
Abstract
Background:
The CROES Nephrolithometry nomogram, S.T.O.N.E. Nephrolithometry Score and Guy’s stone score were introduced for stratification of kidney stones disease on the basis of quantitative stone burden and its distribution. Till date there has been very limited data on head to head comparison of the existing scoring systems. Comparison and analyses among the scoring system helps in further refinement of these systems along with development of new more effective and broadly acceptable nomogram.
Objective:
Predictability of the stone-free status (SFS) and post-operative complication after PCNL by various scoring systems (The CROES nomogram, S.T.O.N.E. nephrolithometry score and Guy’s stone score).
Materials and Methods:
Total 100 adult patients underwent PCNL after considering inclusion and exclusion criteria. All patients underwent Preoperative NCCT scan, investigations of blood (Hb%, PCV, bleeding and coagulation profile, urea, and creatinine), and urine (RE/ME and C/S), Postoperative X ray KUB/NCCT.
Results:
ROC curves were developed for each scoring system to determine the accuracy to predict stone free status. We found CS had significantly higher AUC than other scoring systems [p-value for CS vs GSS = 0.0091 & CS vs SS = 0.000]. So CS has higher accuracy to predict stone free status. None of the scoring system had shown significantly higher AUC than other scoring system in predicting complication.
Conclusion:
CROES Nephrolithometry nomogram is most accurate to predict preoperative stone-free rate. All scoring systems can equally predict perioperative complications and other variables.
Introduction
Percutaneous nephrolithotomy (PCNL) is procedure of choice for renal stone treatment with very low incidence of serious adverse events.1,2 Kidney stone complexity assessment by computed tomography (CT) Scan has become common practice. CT scan image provides accurate stone size estimation along with its distribution in pelvicalyceal system, and pelvicalyceal anomalies if any.
The S.T.O.N.E. Nephrolithometry Score, 3 and the CROES Nephrolithometry nomogram, 4 The Guy’s stone score 5 were introduced for stratification of kidney stone disease on the basis of stone burden, location and its complexity. These scoring nomogram helps in disease categorization tools that ultimately improves patient counselling regarding post-operative outcome and stone clearance and also helps in surgical planning.3,5
Till date there has been very limited data on head to head comparison among existing scoring nomograms. Comparison and analyses of among the scoring system helps in further refinement of these system along with development of new more effective and broadly acceptable nomogram. Thus, we have compared these scoring nomogram for post-operative outcome of PCNL.
Aims and objectives
Primary outcome was ability to predict the stone clearance after PCNL among the scoring systems (CROES nomogram, S.T.O.N.E. nephrolithometry score and the Guy’s stone score). Secondary outcomes were the ability to predict peri and intra operative variables like fluoroscopy time (FT), scope time (ST) procedure time (PT) and length of hospital stay (LOS) and post-operative using modified Clavien-Dindo system.
Materials and methods
Our study design was hospital based prospective observational study conducted in the department of Urology in a tertiary care hospital of eastern India. Total 100 patients, who underwent PCNL during study period were assessed after meeting study eligibility criteria and taking informed written consent. Inclusion criteria were all adult patient > 18 years, patients undergoing PCNL and exclusion criteria were patients without pre-operative NCCT scan of the abdomen, age < 18 years, pre-operative ureteral stent or nephrostomy tube placement in ipsilateral kidney, staged PCNL procedures and patients who had underwent any additional procedure in the same setting. All patients underwent preoperative NCCT scan, investigations of blood (Hb%, PCV, bleeding and coagulation profile, urea, creatinine) and urine (RE/ME and C/S), postoperative X ray KUB/NCCT. Demographic profile of the patients [comorbidities, BMI (Body Mass Index), and preoperative blood levels] were recorded. Stone characteristics were documented for each stone. CROES score, STONE score and Guy’s stone score were calculated for all patients. All PCNL procedures were done in standard prone position technique. Perioperative data [Procedure time (PT), Scope Time (ST), Fluoroscopy Time (FT), hospital stay and post-operative complications if any (modified Clavien-Dindo grading system)] were recorded. Stone free rate according to postoperative x-ray KUB/NCCT (for radiolucent stones).
