
Abstract
Background:
PCNL outcomes among urologists are different because of the vast heterogeneity in the methods for clinical, academic characterisation and evaluation of surgical outcomes of nephrolithiasis. So assessing the preoperative factors that affect SFR (Stone Free Rate) and complications is critical. Heterogeneity in reporting of PCNL outcomes among different centres has led to the invention of nephrolithotomy scoring systems based on preoperative parameters to better counsel patients contemplating PCNL. The Guy’s stone score, CROES nomogram and the S.T.O.N.E score are seen as predictors of stone-free status (SFS) and complications after PCNL. No universally accepted stone scoring system for predicting SFR and complications after PCNL exists. This is a prospective observational study to compare and analyse the existing stone scoring systems (SSS) and to assess the best parameters to predict PCNL outcomes concerning SFR and complications.
Methods:
This study is done in a tertiary level institute in eastern India which included 200 patients who underwent PCNL from November 2019 to November 2021. The relevant operative parameters were documented and compared to the preoperative factors with the help of nephrolithotomy scoring systems.
Results:
The Guy score, CROES nomogram and S.T.O.N.E. score were accurate in predicting the SFR in patients undergoing PCNL. A new IPGMER preoperative stone scoring system based on the most relevant parameters could be used as an alternative to predict SFR and complications in PCNL.
Conclusion:
The Nephrolithometry scoring systems are simple, straightforward and easily reproducible systems to classify the severity of nephrolithiasis and to stratify the complexity of PCNL.
Keywords
Introduction
With the advancements of science and technology the management of kidney stones has undergone a paradigm shift from open surgery to endo-urology. Percutaneous Nephrolithotomy (PCNL) has now become the sheet anchor for management of kidney stones. 1
As per the European Association of Urology (EAU) guidelines the preferred treatment option for larger renal calculi (>2 cm) is PCNL. It is a safe and minimally invasive procedure for removal of renal calculi with low incidence of major complications.2,3 Since its introduction in 1976, PCNL is constantly evolving. The techniques and equipment have changed considerably, improving patient outcome, decreasing complications and morbidity. Outcome of PCNL among urologists varies as each characterises the stone complexities differently and in turn the post-operative results too. So a uniform system to compare the preoperative factors that predict SFR (Stone Free Rate) as well as development of post–operative complications is necessary. 1
Academic reporting of PCNL outcomes among different centres have not been uniform and therefore it has recently led to the invention of stone scoring systems (SSS) based on certain preoperative factors to better counsel patients considering PCNL. 2 The Guy’s stone score (GSS), the S.T.O.N.E.(stone size, tract length, obstruction, number of involved calices and essence) score and the Clinical Research Office of the Endourological Society(CROES) nomogram have often been advertised as the predictors of stone clearance and event free recovery after PCNL. 3 A uniform SSS is therefore essential for patients information, operative decision making and predicting the outcomes of PCNL. 4
However till now there is no universally accepted SSS for PCNL. Different clinical studies indicated that there are some advantages as well as disadvantages of one system to another. Also there is no uniform opinion on how to grade the post PCNL complications. A modified Clavien-Dindo system has been used in various studies to classify the perioperative complications in urologic surgeries.
This is a prospective observational study to compare and analyse the existing stone scoring systems (SSS) and to assess the best parameters to predict PCNL outcomes concerning SFR and complications.
Material and methods
This is a prospective observational study done in a tertiary level institute in eastern India which included 200 patients with renal calculus who underwent PCNL. Duration of the study was from November 2019 to November 2021. Patients aged ⩾12 years were included for analysis in this study. Patients with a preoperatively placed nephrostomy tube in ipsilateral kidney, patients who had undergone any other open, laparoscopic or endoscopic procedure in the ipsilateral kidney or patients with a post admission infective urine culture were excluded from this study.
All patients who were admitted for PCNL underwent preoperative NCCT/ CT Urography scan for evaluation of their stone burden. Guy’s stone score (GSS), STONE score (SS) and CROES score were recorded for each patient according to their history and investigations. Cumulatively the GSS, SS and the CROES nomogram share four variables such as stone size, number, location and staghorn nature of the stone. The other parameters such as stone density, urinary tract obstruction, previous operative history, tract length, case volume per year and aberrant anatomy were incorporated separately. Along with these intra and perioperative data was also recorded. Surgical procedure was performed as per the standard hospital protocol. PCNL was performed by different urologists practising at our institute. We performed standard prone and supine PCNL. We used 18 G diamond tip needle for initial puncture under fluoroscopic guidance. We used a hydrophilic Terumo guidewire over which serial dilatation using metallic Alkens dilators was done. We preferably used a 24 F Amplatz sheath as working channel. For staghorn and partial staghorn stones we mostly used 28–30 F Amplatz sheath. We used a 20 F Wolf Nephroscope to visualise the stones. Fragmentation of stone was done by pneumatic lithotripter (Swiss LithoClast). For stone extraction we use biprong and triprong forceps. 0.9% normal saline was used as the irrigant. Post-operative stone free status was determined on absence of radio-opaque shadow or clinically insignificant stone (<4 mm) on postoperative X-ray KUB/NCCT KUB. Any subsequent post-operative complications were also enlisted in the master chart.
All the data collected were coded and documented in Microsoft Excel sheet which was re-checked and analysed using SPSS statistical software version 22. Normality of distribution was checked using Kolmogorov-Smirnov test. Receiver operating characteristics (ROC) curves were generated for comparing the area under curve (AUC) depicted by each scoring systems for prediction of stone free status and complications and for finding out the diagnostic characteristics. A p-value of <0.05 was considered to be statistically significant.
