
Abstract
Background:
Although a steep posterior tibial slope (PTS) has been reported to cause medial meniscus root tears, few studies have investigated whether the PTS affects healing outcomes
Purpose/Hypothesis:
This study aimed to investigate the influence of PTS on the healing status of repaired medial meniscus posterior roots via second-look arthroscopy. It was hypothesized that a steeper PTS is associated with an increased risk of compromised meniscal healing.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent isolated root repair using modified Mason-Allen sutures between 2019 and 2023 and consented to second-look arthroscopy at 1 year postoperatively were included. The primary endpoint was the morphological healing status characterized as lax versus nonlax tension. Patients were classified into group 1 (nonlax: stable during probing without separation; n = 29) and group 2 (lax: displacement during probing; n = 21). The anatomic PTS was primarily assessed using preoperative lateral radiographic views. Additionally, the medial PTS (MPTS) and lateral PTS (LPTS) were evaluated using preoperative magnetic resonance imaging of the central slices of the respective medial and lateral tibial plateaus. The PTS, MTPS, and LTPS were compared between the 2 groups. The cutoff value associated with lax healing was confirmed.
Results:
The PTS values (mean ± standard deviation) were 6.6°± 3.3° for group 1 and 9.3°± 2.5° for group 2, demonstrating a significantly elevated PTS in group 2 compared with group 1 (effect size, 0.484; 95% CI, 0.237 to 0.672; P = .001) The MPTS value was 5.4°± 3.2° in group 1 and 8.6°± 3.0° in group 2, with a significantly greater PTS in group 2 (effect size, 0.490; 95% CI, 0.245 to 0.676; P = .001). The LPTS value was 4.9°± 2.4° in group 1 and 5.8°± 2.7° in group 2; however, it did not differ significantly (effect size, 0.216; 95% CI, −0.066 to 0.467; P = .126). Based on the cutoff values, a PTS of ≥8.3° (P = .004) and an MPTS of ≥7.7° were identified as a PTS associated with lax healing (P = .001).
Conclusion:
An increased PTS may contribute to lax healing, which in turn progresses to meniscal extrusion after root repair. Consequently, when performing root repair in patients with an increased PTS, it can be anticipated that the postoperative healing and clinical outcomes may not be as favorable as those in patients without an increased PTS.
Medial meniscus posterior root tears (MMPRTs) are radial tears or avulsion injuries occurring at the posterior bony attachment of the medial meniscus.20,34 These tears disrupt meniscal hoop tension, impairing load distribution and increasing articular cartilage pressures, ultimately leading to accelerated degenerative arthritis. 2 Root repair restores hoop tension, normalizes joint biomechanics, and delays osteoarthritis progression.7,9,16 Compared with nonoperative treatment or meniscectomy, root repair demonstrates superior clinical outcomes, including higher functional scores and reduced conversion rates to total knee arthroplasty at both mid- and long-term follow-ups.10,11
Although surgical techniques for MMPRTs have advanced significantly, resulting in improved outcomes, partial healing continues to be occasionally reported.12,13,31,34,35 Various tibiofemoral anatomic factors, including a steeper medial tibial slope, 28 greater varus alignment, 28 narrower intercondylar distances, 3 and notch width, 3 have been documented as major contributors. In particular, a steep posterior tibial slope (PTS) is considered a significant risk factor for MMPRTs because of the increased pressure and shear forces exerted on the posterior meniscus.14,19,26,29,30 This biomechanical environment predisposes the meniscus root to injury by altering loading patterns and stress distribution across the meniscal structure. Consequently, patients with an increased PTS may have a higher risk of initial injury and compromised postoperative healing outcomes. 19
After root repair, the morphological continuity of the repaired root can be assessed using magnetic resonance imaging (MRI). However, second-look arthroscopy allows direct evaluation of the healing results, including the stability and tension of the repaired root. Therefore, second-look arthroscopy is considered to be more reliable than MRI for assessing healing outcomes after root repair. 27
However, although a steep PTS has been reported to cause root tears,14,19,29 few studies have investigated whether the PTS affects healing outcomes using second-look arthroscopy. Given that the integrity of meniscal healing plays a critical role in long-term clinical success, understanding the relationship between the PTS and healing outcomes is essential. Therefore, the present study aimed to determine whether the PTS influences the healing status of repaired medial meniscus posterior roots, as assessed using second-look arthroscopy. It was hypothesized that a steeper PTS would be associated with an increased risk of compromised meniscal healing.
Methods
Study Population
This retrospective study protocol was approved by the Hanyang University Guri Hospital Institutional Review Board (2025-07-047-001), and written informed consent was obtained from all participants. Patients who agreed to undergo both second-look arthroscopy and MRI preoperatively between 2019 and 2023 were included in the study. All patients who underwent MMPRT repair during the study period were screened for eligibility.
MMPRT was defined as a complete radial tear within 9 mm of the medial meniscus posterior bony attachment, as identified on MRI (Intera Achieva; Philips). The diagnostic criteria were as follows: (1) the absence of an identifiable meniscus or the presence of a high-intensity signal replacing the normal dark meniscal signal (ghost sign) in the sagittal plane, (2) a vertical linear defect at the root in the coronal plane, and (3) a radial linear defect at the posterior insertion point in the axial plane.22,25 All root tears included in this study were classified as type 2 according to the LaPrade classification system. 22
The inclusion criteria of root repair were as follows: (1) patients with persistent knee pain in whom MMPRT was confirmed by MRI, (2) patients who underwent arthroscopic pull-out fixation using modified Mason-Allen sutures, (3) patients with a Kellgren-Lawrence (K-L) grade ≤2, (4) patients willing to return to their previous activity level, (5) patients willing to use crutches for at least 6 weeks postoperatively, (6) patients who adhered to postoperative rehabilitation protocols and were willing to modify their lifestyle to avoid deep knee flexion, (7) patients with the presence of a meniscal condition suitable for fixation without complex root tears or degenerative changes, and (8) patients able to undergo second-look arthroscopy and a patient-reported outcome measure evaluation at a minimum follow-up of 1 year. Patients who underwent combined MMPRT repair with high tibial osteotomy, had concomitant ligament injuries or a history of previous knee surgeries, or were unwilling to undergo second-look arthroscopy were excluded (Figure 1). Concomitant high tibial osteotomy was indicated for patients with a varus hip-knee-ankle angle >5°.
