
Abstract
A systematic review of the role of extracorporeal life support (ECLS) in pediatric patients with burn and smoke inhalation injury was undertaken. A systematic search of the literature according to a specific combination of keywords to ascertain the effectiveness of this treatment strategy was conducted. A total of 14 articles out of 266 were considered suitable for the analysis in pediatric patients. The PICOS approach and PRISMA flow chart were followed for the purpose of this review. Despite the limited number of studies on the subject, ECMO in burn and smoke inhalation injury provides an additional level of support in pediatric patients leading to positive outcomes. V-V ECMO demonstrated the best overall survival of all configurations, with similar outcomes to non-burned patients. Prolonged mechanical ventilation prior to ECMO decreases survival and increases mortality by 12% with each additional day off ECMO. Good outcomes have been described for scald burns, dressing changes, and pre-ECMO cardiac arrest.
Introduction
More than 1.5 million children aged 9 years and under sustained burn injuries in the United States within one decade, with 5842 of these resulting in death. A recent retrospective study showed that approximately 3.1% of admitted children also suffered inhalation injury. 1 Thirty percent total body surface area (TBSA) burn is the cutoff point for the initiation of patho-physiological responses that start an immunologic and inflammatory cascade, with increasing morbidity and mortality risk. Additional inhalation injury or sepsis may lead to acute respiratory distress syndrome (ARDS), resulting in multiple organ failure (MOF) and shock, as well as significantly contribute to burn-related morbidity and mortality if more than 60% TBSA burn is present. 2
In many patients with severe burn and/or inhalation injury, conventional mechanical ventilation fails to provide adequate oxygenation. Respiratory or venovenous (V-V) ECMO provides oxygenation and carbon dioxide removal while the lungs can be ventilated with minimal inspiratory pressure, so called “rest settings.” 3 Cardiac or venoarterial (V-A) ECMO is used where cardiovascular support is also required. Extracorporeal membrane oxygenation (ECMO) has been successfully used to treat severe ARDS in children since the early 1990s. The use of ECMO in pediatric burn care has significantly increased over the last decade, particularly in acute respiratory failure. However, studying the risk and benefit of ECMO in pediatric burn patients is challenging since the use of ECMO in this population cannot be predicted. 4
This is the first systematic review of ECMO in pediatric burn care. This paper aims to assess and summarize the literature and available clinical data to elucidate whether there is benefit in terms of outcome associated with the use of ECMO in this demographic.
Methods
A systematic web-based literature search was conducted in Medline/Pubmed and EMBASE, using combined keywords according to established search algorithms: “ECMO” or “Extracorporeal Membrane Oxygenation” or “ECLS” or “Extracorporeal Life Support” and “burn” or “burn injury” or “burn trauma” or “major burn” or “inhalation injury.” All articles were analyzed for age, TBSA burn, type of ECMO used, number of ECMO hours and outcome in terms of mortality. Included were case reports, case series, retrospective reports, and registry analyses. Review articles, editorials and letters to the editor were excluded for low level of evidence. All available studies in the English language were included. The PICOS (participants, intervention, comparison, outcome, and study design (Table 1)) approach for the selection of clinical studies was applied following the systematic search. The literature was discussed and graded, taking the available evidence published up to and including July 31, 2022, and presented in a flow diagram (PRISMA, Table 2). The recommendations of the “Oxford Centre for Evidence Based Medicine” (OCEBM) were used for the assessment and grading of the quality of the studies. Statistics are descriptive.
“PICOS” approach for the selection of studies during the systematic search.

