
Abstract
Background:
While the cardiovascular events decreases after renal transplantation compared with patients on dialysis, it nevertheless remains higher than in the general healthy population. The aim of the present cross-sectional study was to investigate association of hypervolemia with blood pressure, and endothelial functions in kidney transplant recipients.
Methods:
Eighty-two kidney transplant patients (52 male, 30 female, mean age: 51 ± 12.8 years) with stable allograft function were investigated. 59 patients (72%) were suffering from hypertension. The volume status of the patients was determined by using bioimpedance spectroscopy (BIS) as total body water (TBW), extracellular water (ECW), and intracellular water (ICW) and by measuring serum pro brain natriuretic peptide (pro BNP). Blood pressure (BP) was assessed by 24-h ambulatory blood pressure monitoring (ABPM). Endothelial function was measured by flow-mediated vasodilation. Echocardiographic examination was also performed.
Results:
Hypertensive patients had significantly higher TBW (36.3 ± 6.3 L vs 31.7 ± 6.1 L, p = 0.004), and ECW (17.1 ± 2.8 L vs 14.7 ± 3 L, p = 0.002). ECW was correlated with nighttime systolic BP in renal transplant recipients (r = 0.26, p = 0.04). However, there was no correlation between ECW with nighttime-daytime diastolic BP and daytime systolic BP in ABPM. There was a positive correlation between ECW with left atrial diameter, and left ventricular mass index (r = 0.57, p = 0.000; and r = 0.34, p = 0.006, respectively). A significant negative correlation was found between ECW and flow-mediated dilatation (r = −0.3, p = 0.007).
Conclusion:
Increased ECW was associated with hypertension, especially nighttime systolic BP, and endothelial dysfunction in renal transplant recipients. Hypervolemia might be a contributing factor in increased cardiovascular risk in kidney transplant recipients.
Keywords
Introduction
Clinically unapparent volume expansion is an important cause for hypertension in patients with chronic kidney disease. Increased salt and water retention is an important factor for the development of hypertension especially for haemodialysis 1 and peritoneal dialysis patients. 2 However, its role in kidney transplant recipients is not clear. Kidney transplant patients have partially impaired kidney function and can be considered as early-stage chronic kidney disease. This can contribute to salt and water accumulation. Additionally, water and salt retention might occur due to using immunosuppressive drugs such as prednisolone and calcineurin inhibitors. Bioimpedance spectroscopy is a noninvasive method that has been used for volume evaluation in the patients with chronic kidney disease. A few studies have been conducted to assess volume status of the patients with kidney transplant by using BIS. 3
Cardiovascular risk is high in kidney transplant patients and is the most important cause of mortality. 4 We previously reported that endothelial functions improved after kidney transplantation in dialysis patients. However, endothelial functions were still found to be more impaired compared to the control group. 5 Hidden hypervolemia may be an important contributing factor for posttransplant hypertension and endothelial dysfunction. In the present study, we aimed to investigate the possible association of hypervolemia examined by BIS; with blood pressure measured by ABPM, endothelial function, and echocardiographic parameters.
Patients and methods
Study design
In this cross-sectional study, 82 renal transplant recipients aged over 18 years (52 male, 30 female, mean age: 51 ± 12.8 years) were included. All patients were transplanted for more than 6 months and had stable-good allograft function (serum creatinine <2.0 mg/dL). 59 patients (72%) were classified as hypertensive by the conventional, office criteria (⩾140/90) based on European Society of Hypertension guidelines, and/or taking at least one anti-hypertensive medication. 47 of the kidney recipients (57%) were suffering from diabetes mellitus. We excluded patients during pregnancy and lactation, patients with an artificial joint, a pacemaker or defibrillator, an amputated limb, and life-limiting comorbid disease. One patient was also excluded from the study due to lymphedema caused by mastectomy. Demographic features of the patients were summarized in Table 1. Informed consent has been taken from all patients to participate in the study and the study was conducted by ethical principles of the Declaration of Helsinki.
Demographic and laboratory results of the patients (N = 82 patients).
