
Abstract
Hyperbilirubinemia occurs in up to 40% of critically ill. In ICU, hyperbilirubinemia is an independent factor that influences patients’ morbidity and mortality. Jaundice can reflect the course of disease or be caused by treatment (e.g. extracorporeal membrane oxygenation (ECMO)), thus can be difficult to differentiate. Sepsis was also associated with development of jaundice secondary to intrahepatic cholestasis. Prolonged cholestasis should be addressed to avoid liver damage. The patient with diagnosis of septic shock and severe acute respiratory distress syndrome was retrieved to our hospital for ECMO. Three days after initiation of ECMO, the patient developed jaundice, with increase of bilirubin, Gamma-glutamyltransferase and Alkaline phosphatase, without elevation of alanine aminotransferase and INR. Although ECMO was stopped, bilirubin serum levels were increasing, reaching the peak of 18.41 mg/dL of total and 15.67 mg/dL of direct bilirubin. Abdominal computed tomography showed homogeneous liver and non-dilated bile ducts. Viral hepatitis was excluded. CIOMS/RUCAM score was 0. Sepsis-related cholestasis was diagnosed. Despite cessation of sedation, the patient remained unconscious. Hemoadsorption therapy was initiated due to prolonged high levels of conjugated bilirubin. After 48 h of CytoSorb treatment, total bilirubin level was decreased to 2.4 mg/dL, the patient regained spontaneous eyes opening and could be transferred to regional hospital. Hyperbilirubinemia did not return in 3 months. Sepsis-related cholestasis is a diagnosis of exclusion that should be considered in case of jaundice in critically ill patients. In our patient, CytoSorb was a useful therapeutic option in prolonged cholestasis. Adsorption therapy was able to facilitate long-term regain of balance between inflammatory process, cytokine production and bilirubin turnover in the liver.
Keywords
Introduction
Hyperbilirubinemia is defined as total serum or plasma bilirubin level >1 mg/dL (17.1 µmol/L) and occurs in up to 40% of critically ill patients. 1 In ICU settings, hyperbilirubinemia is an independent factor of patient morbidity and mortality. 2 Diagnosis of hyperbilirubinemia can be difficult due to the different origins of this condition, which is hemolytic (pre-hepatic), hepatocellular (hepatic) and obstructive (post-hepatic). Moreover, the most known symptom of hyperbilirubinemia, jaundice, can be difficult to differentiate, especially in critically ill individuals. 3 Jaundice can reflect the course of disease, but may also be caused by implemented treatment. Aetiology of hyperbilirubinemia includes hemolysis, transient hypotension (shock liver), right-side heart failure, pharmacologic toxicity or multiorgan failure. 3 However, cholestasis, which affects both production and secretion of bile, can cause permanent damage of the liver. 4 Sepsis can lead to intrahepatic cholestasis due to dysregulated and prolonged cytokine production. 3 Beside liver dysfunction, sepsis more often causes respiratory and circulatory impairment. In cases of severe acute respiratory distress syndrome (ARDS), ventilatory support can be necessary. Occasionally, more invasive techniques as veno-venous extracorporeal membrane oxygenation (VV-ECMO) have to be implemented to achieve sufficient oxygenation of blood gases. However, ECMO can cause hemolytic hyperbilirubinemia due to erythrocyte disruption on the oxygenator. This process can also lead to jaundice, especially when liver function is impaired, as it happens in sepsis. In cases of prolonged hyperbilirubinemia of both direct and indirect origin, the approach to reduce bilirubin and bile acid levels should be taken to avoid further organ damage, especially permanent liver damage. 4
Therapeutic approaches having evidence of benefit in lowering the bilirubin serum levels include extracorporeal liver support (e.g. molecular adsorbent recirculating system (MARS)) 5 or extracorporeal cytokine hemoadsorption device (CytoSorb). 6 The CytoSorb introduced initially as cytokine absorber, was recently approved by the European Union for reduction of elevated bilirubin and myoglobin serum levels.