Results and analysis
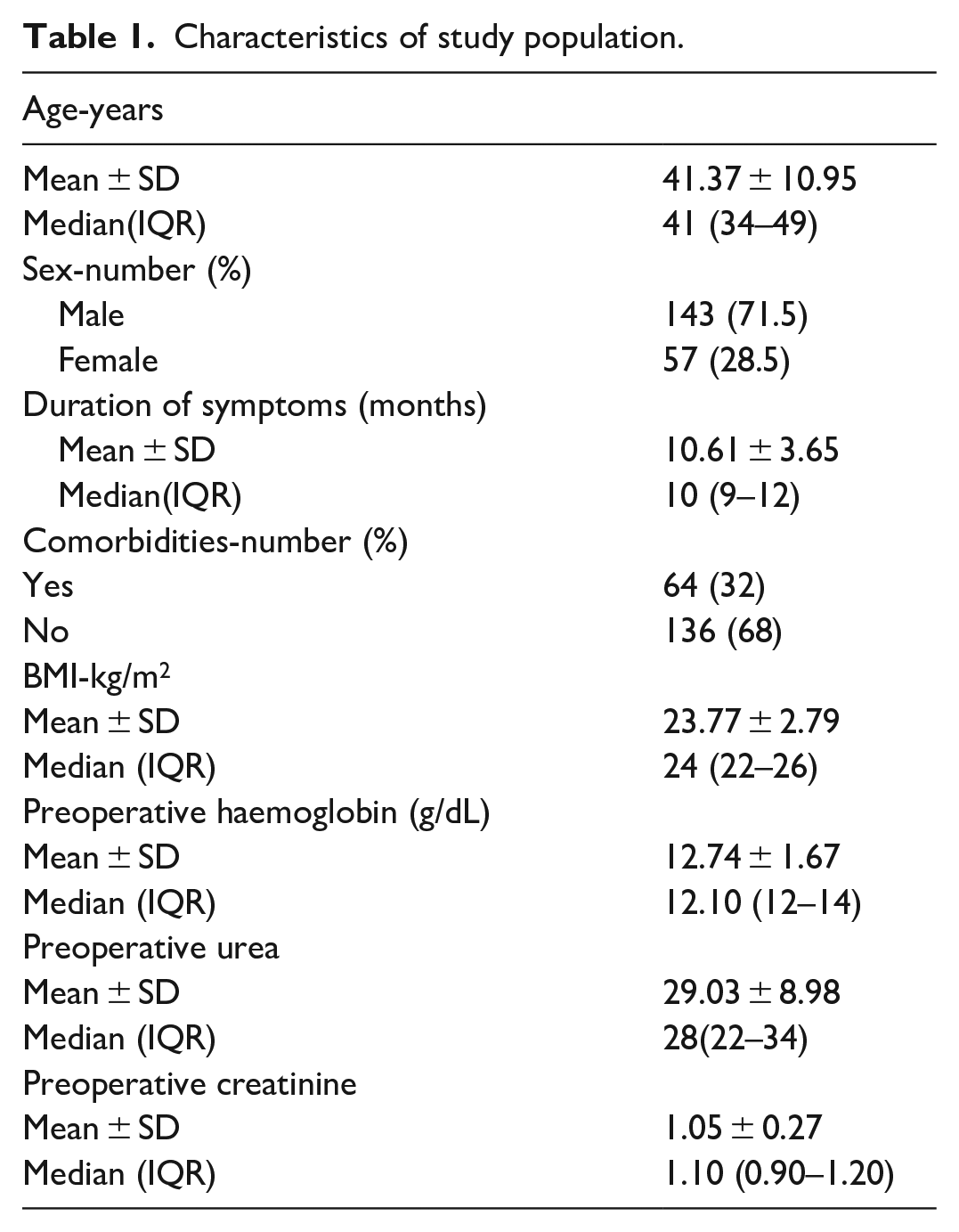
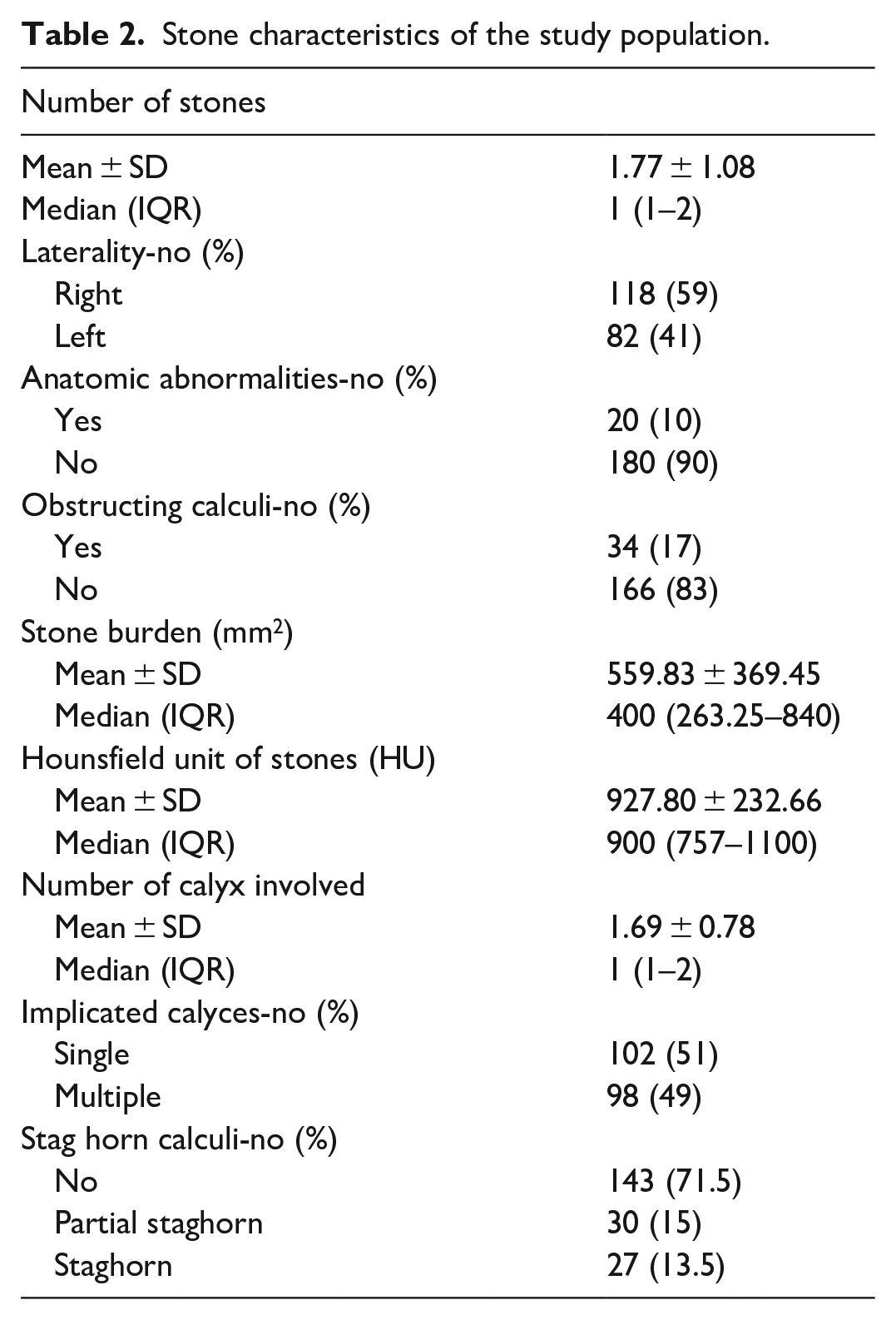
A summary of the demographic profile of our patients including some characteristic features have been shown in Tables 1 and 2. Some stone characteristics of the cases included in the study are shown in Table 2. Most of the patients were male (71.5%). Mean age of the patients included in the study was 41.37 years.
Characteristics of study population.
Stone characteristics of the study population.
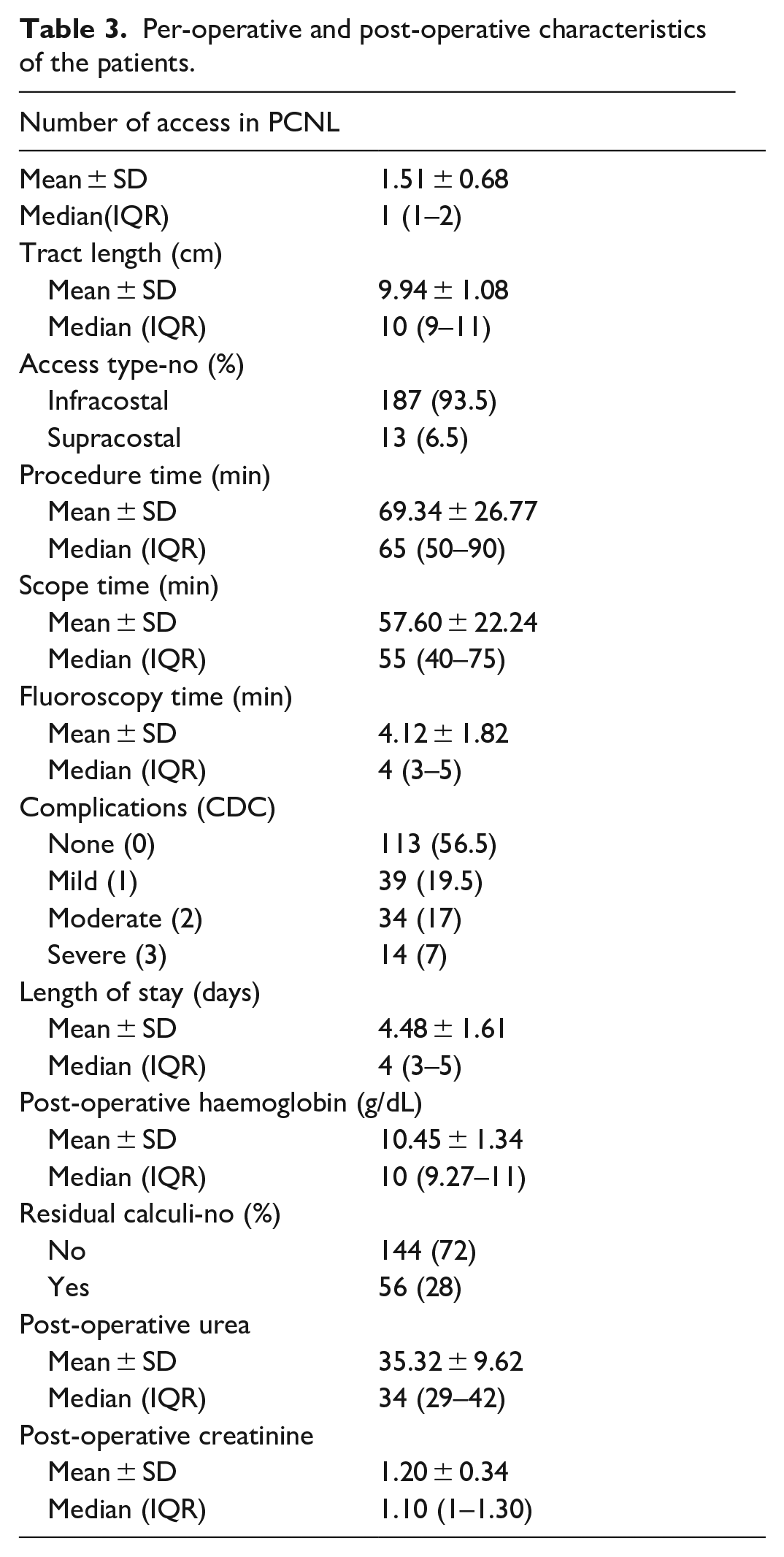
