
Abstract
Objectives:
The aim of this study is to describe the in vitro adsorption of anti-infective drugs onto an extracorporeal cytokine adsorber.
Methods:
Various anti-infective drugs (β-lactams, quinolones, aminoglycosides, glycopeptides, azole antimycotics) were prepared in normal saline 0.9% and human albumin 5%, and pumped through a cytokine cartridge (CytoSorb®; CytoSorbents Corporation, Monmouth Junction, NJ, USA) at a flow rate of 1.2 L/h for 1.5 h. In addition, meropenem and ciprofloxacin were dissolved in reconstituted blood and run through a CytoSorb cartridge, which was integrated into a continuous renal replacement therapy circuit with a flow rate of 2 L/h for 18 h. Samples from the solution, pre- and post-filter, were quantified by high-performance liquid chromatography with ultraviolet detection and fluorescence polarisation immunoassay.
Results:
Observed mean clearance of the drugs in normal saline was 1.22 ± 0.07 L/h. In human albumin, clearance was 1.29 ± 0.08 L/h. In reconstituted blood, clearance of meropenem decreased from 5.4 to 1.4 L/h and for ciprofloxacin from 6.3 to 4.3 L/h within the first 1.5 h because of early drug adsorption. Continuous renal replacement therapy clearance measured without CytoSorb was stable at 2 and 1.7 L/h, respectively. Approximately 400 mg of meropenem and 300 mg of ciprofloxacin had been adsorbed by CytoSorb, suggesting that these amounts are the maximum adsorptive capacity for these drugs.
Conclusion:
In these settings, all tested drugs were adsorbed by the cartridge in relevant amounts. The identified maximum adsorptive capacity and the rapid decline in concentration during the first 1.5 h of CytoSorb use suggest that the administration of an additional dose within the first hours of CytoSorb treatment may be reasonable. In addition, early therapeutic drug monitoring should be considered.
Introduction
Recently, novel cytokine adsorber systems have been developed as a treatment for the ‘cytokine storm’ that occurs during sepsis and septic shock.1,2 These systems are designed for the elimination of middle molecular weight substances like cytokines and mediators. The CytoSorb® adsorber cartridge (CytoSorbents Corporation, Monmouth Junction, NJ, USA) is filled with a porous adsorbent made of polymer beads, which are designed to adsorb molecules from 10,000 to 50,000 Da. Adsorption is achieved through hydrophobic interactions of molecules and the lipophilic surface of the inner channels and pores of the beads. 3 The filter can be used as a stand-alone device or in combination with continuous renal replacement therapy (CRRT). Due to its non-specific adsorptive mechanism, elimination of anti-infective drugs through the cytokine adsorber is possible, even though they usually have a molecular size <2000 Da. After regulatory approval for clinical use, cytokine adsorbers are now increasingly used in critically ill patients with sepsis and septic shock, resulting in various case reports.4–7 In addition, the international CytoSorb register with over 170 centres participating was implemented to record the use and efficacy of cytokine adsorber systems under real-life conditions. 8 However, to date, there is limited data showing the efficacy and effectiveness for clinical outcome parameters. Little is known about pharmacokinetics of anti-infective agents with concomitant use of cytokine adsorptive systems such as CytoSorb. Therefore, the aim of this in vitro study was to evaluate the adsorption capacity of CytoSorb in aqueous solutions and reconstituted blood for commonly used anti-infectives such as vancomycin, gentamicin, meropenem, flucloxacillin, piperacillin, ciprofloxacin, rifampicin, fluconazole and voriconazole.
Materials and methods
The adsorptive capacity of the cytokine adsorbent system CytoSorb was tested using three different experimental settings. Adsorptive capacity for all anti-infective drugs was investigated in an aqueous medium using normal saline (NaCl 0.9%) solution. Moreover, human albumin (HA) 5% was used as a carrier to investigate the effect of plasma-protein binding (PB) on drug clearance (CL). During the experiments, the cytokine adsorber was macroscopically inspected for colour changes. Finally, for meropenem and ciprofloxacin, reconstituted blood was used to determine the potential influence of erythrocytes and potential saturation effects on the CL of these two drugs.
Normal saline and human albumin solutions
Standardised concentrations of vancomycin (40 mg/L), gentamicin (20 mg/L), meropenem (20 mg/L), ciprofloxacin (15 mg/L), piperacillin (80 mg/L), flucloxacillin (80 mg/L), voriconazole (10 mg/L), rifampicin (10 mg/L) and fluconazole (40 mg/L) were used. All anti-infective drugs were dissolved in a total of 1000 mL NaCl 0.9% and 500 mL HA 5%. These solutions were pumped through the cytokine filter at a flow rate of 1.2 L/h with an infusion pump (Infusomat Space®; B. Braun Melsungen, Germany). To ensure drug mixing, the solutions were stirred (190 r/min) continuously throughout the experiments. To avoid recirculation, inlet and outlet of the circulation were fixed to opposing sides of the reservoir (Figure 1). During a circulation time of 1.5 h, samples of the solutions as well as post- and pre-filter samples were obtained. Samples were taken at 0, 5, 20, 35, 55, 75 and 95 min and then stored at −80°C until analysis.