Herein, we describe the case of a patient with hyperbilirubinemia which was developed during VV-ECMO therapy implemented due to severe pneumonia. The patient was successfully treated with CytoSorb hemoadsorption device. We reviewed the literature to present a differential diagnosis and potential treatment of severe hyperbilirubinemia.
Case presentation
Patient’s state at admission
The 58-year-old woman was referred to a tertiary hospital with primary diagnosis of severe ARDS caused by sepsis originating from unspecified pneumonia. The patient was sedated and ventilated for 4 days prior to admission, with elevated positive end-expiratory pressure (PEEP) (15 cmH2O) and high values of FiO2 (0.85–1.0) reaching PaO2/FiO2 ratio of approximately 75 and ETCO2 of 8.8 vol%. Circulatory system was supported with norepinephrine (0.62 µg/kg/min). Patient’s sequential organ failure assessment (SOFA) score at admission was 14. Inflammatory markers were highly elevated (white blood cell 27.8 × 10³/µL, C-reactive protein 473.5 mg/L, procalcitonin 28.7 ng/mL). The RESP score at referral was 3 as we accepted the patient for extracorporeal respiratory support.
Radiological evaluation
The ultrasound lung examination during admission of the patient revealed bilateral C profile in midclavicular lines and B-line artefacts. Hyperkinetic features of circulation were observed during echocardiography with left ventricular ejection fraction of 75%–80% (Simpson method). Chest X-ray on the first day of ICU stay showed massive, merging, bilateral opacities corresponding with consolidations.
Extracorporeal support
VV-ECMO (ILA; NovaLung GmbH, Talheim, Germany) therapy was initiated with collecting cannula inserted into right femoral vein and return cannula into right internal jugular vein. Blood flow was set between 2.5 and 5 L/min and sweep gas flow rate between 1 and 3 L/min. The subcutaneous nadroparin dose of 0.8 mL/day was used as anticoagulant prophylaxis. Continuous veno-venous hemodialysis with regional citrate anticoagulation (CVVHD Ci-Ca) (Multifiltrate; Fresenius, Bad Homburg, Germany) was started simultaneously with ECMO. Three units of blood and platelets were transfused during ECMO support.
Medications
Patient required continuous infusions of norepinephrine (0.12–0.36 µg/kg/min) and dobutamine (3.7–7.8 µg/kg/min) throughout the treatment. Doses of amines and fluid therapy were adjusted according to the echocardiographic imaging. Empiric broad-spectrum antibiotics (meropenem + linezolid + sulfamethoxazole/trimethoprim) were administered until blood and bronchoalveolar lavage (BAL) cultures results were available. After identification of Acinetobacter baumannii from BAL, treatment was modified accordingly (amikacin, tigecycline). Enteral and parenteral nutrition was initiated.
Course of the treatment
Eight days after admission to ICU, patient’s respiratory condition improved allowing discontinuation of the ECMO support. Chest X-rays showed regression of changes in comparison to the day of admission. Mechanical ventilation was continued with PEEP set to 6–8 cmH2O and FiO2 to 0.4–0.6. Norepinephrine infusion was reduced (0.02–0.07 µg/kg/min) and dobutamine drip was stopped. CVVHD was discontinued on day 11 due to stable urine output. However, after cessation of renal replacement therapy, serum levels result of creatinine and urea were increasing. Hence, CVVHD was resumed on day 14. Despite withdrawal of sedation with propofol and fentanyl after 5 days patient remained unconscious (–4 Richmond Agitation-Sedation Scale score).
