
Abstract
Background:
Chronic proximal hamstring tendinopathy (PHT) can cause significant pain and functional impairment, particularly in active individuals. While nonoperative management is the first-line treatment, some patients with persistent symptoms may require surgical intervention.
Purpose:
To evaluate the functional outcomes, return-to-sport rates, and complication profiles of patients undergoing partial tenotomy and reinsertion for chronic PHT.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective cohort study targeted patients who underwent partial tenotomy and reattachment of the proximal hamstring tendons between April 2010 and September 2022. The indication for surgery was refractory chronic PHT symptoms for >6 months. The primary outcome measure was the Parisian Hamstring Avulsion Score (PHAS). Secondary outcomes included the Tegner Activity Scale score, University of California–Los Angeles (UCLA) Activity Scale score, return to sport, postoperative patient satisfaction, and the rate of complications. In this study, the terms “partial involvement” or “complete involvement” refer to the extent of magnetic resonance imaging signal changes across the tendon, rather than to true tendon ruptures or avulsions.
Results:
The study included 42 patients with a mean age of 50.4 years (SD, 10.4 years). The mean follow-up was 4.1 years (range, 2.0-12.6 years). The PHAS score significantly improved from a preoperative mean of 63.0 (SD, 11.4) to 84.2 (SD, 18.2) at the final follow-up (P < .001). The median Tegner Activity Scale score increased from 3.0 (IQR, 2.0-4.0) to 4.0 (IQR, 3.0-5.0) (P < .001), and the median UCLA score improved from 4.0 (IQR, 4.0-6.0) to 8.0 (IQR, 5.0-10.0) (P < .001). At the last follow-up, 30 of 39 patients (76.9%) returned to sport, with 18 of 39 (46.2%) achieving their preinjury sport level or higher. The median time to return to sport was 5.2 months (IQR, 3.7-6.3 months). Patient satisfaction was high, with 82.1% reporting satisfaction with the operated leg. The reattachment failure rate was 4.8%.
Conclusion:
Partial tenotomy and reattachment for chronic PHT result in significant functional recovery, a high return-to-sport rate, and good patient satisfaction.
Proximal hamstring tendinopathy (PHT) is an insertional tendinopathy resulting from repetitive microtrauma at the tendon's insertion on the ischial tuberosity.4,6,9,14,19,23 The cause of PHT is multifactorial, with intrinsic factors such as training errors (rapid increase in intensity or load) and static stretching, as well as systemic and extrinsic contributors, including age, BMI, genetic predisposition, pelvic tilt, and hormonal and metabolic dysfunctions.2,9,16,17 It usually manifests as persistent pain that is worsened by repetitive activity, stretching, or prolonged sitting.7,9,10 Diagnosis is primarily clinical, based on a detailed history and specific provocation tests such as the Puranen-Orava test, bent-knee stretch test, and modified bent-knee stretch test. 3 Magnetic resonance imaging (MRI) is the imaging modality of choice, showing increased signal intensity on T1-weighted sequences, tendon thickening, peritendinous edema, irregular tendon morphology, or neural irritation signs near the sciatic nerve.11,12,23
Current management strategies for PHT predominantly involve nonoperative approaches, including load management, eccentric strengthening exercises, extracorporeal shockwave therapy, corticosteroid injections, and platelet-rich plasma injections.4,6,7,9,14,18,19,23 Despite their widespread use, up to 20% of patients may fail to respond adequately to these treatments, experiencing persistent symptoms beyond 6 months, significantly impairing athletic performance and quality of life.9,14,15 The management of this subset of patients remains challenging, and consensus on surgical intervention is lacking. Furthermore, the literature on the surgical treatment of chronic PHT remains limited, with few robust studies available, often including mixed pathologies or acute injuries rather than isolated chronic tendinopathy.9,14,15
The objective of this study was to evaluate the functional outcomes, return-to-sport rates, satisfaction, and complication profile of patients with chronic PHT treated with partial tenotomy and reattachment.