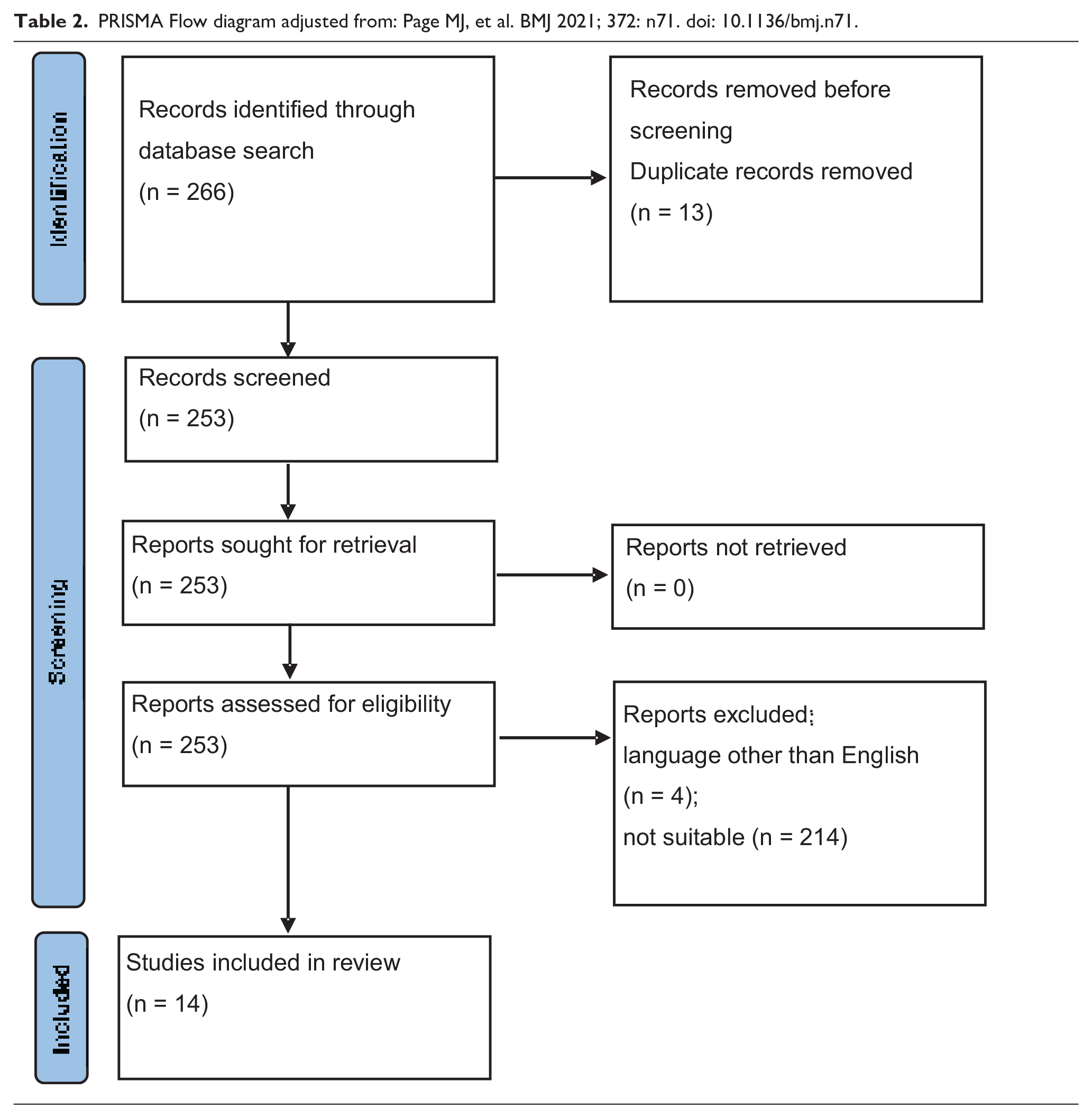
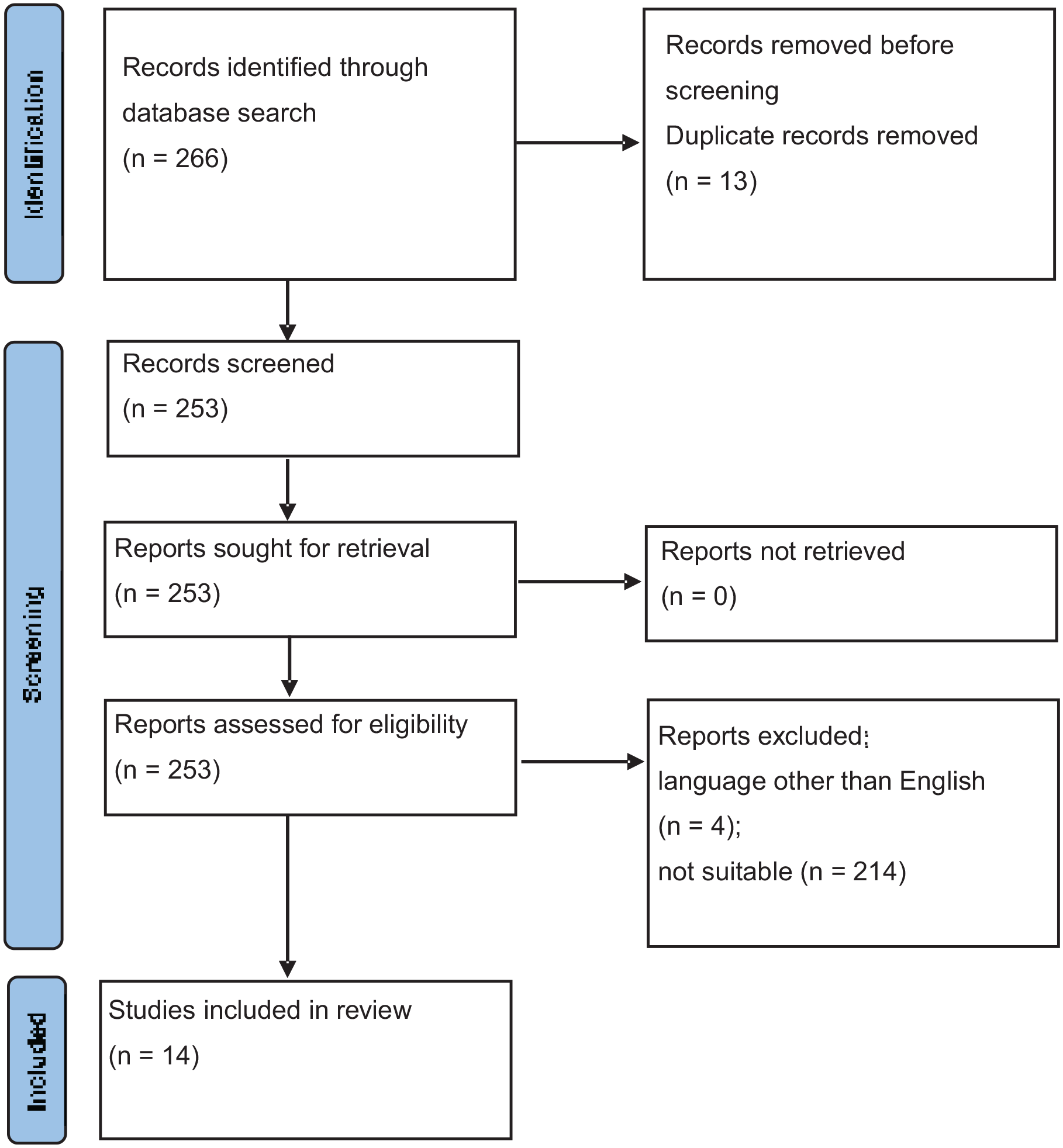
PRISMA Flow diagram adjusted from: Page MJ, et al. BMJ 2021; 372: n71. doi: 10.1136/bmj.n71.
