
Abstract
Background:
Posterior shoulder dislocations are rare but particularly challenging in high-demand populations. While anterior instability has been well studied, limited data exist on the morphological consequences of traumatic first-time and recurrent posterior dislocations.
Purpose:
To quantify posterior glenoid bone loss (pGBL), glenoid version, reverse Hill-Sachs lesions, and acromial morphology in patients with traumatic posterior shoulder dislocations and compare these features between the single and recurrent dislocation groups.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review was conducted using the Military Health System Data Repository to identify patients who sustained traumatic posterior shoulder dislocations between January 2017 and December 2024. These were defined as events requiring manual reduction with subsequent advanced imaging demonstrating a posterior labral tear or posterior bony Bankart lesion, with or without a reverse Hill-Sachs lesion. Morphological features were independently assessed by 2 raters. Measured factors included pGBL (measured by the perfect circle technique (PCT), two-thirds glenoid height methods, and one-third glenoid height method), glenoid version, reverse Hill-Sachs Lesion parameters, and acromial tilt and height. Patients were stratified into single and recurrent dislocation groups. Statistical comparisons were performed using t tests, with significance set at a P value < .05. Linear regression was used to evaluate the relationship between number of dislocations and extent of pGBL.
Results:
A total of 39 shoulders sustained posterior dislocation events with adequate imaging. Patients with multiple dislocations (vs a single dislocation) demonstrated significantly greater mean pGBL across all 3 measurement techniques: PCT (12.4% vs 10.5%; P = .031), two-thirds glenoid height method (13.7% vs 11.5%; P = .021), and one-third glenoid height method with sex-specific adjustments (13.0% vs 10.7%; P = .009). Glenoid retroversion was not significantly greater in the recurrent dislocation group (−11.0° vs −8.0°; P = .252). No significant differences were observed in reverse Hill-Sachs lesion dimensions or acromial morphology between groups. A weak positive correlation was found between the number of dislocations and pGBL (R2 = 0.054).
Conclusion:
After first-time traumatic posterior dislocation, the mean pGBL was approximately 11%. Bone loss increased with recurrent dislocations, approaching thresholds associated with failure after isolated posterior soft tissue stabilization. No association was found with reverse Hill-Sachs lesion size. Early recognition and intervention, particularly in high-demand populations at risk of recurrent dislocation, may be appropriate to prevent pGBL progression.
Posterior shoulder dislocations are uncommon, constituting <4% of all shoulder dislocations, 21 yet they pose unique treatment challenges in high-demand populations such as active-duty servicemembers. While anterior shoulder dislocations and posterior shoulder subluxations have been extensively studied in terms of both pathoanatomy and morphological characteristics,18,21 there is a notable gap in the literature addressing the structural changes resulting from a posterior shoulder dislocation.
Prior literature has emphasized the significance of osseous morphology in contributing to posterior shoulder instability.6,8,18 Key variables of interest include posterior glenoid bone loss (pGBL), increased glenoid retroversion, reverse Hill-Sachs lesions, and variations in acromial morphology, and all variables have been implicated in recurrent posterior instability and treatment failure. 8 Glenoid bone loss (GBL) has been reported in up to 81% of patients with posterior instability, 6 and in some reports nearly 22% of patients with posterior instability had pGBL ≥13.5%. 8 These structural deficits have been associated with an increased risk of failure after both nonoperative and operative management in younger, high-demand populations. 12
Glenoid version also plays a critical role, with increased retroversion predisposing to posterior subluxation and dislocation. 18 Similarly, decreased posterior acromial tilt and coverage and increased posterior acromial height have been independently associated with increased posterior glenohumeral instability.11,15 A comprehensive understanding of these morphological characteristics is key for accurate diagnosis, effective surgical intervention, and prevention of recurrent instability.
The primary aim of this study was to quantify pGBL, glenoid version, and acromial morphology in patients with traumatic posterior shoulder dislocations, and to compare these characteristics between the primary and recurrent posterior dislocation groups. We hypothesized that each subsequent posterior dislocation event would lead to a greater amount of pGBL.