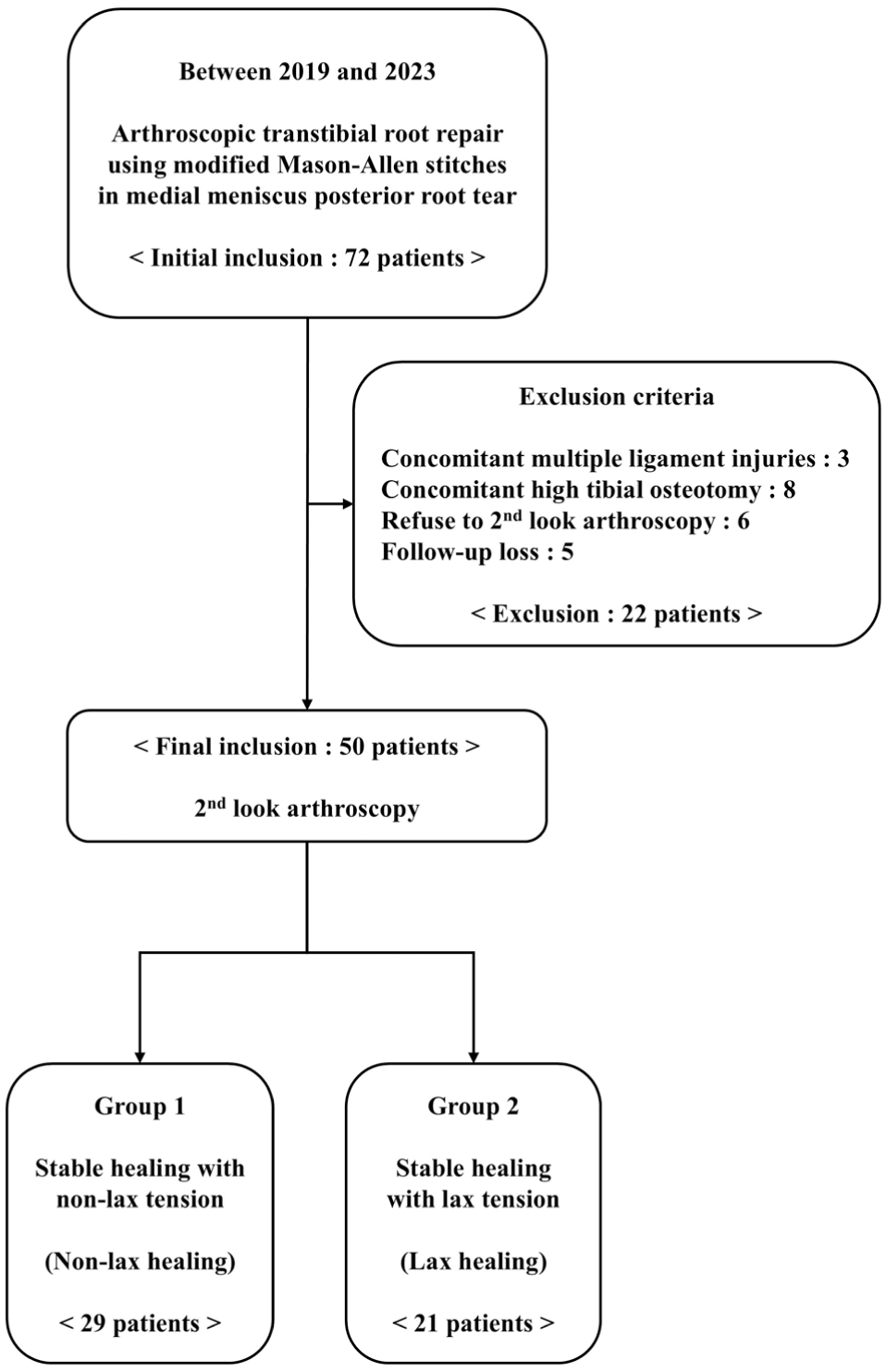
Flowchart of included participants.
During the preoperative period, patients were interviewed in the outpatient department to directly evaluate their clinical scores and radiological findings. Clinical scores were assessed at 3, 6, and 12 months postoperatively and annually thereafter. Patient identification was based on the medical records and prospectively collected data from a clinical database. All medical records were retrospectively reviewed to obtain descriptive and clinical characteristics of the included patients.
Surgical Technique for Pull-out Fixation
All surgical procedures were performed by a single surgeon (K.S.C.) using a transtibial pull-out repair technique with modified Mason-Allen sutures. 8 Once MMPRT was confirmed through arthroscopic examination, a shaver was used to remove fibrous tissue and expose fresh meniscal tissue. A curette was then inserted to create a bone bed at the native root insertion site, located medial to the posterior cruciate ligament and posterior to the medial eminence of the tibia. 33 Subsequently, a crescent-shaped suture hook (Linvatec) loaded with No. 1 polydioxanone (PDS) (Ethicon) was used. The hook tip was passed through a point 5 mm medial to the torn edge of the meniscus. The PDS suture was advanced, and another was placed inside the first suture. A horizontal loop was then completed using the shuttle-relay method. One or 2 simple vertical stitches were added to the overlay and cross the horizontal suture. A single tibial tunnel was created by inserting a Kirschner wire at the far lateral point of the bone bed, immediately medial to the posterior cruciate ligament, following the ACUFEX DIRECTOR MRR Curved Aimer Guide (Smith & Nephew). A metal wire loop was passed through the tibial tunnel and withdrawn along with the PDS suture strands. The meniscus was reduced and stabilized after the sutures were removed. The suture ends were tied over an EndoButton (Smith & Nephew) on the anteromedial tibial cortex. The fixation was performed after elevating the periosteum, with the knee maintained in full extension (0° of flexion).
Postoperative Rehabilitation
Range of motion exercises were initiated after 3 weeks of immobilization and gradually progressed, reaching 90° of flexion by 6 weeks postoperatively. Toe-touch weightbearing with crutches began immediately after surgery, with a brace locked in full extension during the first 3 weeks. Progressive partial weightbearing exercises were initiated at 3 weeks postoperatively. Full weightbearing and progressive closed kinetic chain strengthening exercises were initiated at 6 weeks. A return to activities of daily living was allowed after 3 months. The patients were advised to avoid deep knee flexion beyond 120° to minimize the risk of reinjury. Patients were allowed to return to preinjury activities after 6 months, provided they were pain-free and fully capable of normal daily activities.