We hypothesized that partial tenotomy-reattachment would result in significant improvements in function and activity scores, with a high rate of return to preinjury sport and acceptable complication rates.
Methods
Study Design and Setting
This retrospective cohort study was conducted at the sport surgery center in Paris and included patients operated on between April 2010 and September 2022. The study received approval from the institutional ethics committee, and all patients provided informed written consent before participation. Data belong to the Proximal Hamstring Avulsion Surgery Cohort Study (ClinicalTrials.gov; NCT02906865).
Eligibility Criteria
Patients were eligible if they were >18 years of age, with symptoms confirmed clinically and structural tendinopathic changes confirmed using MRI, and had failed at least 6 months of nonoperative treatment, including physical therapy, shockwave therapy, corticosteroid injections, or platelet-rich plasma. Patients were excluded if they had acute avulsions with tendon retraction, prior ipsilateral hip or hamstring surgery, associated lumbar or sciatic nerve pathology, or a minimum follow-up duration <2 years.
Definition of Tendinopathy and Surgical Indication
Chronic PHT was defined as persistent, deep, localized pain around the ischial tuberosity, typically aggravated by physical activities (eg, running, lunging, and squatting) or prolonged sitting. Clinical diagnosis was supported by MRI findings showing increased signal intensity on T1- and T2-weighted sequences at the tendon, 2 tendon thickening, peritendinous edema, and irregular tendon morphology without tendon retraction. 9 In this study, the terms “partial involvement” or “complete involvement” refer to the extent of MRI signal changes across the tendons (ie, signal limited to 1 or 2 tendons vs signal involving all 3 tendons) rather than to true tendon ruptures or avulsions. Surgical intervention was indicated in cases of functional impairment and failure of nonoperative treatment for 6 months in the presence of these MRI features.
Surgical Technique
All patients were operated on by the senior author (N.L.). Surgery was performed under spinal anesthesia, with patients placed in the prone position on a spine table to maintain hips at 20° and knees at 70° of flexion. A transverse incision was made inferior to the gluteal fold. The muscular fibers of the gluteus maximus were detached from their posterior aponeurosis and retracted laterally, exposing the ischial tuberosity.
The sciatic nerve was systematically identified lateral to the conjoint and semimembranosus tendons. In the presence of adhesions, gentle neurolysis was performed to ensure nerve mobilization. Macroscopically, the tendons appeared largely intact, although signs of peritendinous inflammation and subtuberosity defects could occasionally be palpated. Dissection was directed toward the posteroinferior border of the ischial tuberosity, beneath the insertion of the sacrotuberous ligament and in continuity with the origin of the conjoint and semimembranosus tendons. The posterior surface of the tendons was opened using a 5-mm scalpel incision parallel to the posteroinferior border of the ischial tuberosity, allowing a book-like opening of the conjoint and semimembranosus tendons. This exposure often revealed a subtuberosity detachment and interposed bursitis. Importantly, the anterior portion of the tendon insertion to the ischium was preserved to promote biological healing. The ischial footprint was debrided using a curette to decorticate the bone, and the detached tendon stumps were refreshed. Four 5.5-mm polyetheretherketone suture anchors were inserted into the ischial tuberosity. The tendons were reattached in situ via sequential suture passes using the anchor sutures. A second posterior layer of closure was performed by suturing the tendon aponeurosis to the distal portion of the sacrotuberous ligament using a continuous absorbable braided suture (size 2), thus closing the “book” configuration.
Layered closure was performed without drainage.
All patients received routine venous thromboembolism prophylaxis with low-molecular-weight heparin for 30 days in addition to early mobilization.
Postoperative Rehabilitation
Postoperative immobilization consisted of a hinged brace set at 30° of hip flexion for 3 weeks, then progressively reduced to 20° at week 4, 10° at week 5, and discontinued thereafter. This was followed by allowing progressive flexion. Partial weightbearing was permitted 24 to 48 hours after surgery with crutches. Isometric exercises of the quadriceps and hamstrings were initiated early, with the knee flexed 30°. After 6 weeks, active rehabilitation included dynamic closed-chain quadriceps exercises and active-assisted hamstring work. Between 12 and 16 weeks, patients began brisk walking or light jogging. Sport-specific reconditioning and progressive return to sport were allowed between 16 and 32 weeks postoperatively.