Methods
After approval by the institutional review board, the Military Health System Data Repository was queried for all patients who sustained a posterior shoulder dislocation (International Classification of Diseases 10th Revision, codes S43.024A, S43.025A, S43.026A, S43.024D, S43.025D, and S43.026D) requiring manual reduction (Current Procedural Terminology codes 23650 and 23655) between January 2017 and December 2024 across all military treatment facilities. Patients were included if they had at least 1 traumatic posterior shoulder dislocation, with subsequent advanced imaging (2-dimensional [2D] computed tomography [CT] or 2D magnetic resonance imaging [MRI] studies of the affected shoulder). Both 2D CT and 2D MRI scans were utilized for measurement depending on availability, and the mean slice thickness was 2 mm for CT and 3 mm for MRI. Patients were excluded for posterior shoulder dislocations that occurred in the absence of a discrete traumatic event resulting in significant external force. Chart review was performed to document the number and dates of shoulder dislocation events. In cases in which the exact number of episodes was not described quantitatively (ie, “multiple” or “several”), patients were categorized as having ≥2 dislocations and were included in the recurrent group. Because of the variability in documentation, detailed quantification of total dislocation episodes was not performed.
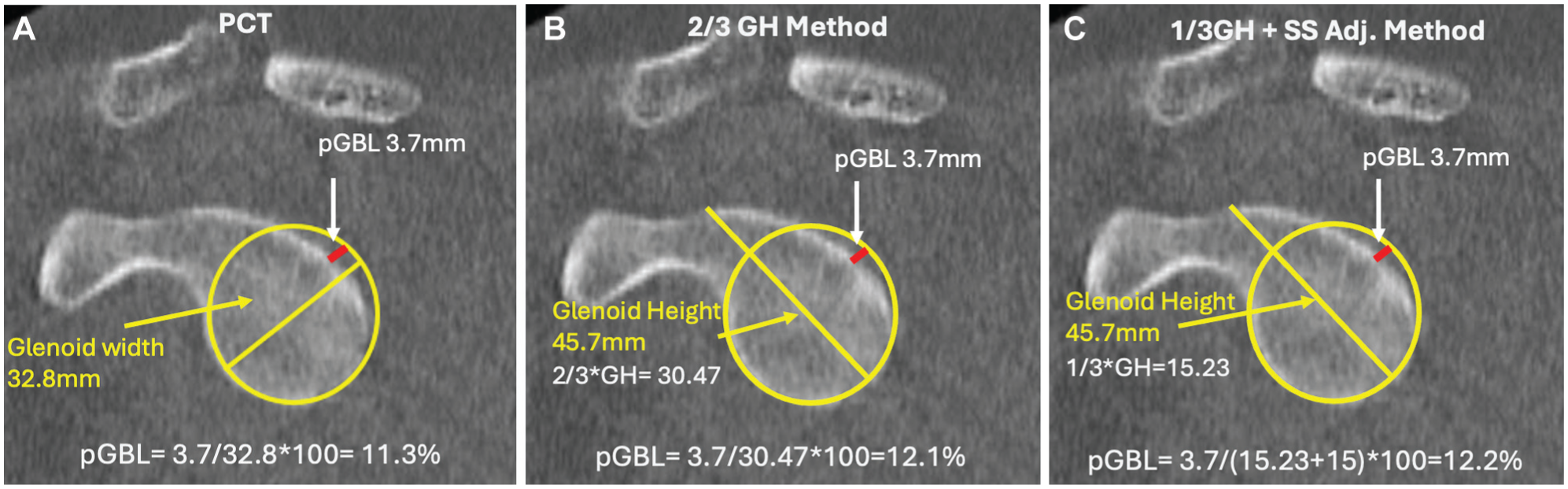
Two orthopaedic surgery residents (H.P.G, A.M.M.) independently assessed CT and MRI scans to quantify the following morphological characteristics: pGBL, reverse Hill-Sachs lesions, glenoid version, and posterior acromial tilt and height. Posterior GBL was measured using 3 previously described techniques: the perfect circle technique (PCT), two-thirds glenoid height method (2/3GH), 13 and one-third glenoid height method (1/3GH) with sex-specific adjustments (13 mm for females, 15 mm for males) 17 (Figure 1). Given that there is no universally accepted gold standard for quantifying pGBL, a multimethod approach was utilized to improve measurement strength and allow comparison across techniques. GBL was measured at the level of the coracoid. Glenoid version (Figure 2) and posterior acromial coverage and height (Figure 3) measurements were done in accordance to previous studies.4,15 Glenoid retroversion was assigned using negative values. The surface area and distance from the medial border of a reverse Hill-Sachs lesion to the subscapularis insertion were recorded (Figure 4). Preinjury imaging was not available for included patients; therefore, measurements of pGBL reflect osseous morphology at the time of imaging and cannot distinguish between acquired bone loss and preexisting glenoid dysplasia.
