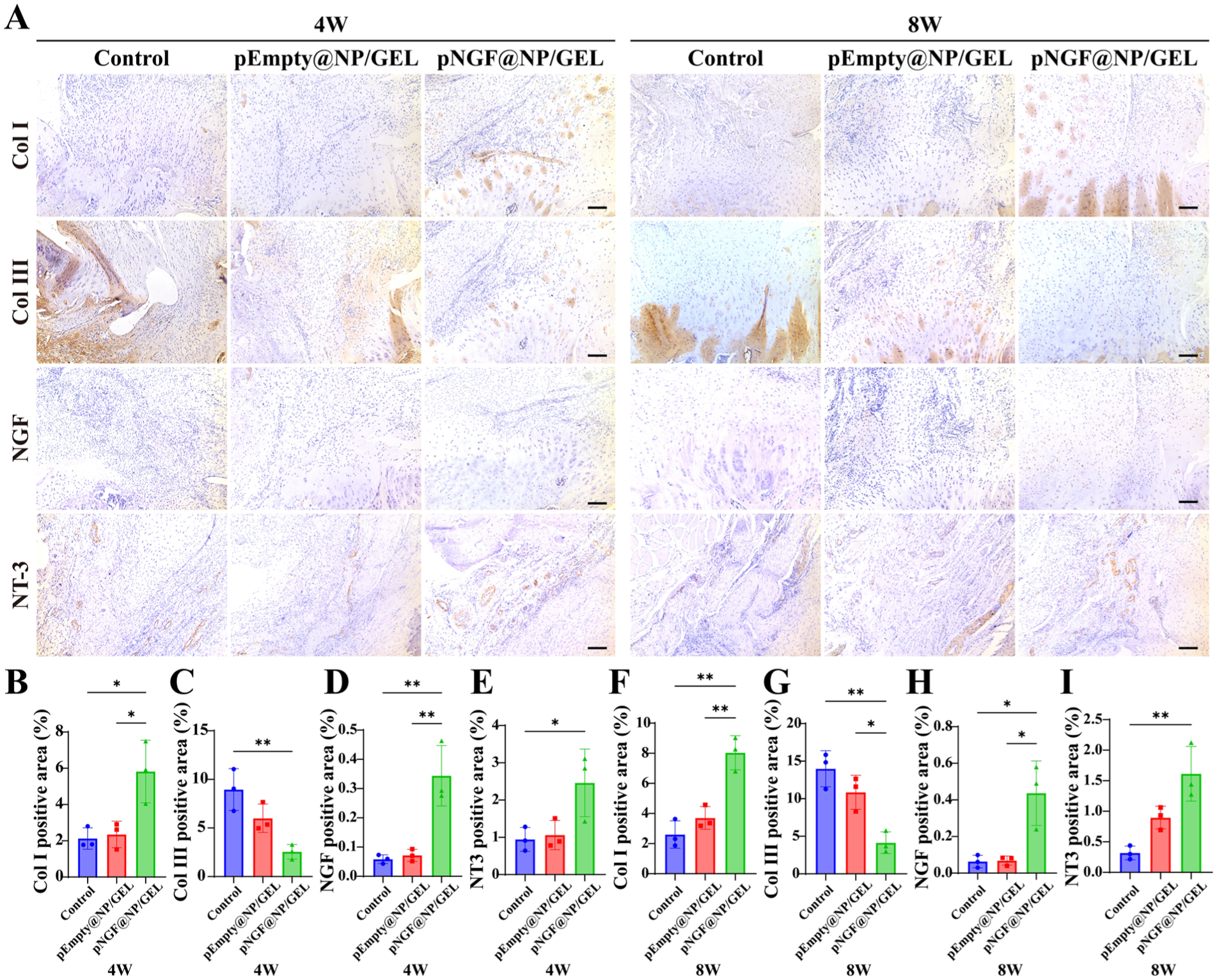
Immunohistochemical staining of key proteins at the tendon-bone interface at 4 and 8 weeks after rotator cuff repair in rats. (A) Representative immunohistochemical staining images of collagen I (Col I), collagen III (Col III), nerve growth factor (NGF), and neurotrophin-3 (NT-3) at the tendon-bone interface at 4 and 8 weeks; scale bar = 100 μm. The pNGF@NP/GEL group showed visibly stronger positive staining for Col I, NGF, and NT-3, and weaker staining for Col III compared with the control and pEmpty@NP/GEL groups at both time points. (B-I) Quantitative analysis of the positive area rate of the 4 proteins (n = 3) at 4 and 8 weeks: (B) Col I, (C) Col III, (D) NGF, (E) NT-3 (4W); (F) Col I, (G) Col III, (H) NGF, and (I) NT-3 (8W). The pNGF@NP/GEL group exhibited a significantly higher positive area rate of Col I, NGF, and NT-3, and a markedly lower positive area rate of Col III at both 4 and 8 weeks relative to the control groups, confirming enhanced mature collagen matrix remodeling, sustained functional NGF expression, and upregulated neurotrophic signaling at the tendon-bone interface after pNGF delivery. Data are presented as mean ± SD. *P < .05; **P < .01. B, bone; I, interface; NGF, nerve growth factor; pEmpty@NP/GEL, empty plasmid-loaded nanosphere-hydrogel composites; pNGF@NP/GEL, NGF-encoding plasmid-loaded nanosphere-hydrogel composites; T, tendon.
