
Abstract
Sleeve gastrectomy is safe and effective in patients with left ventricular assist devices (LVADs) and morbid obesity to improve candidacy for transplantation and increase survival rates. Literature describing warfarin anticoagulation in this population is limited. A single-center, propensity score-matched, retrospective cohort study was conducted to determine if sleeve gastrectomy in LVAD-implanted patients has an effect on warfarin dose requirements in the outpatient setting. Patients were eligible for inclusion if they were 18 years of age or older, underwent LVAD implant at the study center, and were discharged from the hospital on warfarin therapy. They must have at least 8 weeks of available follow-up data post-discharge. Propensity matching was utilized to identify a non-sleeve gastrectomy LVAD-only patients for comparison. A total of 96 LVAD-only patients and 48 LVAD plus sleeve gastrectomy patients were included in the final analysis. Outpatient warfarin requirements increased from baseline over time in both groups, with no significant differences between groups except at month 12, with a mean total weekly dose of 38.1 ± 21.4 mg in the LVAD only group and 46.8 ± 18.6 mg in the LVAD with sleeve gastrectomy group (p = 0.05). The sleeve gastrectomy group had a significantly lower warfarin doses per kilogram of body weight until month 6 post-discharge. The percent time in therapeutic range was significantly lower in the SG group at the 8 week, 3 month, and 6 month interval time point. There were no significant differences in the incidence of bleeding or thromboembolic events.
Introduction
Left ventricular assist devices (LVADs) are a form of mechanical circulatory support, which have improved survival and quality of life for patients with end-stage systolic heart failure.1,2 Continuous-flow LVADs require chronic anticoagulation with warfarin to prevent thromboembolic complications associated with the device. The risk of bleeding is also increased in patients with LVADs, and not simply as a consequence of anticoagulant use, but also the physiologic effects caused by the device. This includes shear stress causing platelet activation, acquired von Willebrand syndrome, and the development of arteriovenous malformations mainly in the gastrointestinal tract, thought to arise from the lower arterial pulse pressure experienced by these patients.3,4 Because of these factors, achieving a balance between prevention of bleeding and thrombosis remains challenging in LVAD-implanted patients.
Obesity is a risk factor for various diseases, and it is prevalent among patients with advanced heart failure. 5 A body mass index (BMI) >35 kg/m2 has been considered a relative contraindication to cardiac transplantation due to worse survival observed in heart transplant recipients above this threshold. This BMI threshold has resulted in obesity being a primary barrier for heart transplant candidacy in certain cases. Bariatric surgery is an effective intervention for weight loss in patients with morbid obesity who have failed lifestyle modifications. 5 Sleeve gastrectomy (SG) has been proven safe, feasible and effective to obtain weight loss for patients with LVADs to improve access for transplantation and increase survival rates.6,7
It is expected that the pharmacokinetics of warfarin post-SG will be altered with adipose tissue reduction and nutrition status, as well as physiological changes in gut absorption, pH and transit time. 8 A 2018 retrospective analysis in patients on chronic warfarin therapy undergoing SG reported a mean 23% dose reduction 1 month post-surgery. Although this was followed by a trend in increased requirements, there remained a statistically significant difference from pre-surgical warfarin doses at 12 months. 9 To our current knowledge, there is no literature available describing warfarin dosing in LVAD-implanted patients post-SG. The purpose of this study was to compare our outpatient warfarin dosing in patients who undergo LVAD implantation with SG with those that have LVAD implantation alone.
Methods
This was a single-center, observational, retrospective cohort review performed with the intent of identifying trends in warfarin requirements based on dose-response in a niche and growing population. The study was approved by the center’s institutional review board. Data was collected through review of electronic medical records.