Clinical Outcomes
Clinical outcomes were assessed using the Lysholm score, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Knee injury and Osteoarthritis Outcome Score (KOOS), and radiological findings. These scores were assessed preoperatively and at the time of second-look arthroscopy. One author (S.H.P.) who was not involved in the surgical procedures evaluated all clinical scores. Preoperative and final clinical scores were compared for each group, and the final results of the groups were compared
Radiological Outcomes
The Rosenberg 45° posteroanterior standing view was used to evaluate the K-L grade and measure medial joint space width both preoperatively and at the final follow-up. 32 The K-L grade (0/1/2/3/4) was assessed based on established criteria, ranging from no degenerative change (grade 0) to severe joint space narrowing with cysts and sclerosis (grade 4). 20 The medial joint space width was measured manually using a graduated magnifying lens on a picture archiving and communication system (PACS). The minimum distance between the subchondral cortical bone margins of the medial femoral condyle and the tibial plateau was selected along the perceived vertical line. Preoperative and final K-L grades and joint space widths were compared within and between groups.
The PTS was measured from a preoperative lateral radiographic view. The center of the tibial shaft was marked at 2 points: 1 cm below the tibial tubercle and 5 cm distally. These points were connected to define the longitudinal tibial axis (line 1). Line 2 was drawn perpendicular to the longitudinal axis. A line connecting the highest anterior and posterior points of the tibial plateau was drawn (line 3). The angle between lines 2 and 3 was defined as the PTS (Figure 2). On the MRI, the medial PTS (MPTS) and lateral PTS (LPTS) were measured at the center of the medial and lateral plateau slices, respectively. Measurements of the LTPS and the MTPS were collected based on the method described by Hashemi et al. 18 The angles between the line perpendicular to the longitudinal axis of the tibia and the tangential lines connecting the uppermost superior-anterior and posterior cortex of the medial and lateral tibial plateaus were measured (Figure 3).
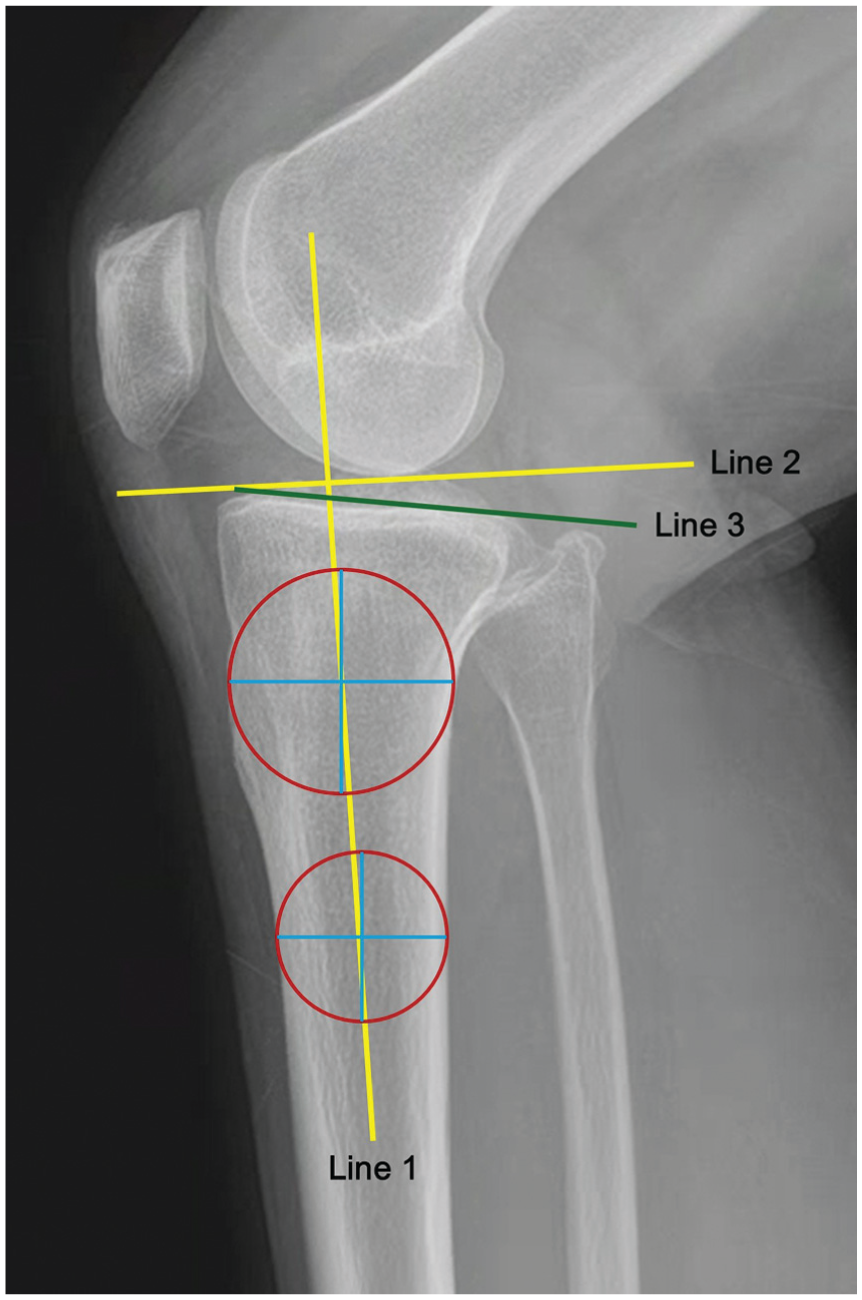
These points (1 cm below the tibial tubercle and 5 cm distally) were connected to define the longitudinal tibial axis (line 1). Line 2 was drawn perpendicular to the longitudinal axis. A line connecting the highest anterior and posterior points of the tibial plateau was drawn (line 3). The angle between lines 2 and 3 was defined as the posterior tibial slope.