Statistical analysis
Data was compiled in Excel spread sheet to prepare the master chart and then analyzed with MedCalc17.9.6. IBM SPSS Statistics 23.0. Categorical data were analyzed using “Pearson Chi-Square” test and continuous data were analyzed using Unpaired t-test. “General Linear Model” was applied for “Tests of Within Subject Effects” with a good fit to the present data (Mauchly’s Test of Sphericity). Mann-Whitney U-test done for ordinal data. Area under curve (AUC) for each scoring systems for ability to predict stone clearance status and post-operative complications were calculated from receiver operating characteristics (ROC) curves and compared. All tests of significance were calculated at 5% absolute precision with p-value of < 0.05.
Result
In our study, we had included total 100 patients after matching inclusion and exclusion criteria. The demographic profile our patients and stone characteristics of them are furnished according to the clearance status in Table 1.
Profile of patients and characteristics of stones.
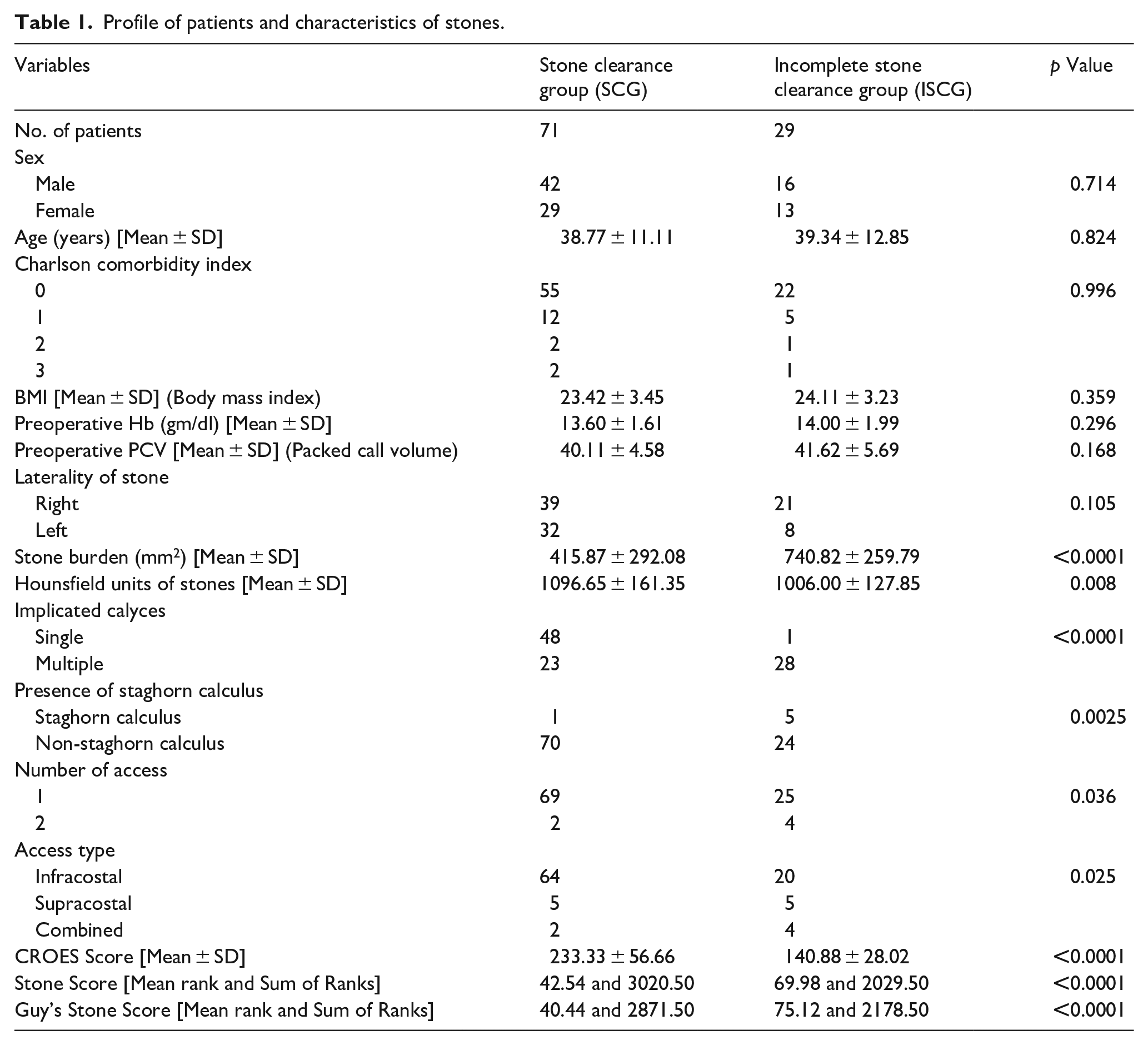
Overall stone clearance rate after PCNL in our study was 71%. Most of our patients were male (58%). We divided our patients into two groups according to stone clearance status. Both the groups were statistically equivalent in terms of sex distribution, age, BMI, comorbidities, preoperative hemoglobin levels and laterality of stones. Presence of staghorn calculus, involvement of multiple calyces and higher stone burden were significantly higher in residual stone group; whereas CROES score, Hounsfield units of stones, single access and infra-costal access during operation were significantly higher in stone free group. Stone clearance rate of each scoring nomogram were calculated and shown in Table 2.