Results
A total of 266 articles were identified of which 54 were initially selected as potentially suitable for the purposes of this study. Further review discarded additional articles and the duplicates leading to a final number of 14 articles between 1994 and 2022 to be included (Table 2). Four case reports presented single cases, two reports reported two cases each, four case series reported data on five, five, six, and 12 cases, and four investigations of the Extracorporeal Life Support Organization (ELSO) registry. Prospective randomized trials were not found. In 14 articles, 329 patients were found of which 2 were adults who were excluded. The remaining total count of pediatric patients was 327. Of these, 291 patients were part of the four ELSO registry investigations. It is highly likely that a major proportion of these patients appear redundantly in the registry analyses (Table 3).
Use of ECMO in pediatric burn care.
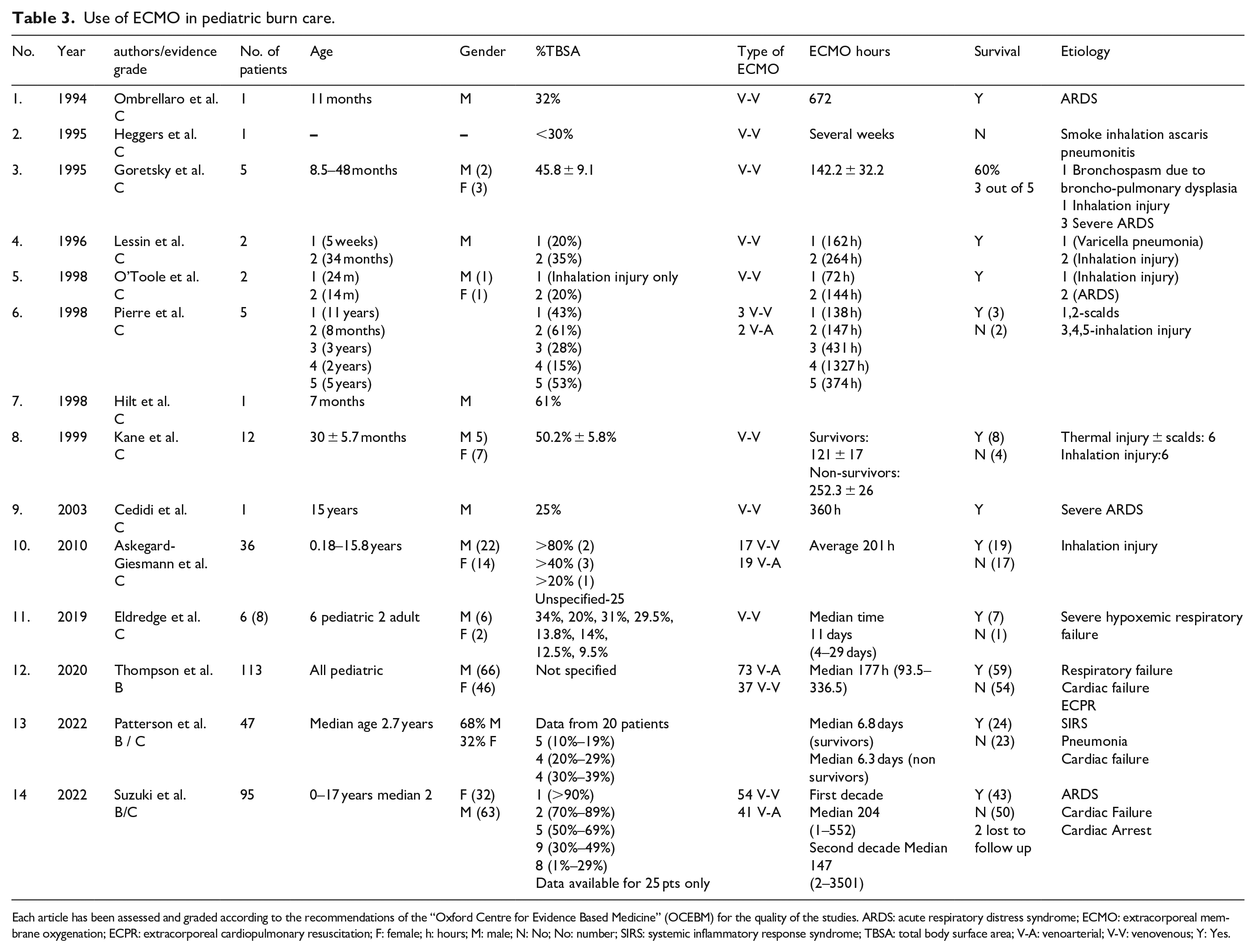
Each article has been assessed and graded according to the recommendations of the “Oxford Centre for Evidence Based Medicine” (OCEBM) for the quality of the studies. ARDS: acute respiratory distress syndrome; ECMO: extracorporeal membrane oxygenation; ECPR: extracorporeal cardiopulmonary resuscitation; F: female; h: hours; M: male; N: No; No: number; SIRS: systemic inflammatory response syndrome; TBSA: total body surface area; V-A: venoarterial; V-V: venovenous; Y: Yes.