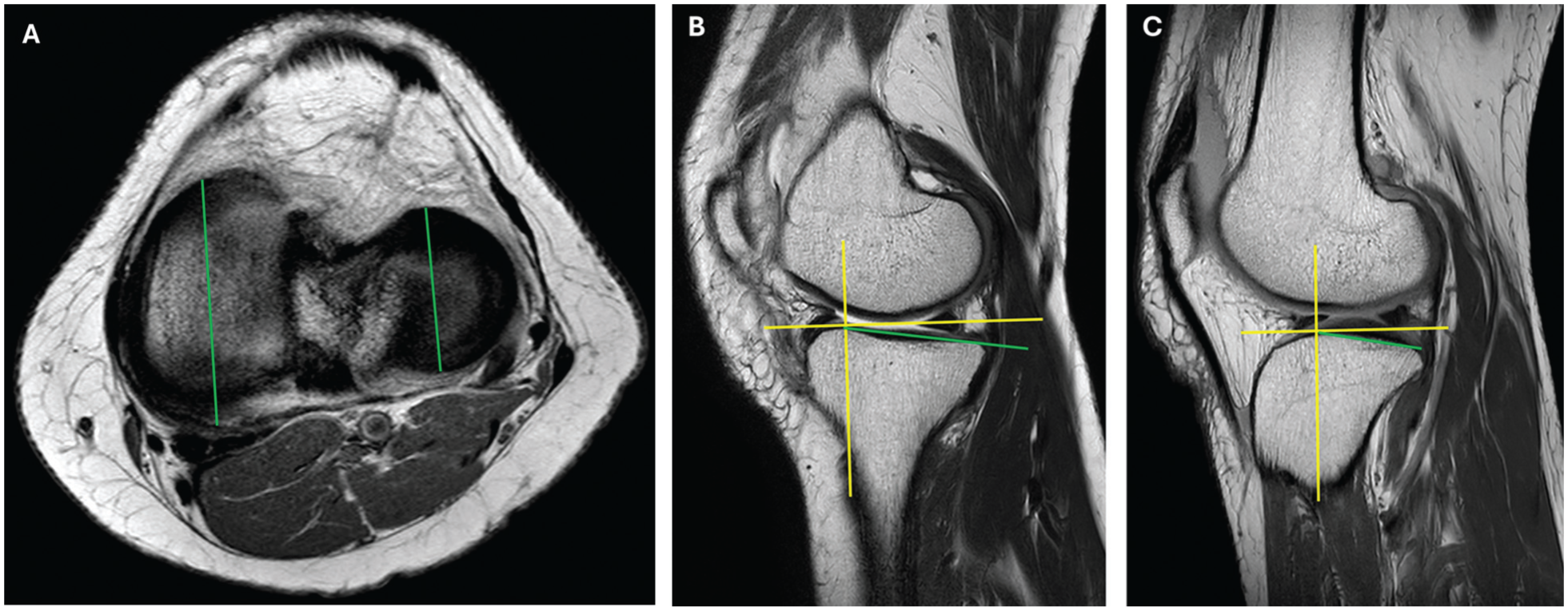
MRI determination of the lateral tibial posterior slope (LTPS) and medial tibial posterior slope (MTPS) according to the measurement method of Hashemi. (A) The corresponding location of the sagittal planes in the medial and lateral aspects of the tibial plateau for determination of the MTPS and LTPS. (B) An axis perpendicular to the diaphyseal axis is reconstructed on the anterior peak of the medial tibial plateau and the MTPS is measured. (C) The same method is used to determine the LTPS.
Radiographic images were examined independently by 2 authors (S.H.P. and K.S.C.) blinded to the procedures used in consultation with a single experienced musculoskeletal radiologist. All radiographic measurements were documented 3 times at 2-week intervals using PACS, and the means of these measurements were used in our analysis. Intraclass correlation coefficients (ICCs) were calculated to determine the interobserver and intraobserver reliability of the differences in the measurements of the PTS, MPTS, LPTS, height of the medial joint space, and K-L grade. An ICC value <0.5 was considered poor agreement; 0.5 to 0.75, moderate; 0.76 to 0.90, good; and >0.90, excellent. 37
Meniscal Healing Results From Second-Look Arthroscopy
With the patient's consent, second-look arthroscopy was performed 1 year postoperatively by the same surgeon who performed the initial root repair procedure. The healing status of the repaired meniscus was assessed by probing and evaluating both the morphological continuity between the meniscus and bone bed (intact vs nonintact) and the tension at the root attachment (lax vs nonlax). Morphological continuity was defined as intact when the root tissue remained connected to the bony footprint. Nonlax tension was indicated by firm resistance of the repaired root to probing, whereas lax tension was indicated by loose tissue on probing. Healing outcomes were classified into 3 categories: (1) intact meniscus with nonlax tension (group 1) (Figure 4A), (2) intact meniscus with lax tension (group 2) (Figure 4B), and (3) healing failure, defined as a nonintact meniscus lacking continuous integration with the bone bed. We utilized a binary classification based on the tactile response to probing—specifically, distinguishing between firm resistance (group 1) and easily displaced tissue (group 2). During arthroscopic examination, the cartilage condition was evaluated according to the International Cartilage Regeneration & Joint Preservation Society classification as follows: grade 1, cartilage exhibits superficial, blunt gaps, as well as superficial cracks; grade 2, cartilage damage depth is <50% of cartilage depth; grade 3, cartilage damage depth is >50% of cartilage depth but does not reach the subchondral bone; and grade 4, there is total cartilage tear with exposure of the subchondral bone. 5
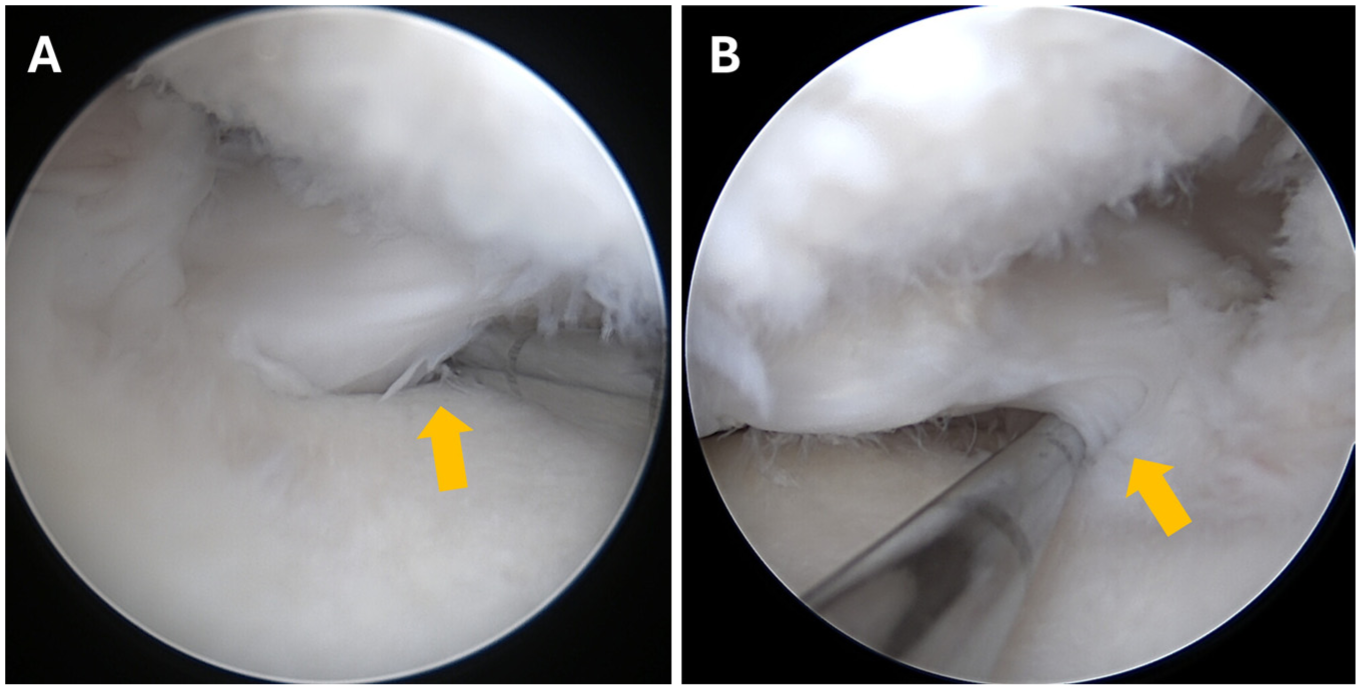
Second-look arthroscopic images with a 30° arthroscope through the anterolateral portal showing the repaired medial meniscus root. (A) Intact roots with nonlax tissues observed by probing. (B) Intact roots with lax tissues observed by probing.