Stone free rate (SFR) post PCNL was 72% in our study. In Table 3, some of the intraoperative and post-operative characteristics of the patients are shown in Any patient having a post-operative retained stone of size >4 mm was considered to have residual calculus. According to stone free status the cases were divided into two groups (Table 4). Stone clearance rate was significantly associated with the stone bulk, staghorn nature of the stones, number of access required during surgery and number of calyces involved (Table 4). No significant association was noted with respect to the stone density in our study. Both the groups were found to be statistically similar with regards to certain demographic factors such as age and sex. In terms of comorbidities, BMI, renal function test, haemoglobin level and laterality of stone both the groups fared similarly. Higher stone burden, involvement of multiple calyces, surgery requiring multiple punctures and presence of staghorn calculus were significantly associated to the residual stone group (Table 4).
Per-operative and post-operative characteristics of the patients.
Analysis of the factors associated with stone clearance.
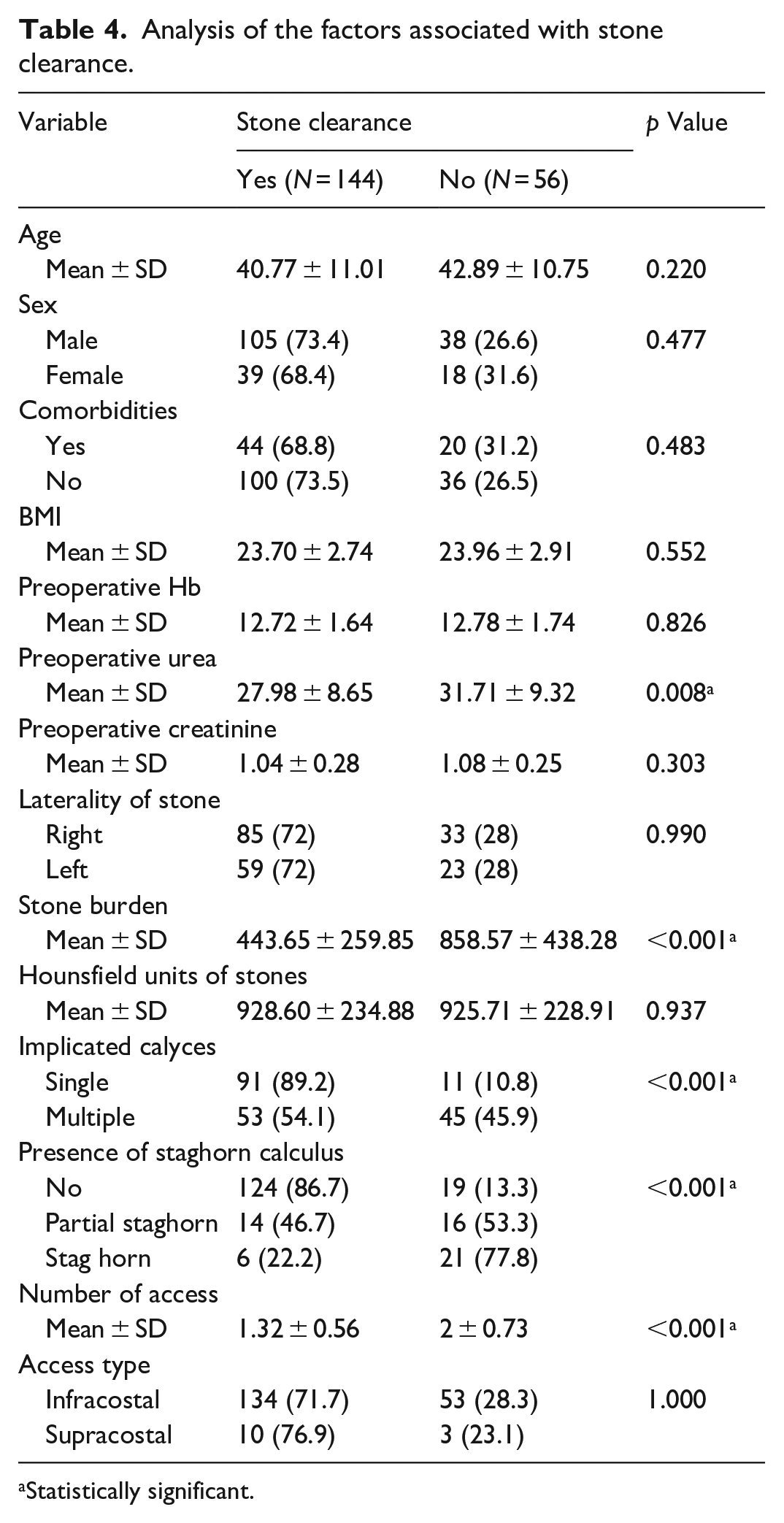
Statistically significant.