Hyperbilirubinemia management
While primary problem of the patient which was severe respiratory failure was diminishing at the same time the patient’s bilirubin turnover was increasingly compromised. During ICU treatment, patient developed jaundice, with a noticeable change of total bilirubin serum levels (0.81 mg/dL at admission; 3.88 mg/dL after 3 days of ECMO therapy; 7.1 mg/dL at day of ECMO discontinuation N: 0.3–1 mg/dL). The bilirubin serum levels were increasing despite discontinuation of ECMO therapy, reaching the peak of 18.41 mg/dL of total bilirubin, 2.74 mg/dL unconjugated bilirubin (N: 0.1–0.3 mg/dL) and 15.67 mg/dL of direct bilirubin (N: 0.2–0.7 mg/dL) on day 13 (total bilirubin serum levels are presented in Chart 1). Gamma-glutamyltransferase (157 IU/mL N: 6–42 IU/mL) and Alkaline phosphatase (228 IU/mL N: 20–70 IU/mL) were increased. The coagulation markers and alanine aminotransferase (ALT) were stable, within normal range (INR 1.11–1.15; prothrombin time 12.8–18.1 s, activated partial thromboplastin time 38.3–55.9 s, ALT 22.6–87.7 IU/L). Abdominal computed tomography (CT) performed on day 11 showed an enlarged liver, homogeneous in structure, with lack of evidence of focal lesions. Intrahepatic bile ducts and common bile duct were non-dilated. Immune testing for viral hepatitis revealed negative HBsAg (0.00) and non-reactive level of anti-HCV antibodies. Calculated CIOMS/RUCAM score was 0.
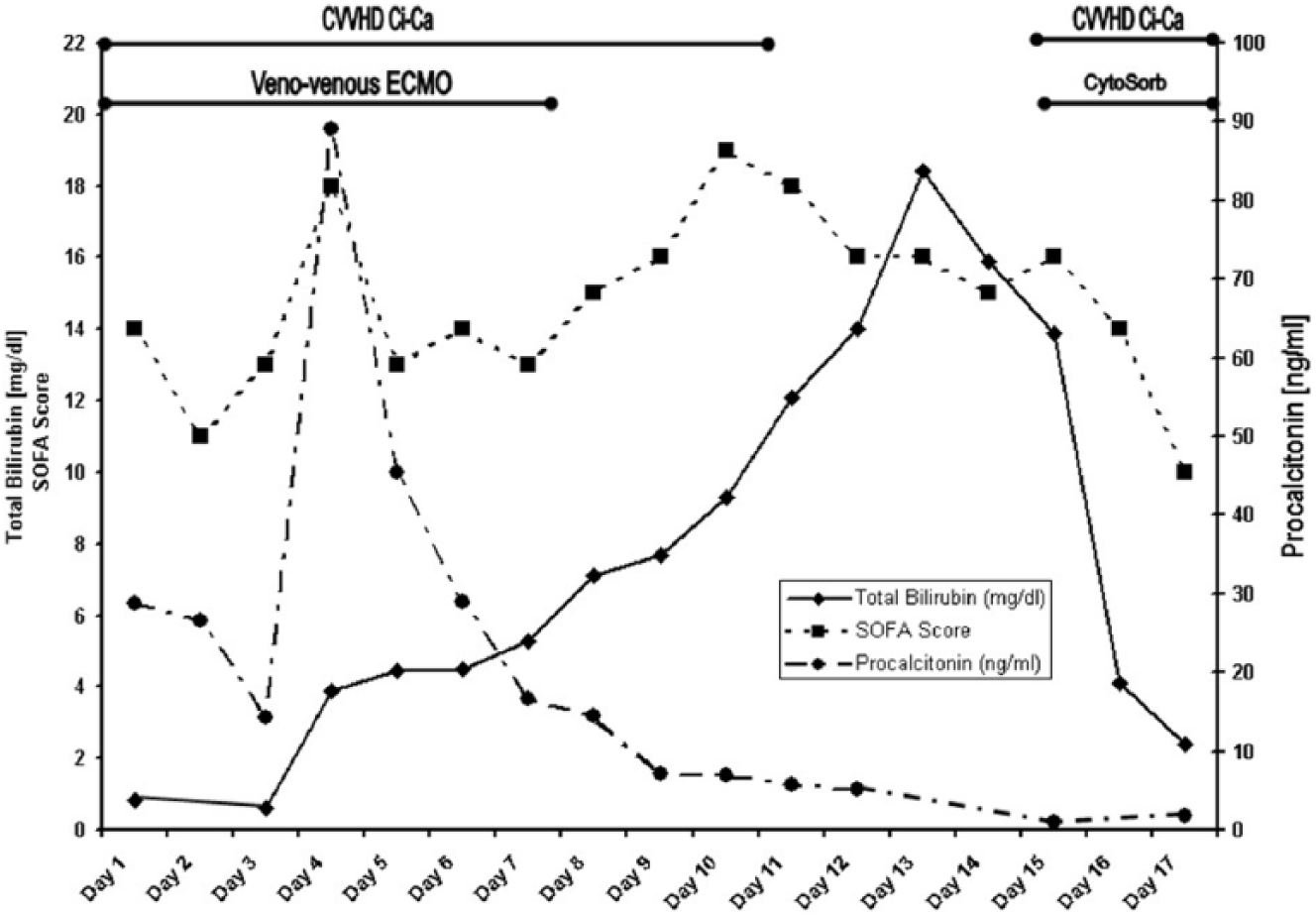