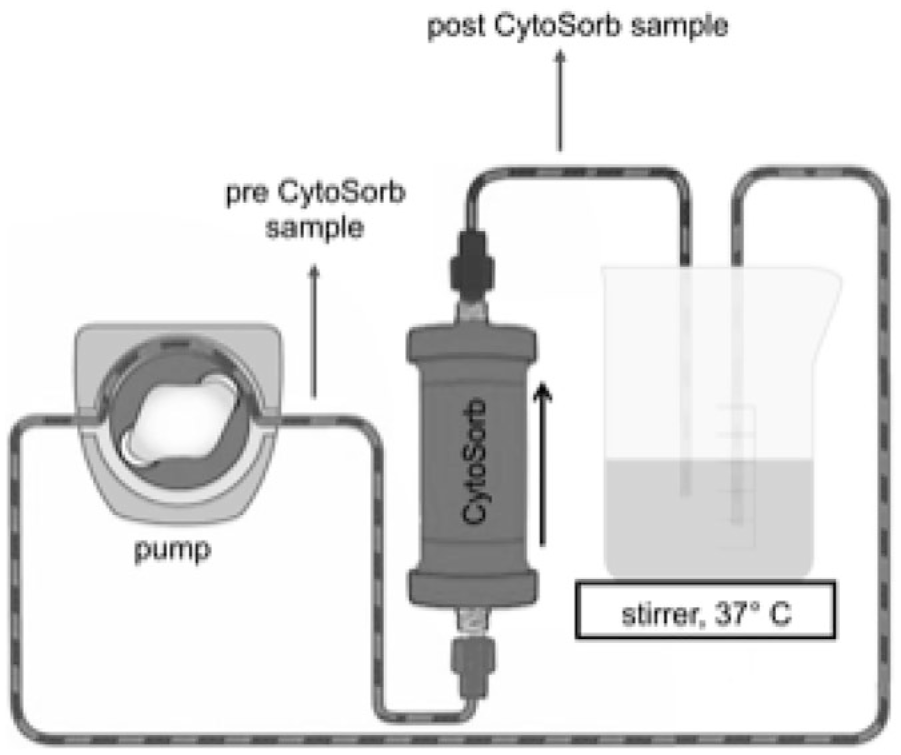
Experimental setup for normal saline and human albumin solutions (adapted from CytoSorbents Europe GmbH).
Reconstituted blood
Reconstituted blood (2.9 L) was obtained by mixing matched plasma and erythrocyte concentrates to achieve a haematocrit of 23%. To avoid clotting, heparin was added to the circuit via continuous infusion of 10,000 I.U./50 mL NaCl 0.9% with a flow rate of 5 mL/h. The Erlenmeyer flask was primed with heparin (10,000 I.U. heparin/50 mL NaCl 0.9%) prior to the start of the experiment. Meropenem and ciprofloxacin were added to the blood solution to achieve a concentration of 16 and 2.5 mg/L, respectively, and infused continuously (meropenem, 192 mg/h; ciprofloxacin, 30 mg/h) during the experiment. Both solutions were run through the CytoSorb cartridge built into a CRRT system (multiFiltrate®; haemofilter AV 600S, Fresenius Medical Care, Bad Homburg, Germany) in continous veno-venous haemodialysis (CVVHD) mode with a blood flow of 12 L/h and a dialysate flow of 2 L/h (Figure 2). Samples were taken from pre- and post-cytokine adsorber and dialysis filter, as well as from the dialysate over a sampling time of 18 h. Samples were taken at 0.5, 1.5, 2.6, 3.6, 4.6, 5.6, 6.6, 8.6, 10.6, 14.5 und 18.3 h after starting the circuit.
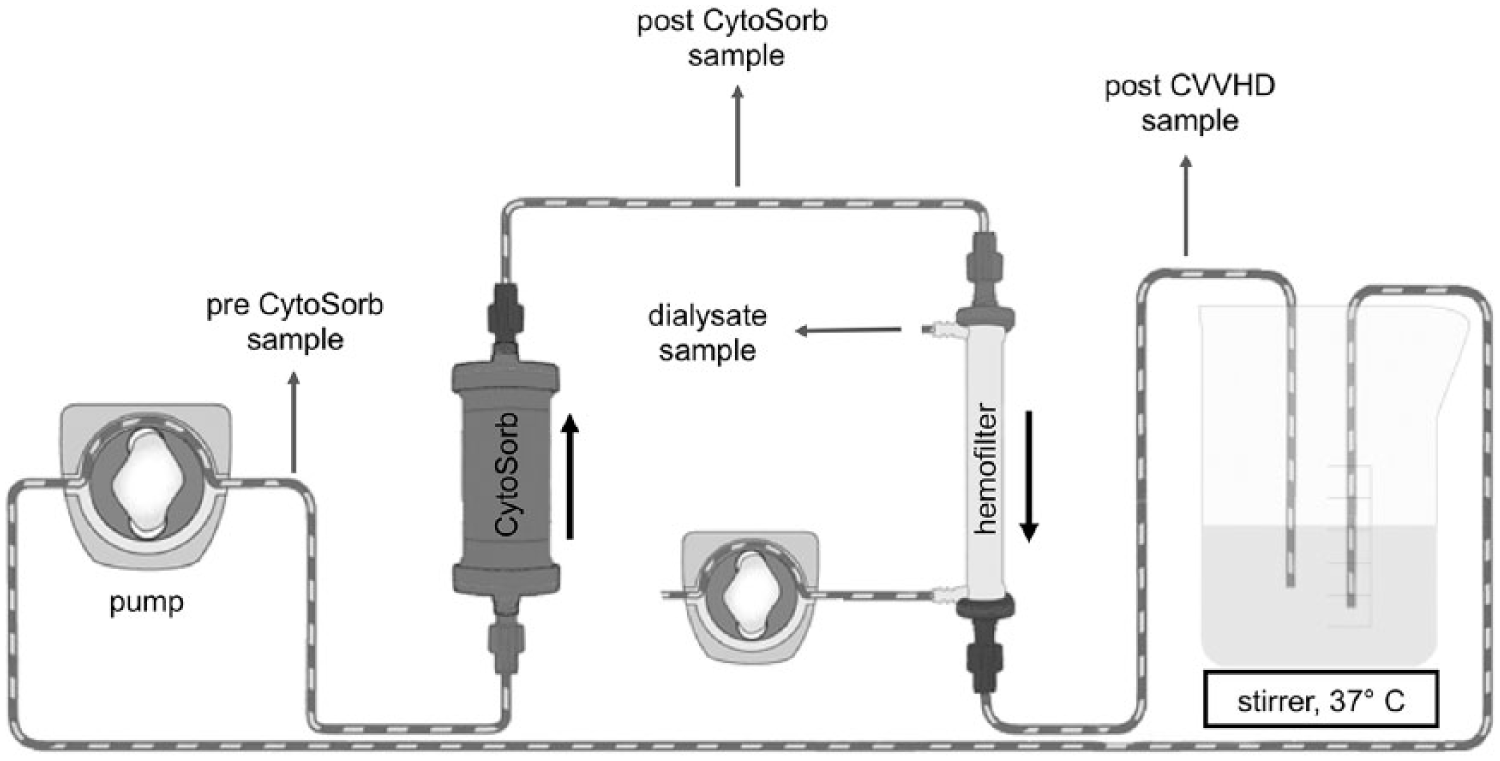
Experimental setup for reconstituted blood using CytoSorb and continous veno-venous hemodialysis (CVVHD) (adapted from CytoSorbents Europe GmbH).
To ensure drug mixing and to avoid clotting, the solutions were kept at 38°C and stirred (190 r/min) continuously throughout the experiments. All samples were immediately centrifuged (3000 r/min, 10 min, 25°C); plasma was separated and then stored at −80°C until analysis.
Analytical quantification