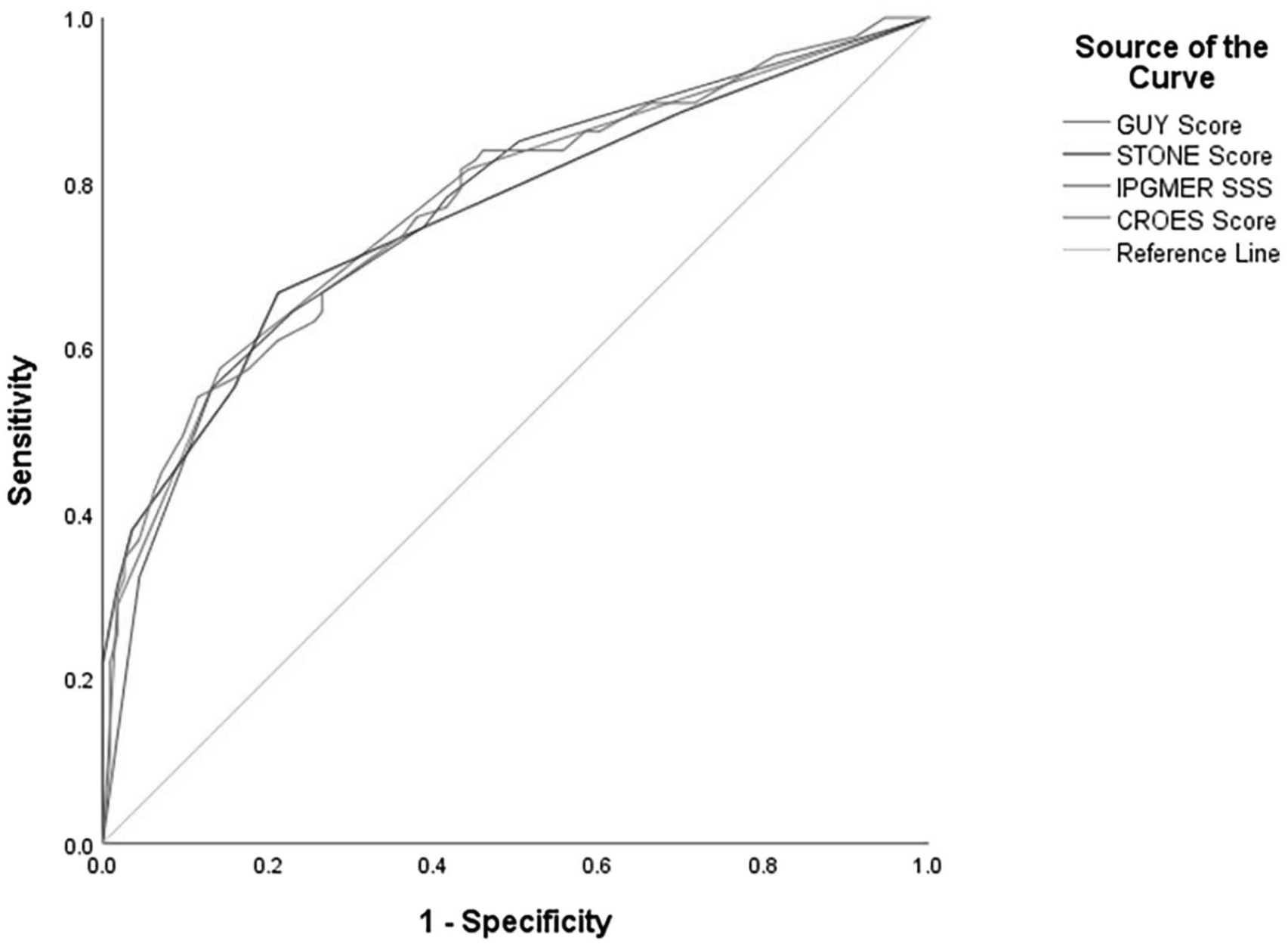
In this study we found that SFR corroborated significantly with low GUY’S score (AUC = 0.836 with 95% CI [0.778–0.894]), low STONE score (AUC = 0.815 with 95% CI [0.745–0.884]) and high CROES score (AUC = 0.830 with 95% CI [0.764–0.896]) (Table 6). All the stone scoring systems could efficiently predict the stone clearance rate (p-value ⩽ 0.001). Stone density was not significantly associated with the outcome. The procedure time, scope time and fluoroscopy time were significantly higher in patients with low CROES score and high STONE score and Guy’s score.
The overall complication rate as per the Clavein-Dindo Grading system was 43.5%. Mostly the complications were minor in nature and were managed by conservative means. Risk of developing post-operative complications as per the modified Clavein-Dindo Grading system was predicted well by the three stone scoring systems and none of them proved their superiority over the other (p-value ⩽ 0.001; Table 8).