Clinical record of patient’s treatment in ICU.
As bilirubin serum levels remained high, the decision was made to install CytoSorb in series into the renal replacement therapy circuit in post-hemofilter position as a last resort. We ran two (24 h each/48 h in total) sessions with the blood flow set to 100 mL/min. The treatment resulted in reduction of total bilirubin concentration (Chart 1), while albumin serum levels remained unchanged (1.5 g/dL one day prior to CytoSorb therapy and 1.5 g/dL after 48 h of adsorption treatment). After the improvement of medical condition (SOFA score 10, Bilirubin serum levels 2.4 mg/dL) patient regained partial consciousness to the point of spontaneous eyes opening and was transferred to the regional hospital for continuation of the treatment. Hyperbilirubinemia did not return in 3-month follow-up period.
Discussion
To our knowledge, this is the first clinical case report of sepsis-induced cholestasis successfully treated with CytoSorb hemoadsorption device in a patient supported with respiratory ECMO. Although respiratory and general state of the patient improved, multiple complications followed, including temporary, partial lower legs ischemia and jaundice. Differential diagnosis and treatment of massive hyperbilirubinemia, which occurred during hospitalisation, was a challenge to clinicians. Possible mechanisms of jaundice that were considered in our patient are listed in Table 1.
Differential diagnosis of jaundice in critical ill.