Discussion
The use of ECMO for the treatment of smoke inhalation injury has been described as early as in 1987, when Brown et al. 5 described the successful use of V-V ECMO for the treatment of smoke inhalation in sheep. In 1996, the UK Collaborative trial of neonatal extracorporeal membrane oxygenation demonstrated that ECMO should be actively considered in neonates with severe but potentially reversible respiratory failure. 6 Even prior to this trial, an isolated case report was published by Ombrellaro et al. 7 for the successful use of ECMO in an 11-month-old for thermal injury and ARDS. At this time, mortality for ARDS in pediatric burn patients was up to 80%. In 1995, Heggars et al. 8 described the use of ECMO for respiratory failure secondary to Ascaris pneumonitis superimposed on smoke induced lung injury. Ascariasis had an additive effect on the smoke-induced lung injury, which resulted in unrecoverable respiratory failure even after several weeks on ECMO. The authors commented on the importance of additive chemotherapy, since ECMO is a bridge to allow treatment and is not a therapy itself. Subsequently, several case series were published by Goretsky et al. 9 in 1995, Lessin et al. 10 in 1996 and O’Toole et al. 11 in 1998 describing the successful use of ECMO in burn induced ARDS. All these case reports described the use of V-V ECMO for respiratory support. Goretsky reported 3 out of 5 patients surviving after ECLS was initiated with a mean age of 26 months. At the time of initiation, the peak inspiratory pressure was >56 cmH2O with FiO2 of 1.0. Lessin described 2 patients with 20% and 35% TBSA with carboxyhemoglobin levels of 26% and 30%. It was reported that anticoagulation for ECMO did not influence dressing changes. Both patients had definitive auto-grafting and were discharged home breathing room air. 9 In a case described by Cedidi and colleagues, a 15-year-old patient with burn and smoke inhalation injury who had developed five-organ failure could successfully be resuscitated with ECMO. 12
In 1998, Pierre et al. 13 described the effective use of V-A ECMO in two patients among their case series of five patients during which they had to convert from V-V to V-A ECMO due to cardiovascular instability. Their main conclusion was that children who experienced perfusion/reperfusion shock injury to the lungs after delayed resuscitation secondary to scald burns had short ECMO runs, and improved survival chance compared to ECMO for other burn injuries. These findings could be confirmed by Hilt et al., 14 who reported a 7-month-old patient who had suffered scald burns from boiling water.
In 1999, Kane et al. 15 published a case series of extracorporeal life support in 12 burn patients with a mean age of 30.3 months and a mean TBSA of 50.2% with full thickness burn of 41.8% TBSA. All patients had received highly invasive ventilation prior to institution of ECLS. However, the non-survivors had the highest ventilatory pressures. The authors suggested that early institution of extracorporeal life support before the onset of baro-trauma improves survival.