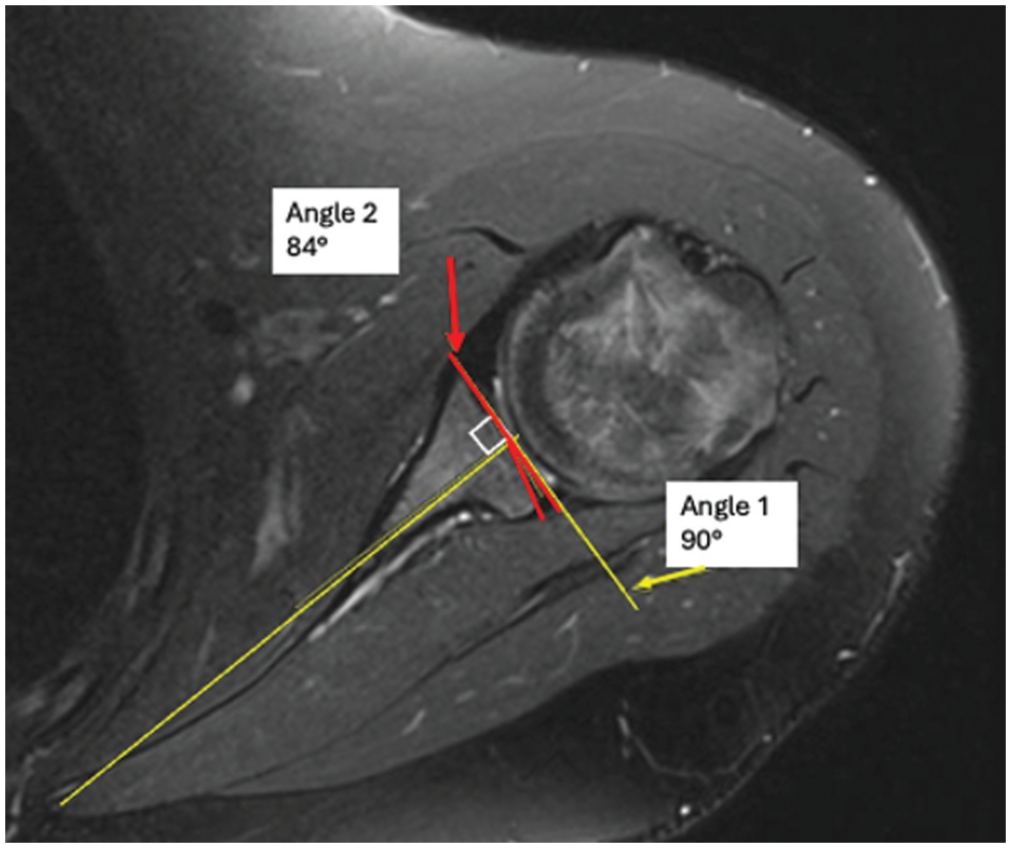
Glenoid version measured according to technique of Friedman et al. 4
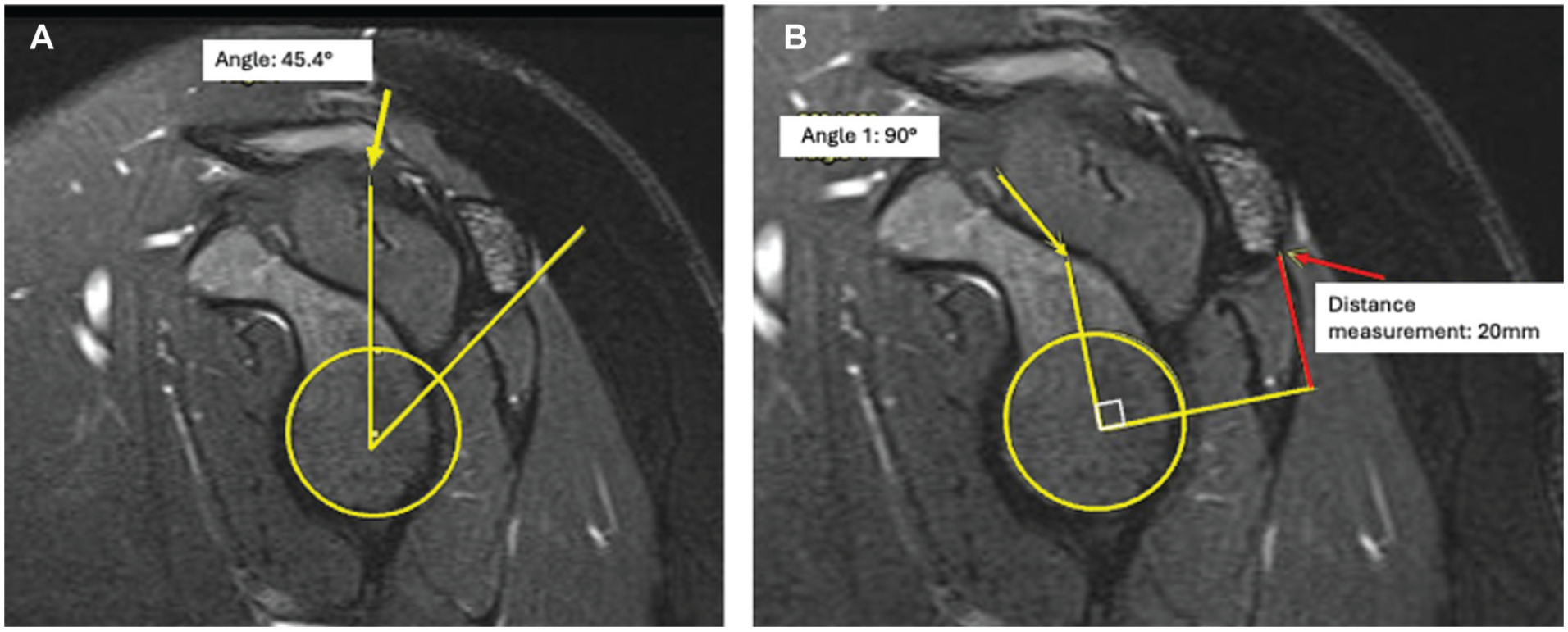
(A) Posterior acromial coverage and (B) posterior acromial height measured according to the techniques of Meyers et al. 15