Vancomycin and gentamicin concentrations were analysed with fluorescence polarisation immunoassay (Axsym; Abbott Diagnostics, Lake Forest, IL, USA). All other drug concentrations were analysed with high-performance liquid chromatography (HPLC) with ultraviolet (UV) detection. Assay validation was performed according to the FDA Guidance for Industry for biochemical method validation using calibration standards and quality controls. 9 Assay performance was previously reported by Roehr et al. 10 Reconstituted blood samples were centrifuged. HA and serum samples were treated with acetonitrile and methanol (1:1) for protein precipitation and centrifuged at 3000 r/min for 10 min prior to analysis. The supernatant was transferred and used for drug quantification.
Pharmacokinetic calculations
Pharmacokinetic parameters of half-life (t1/2) and CL of each drug were calculated using descriptive methods and assuming first-order kinetics and a one-compartment model. The elimination constant (ke) was determined by the slope of the regression line of concentrations and was used for the estimation of drug t1/2 via t1/2 = ln(2)/ke. CL was calculated as follows: CL = ln(2) × Vd/t1/2, with Vd being the volume of the solution in litre (L). Adsorption in the reconstituted blood setting was calculated as follows: Adsorption = Dose added (mg) – (Concentration (mg/L) × Total fluid volume (L)).
To determine the amount eliminated via CRRT and CytoSorb, calculation was as follows
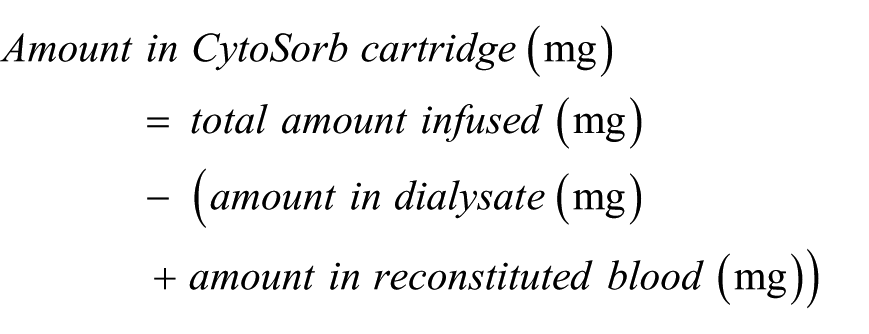
For comparison, similar equations were used to investigate and determine the kinetic properties of renal replacement therapies in clinical data. 11
Results
All experiments were performed under stable conditions without technical problems. The cytokine cartridge was perfused without interruptions. Haematocrit (23%) and pH (7.4) of reconstituted blood remained stable throughout the experiment. There were no signs of blood stasis and no clotting occurred.
Normal saline solutions
There was a steep decrease of all drug concentrations during the first 20 min of the experiment. After this time, no drug was detectable in post-filter samples of the saline solutions except for gentamicin, which was detectable in the post-filter samples for 35 min after the start of the experiment (Table 1).
Pharmacokinetic parameters determined in HA 5% and NaCl 0.9% and general chemical properties.