Stone free status of various scoring nomogram.
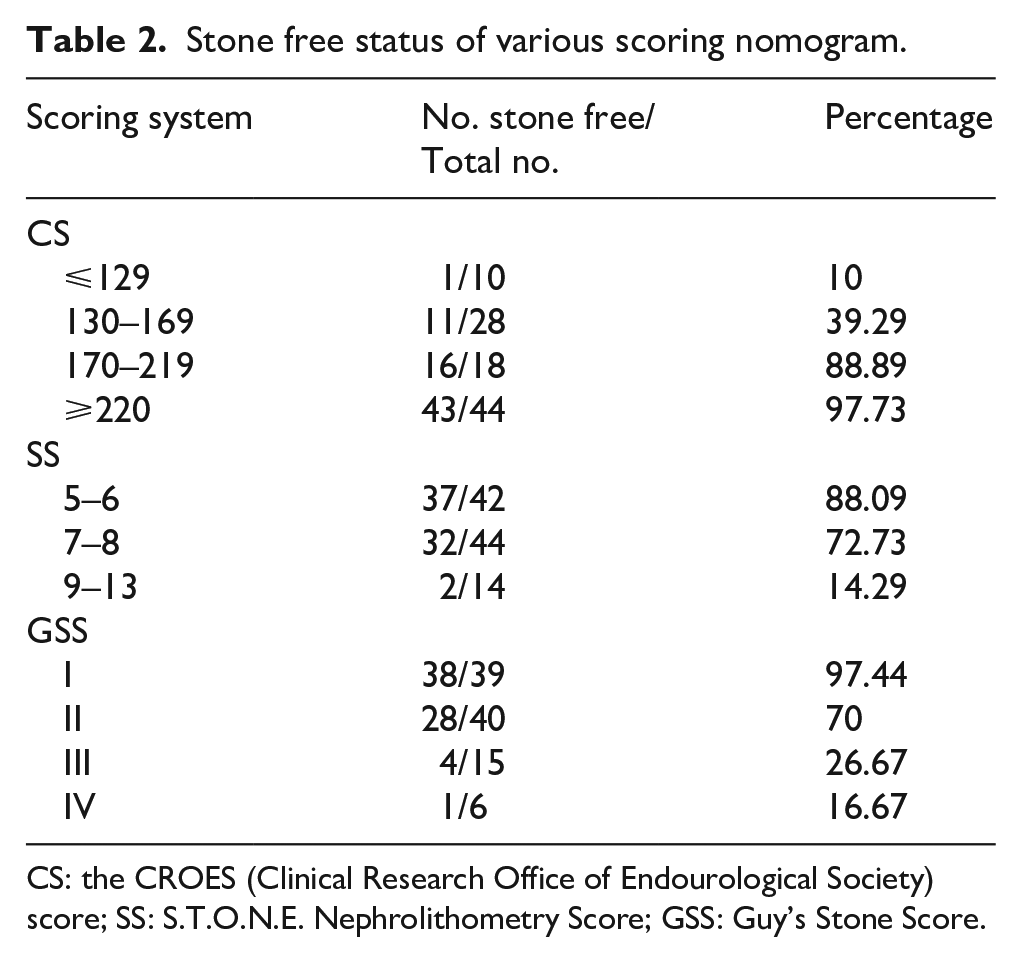
CS: the CROES (Clinical Research Office of Endourological Society) score; SS: S.T.O.N.E. Nephrolithometry Score; GSS: Guy’s Stone Score.