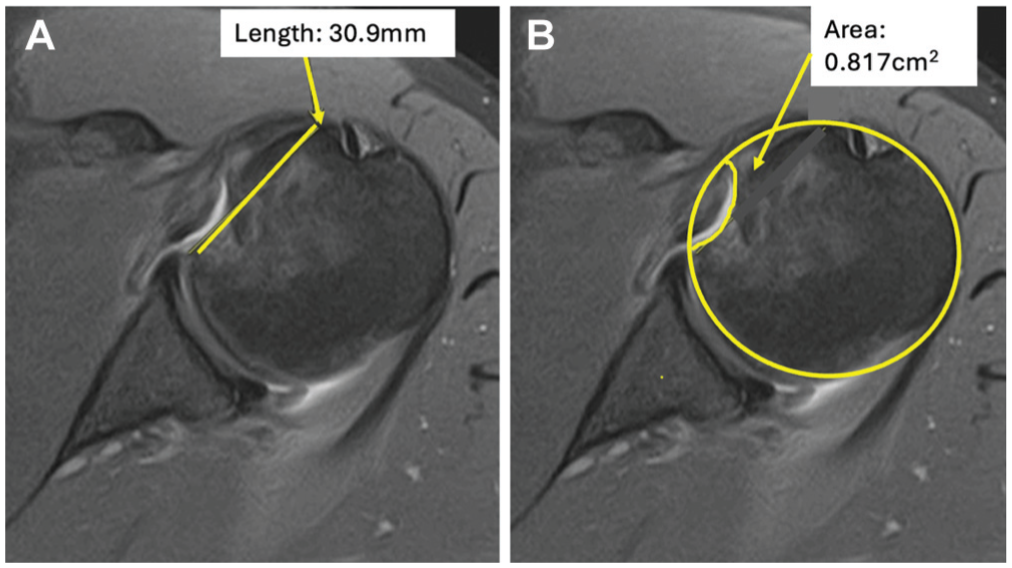
Reverse Hill-Sachs measurements: (A) distance from reverse Hill-Sachs lesion to medial extent of the subscapularis insertion and (B) reverse Hill-Sachs lesion surface area.