Statistical Analysis
Statistical analyses were conducted using the SPSS software (Version 22.0 for Windows; IBM Corp). Statistical significance was set at 5% (P < .05). The Mann-Whitney U test was used to compare variables that were nonnormally distributed as well as other nonparametric data between groups. The Wilcoxon signed-rank test was used to assess the differences between the preoperative and final outcomes within each group. Categorical variables were analyzed using the chi-square test. The Fisher exact test was applied when >20% of the expected cell count exceeded 5. To identify the cutoff values for independent factors, receiver operating characteristic analysis was performed, including calculation of the area under the curve (AUC). The AUC values were categorized as excellent (≥0.9), good (0.8-0.9), fair (0.7-0.8), or poor (<0.7).
Results
This study included 50 patients (Figure 1). The mean age of the participants was 58.2 ± 6.1 years (Table 1), and the mean interval between root repair and second-look arthroscopy was 12.4 ± 1.4 months. There were no significant differences in the baseline clinical characteristics or descriptive characteristics between the groups (Table 1). All patients demonstrated an intact meniscus with continuous integration between the meniscal tissue and bone bed. Among patients with intact healing, 29 (58%) had stable healing with nonlax tension (group 1), whereas 21 (42%) demonstrated stable healing with lax tension (group 2).
Preoperative Demographics, Clinical Scores, and Diagnostic Study Findings of the Groups a
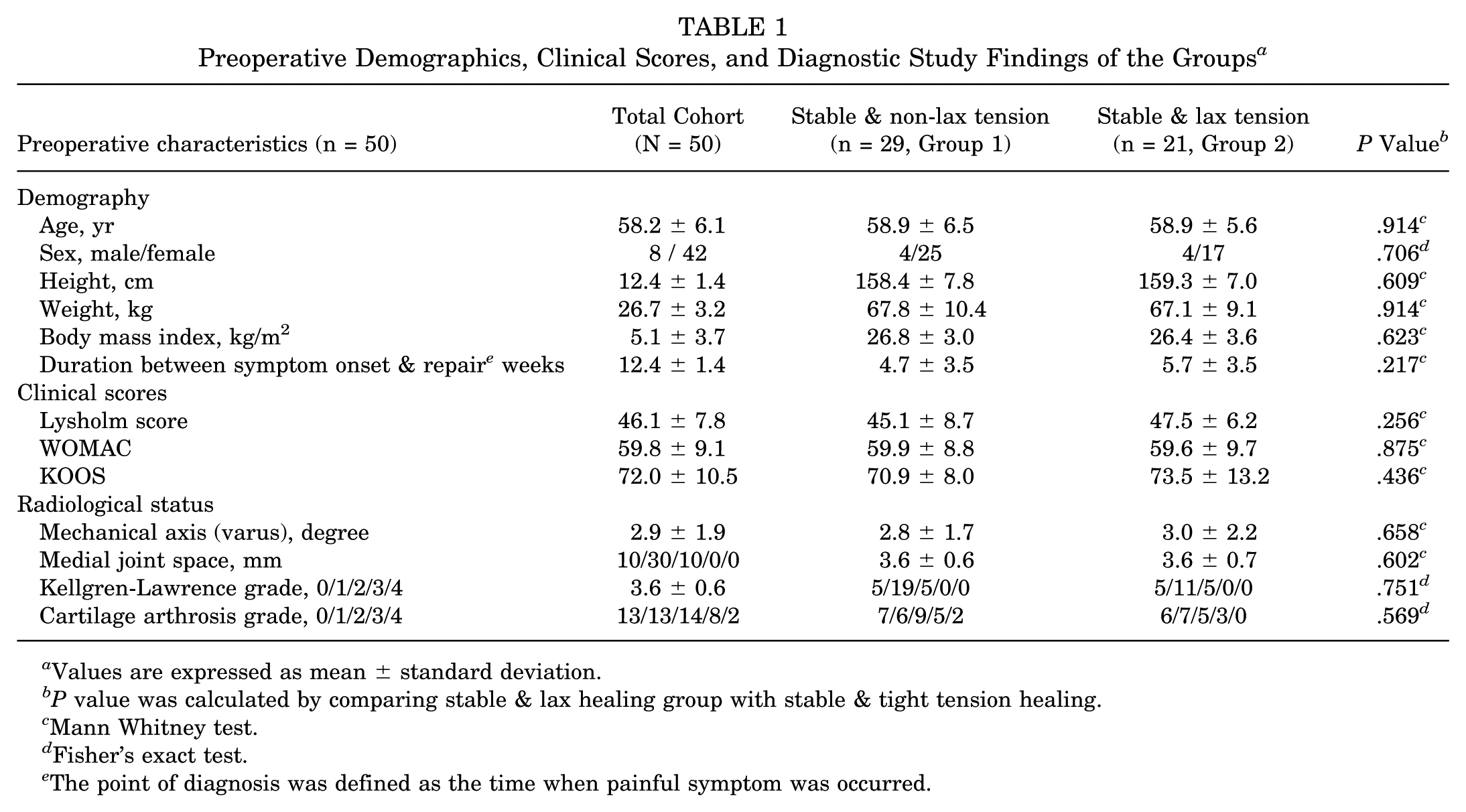
Values are expressed as mean ± standard deviation.