ROC curves was generated to determine the accuracy to predict stone free status (Figure 1(a)) for each scoring system. We found CS had significantly higher AUC than other scoring systems. So CS has higher accuracy to predict stone free status. Now ROC curves were developed for each scoring systems to determine the accuracy to predict complications (Figure 1(b)). None of the scoring system had shown significantly higher AUC than other scoring system in predicting complication.
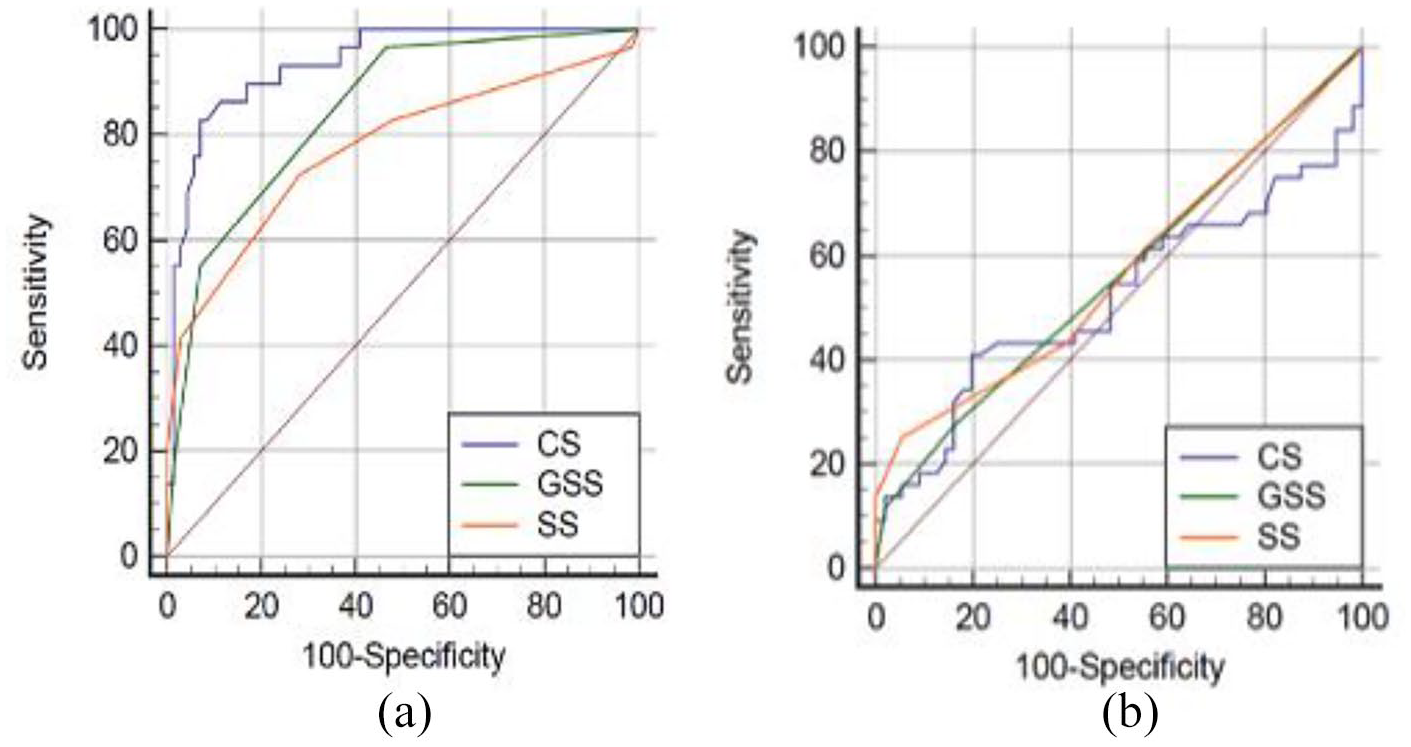
(a) ROC for scoring systems for predicting SFS and (b) ROC for scoring systems for predicting complications.