Patients were identified for inclusion from a comprehensive list of patients implanted with a continuous flow left ventricular assist device (HeartWare HVAD, HeartMate II, and HeartMate 3) at the study center between January 1, 2016 and July 31, 2023. Those that received a concomitant SG during LVAD implantation were identified using current procedural terminology (CPT) codes. Patients were eligible for inclusion if they were ⩾18 years of age at time of implantation with an active warfarin prescription for at least 8 weeks post-discharge. Patients were excluded if they had an allergy, intolerance or contraindication to warfarin, were deceased within 30 days of implant or prior to hospital discharge, had a SG performed in a separate admission prior to LVAD implantation, or were non-adherent to warfarin therapy. Non-adherence was defined by the institution as a missed international normalized ratio (INR) lab follow-up or the documented inability to contact the patient by the medical team. Propensity score matching was utilized to assign non-SG LVAD-implanted patients to patients that underwent concomitant SG and LVAD implantation, in a 2:1 fashion. Patients were matched on the following criteria at baseline: age, INR, albumin and total bilirubin.
The primary endpoint was the comparison of mean total weekly dose requirement of warfarin at baseline (day of initial hospital discharge) and at intervals assessed biweekly thereafter for at least 8 weeks. Secondary endpoints included the time in therapeutic INR range (TTR) calculated using the Rosendaal method, 10 and the mean weight-based total weekly dose requirements. Secondary endpoints were collected at baseline, week 4, and week 8. Safety endpoints included the incidence of major bleeding, minor bleeding, and thromboembolic events. Major and minor bleeding events were defined according to the International Society of Thrombosis and Hemostasis (ISTH) bleeding definitions of major bleeding and clinically relevant non-major bleeding, respectively.11,12 Thromboembolic events were a composite of venous thromboembolism, arterial thromboembolism and pump thrombosis. Data beyond 8 weeks was collected retrospectively for all primary and secondary outcomes at month 3, 6, and 12 if follow-up data was available. Data reporting ceased after time point of patient death, heart transplantation, non-adherence to warfarin therapy, or at 12 months post-discharge.
Normally distributed continuous data were compared using independent Student’s t-test. All categorical data, including baseline characteristics and safety outcomes, were compared using χ2 and Fisher’s exact test as appropriate. Statistical significance was set at a level of p < 0.05. The primary analysis was an unadjusted comparison of mean total weekly warfarin dose between the LVAD plus SG group and LVAD-only group. In addition, a subgroup analysis of the primary endpoint was conducted on patients with an INR goal of 2–3 through the entirety of the study period. Statistical analyses were performed using Jamovi software, version 1.6.23.0 (Sydney, Australia).
Results
Overall, 335 patients were evaluated for inclusion. Of those, 33 met exclusion criteria, leaving 48 patients eligible in the LVAD plus SG group and 254 in the LVAD-only group. After propensity score matching, 48 LVAD plus SG patients were matched, resulting in 96 LVAD-only patients. Therefore, a total of 144 patients were included in the final analyses. Flow diagram of the study is illustrated in Figure 1.

Study algorithm.
There was no statistically significant difference between age, race, LVAD type or CHA2DS2-VASc score between the two groups. There were more males in the LVAD-only group compared to the LVAD plus SG group (83% vs 63%, p = 0.011). The mean weight was expectedly higher in the LVAD plus SG group compared to the LVAD-only group (114.7 kg vs 80.9 kg, p < 0.001), leading to a statistically significant difference between BMIs at 38.9 and 26.6 kg/m2, respectively (p < 0.001). Past medical history at baseline was similar between groups. The majority of patients in both the LVAD-only and LVAD plus SG groups were on aspirin therapy, while only a small but similar portion were on a P2Y12 inhibitor, 5% and 6%, respectively. A composite number of medications that could increase the INR and decrease the INR was similar between groups, and this was not reported in the table. More patients in the LVAD plus SG group were taking a multivitamin and/or nutritional supplement as compared to the LVAD only group (72% vs 35%, p < 0.05). Based on the information reported, the majority of those multivitamins or supplements in each group contained vitamin K; however, 19% of those in each group had an unreported amount. The goal INR range was 2–3 for the majority of patients in each group, although a small subset of patients had other goals documented. A complete list of baseline characteristics are shown in Table 1.
