
Abstract
Background:
Imaging to be used during the workup and follow-up of patients undergoing pyeloplasty is still controversial. Present survey aimed at assessing variations in pre- and post-operative imaging between adults and paediatric specialists in patients undergoing pyeloplasty.
Methods:
A survey of members of the ‘Italian Society of Urology’ (SIU) and the ‘Italian Society of Paediatric Urology’ (SIUP) was conducted using an online platform.
Results:
Respondents included 87 (74.4%) adult and 30 (25.6%) paediatric specialists. Adult specialists were significantly more likely to use a CT scan during preoperative workup (p = 0.001) and postoperative follow-up (p < 0.001). In contrast, paediatric specialists were significantly more likely to recommend voiding cystourethrography during the workup (p < 0.001) and an MRI in cases requiring additional diagnostic study (<0.001). Adult specialists reported to deal significantly more commonly with symptomatic or complicated hydronephroses (p < 0.001). The majority of respondents recommend an ultrasound scan at 1–3 months as first postoperative investigation. Two-third also recommended a nuclear scintigraphy, but 67.8% of adult specialists recommended to perform it within 6 months of surgery whereas 76.7% of paediatric specialists between 6 and 12 months (p < 0.001).
Conclusions:
Present survey suggests quite a significant variation between adult and paediatric specialists in pre- and post-operative assessment of patients requiring pyeloplasty. This may just reflect different attitudes that could be improved with appropriate studies, or essential differences in the condition or the characteristics of treated patients. In any case, such differences are important and should be taken into account.
Introduction
Pyelo-ureteral junction obstruction (PUJO) is a common condition in children and adults alike and pyeloplasty the standard treatment.1–3
Usually, the first sign of PUJO is the radiological detection of hydronephrosis (HN) on an ultrasound (US) scan. HN is a very common finding in general. The widespread use of prenatal US screening of congenital malformations has made HN also the most common anomaly detected antenatally. 4 This phenomenon has created a new condition termed as asymptomatic antenatal HN. 4
The diagnosis of obstruction in patients with HN is still a matter of debate. 5 In a few cases, more commonly adults, the presence of symptoms corroborates the diagnosis of obstruction. In the absence of symptoms, instead, as it is the case in most children and all the infants with antenatal HN, it has become increasingly clear that the presence of HN does not equate per se to obstruction. Nowadays, the most accepted definition of obstructive HN needing treatment is a dilatation that, if left untreated, will cause symptoms or renal damage. 6 In many cases, instead, the HN can remain stable or improve over time. In particular, natural history series of patients with congenital asymptomatic HN have shown that 50%–75% do not require any surgical treatment. 6
An additional issue, again more common in children, is that the diagnosis of HN is not specific. 4 Several conditions, first of all vesico-ureteral reflux (VUR), come into differential diagnosis in patients with HN and, therefore, have to be considered and, if necessary, ruled out during preoperative work-up.
Post-operative imaging can also vary between specialists, but also among physicians belonging to the same speciality. Variations concern both the investigations required and their timing. In particular, it is controversial whether a dynamic renal scan could be avoided postoperatively, especially in presence of an improvement of upper tract dilatation. 7 Regarding the timing, some recommend an early re-evaluation in order to pick-up any persistent/recurrent obstruction which could jeopardise kidney function, whereas others prefer to delay the evaluation while waiting for the spontaneous healing to occur, in a procedure that reportedly has a very low failure rate. 8
Present survey was promoted by the working-group on paediatric urology of the ‘Società Italiana di Urologia’ (SIU) and aimed at assessing variations in pre- and post-operative imaging between adults and paediatric specialists in patients undergoing pyelopalsty.
Material and methods
A survey
Two groups were compared, namely specialists treating mainly or exclusively adult patients, termed as adult specialists, versus those dealing mainly or exclusively with paediatric patients, termed as paediatric specialists.
Descriptive statistics were used to analyse the responses. All the analyses were performed using R software v.1.2.5042. Pearson’s Chi-squared test or Fisher’s exact test, as applicable, were used to compare the two groups. A p < 0.05 was considered statistically significant.
Results
A total of 117 responses were registered including 87 (74.4%) adult and 30 (25.6%) paediatric specialists. The estimated response rate was <5% of potential eligible respondents.