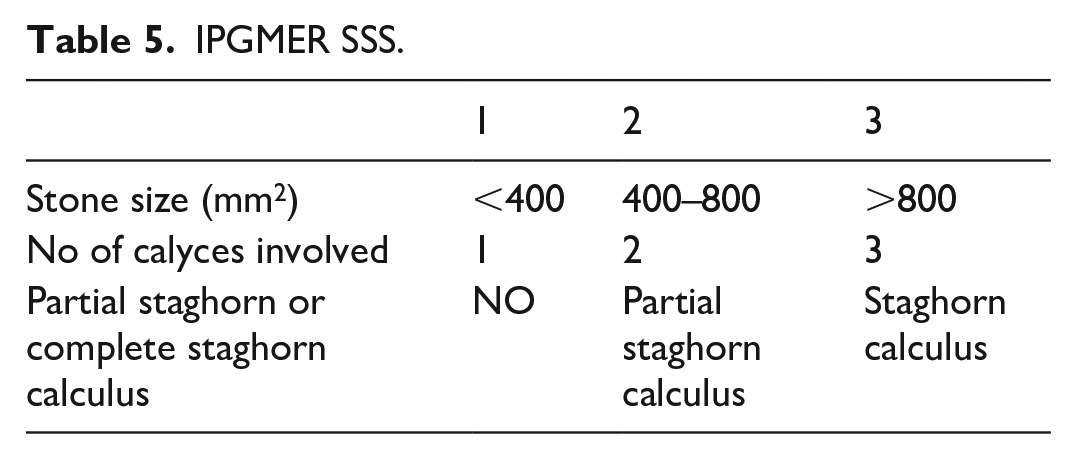
From the results obtained from this study there were certain preoperative clinical factors which were clearly associated with stone free rates (SFR) in PCNL done in this institute. Most of the existing stone scoring systems include multiple factors which are often difficult to remember and cumbersome to apply in a crowded OPD setting. Therefore we would like to suggest a new scoring system including three main pre-operative factors that can predict the outcome of PCNL in terms of SFR. Stone size, number of calyces involved and staghorn nature of the calculus were the prime pre-operative factors found to be significantly related to SFR in PCNL in this study. These can easily be obtained while evaluating the patient in the pre-operative period through investigations like a NCCT scan of kidney, ureter and bladder.
IPGMER pre-operative stone scoring system (IPGMER SSS)
ROC curve of IPGMER SSS was compared to other three stone scoring systems with the intent to validate its predictability in terms of SFR (AUC = 0.831 with 95% CI [0.773–0.889]) (Tables 5, 6 and 7) and risk of development of post-operative complications (AUC = 0.766 with 95% CI [0.698–0.833]; Tables 8 and 9). Predictability of IPGMER SSS was found to be comparable to the other stone scoring systems (Figure 1 and 2).
IPGMER SSS.
AUC of different scoring systems for predicting stone clearance.
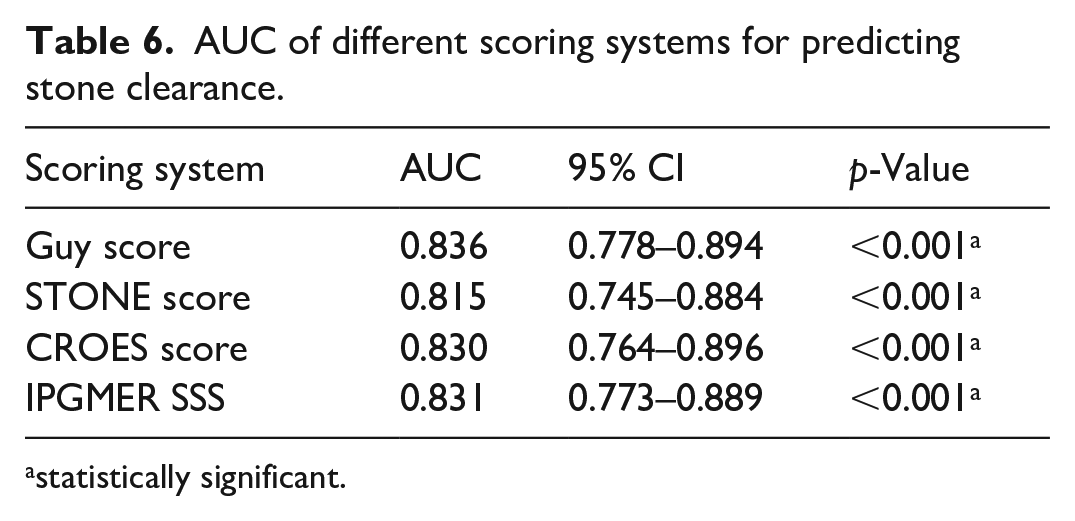
statistically significant.
Diagnostic characteristics of different scoring systems in predicting stone clearance.

AUC of different scoring systems for predicting complications.
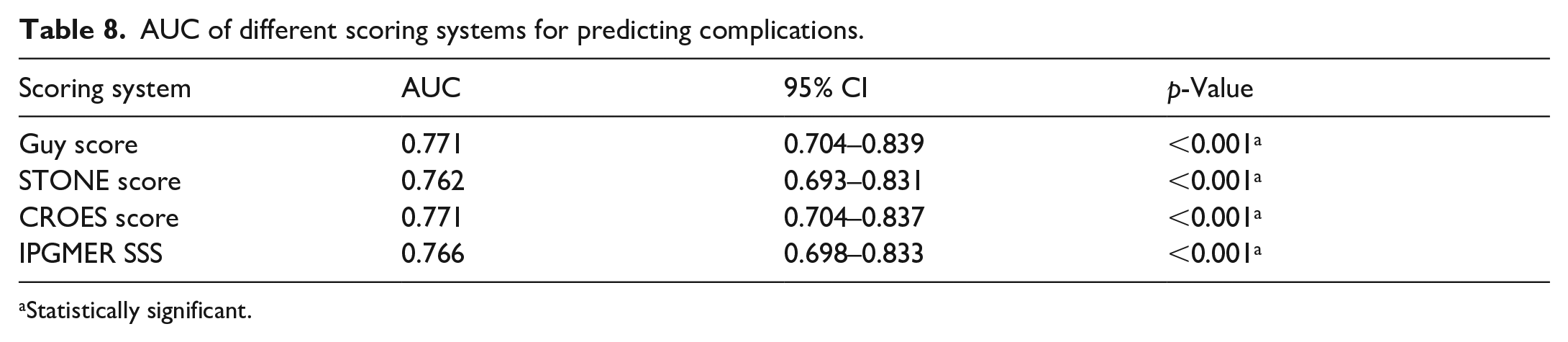
Statistically significant.