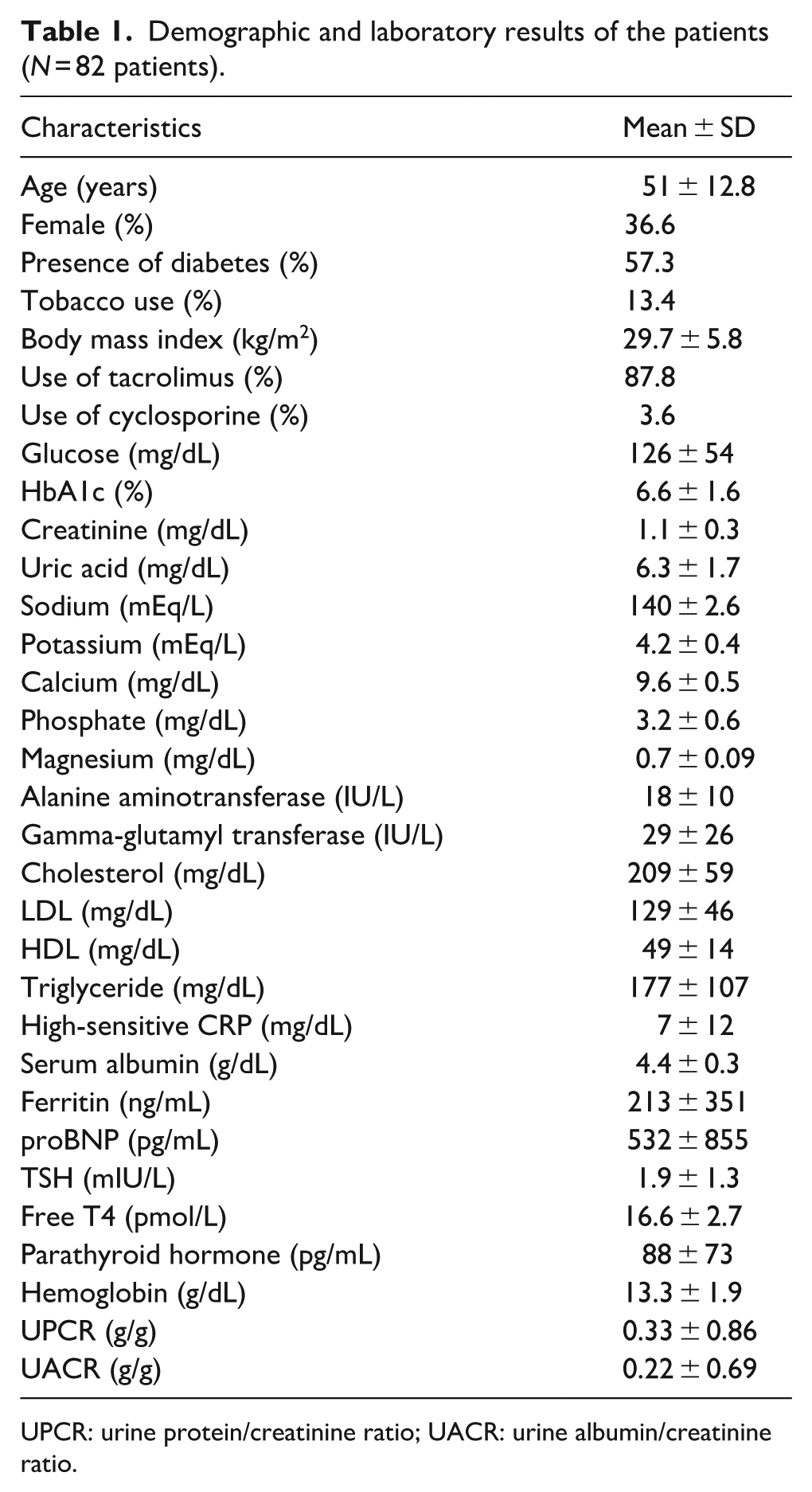
UPCR: urine protein/creatinine ratio; UACR: urine albumin/creatinine ratio.
Biochemical parameters
Serum creatinine, pro BNP, glucose, HbA1c, sodium, potassium, calcium, uric acid, phosphate, magnesium, alanine aminotransferase, gamma-glutamyl transferase, cholesterol, triglyceride, HDL, LDL, high-sensitive CRP, albumin, ferritin, TSH, free T4, parathyroid hormone, hemoglobin, urine protein/creatinine ratio, urine albumin/creatinine ratio, and tacrolimus through levels were measured by standard methods in routine clinical laboratory.