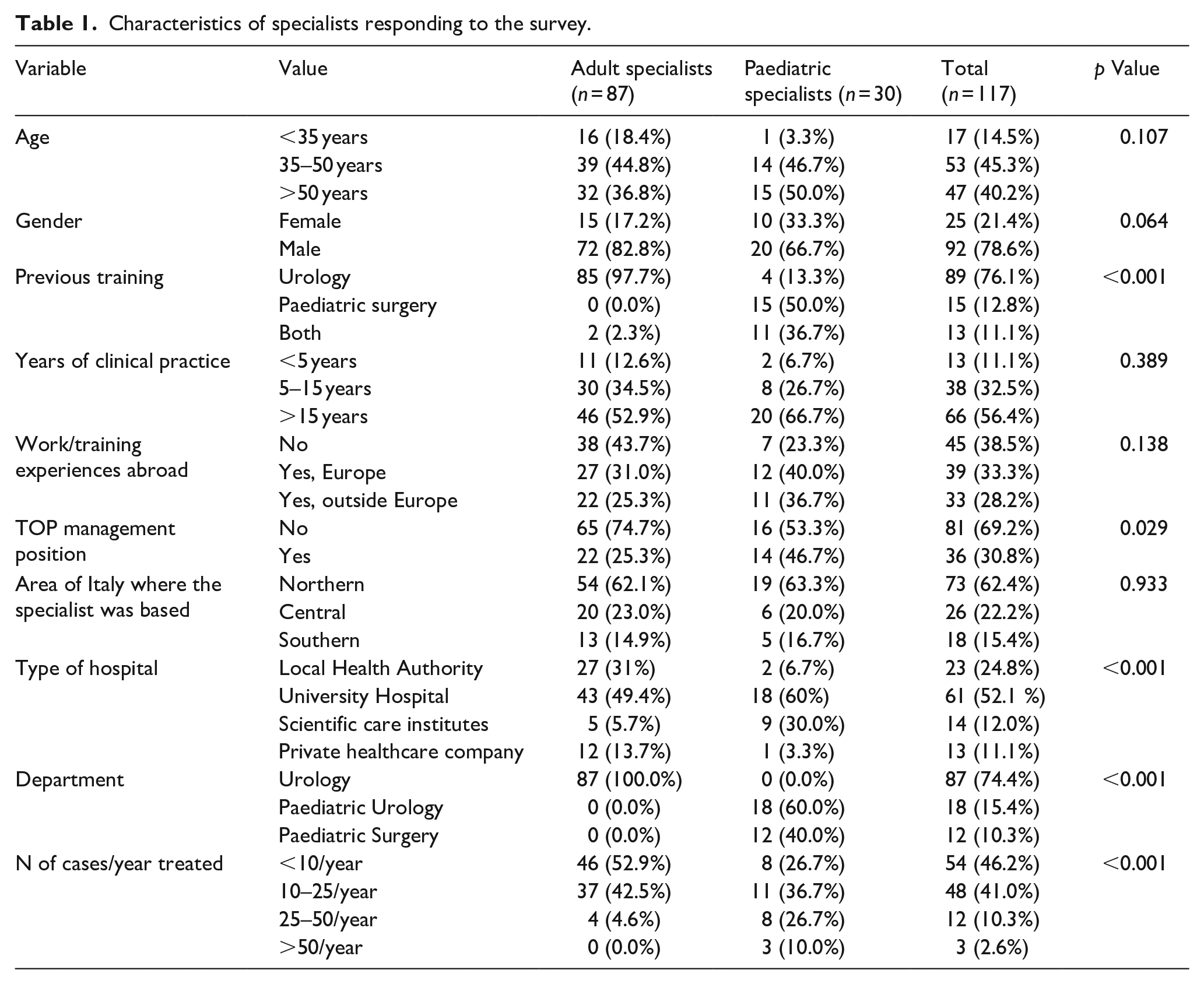
As shown in Table 1, two third of respondents were located in northern Italy, but there was no difference between groups in the geographical distribution across Italy. Paediatric specialists were significantly more likely to have been trained both in paediatric surgery and urology than adult specialists to have received also a paediatric surgery training (36.7% vs 2.3%, p < 0.001). Compared to adult, paediatric specialists were significantly more likely to work in an academic institution (90% vs 55.1%, p < 0.001), and have a top management position (46.7% vs 25.3%; p = 0.029). Moreover, reportedly, paediatric specialists treated a significantly larger number of cases/year (26.7% >25 cases/year and 36.7% 10–25 cases/year vs 50% of adult specialists treating <10 cases/year, p < 0.001).
Characteristics of specialists responding to the survey.