P value was calculated by comparing stable & lax healing group with stable & tight tension healing.
Mann Whitney test.
Fisher's exact test.
The point of diagnosis was defined as the time when painful symptom was occurred.
Clinical Outcomes
Significant improvements in clinical outcomes were observed in both groups 1 and 2 with an increase in the Lysholm score and decreases in the WOMAC score and KOOS from the mean preoperative to postoperative values (P < .05) (Table 2). When comparing the final outcomes between groups 1 and 2, group 1 exhibited more favorable clinical outcomes than group 2 (P < .05) (Table 3); notably, both groups achieved the minimal clinically important differences. 13
Preoperative and Postoperative Clinical Outcomes and Diagnostic Study Findings a
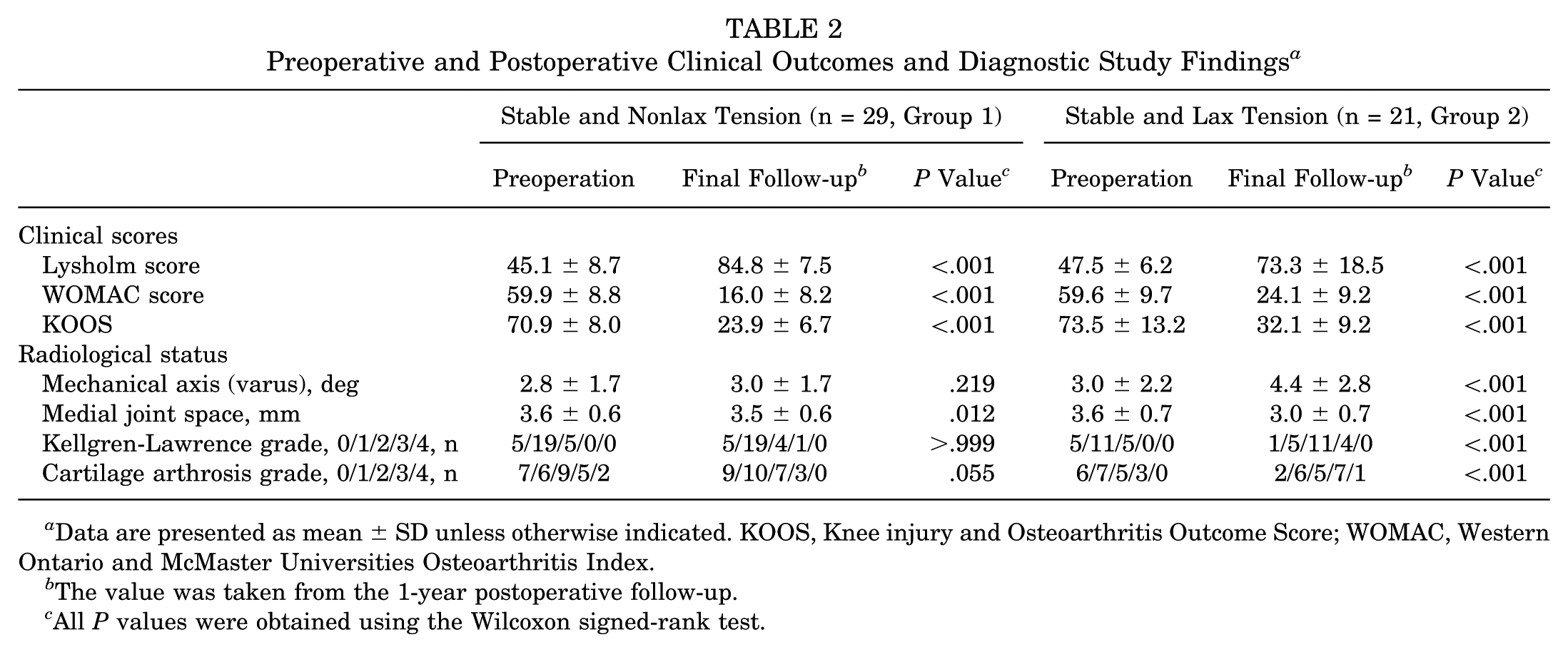
Data are presented as mean ± SD unless otherwise indicated. KOOS, Knee injury and Osteoarthritis Outcome Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
The value was taken from the 1-year postoperative follow-up.
All P values were obtained using the Wilcoxon signed-rank test.
Postoperative Clinical and Radiological Outcomes of Groups 1 and 2 a
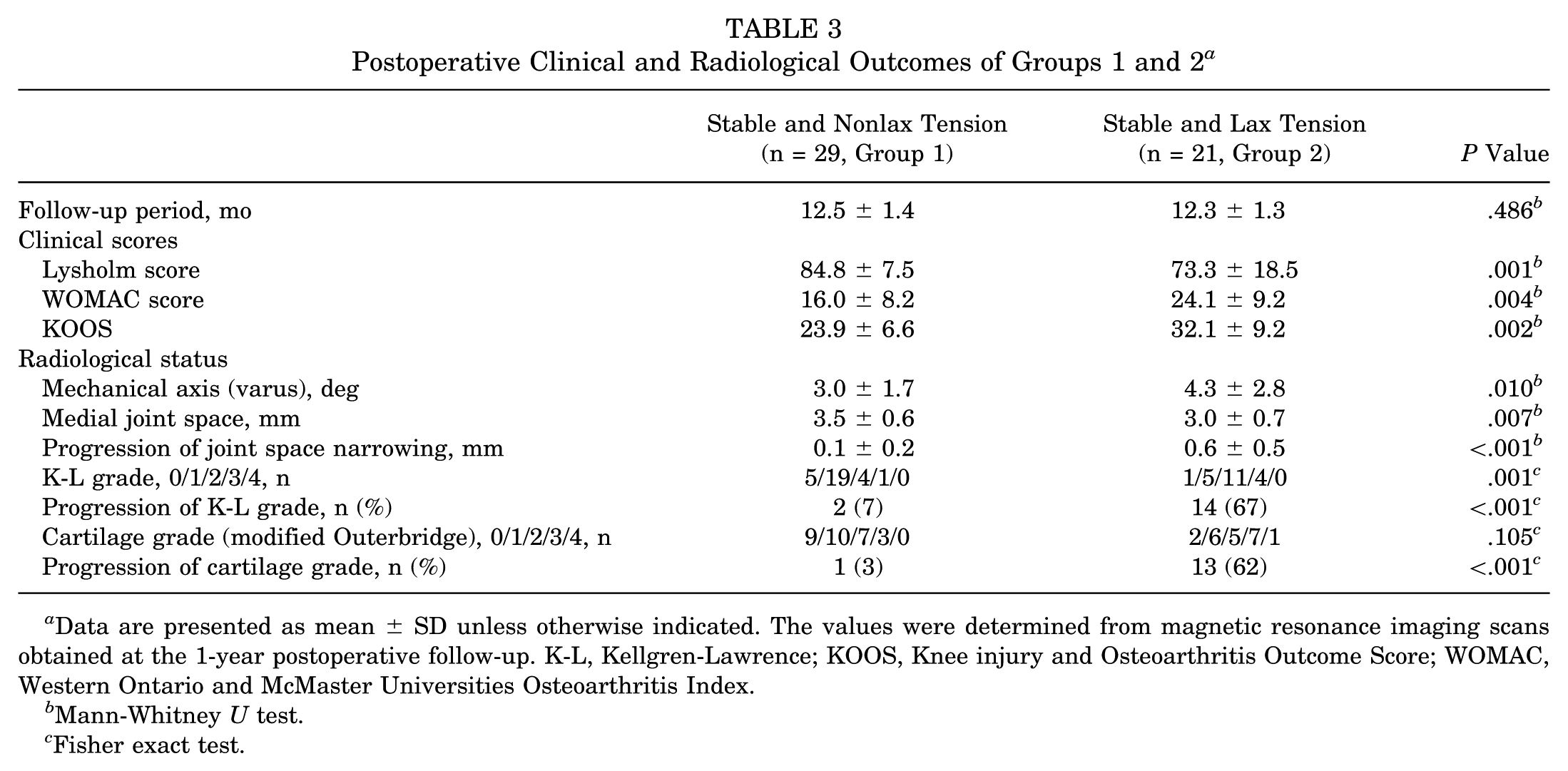
Data are presented as mean ± SD unless otherwise indicated. The values were determined from magnetic resonance imaging scans obtained at the 1-year postoperative follow-up. K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Mann-Whitney U test.