Baseline characteristics.

All values reported as mean ± SD or n (%) unless otherwise specified. p-Values reported when statistically significant.
LVAD: left ventricular assist device; BMI: body-mass index; INR: international normalized ratio; NS: not significant.
The mean total weekly dose of warfarin at baseline was numerically lower in the LVAD plus SG group (30.9 mg) compared with the LVAD-only group (34.9 mg), however this was not statistically significant. The total weekly dose continued to rise through the study period in the LVAD plus SG group where by month 12, this group had a higher weekly dose compared with the LVAD-only group (46.8 mg vs 38.1 mg, p < 0.05). When comparing patients that had an INR goal of 2–3 throughout the study period (n = 40 in LVAD plus SG, n = 82 in LVAD-only), similar results were observed with the exception of a significantly lower dose in the LVAD plus SG group at baseline (Tables 2 and 3).
Warfarin dosing results.
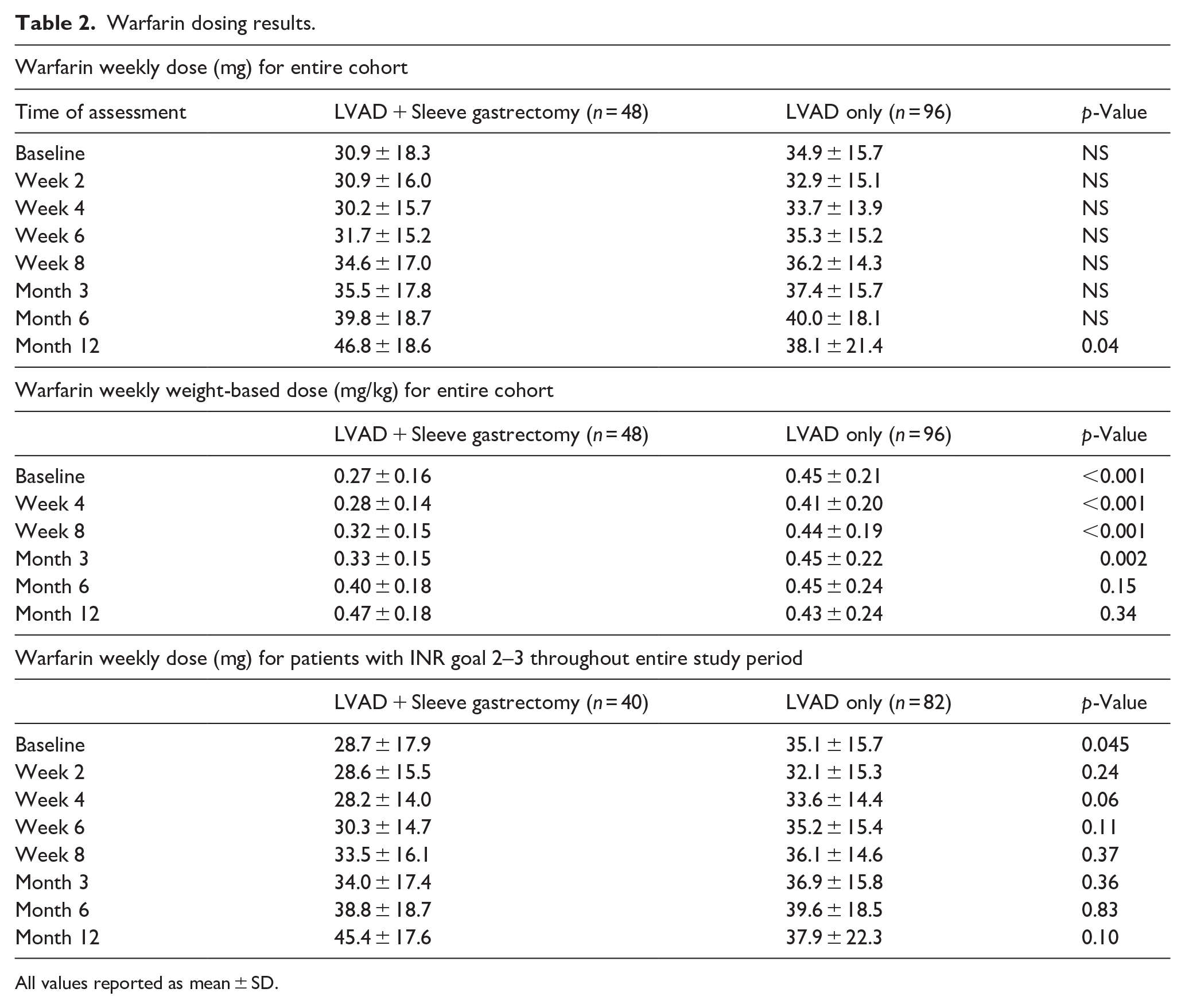
All values reported as mean ± SD.