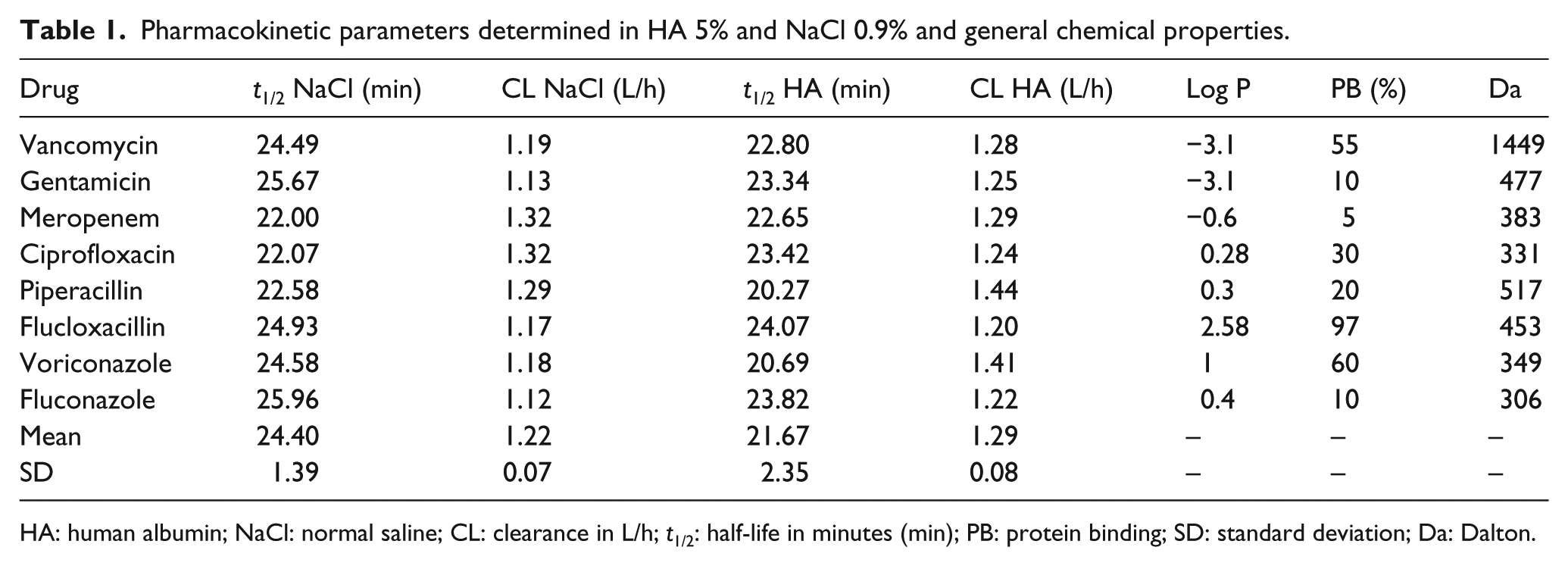
HA: human albumin; NaCl: normal saline; CL: clearance in L/h; t1/2: half-life in minutes (min); PB: protein binding; SD: standard deviation; Da: Dalton.
Observed t1/2 and apparent CL in normal saline were similar across the observed drugs. For example, meropenem, ciprofloxacin and fluconazole showed a t1/2 of 21.07, 22.29 and 22.73 min, and apparent CL values of 1.29, 1.32 and 1.28 L/h, respectively. However, rifampicin showed a lower t1/2 of only 15 min resulting in a higher CL of 2.05 L/h. The mean observed drug CL and t1/2 in normal saline was 1.22 ± 0.07 L/h and 24.40 ± 1.39 min, respectively (Table 1). The decrease in drug concentration in pre-filter samples followed first-order kinetics. After 1.5 h perfusion of the cytokine adsorber, concentrations of the antibiotics meropenem, ciprofloxacin, vancomycin, piperacillin and flucloxacillin were very low or not further detectable (Table 2). The antimycotics voriconazole and fluconazole also showed low concentrations with 0 and 3 mg/L, respectively.
Pre- and post-CytoSorb drug concentrations in NaCl 0.9%.
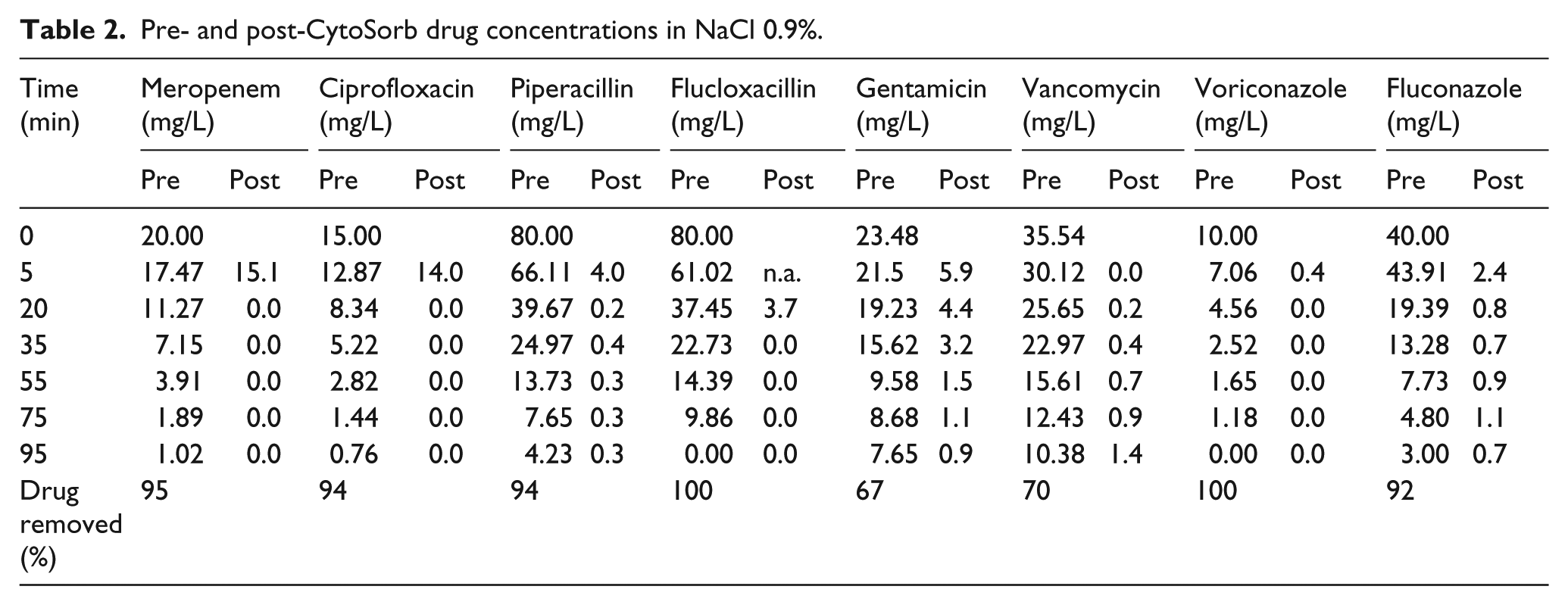
Rifampicin was completely adsorbed within the first 15 min of the experiment. This was accompanied with a visible colour change from white to red of the adsorber cartridge.