Fisher exact test.
Radiological Outcomes
Radiographic assessment revealed favorable outcomes in patients with stable healing (Table 2). When comparing nonlax versus lax tension, group 1 exhibited significantly less progression in K-L grade (7% in group 1 vs 67% in group 2) and medial joint space narrowing (0.1 ± 0.2 mm in group 1 vs 0.6 ± 0.5 mm in group 2) (P < .05) (Table 3).
Regarding the PTS, group 1 demonstrated a significantly lower PTS than group 2 on both the radiographic imaging–measured tibial slope (6.6°± 3.3° in group 1 vs 9.3°± 2.5° in group 2) and the MRI-measured medial slope (5.4°± 3.2° in group 1 vs 8.6°± 3.0° in group 2), whereas no significant difference was observed in the lateral slope (4.9°± 2.4° in group 1 vs 5.8°± 2.7° in group 2) (Table 4).
Postoperative Posterior Tibial Slope of Groups 1 and 2 a
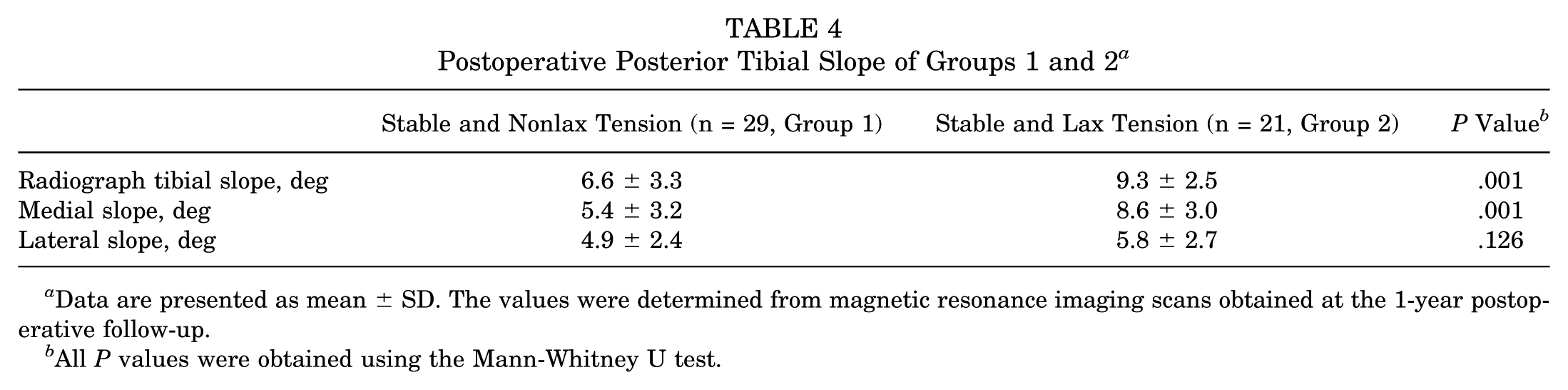
Data are presented as mean ± SD. The values were determined from magnetic resonance imaging scans obtained at the 1-year postoperative follow-up.
All P values were obtained using the Mann-Whitney U test.
The cutoff values for predicting lax tension were 8.3° for the radiographic imaging–measured tibial slope (P = .004) and 7.7° for the medial slope measured using MRI (P = .001). The AUC for PTS was 0.784 (95% CI, 0.652-0.916; P = .001), the AUC for MPTS was 0.788 (95% CI, 0.656-0.920; P = .001), and the AUC for LPTS was 0.627 (95% CI, 0.468-0.787; P = .128).
All ICCs ranged from 0.91 to 0.97, which indicated excellent reliability in this study.
Discussion
The most important finding of the study was that the PTS critically influenced meniscal healing, as confirmed by second-look arthroscopy after pull-out repair for MMPRTs. The lax healing group exhibited a significantly greater PTS and MPTS than the nonlax healing group. This finding suggests that a steeper PTS may interfere with proper meniscal healing, likely because of increased shear stress at the root repair site. The difference in healing quality, as directly visualized using second-look arthroscopy, underscores the biomechanical disadvantage conferred by excessive PTS. While patients with both lax and nonlax healing demonstrated significant clinical improvements after surgery, those in the nonlax group showed superior clinical and radiological outcomes at the final follow-up. These findings emphasize that the PTS is not only a morphological characteristic but also a key factor that can affect the function of the meniscus after root repair.