All statistical analyses were performed using IBM SPSS Statistics (Version 30.0; IBM). Patients were categorized into 2 groups (single dislocation and recurrent dislocations), and means were assessed using an independent-samples t test for each morphological variable. A 2-tailed P value <.05 was considered statistically significant. A linear regression analysis was performed to determine the relationship between the number of posterior dislocations and the extent of pGBL. Intra- and interrater reliability were calculated using intraclass correlation coefficients (ICCs). Reliability was rated as fair (0.4-0.6), good (>0.6-0.8), or excellent (>0.8). After ICCs were calculated and reliability between reviewers was found to be excellent (>0.8), the senior resident’s (H.P.G.) measurements were used for statistical analysis.
Results
A total of 39 shoulders met inclusion criteria. Seven patients had CT scans, 16 patients had MRI scans, and 14 had both CT and MRI scans available for review. In total, 21 CT scans and 30 MRI scans were analyzed for morphological characteristics. All measurements were performed using 2D imaging. The mean age of patients who sustained a single dislocation was 32.7 ± 9.2 years, and the mean age of those with recurrent dislocations was 26.4 ± 8.9 years (Table 1). All 14 (100%) patients with single dislocations were active-duty servicemembers. For the recurrent dislocation group, 22 of 25 (88%) were active-duty servicemembers and 3 of 25 (12%) were dependents. The mechanisms of injury for those with single dislocations were fall (9/14; 64%), seizure (2/14; 14%), military combat training (2/14; 14%), and motorcycle accident (1/14; 7%). The mechanisms of injury for those with recurrent dislocations were falls (9/25; 36%), combat military training (6/25; 24%), seizures (5/25; 20%), sports (4/25; 16%), and motorcycle accident (1/25; 4%). The mean follow-up time in months was 51.8 ± 36.0 months for the single dislocation group and 44.1 ± 29.9 months for the recurrent dislocation group (P = .238).
Descriptive Characteristics for Those With Single Versus Recurrent Dislocations a
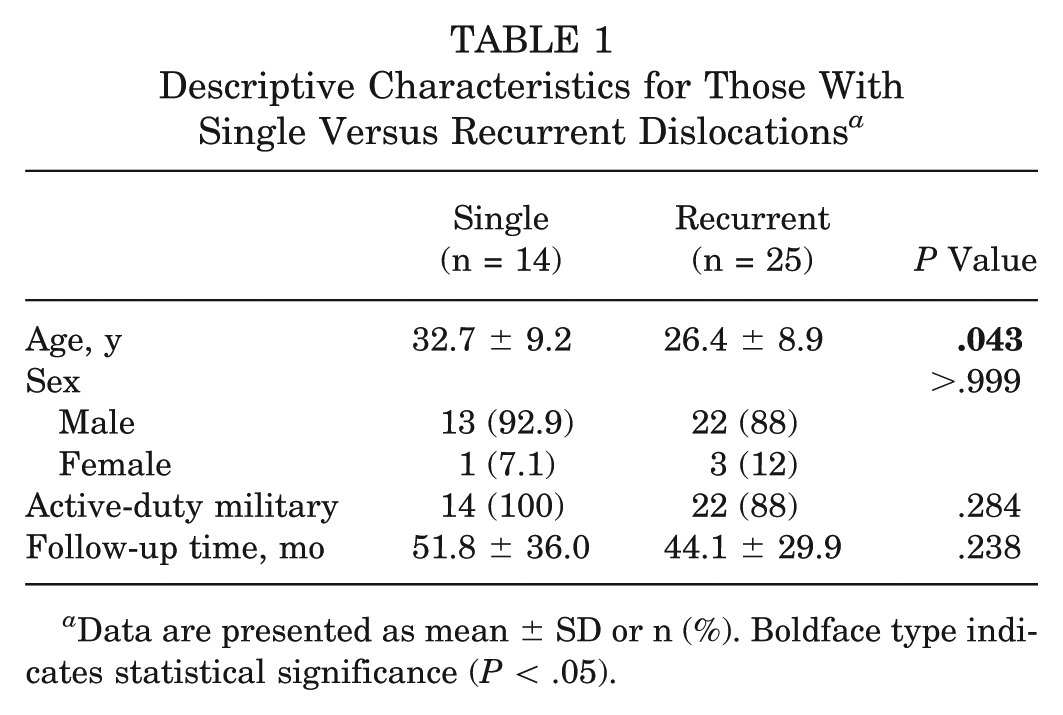
Data are presented as mean ± SD or n (%). Boldface type indicates statistical significance (P < .05).