Human albumin solutions
Within the first 60 min of the investigation, the decrease in drug concentration followed first-order kinetics. Observed t1/2 and CL were homogeneous among the anti-infective drugs. For example, meropenem, ciprofloxacin and fluconazole showed a t1/2 of 22.65, 23.42 and 23.82 min, respectively. The corresponding CL values were 1.29, 1.24 and 1.22 L/h, respectively. The mean CL and t1/2 in HA were 1.29 ± 0.08 L/h and 21.67 ± 2.35 min, respectively (Table 1). Antibiotic and antimycotic concentrations fell rapidly within the first 20 min. After approximately 1 h, there was no further drug removal for flucloxacillin, voriconazole, meropenem and ciprofloxacin. In contrast, vancomycin, gentamicin, fluconazole and piperacillin were steadily removed throughout the experimental period (Table 3).
Pre- and post-CytoSorb drug concentrations in HA 5%.
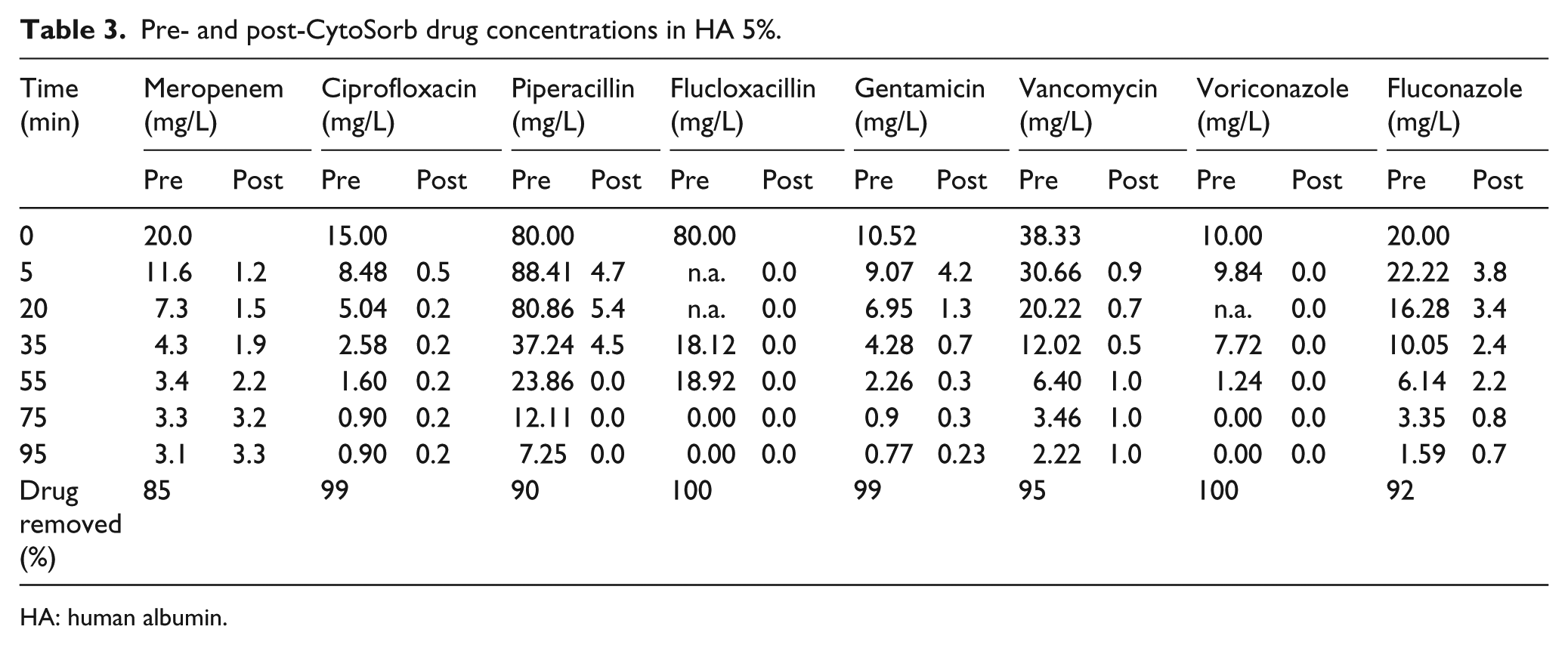
HA: human albumin.