Diagnostic characteristics of different scoring systems for predicting complications.

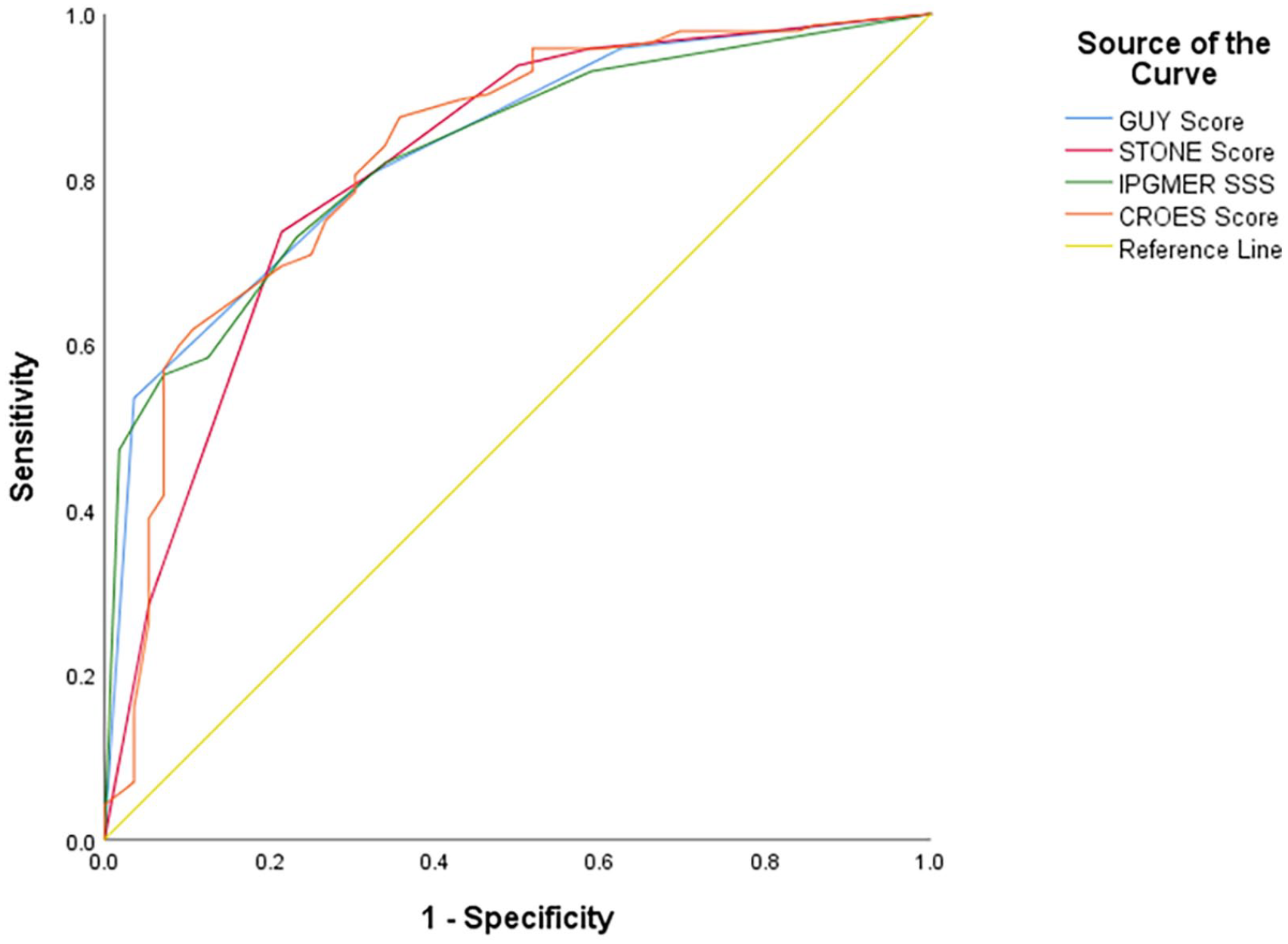
ROC curve comparing different scoring systems in predicting stone clearance.
ROC curve comparing different stone scoring systems in predicting complications.
Discussion
For large kidney stones in a functional kidney, PCNL is the preferable therapeutic option for urologists and its success depends on number of pre-operative factors. From its inception surgeons and tried to predict the optimal outcome of PCNL. Although the basis of developing the existing scoring systems was different yet they were meant to predict stone-free rates and complications in PCNL. They helped in understanding the disease complexity and provided the surgeon and patient with information on the possible outcome of surgery.3,4 To make a scoring system universally acceptable, it should be easy, straightforward with ample predictability rate of stone free rate (SFR) and complications.3 –5
In this study we made an attempt to compare the outcome of three existing SSS in a single cohort of patients who underwent PCNL in our tertiary care institute. Despite the heterogeneity in the variables included in the different stone scoring systems, comparison was made in a single cohort of cases using relevant statistical methods.