Outcome Measures
The primary outcome was the Parisian Hamstring Avulsion Score (PHAS) assessed at the last follow-up. 13 Secondary outcomes included the Tegner Activity Scale score, 20 University of California–Los Angeles (UCLA) Activity Scale score,1,22 patient satisfaction (dichotomous: yes/no), return to sport (rate, level compared to preinjury, and time to return), and rate of postoperative complications, including reattachment failure.
Data Collection
Data were collected prospectively using an online survey-based software system (Websurvey). The operating surgeon or clinical fellow entered all medical and surgical data, while patient-reported outcome measures and demographic information were completed directly by patients. Surveys were sent electronically at regular intervals after consultations, with automated email reminders issued multiple times. When patients did not respond electronically, they were contacted by telephone on 2 separate occasions to maximize follow-up. Postoperative outcomes were recorded at the last available follow-up, with a minimum duration of 2 years. Imaging reports were reviewed to confirm the diagnosis and injury characteristics.
Patient Selection and Flow
Among the 54 eligible patients, 2 declined participation and 10 were lost to follow-up. A total of 42 patients were included in the study. After excluding 2 cases of reattachment failure, 40 patients were included in the analysis evaluating functional outcomes and return to sport.
Statistical Analysis
Descriptive statistics are used for demographic and baseline clinical variables. Continuous data are reported as mean with standard deviation or median with interquartile range depending on the distribution assessed by the Shapiro-Wilk test. Paired comparisons between pre- and postoperative outcome scores were performed using the Wilcoxon signed-rank test. A P value <.05 was considered statistically significant. All statistical analyses were conducted using R software (Version 4.2; R Foundation for Statistical Computing).
Results
Patient Characteristics
A total of 42 patients (76.2% female; mean age, 50.4 years; SD, 10.4 years) were included in the study. Most patients (76.2%) had complete tendon ruptures involving all 3 tendons, with a mean follow-up of 4.1 years (range, 2.0-12.6 years) (Table 1).
Patient Characteristics (N = 42) a
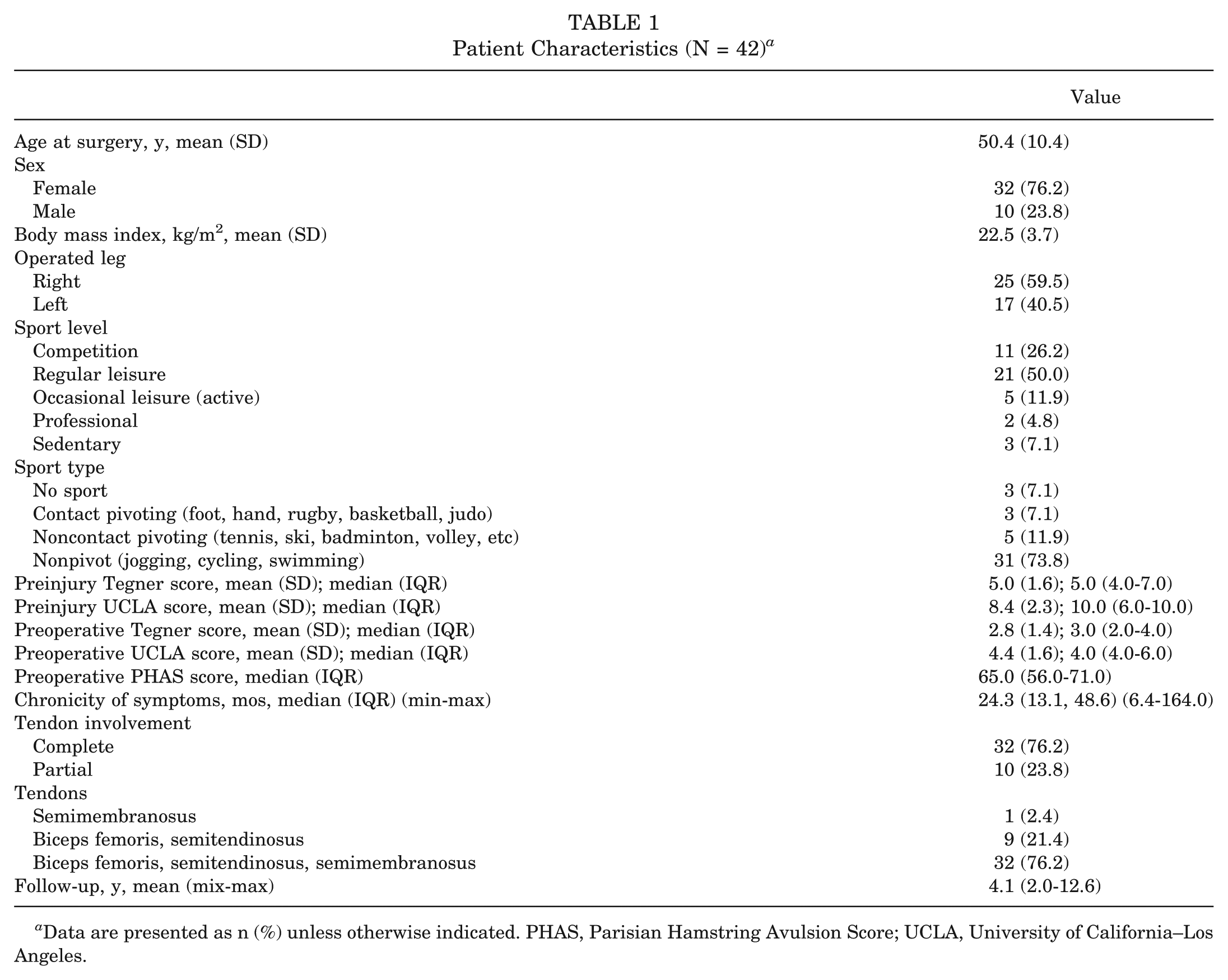
Data are presented as n (%) unless otherwise indicated. PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California–Los Angeles.
Primary Outcome: PHAS
At a mean follow-up of 4.0 years (range, 2.0-12.6 years), statistically significant improvements were observed in the entire cohort (N = 42). The PHAS score improved from a preoperative mean of 63.0 (SD, 11.4) to 84.2 (SD, 18.2) postoperatively (P < .001). When analyzing the subgroup of patients without reattachment failure (N = 40), the median PHAS score improved from 65.0 (IQR, 58.0-71.0) to 92.8 (IQR, 74.5-97.0) (P < .001) (Table 2).