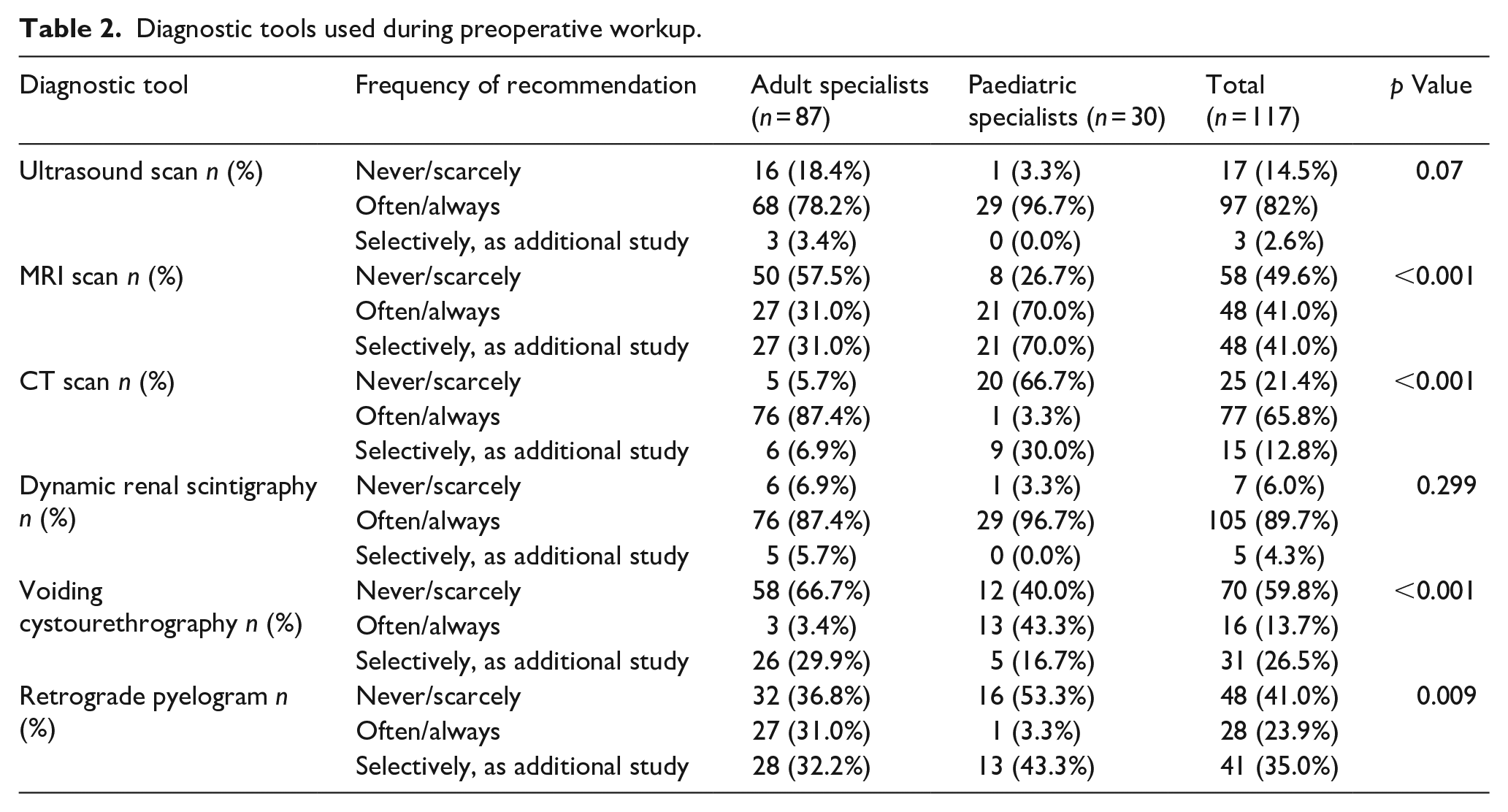
As for preoperative workup (Table 2), specialists agreed on the role of ultrasound and dynamic scintigraphy that 80% or more of the responders of both groups recommended ‘often or always’. Adult specialists were significantly more likely to recommend a CT scan (‘always/often’ 87.6% vs 3.3%, p = 0.001) and a preoperative retrograde pyelography (‘always/often’ 31% vs 3.3%, p = 0.009). Paediatric specialists, instead, significantly more often recommend an MRI in cases requiring additional diagnostic study (70% vs 31%, <0.001). Finally, paediatric specialists seemed significantly more likely than adult ones to recommend a voiding cystourethrography (VCUG) than the adult colleagues (‘always/often’ 43.3% vs 3.4%, p < 0.001).