We found that the Guy’s stone score (GSS), S.T.O.N.E. score (SS) and the CROES nomogram have good efficiency to predict SFS. In the current study, CROES score had slightly better predictability of SFR than the others. But this finding was not echoed on the previous studies on stone scoring systems. This difference may be a function of the fact that such stone scoring system was developed based on different population of patients with separate characteristics which might have introduced an intrinsic bias favouring predictive efficacy. Similar to all the previous relevant articles, stone size was found to be one of the most important predictor of stone clearance.
All the three scoring systems had efficiently predicted the risk of post-operative complications in this study. All the stone scoring systems analysed the important variables in PCNL in a simple and efficient manner.
Four separate series by Thomas et al., 4 Mandal et al., 6 Vicentini et al. 7 and Ingimarsson et al. 8 validated the GSS. It had efficiently predicted the SFS. Jeong et al. 9 analysed the S.T.O.N.E. scoring system in a multi-institutional study including 850 patients. In this study SFS was predicted significantly. Till now CROES nomogram has been validated only with few studies.3,10
Due to lack of universal standardised definitions of partial and complete staghorn calculus there were significant differences in outcome of the studies on stone scoring systems. Thomas et al. 4 showed the importance of this fact in their study.
Kumar et al. 11 concluded that CROES nephrolithometry nomogram (CNN) is a more comprehensive stone scoring system as it allows accurate risk stratification for residual calculus after PCNL. CNN in this study was not efficient in predicting complications. This finding did not match with our study as we found that all the three scoring systems predicted the development of complications equally. The CNN is a rather complex system to remember and apply on a daily basis in a busy OPD setting. Labadie et al. 12 had shown in his study that all three stone scoring systems predicted SFS in PCNL with similar efficacy. The GSS and SS were associated with estimated blood loss and Length of Stay (LOS). In our study all the scoring systems were found to be predictive of LOS. Compared to other studies, we did not find any relationship of stone clearance with stone density.13,14 Presence or absence of hydronephrosis did not affect the stone-free rate in our study. 15
Vicentini 16 showed similar predictive accuracy of the existing stone scoring systems. Labadie et al. 12 showed that SS was better in risk stratification than the GSS and it can be applied much easily than the CROES nomogram. Although the GSS is easy to use, it has only four grades and provides limited opportunity to accurately classify the stone burden based on the disease severity. 7 Thus it cannot be considered as the ideal stone scoring system for patient counselling and data reporting. 17
Yarimoglu et al. 18 revealed that the existing SSS were equivalent to one another in predicting stone clearance. A recent study published by Singla et al. 19 demonstrated good efficacy of the three stone scoring system in predicting SFS and a weak correlation in determining the risks of complications post PCNL.
We had tested a simpler new stone scoring system named IPGMER pre-operative Stone Scoring System (IPGMER SSS) which included three main pre-operative factors that can predict the rate of stone clearance in PCNL. These factors were significantly associated with SFR in PCNL done in our institute. Size of the stone, number of calyces involved and staghorn nature of the calculus were the factors included in the IPGMER pre-operative Stone Scoring System (IPGMER SSS). On comparison with the existing scoring systems IPGMER SSS fared well with comparable outcome with respect to SFR. IPGMER SSS was able to predict the probability of developing post-operative complications similar to that of the other stone scoring systems. Before recommending this stone scoring system for regular use further studies need to be done especially across different institutes to establish its validity.
In this study we have tried our best to follow the criteria for selection and use standardised methods of PCNL before analysing the data. Some of the limitations of our study were the number of cases and exclusion of patients who had undergone ipsilateral surgery or had a nephrostomy tube in situ. Including such cases though would have enhanced our learning but on the other hand it would have made the comparison of results difficult. The high complication rate seen in this study might be attributed to the complexity of the cases as well as the part of learning curve of a student training institute. Further prospective multi-institutional data are necessary to determine a standard stone scoring system that can effectively predict post-PCNL outcomes.
Conclusion
The Nephrolithometry scoring systems are simple, straightforward and easily reproducible systems to determine the magnitude of stone burden and to stratify the complexity of PCNL. The Guy score, S.T.O.N.E. score and CROES nomogram could sufficiently predict stone clearance in patients contemplating PCNL. The CROES score seemed slightly ahead of the others in our study. All the stone scoring systems were up to the mark in predicting post-operative risk of complications. These scoring systems help in proper patient counselling and give them an assessment of post-operative outcome before undergoing PCNL. IPGMER pre-operative stone scoring system (IPGMER SSS) could be used as an alternative to predict SFR and complications in PCNL. Further investigations are required before prescribing the best stone scoring system for predicting the outcomes of PCNL.
Footnotes
Acknowledgements
We would like to thank the Institutional Ethics Committee for their help in approving this study. We would also like to thank the patients for their contribution in this study.
Author contributions
BH – responsible for analysis and writing the manuscript; DS – responsible for conceptualisation and review editing; SC – responsible for conceptualisation and review editing; DKP – responsible for conceptualisation and supervision; All the authors have read and approved this manuscript for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional ethical clearance was taken on 04/02/2020 (IPGME&R/IEC/2020/048R).
Consent to participate
Informed consent was taken from all the patients.
Consent for publication
All the authors have unanimously given consent for this article to be published in your esteemed journal.
Availability of data and material
All the data including master chart, are available at your earliest request.