Evaluation of volume status
TBW, ECW, and ICW were measured by bioimpedance spectroscopy via determining electrical resistances (Body composition monitor from Fresenius Medical Care, Deutschland GmbH). Four electrodes were placed on the hand and foot of the contralateral side to the arteriovenous fistula. Two electrodes on the hand were located in the metacarpophalangeal joint and the corpus. Two electrodes on the foot were placed in the metatarsophalangeal joint and 6 cm apart from it. The body composition monitor works by analyzing the total body electrical impedance against an alternating current (0.2 mA) at fifty different frequencies (5–1000 kHertz). The reliability of the results was decided by the automatically calculated q index.
Ambulatory blood pressure monitoring
Ambulatory blood pressure monitoring (ABPM) (Suntech Oscar 2 Classic ABPM) has a wearable device with a blood pressure cuff that takes blood pressure readings every 30–60 min assessed blood pressure variability over 24 h. Assessed parameters were mean 24 h, daytime and nighttime systolic BP and diastolic BP. BP reports of the patients were generated with data recorded by the device.
Echocardiography examination
Echocardiography examination was performed using the Vivid 7 Echocardiography device using a middle-range frequency (3–8 MHz). Three transducer locations (“windows”) provided access to consistent imaging planes: the right parasternal location, the left caudal (apical) parasternal location, and the left cranial parasternal location. Left ventricular and atrial geometry, pulmonary arterial pressure, ejection fractions, mitral, aortic, and tricuspid valves were examined by transthoracic echocardiography.
Evaluation of endothelial function
Endothelial function was measured by flow-mediated vasodilation (GE Vivid 3 Echocardiography, 10 MHz linear probe). Brachial artery flow-mediated vasodilation was assessed for changes in brachial artery diameter after a 5-min blood pressure cuff arterial occlusion.
Statistical analysis
All analyses were performed using the SPSS 21.0 statistical software package. Continuous variables in a group data were expressed as mean ± standard deviation (mean ± SD). Categorical variables were given with numbers and percentages. Parametric tests were used in the analysis of continuous variables, since the distribution of all continuous variables was normal. Pearson correlation analysis was used to examine the relationship between continuous variables. The statistical significance level was set to p < 0.05.
Results
Eighty-two kidney transplant patients (52 male, 30 female, mean age: 51 ± 12.8 years) were examined. The baseline characteristics of the patients are shown in Table 1.
Hypertensive patients had significantly higher TBW (36.3 ± 6.3 L vs 31.7 ± 6.1 L, p = 0.004), ECW (17.1 ± 2.8 L vs 14.7 ± 3 L, p = 0.002), and increased pro BNP values (658.2 ± 938.3 pg/mL vs 225.6 ± 506.1 pg/mL, p = 0.014) compared with the normotensive group. Left atrium diameter (4.0 ± 0.4 cm vs 3.6 ± 0.3 cm, p = 0.001), left ventricular mass index (126.6 ± 26.8 g/m2 vs 100.1 ± 16.3 g/m2, p = 0.000), and septum thickness (1.4 ± 0.1 cm vs 1.2 ± 0.1 cm, p = 0.001) were also found to be significantly higher in the hypertensive group. In terms of examining endothelial function, flow mediated dilatation of hypertensive patients was found to be lower, but not reaching statistically significance (10.7% vs 9.4%, p = 0.3) (Table 2).
Comparison results of hypertensive kidney transplant recipients with normotensive kidney transplant recipients.