Diagnostic tools used during preoperative workup.
Most indications did not differ between specialists (Table 3). However, adult specialists mentioned a symptomatic or complicated obstruction to be an indication for surgery significantly more commonly than paediatric ones (74.2% vs 23.3%, p < 0.001) whereas a loss of function on two subsequent renal scintigraphies in an otherwise asymptomatic patient was a significantly more uncommon indication in adult than paediatric practice (‘very rare/rare’ 41.4% vs 20%, p = 0.042).
Indications for surgery.
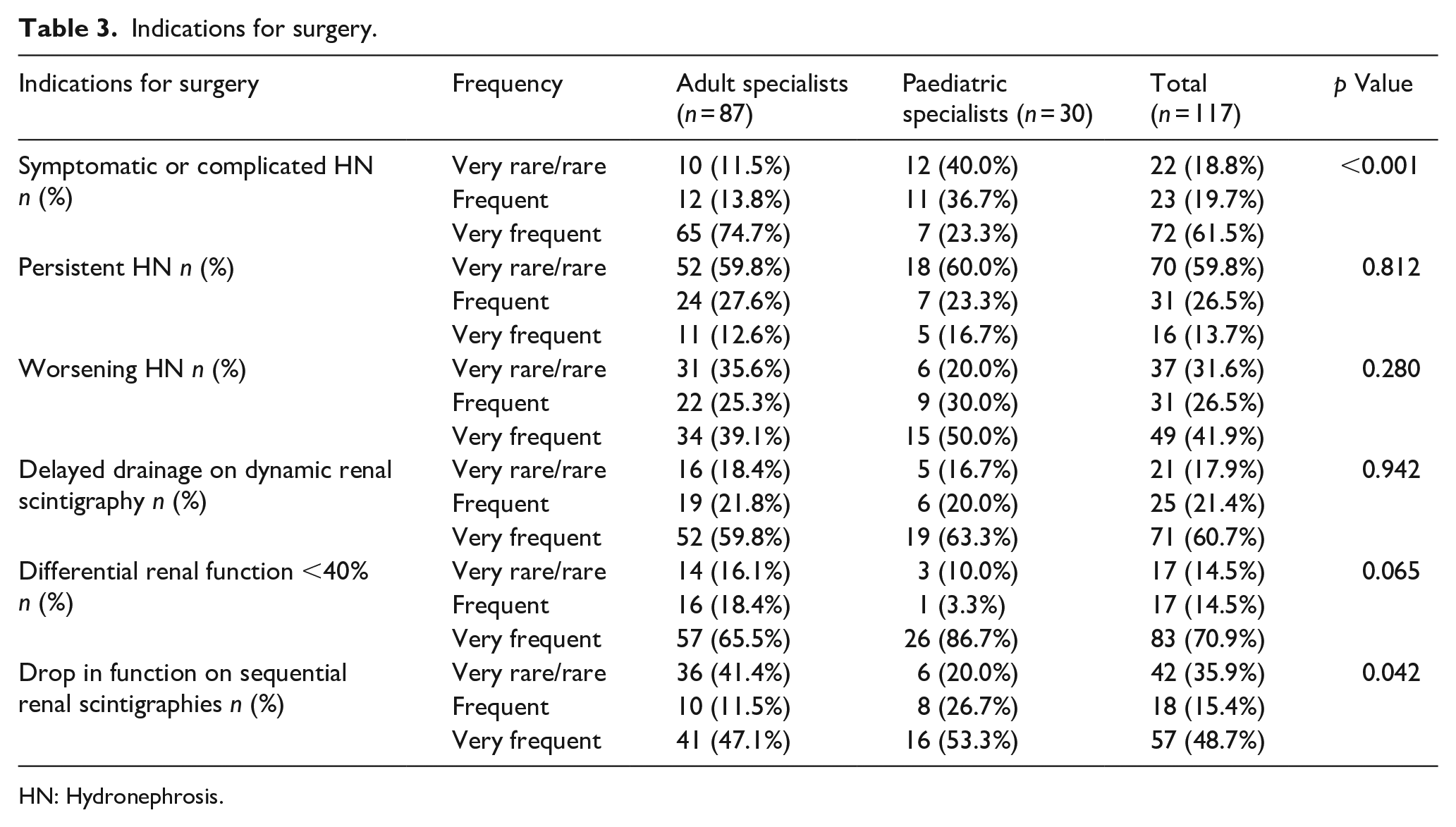
HN: Hydronephrosis.