Preoperative and Last Follow-up Score Comparison a
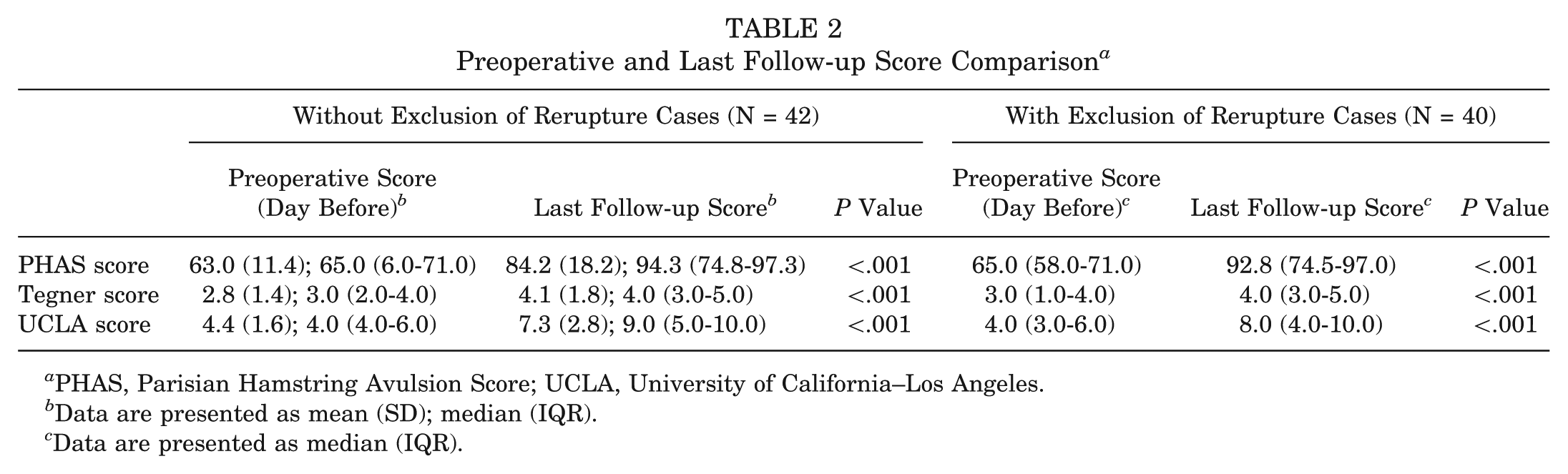
PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California–Los Angeles.
Data are presented as mean (SD); median (IQR).
Data are presented as median (IQR).
Secondary Outcomes
Significant postoperative improvements were also observed in both Tegner and UCLA activity scores. The median Tegner score increased from 3.0 (IQR, 1.0-4.0) preoperatively to 4.0 (IQR, 3.0-5.0; P < .001), and the median UCLA score improved from 4.0 (IQR, 4.0-6.0) to 8.0 (IQR, 5.0-10.0; P < .001). Detailed comparisons for the subgroup without reattachment failure (N = 40) are provided in Table 2.
At the last follow-up, 30 of 39 patients (76.9%) returned to sport, with 18 of 39 (46.2%) achieving their preinjury sport level or higher. The median time to return to sport was 5.2 months (IQR, 3.7-6.3 months). Patient satisfaction was high, with 82.1% reporting satisfaction with the surgical outcome (Table 3).
Functional Results and Return to Sport at Last Follow-up a
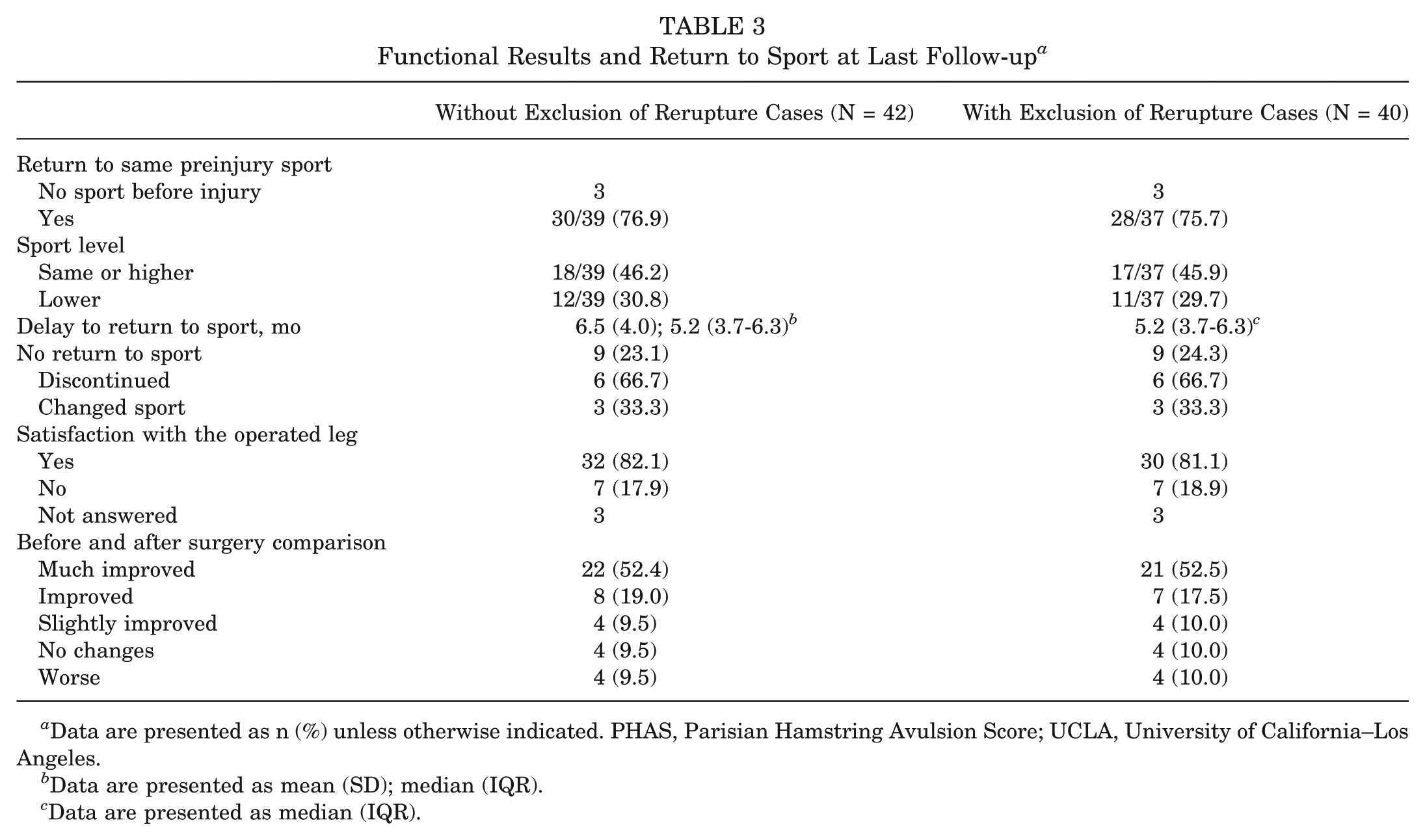
Data are presented as n (%) unless otherwise indicated. PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California–Los Angeles.
Data are presented as mean (SD); median (IQR).
Data are presented as median (IQR).
Complications
Complications were uncommon, with only 2 cases (4.7%) of tendon reattachment failure; no infections, nerve injuries, or thromboembolic events were observed. Both reattachment failures occurred during the first postoperative month, secondary to an accidental fall during early rehabilitation. In both cases, MRI confirmed loss of continuity at the reattachment site, and revision surgery with reattachment using new suture anchors was successfully performed. The outcomes of these revisions are outlined in Table 4. Both patients achieved excellent functional outcomes at 3 and 8 years of follow-up, respectively. Patient 1 reported a PHAS score of 94.5, UCLA score of 10, and Tegner score of 5, returning to sport at a lower level after 16.6 months. Patient 2 reported a PHAS score of 100, UCLA score of 10, and Tegner score of 6, returning to the same preinjury sport level after 11.2 months. Both patients reported satisfaction with the revision surgery.