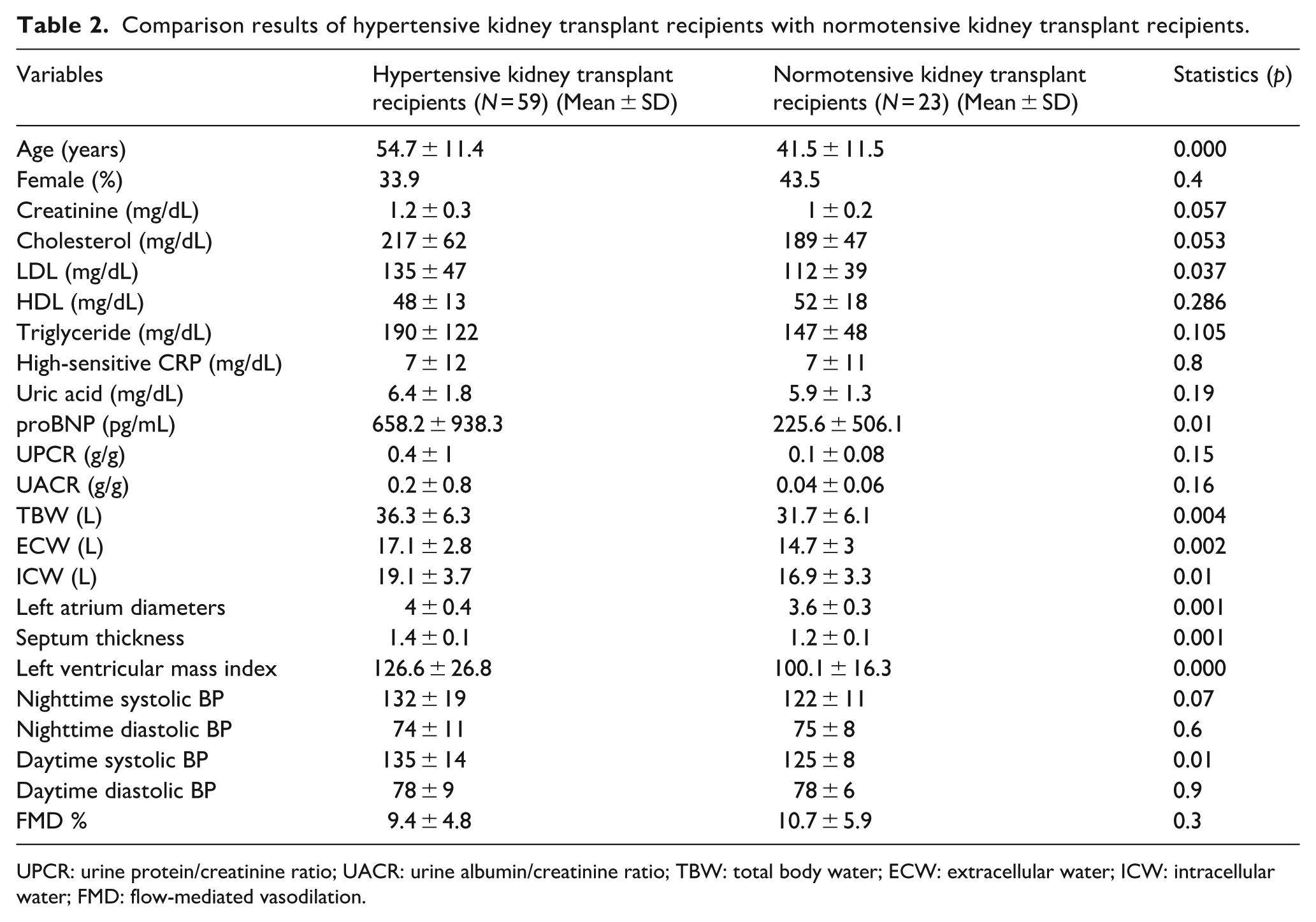
UPCR: urine protein/creatinine ratio; UACR: urine albumin/creatinine ratio; TBW: total body water; ECW: extracellular water; ICW: intracellular water; FMD: flow-mediated vasodilation.
On correlation analysis between bioimpedance parameters and ABPM, ECW was correlated with nighttime systolic BP in renal transplant recipients (r = 0.26, p = 0.04). However there was no correlation between ECW with nighttime-daytime diastolic BP and with daytime systolic BP in ABPM (r = 0.16, p = 0.2; r = −0.006, p = 0.9; r = 0.08, p = 0.49 respectively). Additionally, TBW and ICW were not associated with any parameters of ABPM. ECW was also correlated with serum pro BNP levels (r = 0.25, p = 0.03). On correlation analysis between pro BNP and ABPM, pro BNP was correlated with nighttime and daytime systolic BP in renal transplant patients (r = 0.40, p = 0.002; r = 0.28, p = 0.03). However there was no correlation between pro BNP with nighttime-daytime diastolic BP in ABPM (r = 0.23, p = 0.08; r = −0.01, p = 0.9).
ECW was also correlated with nighttime systolic BP in renal transplant recipients with diabetes (r = 0.46, p = 0.004). However there was no correlation between ECW with nighttime-daytime diastolic BP and with daytime systolic BP in ABPM of those (r = 0.16, p = 0.34; r = −0.10, p = 0.4; r = 0.27, p = 0.1 respectively).
There was a positive correlation between ECW with left atrial diameter, septum thickness, and left ventricular mass index (r = 0.57, p = 0.000; r: = 0.4, p = 0.000; and r = 0.34, p = 0.006, respectively).