Almost 10 years later, in 2010, Askegard-Giesmann and colleagues published a 10-year review of the Extracorporeal Life Support Organization (ELSO) registry for pediatric burns patients. They suggested that the outcome from ECMO in burn patients is comparable to non-burn related respiratory failure. 16 In 2012, Asmussen et al. 17 conducted a systematic review on the use of ECMO for hypoxemic respiratory failure resulting from burns and smoke inhalation injury. Even though this publication included a mixed pediatric and adult population, it was the first of its kind in burn care. The authors suggested that ECMO run times of less than 200 h correlated with higher survival. They also found that survival was better with scald burns compared to flame burns. However, as with hypoxemic respiratory failure of any other etiology, ECMO should be considered early in burn patients before irreversible damage from fibrosis and ventilator-induced lung injury, particularly in young patients with less than 50% TBSA burn occurs.
In 2019, Eldredge and colleagues investigated a 10-year institutional database including eight patients. At ECMO initiation, the average APACHE score, SOFA score, and P/F ratio were 21, 9, and 59, respectively, and seven out of eight patients survived. 18
The most recent data comes from three different ELSO Registry reviews, published by the groups of Thompson 19 in 2020, Suzuki 20 in 2022 and Patterson 21 in 2022. Thompson et al. 19 identified 113 patients between 1990 and 2016. The highest survival (55.7%, n = 97) was found for respiratory support compared to cardiac failure (33.3%, n = 6) or extracorporeal cardiopulmonary resuscitation (30%, n = 10). Patients supported on V-V ECMO presented the best overall survival at 62.2% (n = 37). Interestingly, surgical site bleeding in burn patients were similar to other surgical patients placed on ECMO at 22.1%. Cardiac arrest prior to cannulation had significantly increased hospital mortality. In addition, other complications including the need for inotropes, presence of gastrointestinal hemorrhage, and hyperglycemia (glucose > 240 mg/dL) were associated with increased mortality. Of the patients with documented TBSA <60%, survival was 70%. Another ELSO Registry review from 1999 to 2018 for patients of 18 years and under was conducted by Suzuki et al. 20 The data were divided into two decades, the first (1999–2008) and the second (2009–2018). The authors observed that the use of ECMO increased over time, with V-V ECMO as the most common configuration. Patients with pre-ECMO cardiac arrest demonstrated significant improvement in mortality during the second decade (54.5% vs 0%; p = 0.043). Most common complications were metabolic and renal in non-survivors during the first decade, whereas cardiovascular and neurologic complication were higher in the second decade. The authors suggested that pre-ECMO cardiac arrest is no longer a contraindication for ECMO. Patterson et al. 21 investigated this registry with focus on pediatric burn patients without inhalation injury between 2010 and 2020. The authors used a multivariable logistic regression to assess the association between mortality and pre-cannulation mechanical ventilation duration before ECMO initiation. A cohort of 47 patients had a median of 2.7 years of age with a mortality of 48.9%. Their regression modeling demonstrated that each additional day on mechanical ventilation before ECMO cannulation increased mortality by 12%.
Conclusion
Evidence from this systematic review is limited due to a small number of publications with relatively low level of evidence. However, this study confirms that ECMO in burn and smoke inhalation injury does provide an additional level of support in pediatric patients. V-V ECMO presented the best overall survival of all configurations and can quickly reduce carboxyhemoglobin levels. ECMO outcomes are similar to those observed in non-burn patients. Prolonged mechanical ventilation before ECMO is associated with decreased survival, with each additional day on mechanical ventilation increasing mortality by 12%. ECMO shows good outcomes in scald burns and dressing changes have been performed safely despite anticoagulation. Pre-ECMO cardiac arrest is no longer a contraindication for ECMO. However, ECMO should not be used as a salvage treatment but rather considered an option if a positive outcome is foreseen to be a likely event.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.