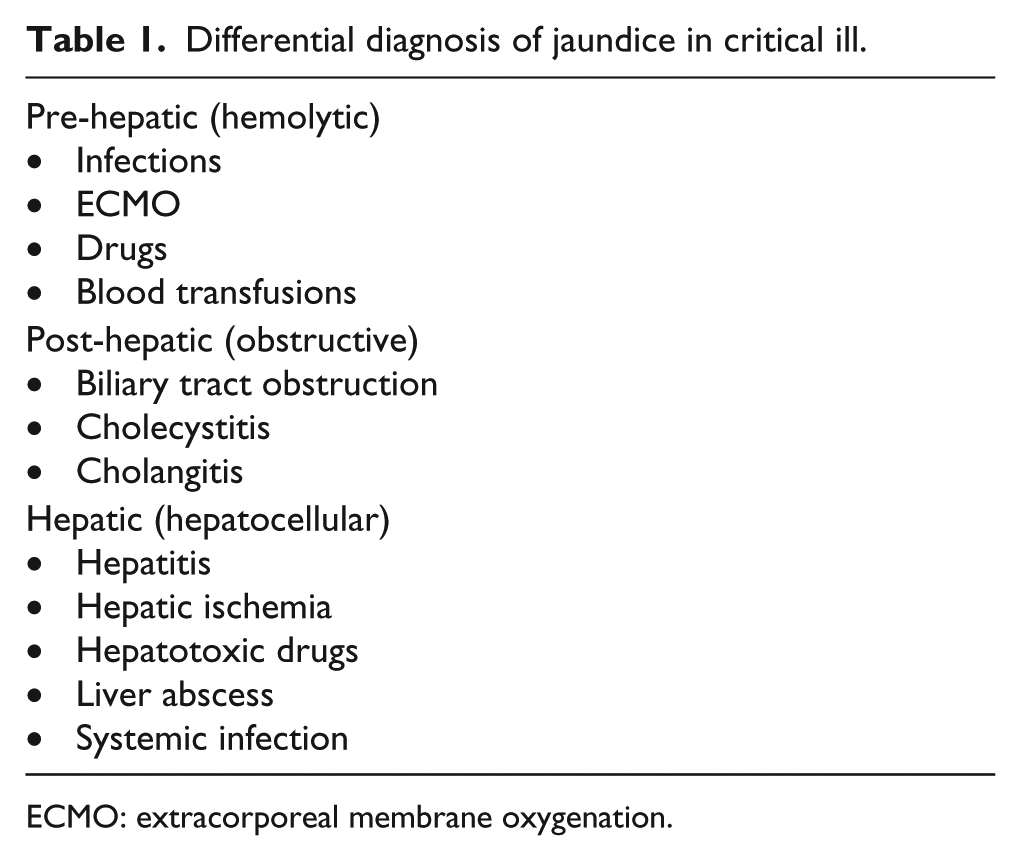
ECMO: extracorporeal membrane oxygenation.
Hemolysis associated with ECMO is a known adverse event caused by shear stress generated by flow through the circuit and oxygenator. 7 Increased red blood cells disintegration leads to elevation of unconjugated bilirubin serum levels. Although primarily in our patient bilirubin serum levels were increasing and haemoglobin was decreasing during ECMO support, on day 7, blood results showed total bilirubin level of 5.29 mg/dL and direct bilirubin of 5.12 mg/dL (N: 0.2–0.7 mg/dL), ruling out the unconjugated bilirubin as a cause of hyperbilirubinemia. The elevated unconjugated bilirubin serum levels reached a peak of 2.74 mg/dL (N: 0.1–0.3 mg/dL) 5 days after discontinuation of ECMO, while conjugated bilirubin that was the main diagnostic and treatment challenge peaked at 15.67 mg/dL. Total bilirubin serum levels are presented in Chart 1.
Differential diagnosis of increased conjugated bilirubin serum levels includes hepatocellular/hepatic or obstructive causes. In the case of our patient obstruction or hepatocellular cause like liver abscess were ruled out with the performance of abdominal CT, which revealed non-dilated ducts and liver that was homogeneous in structure. Majority of hepatocellular/hepatic causes (Table 1), for example, acute liver failure, hypoxic hepatitis can be excluded by reference range of liver function tests (INR, ALT). 8 Our patient presented stable, non-elevated level of ALT and INR throughout the whole treatment period.