Clinical outcomes.
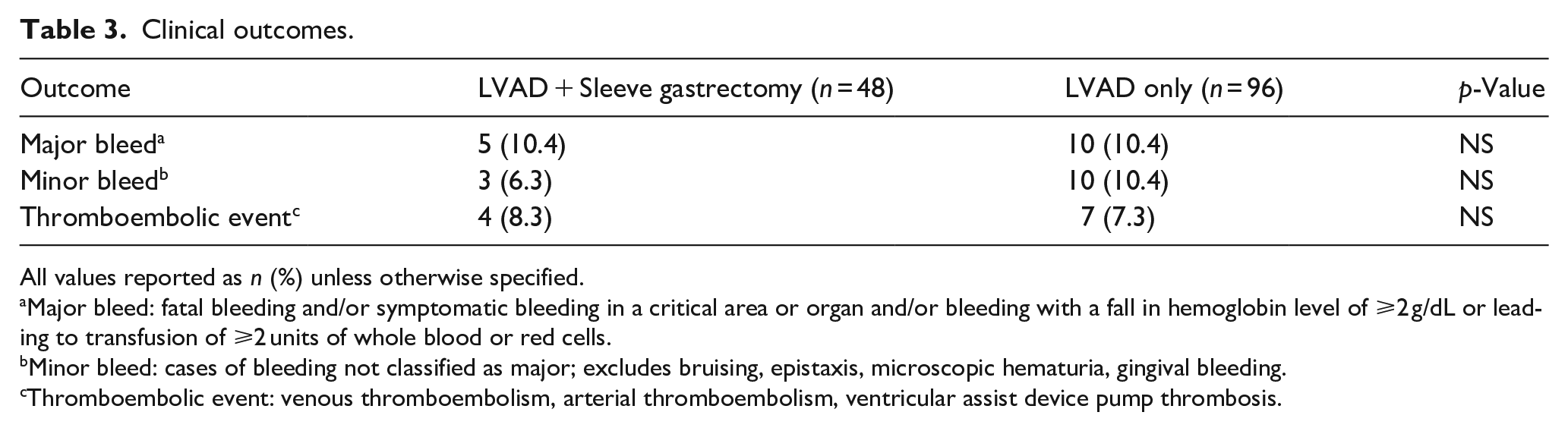
All values reported as n (%) unless otherwise specified.
Major bleed: fatal bleeding and/or symptomatic bleeding in a critical area or organ and/or bleeding with a fall in hemoglobin level of ⩾2 g/dL or leading to transfusion of ⩾2 units of whole blood or red cells.
Minor bleed: cases of bleeding not classified as major; excludes bruising, epistaxis, microscopic hematuria, gingival bleeding.
Thromboembolic event: venous thromboembolism, arterial thromboembolism, ventricular assist device pump thrombosis.
The analysis of TTR revealed that it was lower in the LVAD plus SG group throughout the study period, however this difference was observed to be statistically significant at week 8, month 3, and month 6 intervals (Figure 2).