Since no rising in concentrations was measured at the end of both experiments, no redistribution could be detected for all of the investigated drugs.
Reconstituted blood
Within the first 1.5 h, the cytokine adsorber CL (L/h) for ciprofloxacin decreased from 6.3 to 4.9 L/h with an estimated t1/2 of 28 min (Figure 3(a)). For meropenem cytokine adsorber, CL decreased from 5.4 to 1.4 L/h with a t1/2 of 34 min (Figure 3(b)). Significant removal of meropenem and ciprofloxacin occurred within the first 1.5 h of cytokine adsorber use. Within the first 0.5 h, a decrease in meropenem concentration of approximately 45% and for ciprofloxacin of approximately 52% occurred, measured by pre- and post-cytokine cartridge levels.
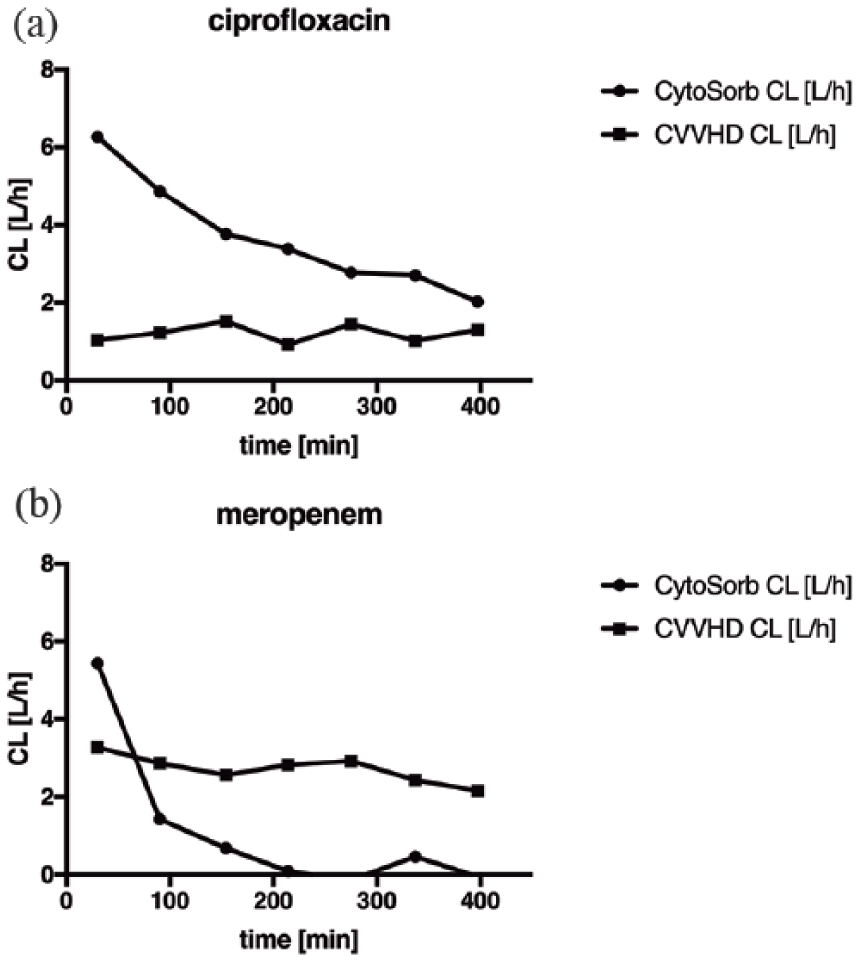
Ciprofloxacin (a) and meropenem (b) clearance (CL) under CytoSorb and continous veno-venous haemodialysis (CVVHD).
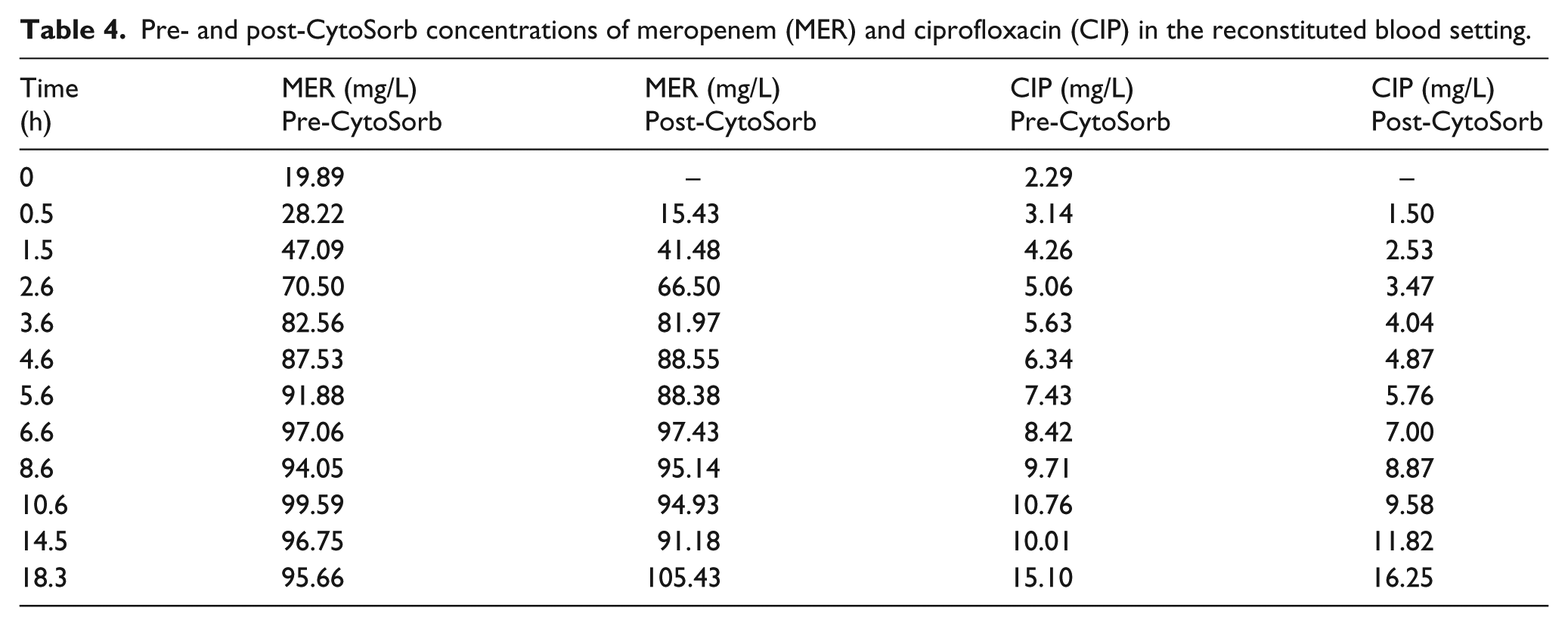
After 4 h, there were no significant changes in meropenem concentrations across pre- and post-cytokine adsorber samples, whereas significant changes in concentration of ciprofloxacin could be measured for up to 10 h while using the cytokine cartridge (Table 4). During the total observation period of 18 h, 394 mg of meropenem and 284 mg of ciprofloxacin were adsorbed by the cytokine cartridge. In contrast to that, 2870 mg of meropenem and 235 mg of ciprofloxacin were removed by continous veno-venous haemodialysis (CVVHD).
Pre- and post-CytoSorb concentrations of meropenem (MER) and ciprofloxacin (CIP) in the reconstituted blood setting.
The mean dialysis CLs (L/h) of meropenem and ciprofloxacin were 2.0 and 1.7, respectively (Figure 3(a) and (b)). They remained stable throughout the experiment and no saturation effects were observed.
Discussion
During the experiment, commonly used antibiotics and antimycotic drugs for the treatment of bacterial and fungal infections were investigated. The substances showed a wide range in PB (0%–97%), 12 lipophilicity (log P -3.1- 2.7) 13 as well as in molecular weight (306–1449 Da). 12 In contrast to the previous investigation by Reiter et al., 14 where initial drug concentrations were very high, for example, vancomycin 1048 mg/L or gentamicin 153 mg/L, we chose initial drug concentrations according to those achieved therapeutically, for example, gentamicin 20 mg/L and vancomycin 40 mg/L, representing observed serum concentrations in humans. We observed a considerable high apparent adsorptive CL of anti-infective compounds during the first 20 min of the use