The pNGF@NP/GEL group showed significantly elevated NGF positive area rate at 4 weeks (0.3% ± 0.1% [P = .003] vs control, 0.06% ± 0.02% [P = .004] vs pEmpty@NP/GEL, 0.07% ± 0.02%) and 8 weeks (0.4 ± 0.2 [P = .011] vs control 0.06% ± 0.03% [P = .012] vs pEmpty@NP/GEL, 0.07% ± 0.02%), verifying sustained functional NGF expression after plasmid transfection into tenocytes (Figure 7, A, D, H).
Between tendons and muscles, the pNGF@NP/GEL group had a significantly higher NT-3 positive area rate at 4 weeks (2.5% ± 0.9% [P = .048] vs control 0.9% ± 0.3% [P = .064] vs pEmpty@NP/GEL, 1.1% ± 0.4%) and 8 weeks (1.6% ± 0.4%, P = .004 vs control 0.3 ± 0.1 [P = .051] vs pEmpty@NP/GEL, 0.9% ± 0.2%) (Figure 7, A, E, I).
Discussion
The present study systematically investigated the therapeutic efficacy of localized pNGF delivery in an acute RCT model. Notably, as the core bioactive factor, NGF significantly enhanced healing of the TBI across structural, functional, and histological levels—with a critical innovative perspective: building upon previous strategies that have addressed cellular proliferation, ECM remodeling, or anti-inflammatory responses in TBI repair, we innovatively integrate NGF's inherent neuroregulatory properties into the intervention, achieving a more comprehensive and multifaceted healing effect.
NGF bridges neural regulation and tissue repair by promoting peripheral nerve reinnervation and modulating neural-immune-stromal cell crosstalk, optimizing the TBI repair microenvironment.5,23 In vitro, NGF regulated tenocyte behavior in a biphasic dose-dependent manner (2.5 μg as optimal for proliferation/migration, 10 μg inhibitory), 12 with elevated NGF protein expression confirming successful pNGF transfection and molecular mediation of tenocyte responses. 24 In vivo, NGF reduced inflammation, promoted fibrocartilaginous transition zone formation, and improved ECM maturation (upregulated Col I, downregulated Col III)2,9; the pNGF@NP/GEL group exhibited superior biomechanics (~51% higher maximum load, ~90% higher stiffness) and functional recovery, consistent with NGF's pleiotropic effects. 22 Consistent with excellent functional recovery, the pNGF@NP/GEL group exhibited a significantly elevated pain threshold at 8 weeks, contradicting the theoretical risk of NGF-induced hyperalgesia. This favorable outcome is attributed to the NP-GEL system's localized, sustained delivery—confining NGF to the TBI avoided nociceptor overactivation, while improved tissue integration and reduced inflammation indirectly attenuated pathological pain, highlighting the system's dual efficacy in promoting healing and mitigating adverse effects. 10 This pH-responsive profile matches TBI healing stages: rapid burst release in the inflammatory phase (0-3 days), sustained optimal delivery in the proliferative phase (3-14 days), and gradual decline in the remodeling phase (14-28 days). 35 The NP-GEL system's pH-responsive, localized release overcame exogenous NGF's limitations (short half-life, off-target hyperalgesia), maximizing bioavailability at the TBI.
An unexpected finding was the increase in the pNGF@NP/GEL group, supported by micro-CT (higher BV of HO) and NT-3 immunohistochemical evidence. Notably, this elevated BV of HO was not associated with statistically significant differences in HO bone mineral density or BV/TV ratio relative to control groups, and virtually all observed HO lesions were small in size, nonlocalized to the subacromial space or supraspinatus insertion site—key anatomical regions where pathological HO would cause clinical impairment of joint mobility or impinge on TBI healing (Figure S4, available online). 21 Meanwhile, the mild upregulation of NT-3 observed in this study represented a secondary physiological response to NGF-mediated tissue regeneration, rather than a deleterious off-target effect. This modest NT-3 elevation remained restricted to the local repair microenvironment. It did not induce structural abnormalities or functional deficits at the tendon-bone interface, further confirming the favorable safety profile of localized NGF delivery for rotator cuff repair. 28 As a complication of RCR that impairs joint mobility, HO reflects the complexity of neurotrophin-mediated repair. 13 Consistent with previous reports linking NT-3 to mesenchymal progenitor osteogenic differentiation, 36 pNGF upregulated NT-3, suggesting NGF-NT-3 crosstalk in trauma-induced HO, 11 highlighting a pro-healing/HO risk trade-off that warrants optimization for clinical use. This mild effect reflects NGF's pleiotropy—a key FDA concern for growth factor approval (eg, BMP-7’s limited Humanitarian Device Exemption) due to off-target osteogenesis. Our findings highlight that targeted, controlled delivery via the NP-GEL system mitigates this risk: confining 2.5 μg pNGF to the TBI yielded therapeutic healing effects while limiting HO to non-pathological, non-critical anatomical sites (no subacromial impingement risk), addressing a key FDA regulatory consideration for growth factor translation. 21