There was a strong negative correlation between flow mediated dilatation with age (r = −0.38, p = 0.001), smoking (r = −0.27, p = 0.01), body mass index (r = −0.34, p = 0.003), nighttime systolic BP (r = −0.29, p = 0.02), daytime systolic BP (r = −0.29, p = 0.02), calcium (r = −0.26, p = 0.02), and pro BNP (r = −0.26, p = 0.04). A significant negative association was found between ECW and flow-mediated dilatation (r = −0.3, p = 0.007). There were no correlation between FMD with urine protein creatinine ratio (UPCR) and urine albumin creatinine ratio (UACR) (r = −0.02, p = 0.8; r = −0.06, p = 0.6).
UPCR and UACR were correlated with pro BNP (r = 0.4, p = 0.001 and r = 0.44, p = 0.000), septum thickness (r = 0.38, p = 0.004 and r = 0.43, p = 0.001), and left ventricle mass index (r = 0.34, p = 0.01 and r = 0.42, p = 0.002). UACR were also strongly associated with daytime and nighttime systolic BP (r = 0.36, p = 0.01 and r = 0.39, p = 0.004), while were not correlated with daytime and nighttime diastolic BP (r = 0.27, p = 0.055 and r = 0.26, p = 0.06).
Discussion
The most common cause of death in kidney transplant patients is still cardiovascular reasons. Hypertension is common in this group of patients, and transplant renal artery stenosis, used immunosuppressive drugs such as calcineurin inhibitors, corticosteroids, and decreased nephron mass are implicated. Role of hypervolemia on hypertension in patients with advanced stage of CKD such as hemodialysis and peritoneal dialysis is well known.2,6 However, there are limited studies examining the relationship between hypertension and volume in kidney transplant recipients.
Sezer et al. 3 found TBW and ECW were significantly correlated with office systolic BP in the kidney transplant recipients who were using ⩾1 antihypertensive treatment. In the present study, blood pressure has been examined by ABPM and it was primarily aimed to investigate the relationship between the main component of the 24-hour ABPM profile and ECW in adult transplant recipients. Among the various BP metrics, nighttime systolic BP was found correlated with ECW (Figure 1). Consistent with these findings, serum pro BNP level was also correlated with nighttime systolic BP in addition to daytime systolic BP. Correlation between ECW and nighttime systolic BP was more powerful in diabetic patients. Patients with diabetes are more prone to hypervolemia due to the increased Na reabsorption along with glucose in proximal tubule. In fact, it has been shown that ECW volume decreases with the use of SGLT2 inhibitors in diabetic patients. All these findings suggested that hidden hypervolemia was associated with increase in systolic BP especially night-time in renal transplant recipients which is more prominent in diabetic patients. It was reported that night-day BP ratio rather than office BP is the stronger correlates of an indicator of target-organ damage in kidney transplant patients. 7 For that reason, salt restriction or decrease of ECW by using medications such as SGLT-2 inhibitors might have significant impact on target organ damage and cardiovascular mortality in kidney transplant recipients as well as shown in diabetic general population. There is no study reporting the relationship between volume measured by BIA and blood pressure examined by ABMD in kidney transplant recipients.
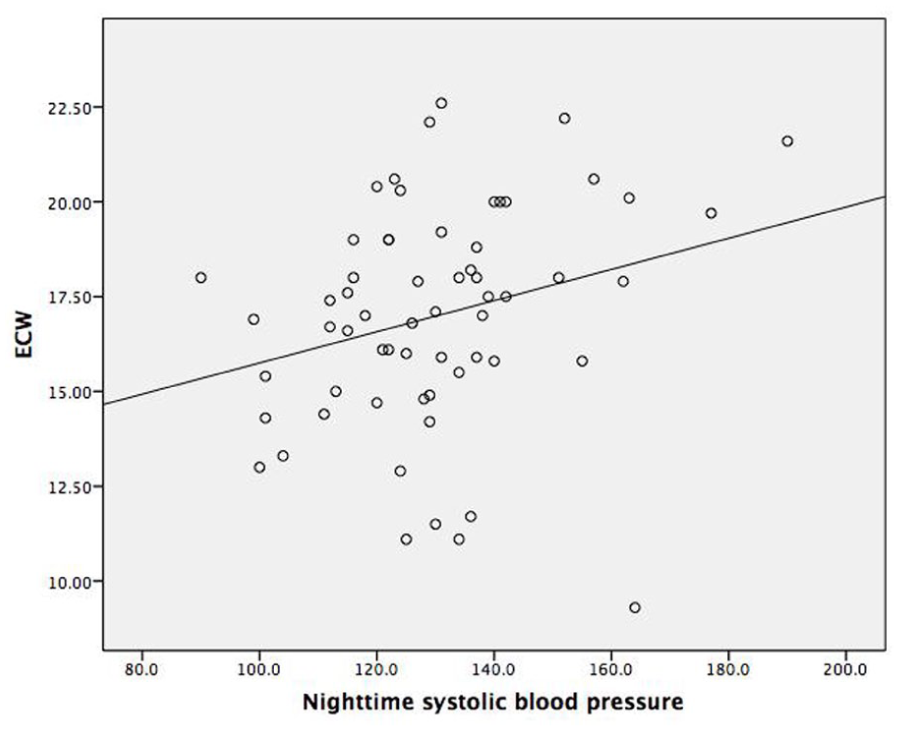
Nighttime systolic BP was found correlated with ECW.