Outcomes of Revision Surgery Cases a
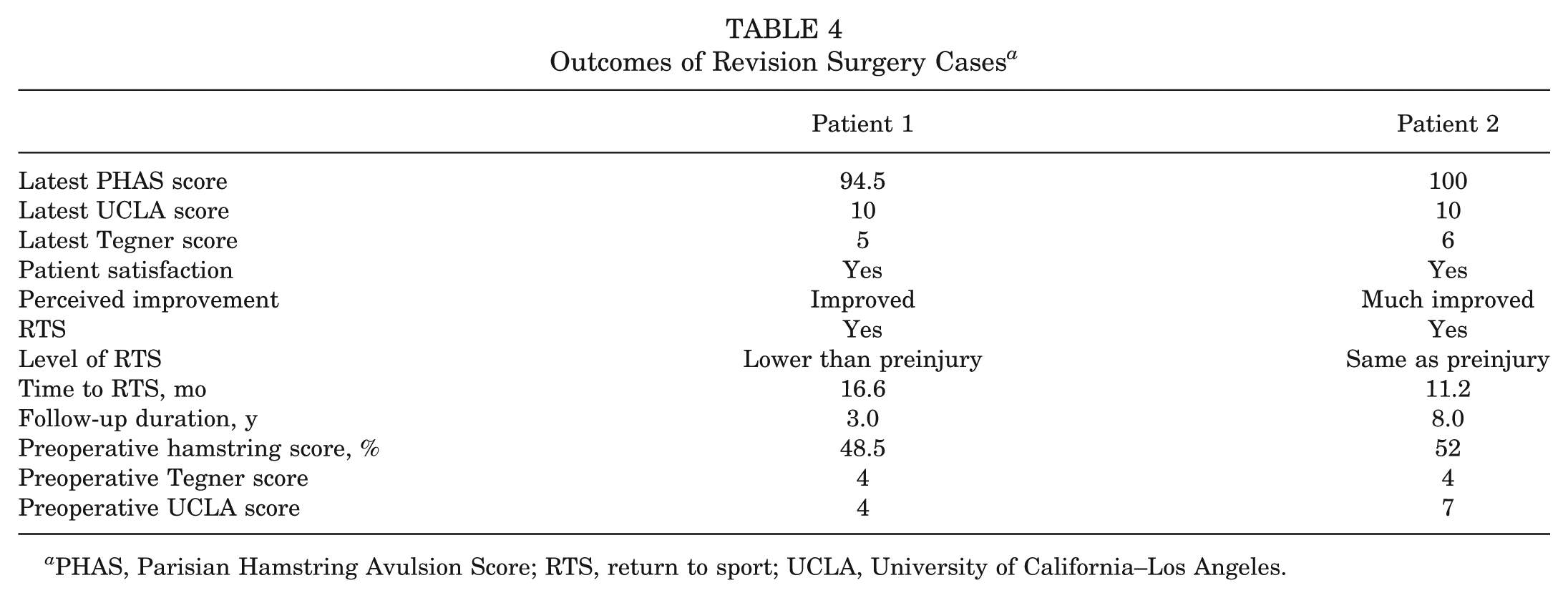
PHAS, Parisian Hamstring Avulsion Score; RTS, return to sport; UCLA, University of California–Los Angeles.
Discussion
The main finding of this study was that partial tenotomy and reattachment of the PHT resulted in significant functional improvement and a high return-to-sport rate in patients with chronic PHT unresponsive to nonoperative treatment.
Postoperative improvements in patient-reported outcome measures were substantial. The mean PHAS score increased significantly from 63.0 (SD, 11.4) preoperatively to 84.2 (SD, 18.2) at the final follow-up (P < .001). This magnitude of improvement is consistent with other surgical series despite the heterogeneity of scoring systems used. For instance, Costa et al 5 reported a single case with a VISA-H score increase from 23 to 100 after conjoint tendon reinsertion and semimembranosus tenotomy. Fitzpatrick et al 8 conducted a retrospective study evaluating outcomes of 8 patients (9 hips) with chronic PHT treated surgically by debridement and suture anchor repair without sciatic nerve decompression. At a mean follow-up of 6.7 years, patients reported excellent pain relief, with mean numeric pain scores of 0.6 at rest and 4.0 during activity. Functional outcomes were favorable, with a mean Lower Extremity Functional Scale score of 81.1 and Single Assessment Numeric Evaluation score of 74.9.