Another potential cause of jaundice in ICU includes drug-induced cholestasis that usually occurs weeks or months after the start of the treatment. Furthermore, individual drugs hepatic toxicity tends to have a characteristic signature, 9 for example, psychotropic agents, antibiotics and nonsteroidal anti-inflammatory usually cause cholestasis with hepatitis. 10 Among drugs administered during hospitalisation, meropenem, linezolid, tigecycline, fluconazole, mycamine and sulfamethoxazole/trimethoprim had the potential to induce hepatotoxicity. CIOMS/RUCAM score, used for detection of drug-induced cholestasis, was 0 in the case of our patient, excluding the possibility of drug-associated liver injury. 11 In addition, study reports on drug-induced cholestasis show a pattern of recurring elevation of bilirubin serum levels after hemadsorption treatment, which did not occur in our patient. 12
Sepsis-related cholestasis is a diagnosis of exclusion that should be considered in case of jaundice in critically ill patient. It can be recognised by the presence of increased inflammatory markers and elevated serum bilirubin levels, without raise of liver enzymes. Sepsis can decrease canalicular transport, resulting in intrahepatic cholestasis. 13 The invasion of bacteria in liver is not the main mechanism in that process. 14 Cytokines released as a response to endotoxemia along with lipopolysaccharides (LPS) released by bacteria play the major role in genesis of cholestasis. 15 Adenosine triphosphate-dependent bile salt export pump (BSEP) excretes bile salts into Bile canaliculi. Cytokines such as tumour necrosis factor and interleukin-1 affect gene expression of BSEP at both the transcriptional and post-transcriptional levels. 16 The other mechanism of sepsis-related cholestasis includes the inhibition of basolateral membrane Na-K-ATPase activity, decreased basolateral membrane fluidity, down-regulation of transporters and decreased NTCP and MRP2 functions. 17 Forementioned processes, which are mainly affected by endotoxins and cytokines, lead to cholestasis. The diagnosis of sepsis-related cholestasis in our patient was made by exclusion of other potential causes of patient’s condition, according to the existing literature.5,13,17 We postponed liver biopsy until the result of hemoadsorption therapy, which has proven to be successful, making the need of invasive diagnostic procedures redundant.
We initiated CytoSorb in our patient as the treatment of last resort in jaundice. Prolonged cholestasis has proven to cause oxidative stress, mitochondrial toxicity, hepatocytes apoptosis as well as spread of bacterial infections, aggravation of hypotension due to vasodilatory properties of bile acids and impairment of the renal function. 18 The mechanism of action of CytoSorb is based on membrane adsorption of predominantly hydrophobic, protein-bound molecules sized between 5 and 60 kDa, which include bilirubin, cytokines and bile acids. In the case of our patient bilirubin serum levels, after the treatment was significantly reduced (Chart 1), confirming the usefulness of CytoSorb in high bilirubinemia, as shown in the recent case-series retrospective analysis. 19 Complementary to the mentioned study, we mainly focused on the differential diagnosis of jaundice in ICU patient. Moreover, the course of hemadsorption therapy did not affect albumin serum levels, which confirms the observations of the CytoSorb kinetics in vitro. 6
One of the drawbacks of our case report is the lack of measurement of cytokine levels throughout the treatment, due to institutional limitations. Thus, we cannot directly confirm the influence of CytoSorb on inflammatory response in our patient. Cross-absorber levels were not measured; therefore, we cannot state about direct causal relationship between CytoSorb and decrease of bilirubin serum levels. Another limitation of our case report is the fact that slight decrease of bilirubin prior to installation of hemadsorption device was observed and we are unable to rule out the additional impact of spontaneous hepatic recovery on bilirubin decline. However, we strongly believe that the initiation of CytoSorb therapy was the primary reason for the resolution of sepsis-induced cholestasis.
Clinical state of the patient significantly improved after bilirubin levels had been decreased and the patient could be transferred to regional hospital. Moreover, hyperbilirubinemia did not return in 3-month follow-up period, suggesting that adsorption therapy could facilitate regaining of balance between inflammatory process, cytokine production and bilirubin turnover.
To conclude, sepsis-related cholestasis should be considered in the differential diagnosis of jaundice in critically ill patient. We proposed diagnostic pathway in case of isolated hyperbilirubinemia (Chart 2). Further studies are needed to fully elucidate the scope of hemoadsorption therapy in case of jaundice and its usefulness to alter the outcome in ICU patient.