The healing status of the repaired meniscus root is critical because it directly influences postoperative meniscal extrusion and the progression of arthritis. MRI and second-look arthroscopy have been used to confirm healing status after root repair, although the evaluation criteria differ between these modalities. Although the healing outcomes reported in various studies vary, second-look arthroscopy remains a more reliable method for assessing healing because it directly evaluates the actual tension and attachment status of the repaired root. A systematic review reported that MRI indicated 69% complete healing, 28% partial healing, and 3% nonhealing postoperatively, whereas arthroscopic assessments showed 48% complete healing, 42% partial healing, and 10% nonhealing postoperatively. 16 Given that the primary goal of root repair is to restore meniscal hoop tension, second-look arthroscopy results, which provide direct visualization of the healing status, are considered more clinically relevant than MRI findings. In addition to evaluation, the selection of an appropriate surgical technique is important. Compared with simple sutures, complex suture patterns incorporating locking mechanisms generally demonstrate superior maximum failure loads. However, findings regarding reduced displacement during cyclic loading remain inconsistent. 15 While some studies report improved stability, others suggest that looped suture configurations can actually increase laxity; this phenomenon is often attributed to the bungee effect.6,23 Modified Mason-Allen repairs have shown decreased meniscal extrusion and favorable radiological outcomes. 24 An intact meniscus with nonlax tension observed on second-look arthroscopy indicates effective restoration of meniscal hoop tension. In medial meniscus root repair, surgeons should aim to achieve stable healing with minimal laxity; thus, robust surgical techniques and precise evaluation methods are crucial.
Radiographic progression of osteoarthritis differed substantially according to the healing status observed at second-look arthroscopy. Regarding radiographic outcomes, the nonlax group demonstrated superior joint preservation; only 2 knees (7%) in the nonlax group exhibited an increase in K-L grade, with minimal joint space narrowing of 0.1 mm. In contrast, the lax group showed significant structural deterioration, with 14 knees (67%) presenting K-L grade progression and significantly greater joint space narrowing (0.6 mm) during follow-up. Our findings corroborate recent reports indicating that nonlax healing is a prerequisite for joint preservation. Notably, knees with lax healing were found to undergo structural worsening despite improved clinical scores, whereas nonlax healing was associated with significantly less radiographic progression. Therefore, achieving a stable, nonlax repair should be the primary surgical objective to mitigate osteoarthritic deterioration.12,21,36
The PTS plays a critical role in knee biomechanics and stability. An increased PTS posteriorly displaces the tibiofemoral contact point, thereby elevating posterior stress on the tibial plateau.1,17 These biomechanical alterations exacerbate anteroposterior instability and may adversely affect the healing process in the posterior compartment. Therefore, when performing root repair in patients with an increased PTS, surgeons should consider adopting augmented strategies to optimize healing. Such measures may include the use of more robust suture materials or configurations, a more conservative rehabilitation protocol, or concomitant meniscotibial ligament repair.
The PTS influences numerous knee pathologies, with recent reports suggesting it as a contributing factor for meniscus root tears.14,19,29 In conjunction with greater varus alignment, narrower intercondylar distance, and reduced notch width, particularly multiple tibiofemoral anatomic features such as a steeper slope of the medial tibial plateau are associated with the occurrence of MMPRTs. 29 Additionally, several previous studies have reported that MPTS is implicated in degenerative meniscal injuries, with most indicating that increased MPTS elevates the risk of medial meniscus tears and MMPRTs.4,14,19 Conversely, the lateral tibial slope exerts minimal influence on MMPRT incidence; however, an increased LPTS correlates significantly with a heightened risk of lateral meniscus tears and lateral meniscus posterior root tears.14,19 In fact, the current study also found differences between the 2 groups regarding radiographic based PTS and MPTS; however, no difference was observed in LPTS.
Importantly, this study did not solely compare PTS values between groups but also aimed to identify the cutoff values of PTS associated with lax healing after root repair. According to our findings, a PTS of ≥8.3° or MPTS of ≥7.7° was associated with a significantly increased likelihood of lax healing. Therefore, in patients with PTS or MPTS values exceeding these thresholds, root repair may carry a higher risk of lax healing, potentially leading to unfavorable postoperative outcomes.
Limitations
This study has several limitations. First, owing to its retrospective and nonrandomized design, selection bias may have affected the inclusion of participants. Nevertheless, baseline descriptive and clinical data were prospectively collected from a registry. Second, the sample size was relatively small, in addition to the lack of a control or comparison group. Third, the follow-up duration was short, limiting the ability to evaluate the long-term effects of the healing status on arthritic progression. Nevertheless, stable healing with adequate tension is believed to play a key role in restoring meniscal hoop function after root repair. Fourth, follow-up MRI findings were not included because postoperative imaging could not be performed in all patients. Fifth, we acknowledge a partial overlap with our previously reported patient cohort. 13 However, a significantly expanded cohort (a 50% increase) addresses a distinct research question, justifying this work as an independent investigation rather than a redundant analysis. Sixth, the classification of lax versus nonlax healing was based on a qualitative arthroscopic assessment; no instrumented, quantitative measurements of tension were utilized. Seventh, all second-look evaluations were performed by a single experienced knee surgeon, and inter- or intraobserver reliability for this classification was not assessed. Eighth, root repair was performed using a single tibial tunnel technique, which may be associated with a higher failure rate compared with the double tibial tunnel technique. Ninth, while full weightbearing was delayed for 6 weeks, immediate toe-touch weightbearing for balance may have introduced minor loading, potentially leading to lax healing. Furthermore, biomechanical evidence suggests that the cinch-type sutures utilized herein may be susceptible to loosening under cyclic loading. This potential for construct elongation could be a contributing factor to the observed laxity.6,23 Tenth, patients who agreed to undergo second-look arthroscopy may differ from those who declined, which may introduce selection bias and limit the generalizability of the findings. Eleventh, we did not evaluate postoperative PTS. However, patients requiring high tibial osteotomy were excluded from this study, and isolated meniscus root repair is a soft tissue procedure that does not alter tibial bony architecture. Thus, postoperative PTS was assumed to remain consistent with preoperative values. Lastly, because this was a retrospective study, a priori power analysis was not performed and the sample size was based on available eligible patients; therefore, the possibility of limited statistical power for some comparisons should be considered.
Conclusion
An increased PTS may contribute to lax healing, which in turn progresses to meniscal extrusion after root repair. Consequently, when performing root repair in patients with an increased PTS, it can be anticipated that the postoperative healing and clinical outcomes may not be as favorable as those in patients without an increased PTS.
Footnotes
Acknowledgements
The authors thank all the patients for their time and commitment to the present study.
Submitted August 22, 2025; accepted April 7, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was obtained from Hanyang University Guri Hospital Institutional Review Board (2025-07-047-001).