The mean pGBLs for the single dislocation group were 10.5% (PCT), 11.5% (2/3GH), and 10.7% (1/3GH). For the recurrent dislocation group, the mean GBLs were 12.4% (PCT), 13.7% (2/3GH), and 13.0% (1/3GH) at the most recent MRI/CT evaluation. The recurrent dislocation group demonstrated significantly greater bone loss across all measurement methods (P < .05). No other morphological characteristics were significantly different between groups (Table 2). A regression analysis demonstrated that additional shoulder dislocations were associated with a small, nonsignificant increase in pGBL of 0.29% (β = 0.233; P = .093). However, with an R2 value of only 5.4%, the overall variability in pGBL is primarily driven by factors other than dislocation frequency.
Morphological Variables for Those With Single Versus Recurrent Shoulder Dislocations a
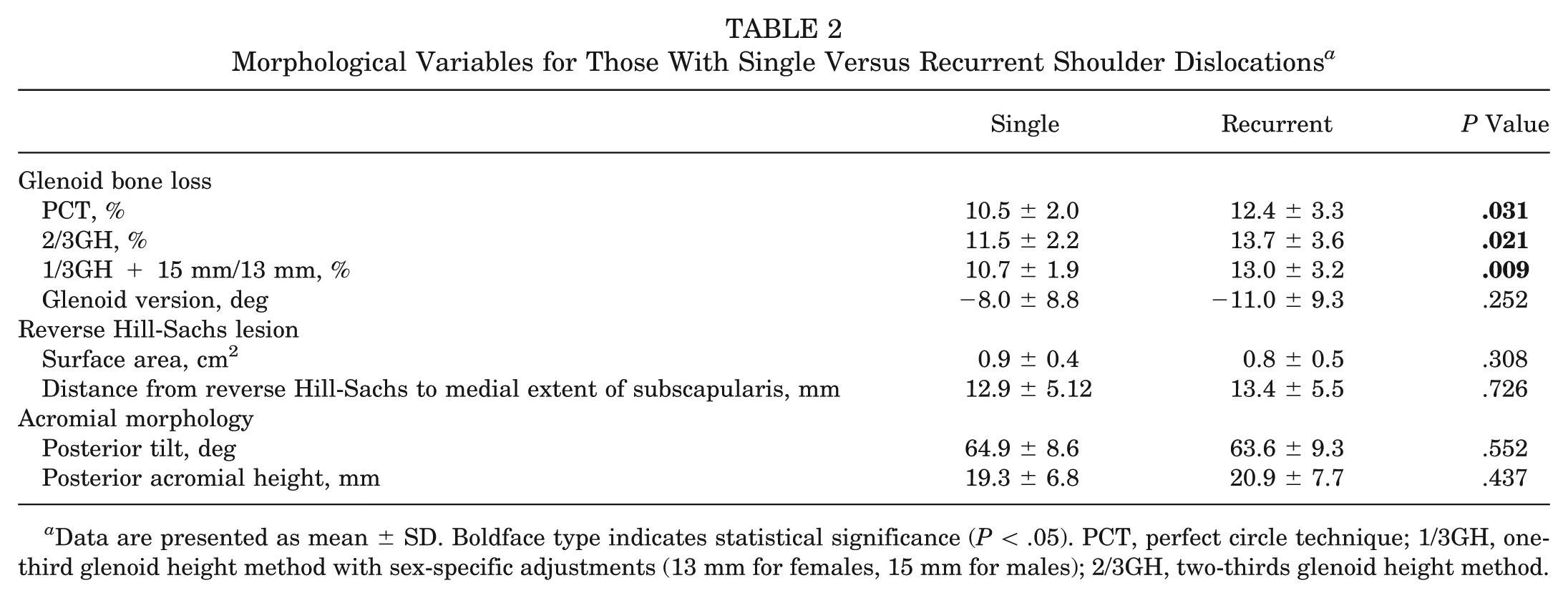
Data are presented as mean ± SD. Boldface type indicates statistical significance (P < .05). PCT, perfect circle technique; 1/3GH, one-third glenoid height method with sex-specific adjustments (13 mm for females, 15 mm for males); 2/3GH, two-thirds glenoid height method.
Discussion
The most important finding of this study is that recurrent posterior shoulder dislocations are associated with significantly increased pGBL, with mean values exceeding previously described critical thresholds associated with failure after isolated posterior soft tissue stabilization.1,6,15,18 Although the absolute difference in pGBL between groups was approximately 2%, its clinical significance should be interpreted in the context of established critical thresholds. Prior literature has identified 11% to 15% pGBL as a threshold associated with failure of isolated soft tissue stabilization1,5,12,16; thus, even small increases may be clinically meaningful as they shift patients beyond this range.