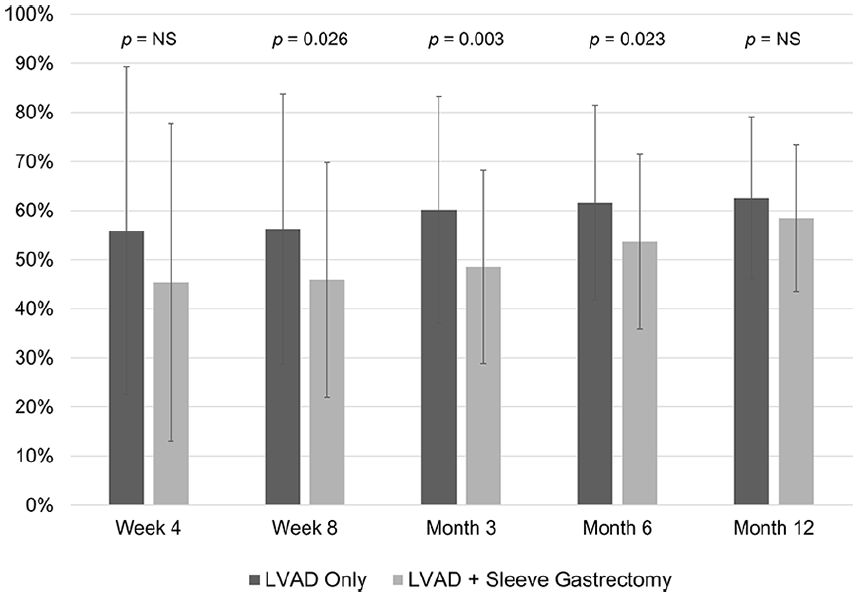
INR time in therapeutic range comparison.
To account for body weight differences and changes throughout the study period, weight-based dosing of warfarin was analyzed. Total weight-based weekly dose in the LVAD plus SG group increased from 0.27 mg/kg at baseline to 0.32 mg/kg at week 8 and 0.47 mg/kg at month 12. There was no observable trend in the LVAD-only group (Table 2). Mean body weight trends are also illustrated for both groups, with a steady decline observed in the LVAD plus SG group and a steady increase seen in the LVAD alone group (Figure 3).

Mean observed weight at assessment intervals.
There were no differences in clinical events including bleeding or thromboembolic events observed between groups for the duration of the study period. For safety, the incidence of major bleeding was 10% in each group, all documented as gastrointestinal bleeds in the LVAD plus SG group, and the majority of bleeding being intra-cranial in the LVAD-only group. There was no difference in major or minor bleeding events. A low rate of thromboembolic events were observed.
Discussion
The purpose of this study was to determine if there are identifiable trends in warfarin dose requirements following bariatric SG in LVAD-implanted patients. Our findings indicate that warfarin requirements are generally lower at baseline post-SG, especially when compared in a weight-based fashion, but by 12 months, the LVAD plus SG group require higher doses compared with LVAD-implanted patients that have not undergone SG. Prior to the study we expected the absolute difference in warfarin doses to be much lower in the LVAD with SG group, however differences including body size, nutritional supplements and vitamin therapy may all be reasons to explain why the absolute differences in warfarin dose were not significantly different. To our knowledge, there are no studies that look at warfarin requirements specifically in the LVAD population following bariatric surgery; however, the literature available on warfarin for other indications following bariatric surgery suggests there is a dose reduction in the first month post-operatively, followed by a trend toward increased dose requirements the farther out from surgery. 8 While the majority of patients included in our study were started on warfarin only after LVAD implantation, pre-procedural warfarin requirements are not available.