of the cytokine adsorber in HA and normal saline. This is in accordance to the findings of Reiter et al. 14 who also found a high adsorption of vancomycin, gentamicin and teicoplanin during the first 15 min of treatment with a cytokine adsorber. Comparing the adsorption results in HA and normal saline showed no significant deviation within the CL values. Even though several drugs such as flucloxacillin show a high PB of up to 97%, 15 no major effect of PB could be identified. In critically ill patients, lower serum albumin concentrations with less than 35 g/L are frequently observed. 16 However, even when using higher albumin concentrations of 50 g/L (5%), representing more potential binding sites for anti-infective agents, no significant differences in CL during the first hour of the experiment could be identified. Taking a closer look to the concentrations, it becomes obvious that some drug concentrations in normal saline fall more rapidly than in albumin and vice versa. Therefore, further studies are needed to confirm which physicochemical characteristics of drugs are relevant for the adsorption on cytokine cartridges. But this suggests that the adsorber is potentially able to eliminate even substances with a high PB. This might be due to a potentially higher binding affinity between the anti-infective drugs and the cytokine adsorber than between drug and albumin.
In the aqueous solution setting rather low flow rates (1.2 L/h) were used, this was due to the use of an infusion pump and its maximum flow rate. This flow rate results in a long contact time between drug and sorbent surface, potentially leading to a higher adsorption ratio. In clinical practice, much higher blood flow rates (9–12 L/h) are used, especially in combination with CRRT resulting in a shorter contact time. Therefore, our results might have overestimated the adsorbent capacity for anti-infective drugs in aqueous solutions. This also indicates that only experiments using blood would be relevant for clinical practice.
Furthermore, high drug elimination rates were also observed in the reconstituted blood experiment. The initial drug CL by CytoSorb was 5.4 L/h for meropenem, which was higher than reported for CRRT in clinical data (approximately 3 L/h). 17 The mean CRRT CL for meropenem and ciprofloxacin of 2.0 and 1.7 L/h, respectively, corresponds to the selected dialysate flow of 2 L/h, which is in accordance with the findings of Roehr et al. 10 who found CLs of 1.9 for meropenem and 1.7 L/h for ciprofloxacin during CRRT.