Posterior shoulder instability remains a challenging entity to treat, as the presentation may be subtle and include more nonspecific symptoms. As a result, posterior shoulder instability may be unrecognized or misdiagnosed, leading to delay in proper treatment. 19 Additionally, the underlying risk factors are not well delineated or understood, further complicating management.
Previous literature has referenced several morphological characteristics that may contribute to posterior instability events, such as glenoid version, GBL, and acromial morphology. Owens et al 18 demonstrated that increased glenoid retroversion significantly predisposed patients to posterior instability. Similarly, Gottschalk et al 5 reported that patients with posterior instability have a significant increase in retroversion, and those with >16° of retroversion were significantly more likely to experience a contralateral injury. In a more recent study, Livesey et al 11 found patients with posterior instability can exhibit altered acromial morphology and decreased posterior coverage. As a result, this may decrease posterior humeral head coverage and increase the risk of posterior instability, although this was not a significant finding in our cohort of patients. The difference in our results may be attributed to differing patient populations. Livesey et al 11 included subluxation and dislocation events, while our study only included traumatic posterior dislocations confirmed on imaging that required manual reduction, which may have occurred due to the mechanism of injury regardless of small variations in posterior coverage. Additionally, the Livesey et al 11 study used MRI exclusively, while we incorporated MRI and CT, which may have introduced heterogeneity in our measurements.
The aim of our study was to quantify pGBL, glenoid version, reverse Hill-Sachs lesions and acromial morphology in patients with traumatic posterior shoulder dislocations. Our hypothesis that recurrent posterior shoulder dislocation would result in further pGBL was confirmed in our study. Our results also demonstrated a higher percentage of bone loss with recurrent dislocations, compared to a single dislocation. Given that there have been several previously conducted studies that demonstrate meaningful bone loss with single-event dislocations,1,16 our findings further support the importance of assessing bone loss with advanced imaging, even after first-time dislocation events.8,19 These findings become increasingly relevant in active, high-performing servicemembers that are at a higher risk of experiencing recurrent shoulder instability. 21 Previous literature 8 pertaining to a military population who had undergone arthroscopic isolated stabilization of the posterior labrum reported that 69% had some degree of pGBL. Although this study 8 reported a 90% rate of return to duty, those with critical bone loss were statistically less likely to return to full duty. 8 This further emphasizes the importance of identifying pGBL and addressing it properly to optimize outcomes.
Several techniques have been described to quantify GBL, most of which were originally developed and validated in the setting of anterior shoulder instability and subsequently adapted for use in pGBL. As a result, each method carries inherent advantages and limitations when applied to posterior instability. The PCT is one of the most widely utilized methods and allows for comparison with prior literature. However, as it was developed in the setting of anterior instability, its application to pGBL may be limited and can result in overestimation when the posterior rim is deficient. The 2/3GH method has been shown to improve reliability using a linear measurement based on preserved glenoid height, reducing dependence on anterior rim morphology. Similarly, the 1/3GH method incorporates an anatomic reference that may better approximate native glenoid dimensions, although it assumes consistent proportional relationships that may vary between individuals. In the absence of a gold standard for measuring pGBL, we utilized all 3 techniques. The consistency of increased pGBL in those with recurrent dislocations across all methods, as well as excellent interrater reliability observed across all measurement techniques (ICC > 0.8), supports the strength of our findings despite the known limitations of each individual technique. Our results suggest that these common measurement techniques (PCT, 2/3GH, and 1/3GH) can be applied with high reproducibility in the posterior setting. This is clinically relevant, as accurate and reliable quantification of pGBL is essential for surgical decision-making.
The correlation coefficient (β = 0.233) and the small proportion of variance (R2 = 0.054) reveal that dislocation frequency alone is not a strong determinant of bone loss severity. Hence, this suggests that the remaining variance could be due to other factors that were unaccounted for, such as injury mechanism, quality of tissue, patient age, or other comorbidities. Green et al 6 looked at risk factors for GBL in the setting of posterior glenohumeral instability addressed with primary arthroscopic shoulder stabilization and found that athletic status and dominant arm involvement were independent risk factors for bone loss >13.5%. These findings attests to the complexity of this diagnosis and warrants further investigation to identify additional variables that are predictive of posterior dislocations and risk factors that increase the rate of pGBL.