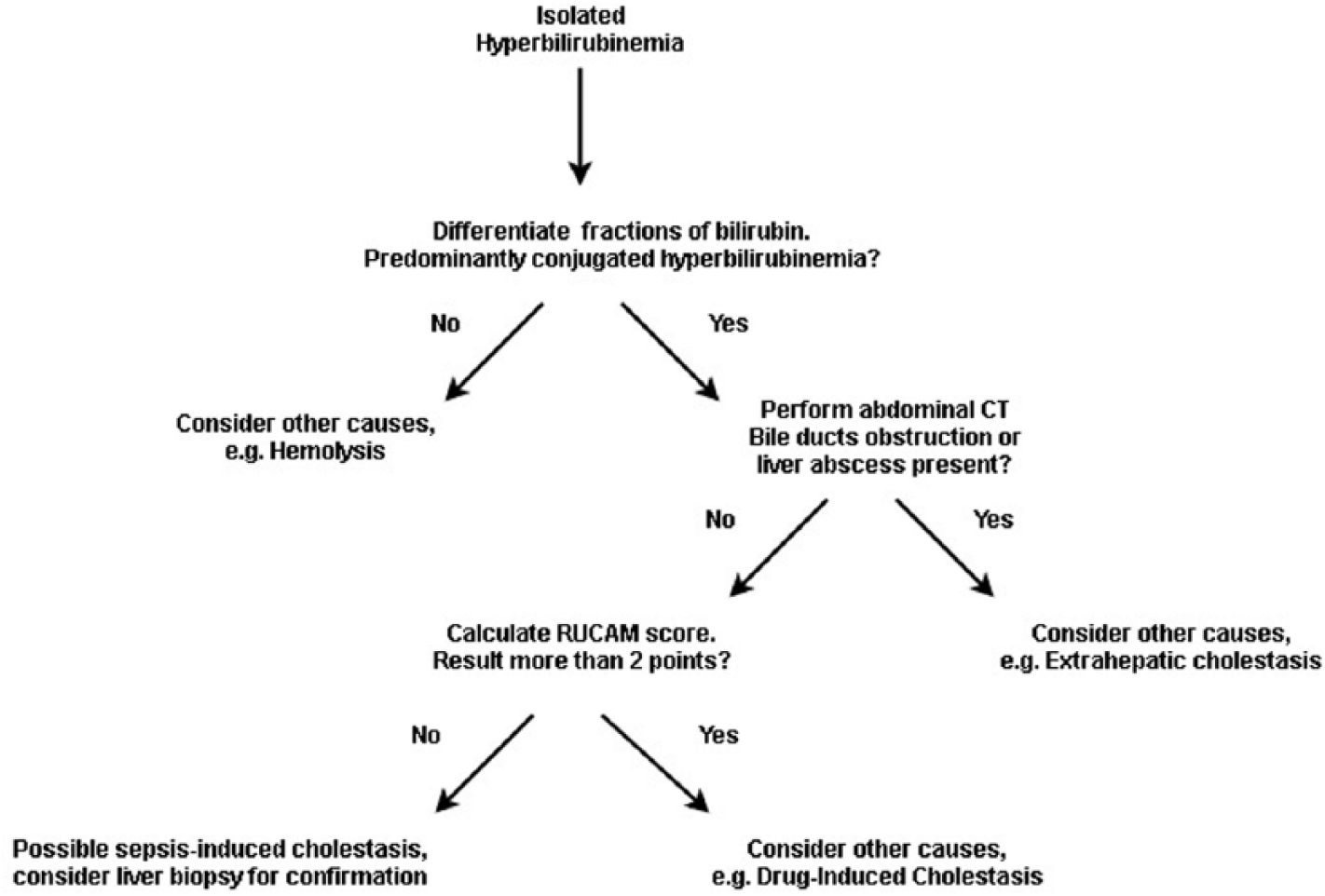
Proposed diagnostic pathway for sepsis-induced cholestasis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.