Despite comprehensive evaluations, this study has several limitations. First, the acute rat RCT model (no chronic degeneration/fat infiltration) and short follow-up (4/8 weeks, no ≥12-week time point) limit translational applicability, alongside inherent rat-human TBI structural/mechanical differences. 14 Second, only male rats and young tenocytes were used; thus, sex- and age-related differences in tendon healing or NGF responsiveness require validation. Third, the optimal clinical pNGF dose remains unclear, as both in vitro biphasic migration (excessive NGF may inhibit cell function) and in vivo HO reflect dose-dependent effects. 12 Indirect evidence for clinical dose range estimation is derived from body surface area allometric scaling (1:69 for rat-to-human) and local delivery bioavailability: the 2.5 μg optimal rat dose translates to a theoretical human local dose of 190-230 μg (calibrated for 100% local bioavailability of the NP-GEL composite and 74% to 89% in vitro release efficiency), with a loaded dose of 200 to 300 μg recommended to compensate for unreleased residual pNGF, consistent with clinical precedents for local growth factor delivery in rotator cuff repair. 25 Fourth, the downstream molecular pathways through which NGF regulates TBI healing remain incompletely elucidated. Nevertheless, these limitations do not overshadow the study's contributions: we validated NGF's core therapeutic role in promoting TBI healing structurally, functionally, and histologically, offered robust preclinical evidence for localized NGF delivery in RCT, pinpointed key optimization directions (eg, dose refinement, mechanism exploration), and laid a foundation for NGF-based clinical RCT therapies.
Conclusion
NGF gene delivery effectively enhances TBI healing in a rat model of acute RCT histologically, structurally, and functionally via NP-GEL composites, accompanied by mild NT-3 upregulation and increased HO, although not in clinically concerning regions. Thus, this strategy holds translational potential to improve the clinical outcomes of RCTs.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261449709 – Supplemental material for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model
Supplemental material, sj-docx-1-ajs-10.1177_03635465261449709 for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model by Ye Yuan, Yurou Zhao, Jiaqi Cheng, Junxi Lu, Hao Feng, Feng Zhang, Xingyu Zhu, Yongxin Hu, Youlang Zhou and Yucheng Sun in The American Journal of Sports Medicine
Supplemental Material
sj-docx-2-ajs-10.1177_03635465261449709 – Supplemental material for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model
Supplemental material, sj-docx-2-ajs-10.1177_03635465261449709 for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model by Ye Yuan, Yurou Zhao, Jiaqi Cheng, Junxi Lu, Hao Feng, Feng Zhang, Xingyu Zhu, Yongxin Hu, Youlang Zhou and Yucheng Sun in The American Journal of Sports Medicine
Supplemental Material
sj-jpg-3-ajs-10.1177_03635465261449709 – Supplemental material for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model
Supplemental material, sj-jpg-3-ajs-10.1177_03635465261449709 for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model by Ye Yuan, Yurou Zhao, Jiaqi Cheng, Junxi Lu, Hao Feng, Feng Zhang, Xingyu Zhu, Yongxin Hu, Youlang Zhou and Yucheng Sun in The American Journal of Sports Medicine
Supplemental Material
sj-jpg-4-ajs-10.1177_03635465261449709 – Supplemental material for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model
Supplemental material, sj-jpg-4-ajs-10.1177_03635465261449709 for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model by Ye Yuan, Yurou Zhao, Jiaqi Cheng, Junxi Lu, Hao Feng, Feng Zhang, Xingyu Zhu, Yongxin Hu, Youlang Zhou and Yucheng Sun in The American Journal of Sports Medicine
Supplemental Material
sj-jpg-5-ajs-10.1177_03635465261449709 – Supplemental material for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model
Supplemental material, sj-jpg-5-ajs-10.1177_03635465261449709 for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model by Ye Yuan, Yurou Zhao, Jiaqi Cheng, Junxi Lu, Hao Feng, Feng Zhang, Xingyu Zhu, Yongxin Hu, Youlang Zhou and Yucheng Sun in The American Journal of Sports Medicine
Supplemental Material
sj-jpg-6-ajs-10.1177_03635465261449709 – Supplemental material for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model
Supplemental material, sj-jpg-6-ajs-10.1177_03635465261449709 for Nerve Growth Factor Gene Delivery via Nanosphere-Hydrogel Composites and Tendon-Bone Interface Healing in a Rat Rotator Cuff Tear Model by Ye Yuan, Yurou Zhao, Jiaqi Cheng, Junxi Lu, Hao Feng, Feng Zhang, Xingyu Zhu, Yongxin Hu, Youlang Zhou and Yucheng Sun in The American Journal of Sports Medicine
Footnotes
Submitted November 30, 2025; accepted April 11, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Natural Science Foundation of China (No. 82302704).
Ethical approval was obtained from the Institutional Animal Care and Use Committee of the School of Medicine, Nantong University (study No.: S20210227-002).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.