The remaining variables in our study, to include glenoid version, reverse Hill-Sachs lesion size, and acromial tilt and height, did not yield statistically significant results, which suggests that, acknowledging type 2 error risk in this small series, these factors may not play a strong role in progression to recurrent posterior shoulder dislocation. However, prior literature has revealed a trend that increasing glenoid retroversion >10° may be a predisposing factor to posterior instability. 18 In the current study, mean glenoid retroversion was –8.0°± 8.8° in patients with a single traumatic posterior dislocation and –11.0°± 9.3° in those with recurrent dislocations, not significantly different. Owens et al 18 reported a significant 17% increased risk of posterior instability with each 1° increase in retroversion. The difference in these findings is likely due to the types of posterior instability studied, as more subtle anatomic changes may be more likely to allow for subluxation posterior instability events than the more uncommon and traumatic frank dislocations examined in this series.
Our study exhibits several strengths. We utilized multiple validated measurements when measuring pGBL, all of which were manually calculated by 2 independent raters with excellent interrater reliability. Additionally, the Military Health System allows for long-term imaging surveillance, as these events can be identified and imaging can be accessed, even if a patient relocates to a new duty station.
There are also various limitations to this study. The retrospective nature of the study and the use of administrative coding to identify patients predispose data to selection bias; furthermore, the study is limited by the extent and detail of the information included in the medical record. However, this was mitigated through detailed chart review to confirm inclusion criteria, traumatic mechanism, reduction event, and imaging confirmation. Furthermore, the PCT may overestimate pGBL, as it relies on anterior inferior glenoid morphology to reconstruct the native glenoid. To mitigate this limitation, we incorporated additional measurement techniques less dependent on anterior rim geometry. In addition, the relatively small sample size also limits our ability to definitively draw conclusions for certain variables, such as glenoid version, and predisposes to type 2 errors. Demographic differences between groups may represent a potential source of confounding. In this cohort, patients with recurrent dislocations were significantly younger (P = .043) than those with a single dislocation, which may reflect higher activity levels or greater risk exposure. MRI data before the initial onset of dislocation were also not available for most patients, given that there was likely no indication for advanced imaging before injury. As a result, it is not possible to definitively determine whether measured pGBL represents true acquired bone loss or preexisting osseous morphology, such as glenoid dysplasia. Therefore, the reported pGBL values may reflect baseline posterior glenoid deficiency, rather than interval bone loss after instability events. Baseline imaging would have provided additional comparison data, allowing us to better characterize the changes seen with dislocation events.
Imaging modality heterogeneity represents a limitation, as not all patients underwent CT imaging, the reference standard for osseous GBL assessment.2,7 However, MRI has demonstrated comparable accuracy, with multiple studies showing no significant differences in GBL measurements between modalities across both 2D and 3D techniques.3,9,10,14,20 Agreement between modalities has been reported, with GBL differences typically within a small margin (<2%), with excellent intermodality reliability.9,10 This suggests that imaging modality did not significantly impact the measurement of pGBL in this study. This heterogeneity also reflects real-world clinical practice, where MRI is frequently utilized in the evaluation of shoulder instability, due to the advantage of concurrent evaluation of soft tissue pathology, and avoidance of radiation exposure. 20
Conclusion
After first-time traumatic posterior dislocation, the mean pGBL was approximately 11%. Bone loss increased with recurrent dislocations, approaching thresholds associated with failure after isolated posterior soft tissue stabilization. No association was found with reverse Hill-Sachs lesion size. Early recognition and intervention, particularly in high-demand populations at risk of recurrent dislocation, may be appropriate to prevent pGBL progression.
Footnotes
Submitted December 14, 2025; accepted April 30, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.M.F. received support for education from Supreme Orthopedic Systems. B.W.H. received support for education from Supreme Orthopedic Systems. J.F.D. received support for education from Supreme Orthopedic Systems and SouthTech Orthopedics; compensation for services other than consulting from Arthrex; royalties from SLACK; is a board or committee member of SOMOS, AAOS, AOSSM, and AANA; and is on the editorial board of AJSM. All the authors are employees of the US Government. This work was prepared as part of their official duties. Title 17 USC §105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 USC §101 defines a US Government work as a work prepared by a military servicemember or employees of the US Government as part of that person’s official duties. The contents of this publication are the sole responsibility of the author(s) and do not necessarily reflect the views, opinions, or policies of the Department of Defense (DoD) or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the US Government.