During the whole experiment using reconstituted blood, approximately 300 mg of ciprofloxacin and 400 mg of meropenem were eliminated over 18 h via CytoSorb. However, since the CL was significantly lower after 1.5 h, the largest share of meropenem and ciprofloxacin removal occurred early after initiation of CytoSorb. Therefore, higher doses of anti-infective drugs for the first hours of therapy with CytoSorb might be advisable to saturate drug binding to the adsorber and achieve adequate plasma concentrations according to their pharmacokinetic/pharmacodynamic targets and break points for susceptible bacteria. 18 Timely and optimal drug exposure could be maintained effectively through routine therapeutic drug monitoring. 19
For all in vitro experiments, maximum adsorption occurs within the first 60 min after the installation of the CytoSorb System. Irrespective of the carrier solution, a very high initial drug loss could be observed in all experiments. Since a combination of several anti-infective drugs was tested in one solution, this might not represent the clinical setting where less substances are used simultaneously. The presence of many drugs potentially binding to the cytokine adsorber might have influenced its binding capacity. Therefore, a potential underestimation of the adsorptive capacity is possible but might not be relevant because of the high overall CL. In septic shock and especially in recurrent sepsis episodes, often multi-drug resistant gram-negative pathogens are present (e.g. Pseudomonas spp.). Therefore, our unit commonly uses empirical combination therapy containing double Gram-negative coverage with meropenem and ciprofloxacin until culture results are available. Thus, we focussed on meropenem and ciprofloxacin in our investigation. Therefore, further studies are needed to confirm similar behaviour under CytoSorb therapy.
Limitations
Due to the experimental setting, there are several limitations of these in vitro results. The results from the aqueous and HA solutions cannot be extrapolated to critically ill patients. Furthermore, the solutions do not contain cellular components such as erythrocytes, platelets and human proteins, which may influence the adsorptive capacity of the CytoSorb cartridge and apparent drug CL. To partially compensate this effect, reconstituted blood composed of plasma and erythrocyte concentrates was used at physiologically relevant concentrations. However, platelets and other proteins such as alpha-1 globulins, alpha-2 globulins and immunoglobulins were not present. The haematocrit of 23% was relatively low, but this is not uncommon in critically ill patients. 20 A higher proportion of cellular components in vitro and in vivo may decrease the adsorptive capacity by blocking the surface of the polymer beads in the cartridge. Moreover, we have not studied a possible release of anti-infectives from a fully saturated system. With using a continuous infusion method, we created a fully saturated system, shown by the accumulation of meropenem and ciprofloxacin levels. But the accumulation ratio of anti-infectives was nearly equivalent to the infusion ratio, and therefore desorption of meropenem and ciprofloxacin seems less likely. Furthermore, we used small volumes (2.9 L reconstituted blood) and drug amounts to achieve pharmacokinetically relevant concentrations which are different drug amounts which are present in a clinical scenario. Therefore, the time course for decreasing concentrations of drug as it binds to the adsorber may be slower in clinical practice. This was confirmed by the experiment in reconstituted blood, where we quantified the amount of drug able to be adsorbed by the cartridge.
Conclusion
The results of our in vitro experiments show that all investigated drugs are adsorbed to the surface of the CytoSorb adsorber and are removed by the combined CRRT system to varying but clinically relevant degrees. Anti-infective drugs are removed from the circulation by CytoSorb in a non-linear fashion as opposed to CRRT. In contrast to CRRT where drugs are removed in a continuous fashion, the use of CytoSorb appeared to saturate the adsorbent surface leading to a reduction in CL over time. For meropenem and ciprofloxacin, we found that the initial adsorptive capacity corresponded to a single dose of approximately 400 and 300 mg, respectively, meaning that this represents the maximum amount of drug that could be adsorbed. This suggests that the administration of an additional dose within the first hours of initiation of the cytokine adsorber may be reasonable. Moreover, with each routine change of the cytokine adsorber system after 8, 12 or 24 h, an extra dose of meropenem and ciprofloxacin should be considered to maintain optimal drug exposure. To optimise anti-infective drug dosing in septic patients treated with CytoSorb and CRRT, further studies are needed to investigate the in vivo effect of extracorporeal blood purification systems on the pharmacokinetics of these drugs. Most importantly, our results emphasise the importance of early therapeutic drug monitoring for patients not only on renal replacement therapy but also on cytokine adsorber therapy to avoid underdosing of anti-infective drugs.
Footnotes
Acknowledgements
C.K. made substantial contribution to conception, study design, sample analysis, data collection, data analysis and interpretation of data, and drafting the manuscript and approved the final version to be published. A.C.R. made substantial contribution to conception, study design and revising the manuscript for intellectual content and approved the final version to be published. J.A.R. made substantial contribution in revising the manuscript for intellectual content and approved the final version to be published. O.R.F. made substantial contribution to study design, data collection sample analysis and revising the manuscript for intellectual content, and approved the final version to be published. A.B. made substantial contribution to conception, study design and data collection, sample analysis and drafting, and revising the manuscript for intellectual content and approved the final version to be published. A.N. made substantial contribution to conception, study design and data collection, sample analysis and drafting, and revising the manuscript for intellectual content and approved the final version to be published. D.W. made substantial contribution to conception, study design, drafting and revising the manuscript for intellectual content and approved the final version to be published. S.B. made substantial contribution in revising the manuscript for intellectual content and approved the final version to be published. S.K. made substantial contribution to conception, study design and data collection, sample analysis, and drafting and revising the manuscript for intellectual content and approved the final version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.A.R. is funded by a Practitioner Fellowship from the National Health and Medical Research Council of Australia (APP1117065) and would like to acknowledge funding from the National Health and Medical Research Council of Australia for a Project Grant (APP1044941) and Centre for Research Excellence (APP1099452).