Patients with LVADs have historically exhibited labile INRs, leading to less time in therapeutic range and potential for increased adverse events.13 –15 This reinforces the need for frequent INR monitoring in this population. Our study noted TTR <60% in the immediate post-operative period, followed by increased percent TTR as patients were monitored farther out from surgery, which is in line with other literature. Patients with concomitant SG were observed to have lower TTR compared with those that did not undergo SG at several of the intervals assessed, indicating that these patients may require closer monitoring and consideration of other factors, including physiologic changes to the body, drug pharmacokinetics, and drug–drug interactions.
We were pleased that there was no increased incidence of bleeding or thromboembolic events in the LVAD with SG group compared to the LVAD alone group, however we must acknowledge the size of our study and lack of power analysis for these outcomes limits any ability to formulate firm conclusions related to clinical outcomes.
It is not surprising to have observed higher baseline body weights in the LVAD plus SG group compared with the LVAD-only group. These patients are more likely indicated for a bariatric procedure based on BMI, and to assist in transplantation candidacy. There was an inverse pattern observed between weight and weight-based warfarin dosing in this group. As weight decreased, the warfarin dose per kilogram of body weight increased in the LVAD with SG group. This suggests that warfarin dosing in this population is not explicitly associated with body weight, and there may be other factors that counter an expected reduction in warfarin dose that may accompany weight loss. We can speculate that nutritional status, particularly serum protein and vitamin K absorption may improve as patients recover from LVAD and SG surgery. We would also be remiss not to acknowledge that there are differences in hemocompatibility events expected based on the type of LVAD implanted, with lower events expected in Heartmate 3 implanted patients. 16 Because of this we would expect the TTR and quality warfarin management to have a lesser impact in the LVAD with SG implanted with the more hemocompatible Heartmate 3 device.
This study was performed at a large, academic medical center, and it is important to consider that patients included were followed and managed outpatient by a pharmacist-run clinic with frequent anticoagulation monitoring. We recognize that this structure is not feasible or available for all centers performing LVAD procedures, but in our experience we have seen improved TTR when compared to previous standard of care. 14 We hope that our findings illustrate the need for close INR monitoring and will encourage clinicians to identify trends in warfarin doses, to better understand this population and optimize future management.
Due to the retrospective design of this study, baseline characteristics and outcomes relied heavily on the accuracy of documentation in medical records. The ambulatory nature of the study and a less-controlled patient environment may lead to variations in outcome reporting, and in addition, consideration of patient lifestyle and adherence when interpreting the findings. Although medication and supplement information was collected, our study did not analyze the potential role of drug–drug and drug–nutrition interactions on warfarin requirements as we felt the specific vitamin and nutritional products utilized and adherence throughout the evaluation period could vary significantly in the outpatient setting. We did not distinguish between destination therapy and bridge to transplant LVAD implantation purpose between groups, thus other patient factors common to destination therapy patients may also have impacted the TTR observed within the groups. Lastly, intermittent hospitalizations throughout the study period may have affected patient’s total weekly dose requirements and percent TTR.
Conclusion
This study demonstrated lower weight-based warfarin dose requirements in LVAD patients who have undergone concomitant SG compared to patients with LVAD alone, however there is a trend toward higher absolute dose requirements by month 12. There was a more labile INR observed in the LVAD with SG population, evidenced by a reduced TTR which may predict complications and require additional follow-up.
Footnotes
Acknowledgements
None
Author contributions
Stephanie Robertson, PharmD designed and implemented the research, performed data collection, analyzed the data and wrote the initial draft of the manuscript. Elaine Chow, PharmD and Phillip Weeks, PharmD contributed to the research idea conception, supervised the project, assisted in data analysis and provided editorial comment for the final manuscript. Brian Gulbis, PharmD assisted in data collection, assisted in data analysis and provided editorial comment for final manuscript. Sriram Nathan, MD, Maria Patarroyo-Aponte, MD, Shinil Shah, DO, EdD, Kulvinder Bajwa, MD, Biswajit Kar, MD, and Igor Gregoric, MD all contributed to research idea conception, assisted in data analysis, and provided editorial comments for final manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.