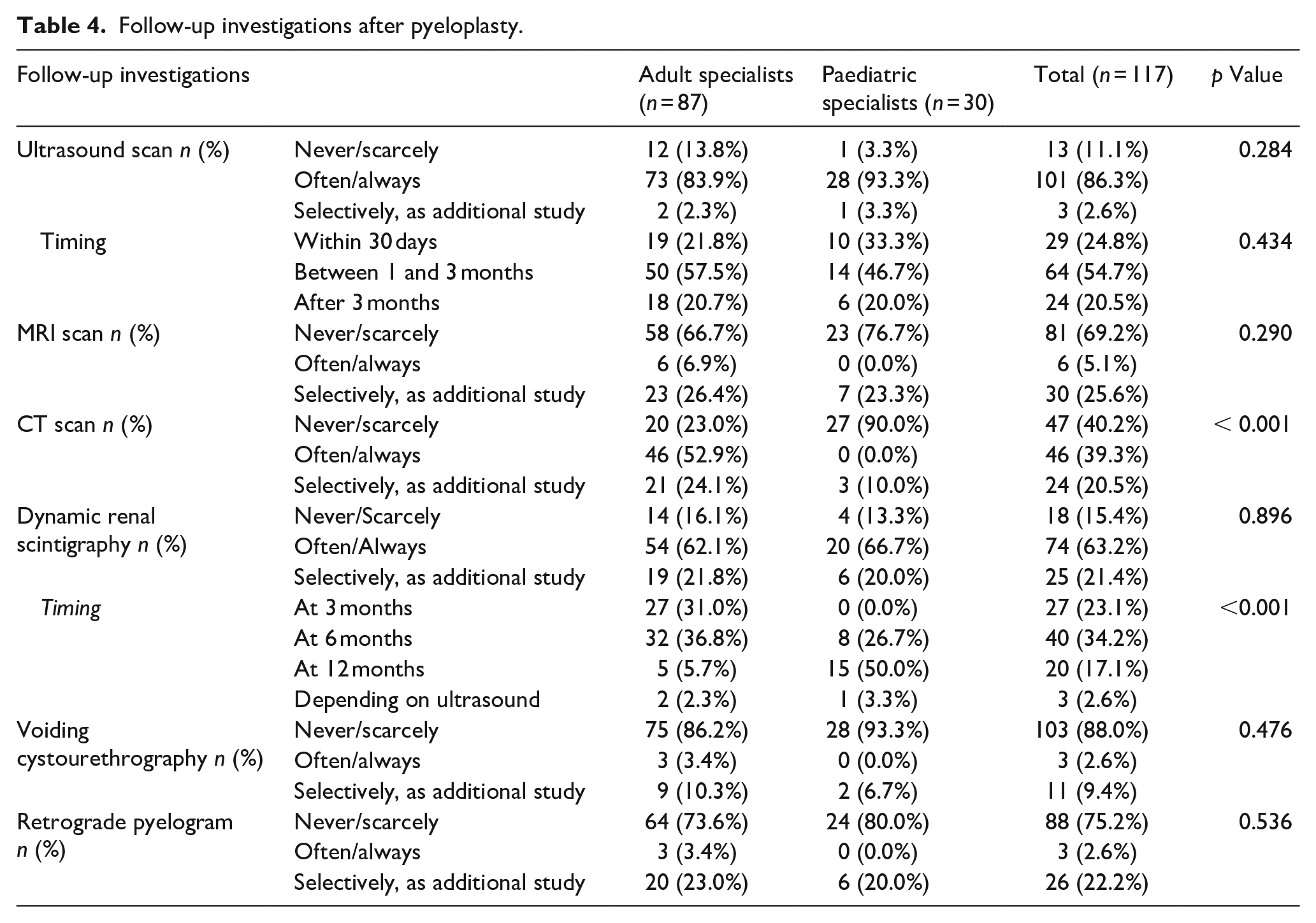
Regarding postoperative follow-up (Table 4), the majority of respondents (54.7%) in both groups recommended the first postoperative control at 1–3 months. In general, all respondents recommended repeating the same investigations performed during preoperative work-up including a CT scan for adult specialists (52.9% vs 0% of paediatric specialists, p < 0.001). However, in contrast to the 89% of respondents recommending a dynamic renal scintigraphy preoperatively, only 63% recommended this investigation postoperatively, without difference between groups. Still, 67.8% of adult specialists preferred performing it within 6 months of surgery (31% at 3 months), whereas 76.7% of paediatric specialists between 6 and 12 months (50% at 12 months), p < 0.001.