Our patients were then evaluated for procedure time (PT), scope time (ST), fluoroscopy time (FT), hospital stay and post-operative complication rate (modified Clavien-Dindo Classification) among the different scoring system group. Results are shown in Table 3.
Peri-operative variable And length of hospital stay among different scoring system group.
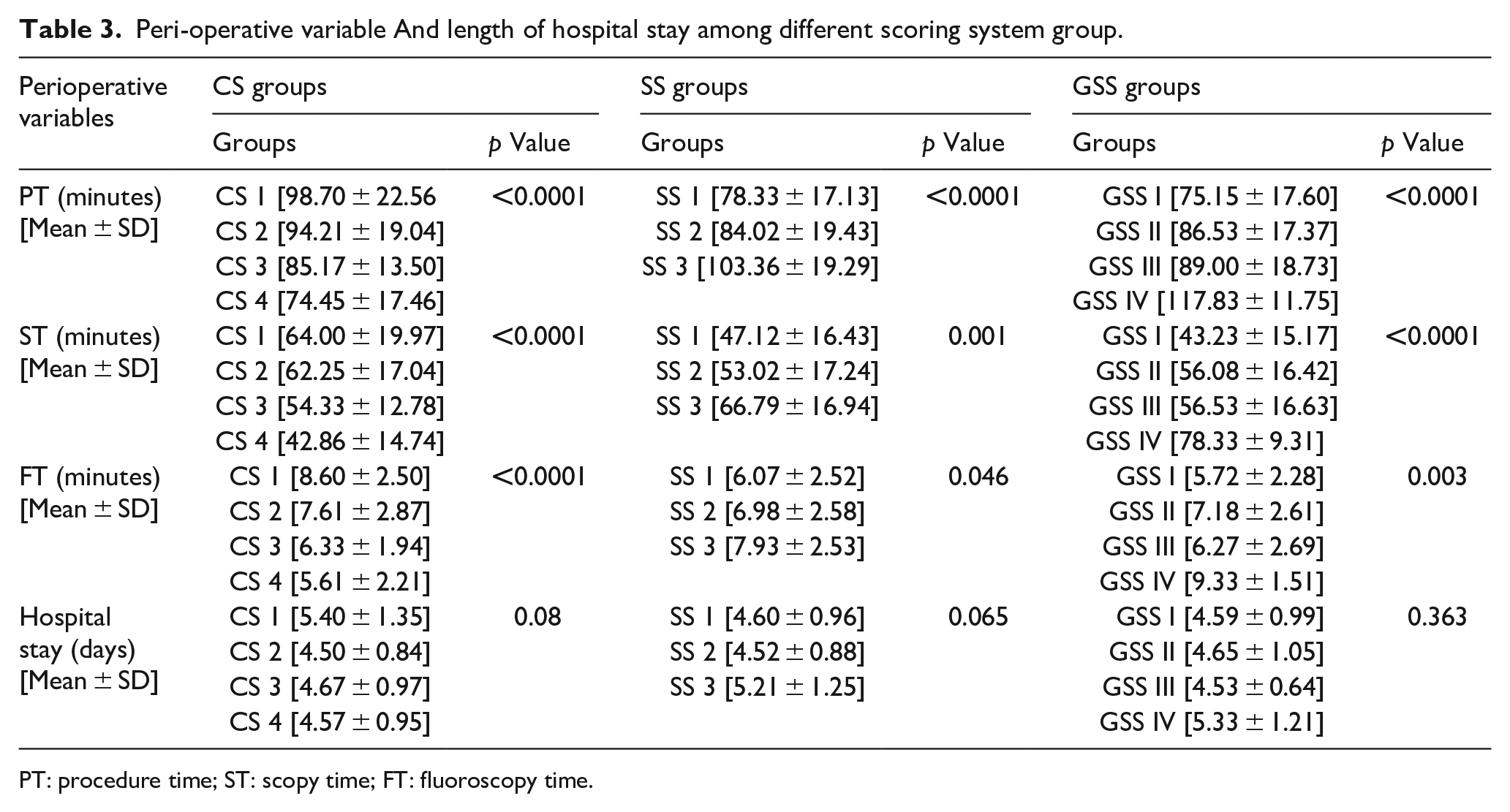
PT: procedure time; ST: scopy time; FT: fluoroscopy time.