In our cohort, 76.9% of patients returned to sport at a median of 5.2 months, and 46.2% resumed at their preinjury level or higher. These findings are in line with the most robust series in the literature.2,15 Lempainen et al 15 reported on 103 surgical cases, primarily among competitive athletes, and found that 89% returned to their previous sporting level, with a mean time to return of 5 months (range, 2-12 months). Their technique included semimembranosus tenotomy with tendon reattachment and systematic sciatic nerve exploration and neurolysis. 15 Similarly, Benazzo et al 2 analyzed 17 high-level athletes and observed a 100% return to sport, with 88% rated as having excellent outcomes. They found a faster mean return-to-sport time of 4.4 months. Our return-to-sport data support these findings and reinforce the clinical value of surgical treatment, particularly in athletic populations in which recovery of preinjury performance is critical.
There is notable variability in surgical techniques described in the literature for chronic PHT, reflecting differing philosophies on tendon load redistribution, neural involvement, and fixation. Lempainen et al 15 advocated for semimembranosus tenotomy with reattachment to the biceps femoris, rather than to bone, with the goal of offloading the diseased tendon—based on the observation that semimembranosus injuries often demonstrate delayed recovery. Costa et al 5 proposed a modification of the Lempainen technique by performing debridement of the conjoint tendon and direct reinsertion into the ischial tuberosity using suture anchors, combining anatomic fixation with neural decompression. However, their technique was not supported by a published cohort. 5 Benazzo et al 2 used partial tenotomy or multiple punctures of the fibrotic tendon to reduce tension, along with sciatic neurolysis extending up to 10 cm distal to the ischial tuberosity and myotendinous relaxation. In contrast, Fitzpatrick et al 8 described suture anchor repair without sciatic nerve exploration, focusing on structural tendon reattachment. These differing strategies underscore the ongoing debate regarding the relative importance of mechanical, neural, and biological factors in the management of chronic PHT. Our technique, partial tenotomy and reattachment, is not unique in itself but integrates principles from previously described procedures, including semimembranosus tenotomy, partial tenotomy, tendon debridement, and suture anchor repair. Unlike isolated semimembranosus tenotomy, our approach preserves the anterior insertion and systematically reattaches the tendon complex to the ischial tuberosity.
Previous imaging studies have suggested that the semimembranosus tendon is most frequently involved in PHT, even in asymptomatic populations. 21 However, our series differs in that it included only surgically treated patients with refractory symptoms, which may represent a distinct subgroup. In this context, we observed a predominance of conjoint tendon involvement. On the other hand, our study defined partial and complete involvement as the extent of MRI signal abnormalities (1 or 2 tendons vs all 3 tendons) rather than true acute ruptures or retracted avulsions. This ensured that the spectrum we studied corresponds to chronic tendinopathy with or without widespread involvement, which differs from acute avulsion injuries.
In the current series, complications were limited to 2 cases (4.7%) of reattachment failure, with no wound problems, infections, nerve dysfunction, or sensory disturbances. Reported complication rates in the literature include wound issues and transient sciatic symptoms in 2% to 7% of cases, occasional paresthesia related to nerve handling, and potential neural irritation acknowledged with posterior approaches.2,8,15
This study is further strengthened by its exclusive focus on isolated chronic tendinopathy cases, excluding acute avulsions or partial tears, and by the use of validated outcome measures. However, limitations include its retrospective type of analysis, lack of a comparative nonoperative cohort, and limited subgroup analysis due to sample size. The sample size, although among the largest reported series on surgical treatment of chronic PHT, corresponds to a relatively low number of cases per year over a 12-year period. Furthermore, all procedures were performed by a single experienced surgeon, which ensures technical consistency but may limit generalizability, as outcomes could differ in other surgical settings.
Conclusion
Partial tenotomy and reattachment of the proximal hamstring tendons offers a safe and effective treatment option for patients with chronic PHT refractory to nonoperative management. This approach leads to significant improvements in functional outcomes, a high rate of return to sport, and excellent patient satisfaction, with a low complication profile.
Footnotes
Submitted October 14, 2025; accepted April 30, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. is a consultant for Websurvey Society. A.H. is a consultant for Arthrex and DePuy.for Arthrex and DePuy.
Ethical approval was obtained from University Hospital Pitié Salpétrière.
Data Accessibility Statement
Data are available on reasonable request.