Although endothelial function improves after kidney transplantation, endothelial dysfunction is also present in this group of patients. In a previous study performed in pediatric kidney transplant recipients, ECW/TBW was found to be an independent factor of the ambulatory arterial stiffness index, which reflects volume and pressure dependent load of arterial system. 8 In the present study, endothelial function was evaluated by measuring FMD. Significant negative association was found between ECW and FMD (Figure 2) suggesting that fluid retention may influence endothelial function. Consistent with this finding, there was also strong negative correlation between pro BNP and FMD. Improvement in endothelial dysfunction in kidney transplant recipients may be associated with improvement in volume status as well as uremia.
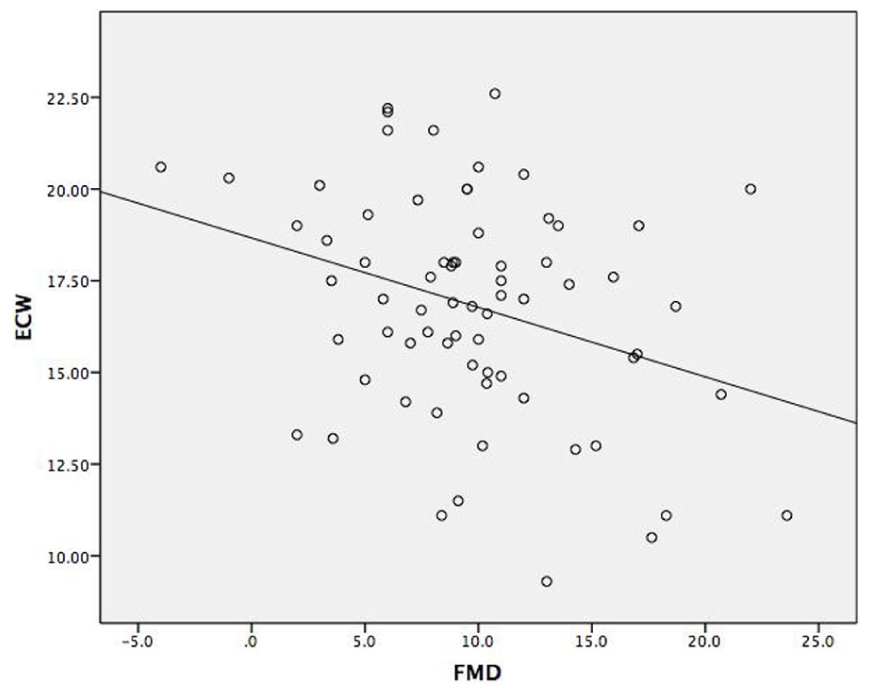
Significant negative association was found between ECW and FMD.
In conclusion, increased ECW was associated with nighttime systolic BP, left ventricular hypertrophy, and endothelial dysfunction in renal transplant recipients. Hypervolemia might be a contributing factor in increased BP and endothelial dysfunction in this group of patients.
Footnotes
Author contributions
Conceptualization and design: Seda Safak Ozturk, Alaattin Yildiz
Data collection and analysis: Seda Safak Ozturk, Nadir Alpay, Derya Baykiz, Ahmet Burak Dirim, Nurana Garayeva, Ahmet Kaya Bilge, Alaattin Yildiz
Manuscript writing: Seda Safak Ozturk, Alaattin Yildiz
Critical revision of the manuscript: Alaattin Yildiz
Data availability statement
The authors declare that data supporting the findings of this study are available.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics
The patients were thoroughly informed about the study, and their consents were obtained. Since no interventions were performed on the patients, an ethics approval was not required. All procedures performed in the study were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.