Discussion
Although there are different developmental concepts for all three scoring systems, these scoring systems are developed for disease stratification tools, predictability of stone free status and postoperative complication along with better patient pre-operative counseling.4–6 Combining CROES nomogram (CS), S.T.O.N.E. score (SS), Guy’s stone score (GSS), comprises 11 variables, out of that only four are shared by all, those are stone size, location, number, and staghorn status. The non-shared variables (number of stones, renal anatomy, stone density, tract length, past treatment history, renal pelvic obstruction case volume per year, and spinal abnormality or injury) are included separately in scoring system. Abnormal pelvicalyceal anatomy and diverticular stone has been included only in GSS. However, from large scale study there was no association between abnormal renal anatomy and inferior surgical outcomes.7,8
We analyzed these scoring systems in a single cohort of subjects who underwent PCNL. Although analysis and direct comparison of scoring nomogram is complex due to its heterogenous nature, these can be compared using reliable statistical methods in single cohort.
In contrast to previous study, our study shows CROES score has more predictive capacity of SFS than other two systems. This discrepancy might be due to the fact that each nomogram was developed based on specific cohort of patients tested, which adds an intrinsic bias favoring predictability. Similar to previous studies, stone size remains most consistent factor to predict perioperative complication and stone free status. 8
In addition to the primary outcome, three scoring systems were significantly associated with intra-operative outcomes (PT, ST, and FT). Previous study showed that it is the urologist’s decision to use the preferred scoring system as all three systems have equal predictive abilities. In our study, CROES nomogram showed its clear superiority over other systems in respect to the secondary outcomes.
In few previous seminal studies external validation of the GSS was reported and this score effectively predicts SFS.4,9–12 Inter-observer reliability found to be excellent between GSS and S.T.O.N.E. score.11,13 Kumar et al. 14 concludes that CNN is rather comprehensive scoring system in comparison to GSS with good risk stratification for residual stone after PCNL with disadvantage of cumbersome to use in daily clinical practice.
In our study, none of scoring systems was found inferior than other in predicting post-operative complication. The optimal scoring system should be easy to be implemented, comprehensive and reproducible for standard reporting and comparison in all case.
Labadie et al. 15 concluded that SS is comprehensive with accurate risk stratification and easy applicability than other nomogram because it can be remembered with simple acronym. Since NCCT is investigation of choice for diagnosis and management of urolithiasis, SS seems to be easily implementable with uniform reporting. 10
In contrast recent study by Singla et al. 16 shows all three scoring systems have equal predictability for SFS and post-operative complications. An abbreviation of the S.T.O.N.E. score (S.O.N. score), was proposed by them and it seemed to be equally predictive.
The Table 4 shows results of different Comparative studies of CROES nomogram, S.T.O.N.E. score and Guy’s stone score.
Results of different comparative of CROES nomogram, S.T.O.N.E. score and Guy’s stone score from various study.

Possible limitations of study were exclusion of patients with nephrostomy tube or ureteral stent placed pre operatively and prior ipsilateral surgery. Outcome of PCNL in these selected groups of patients is variable and complex. Larger multi-institutional prospective studies are needed to determine a single best scoring system.
Conclusion
Preoperative NCCT scan is an important tool for diagnosis and decision making. CROES Nephrolithometry nomogram is most accurate to predict preoperatively stone-free rate. All scoring systems can equally predict perioperative complications and other variables. The Nephrolithometry scoring systems help to stratify the complexity of PCNL. These help in better patient counselling preoperatively about need for ancillary treatment.
Footnotes
Author contributions
Souvik Chatterjee: Conception, Design, Materials, Data collection and processing, Analysis and Interpretation, Writing. Anand Abhishek: Materials, Analysis and Interpretation, Writing, Literature Review. Kaniska Samanta: Materials, Data collection and processing, Writing. Anupama Ghosh: Analysis and Interpretation, Writing, Critical Review. Soumendra Nath Mandal: Supervision, Writing, Critical Review. Dilip Karmakar: Design, Supervision, Critical Review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics committee approval
Approved by Institutional ethics committee.
• Institute name—Calcutta National Medical, Kolkata, India
• Approval number—CNMC/57/2015
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article