Follow-up investigations after pyeloplasty.
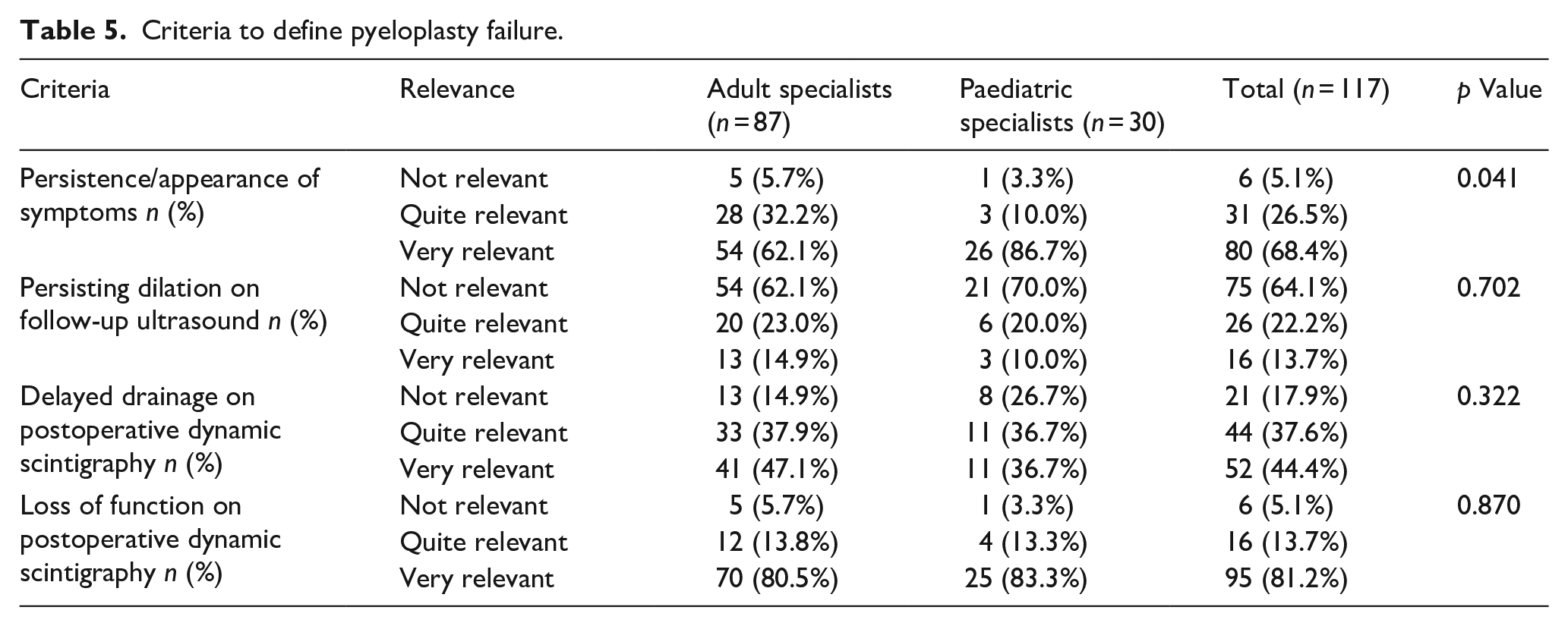
In terms of definition of pyeloplasty failure, responses were not much different between specialists (Table 5). Most agreed a persisting dilatation and a delayed drainage on the renal nuclear scan to be poor indicators of failure. In contrast, the presence of symptoms, persisting or appearing de novo, and a drop in differential function on postoperative scintigraphy were generally considered signs of failure.
Criteria to define pyeloplasty failure.
Discussion
Present survey showed significant variations between adult and paediatric specialists in the imaging performed during preoperative work-up and postoperative follow-up of patients undergoing pyeloplasty for UPJO. Adult specialist recommended more commonly a CT scan and/or a retrograde pyelography preoperatively and a CT scan during follow-up, whereas were much more unlikely to recommend a VCUG in the preoperative work-up and an MRI in patients requiring additional study of upper urinary tract anatomy.
Such differences are in part be consistent with current guidelines of the European Association of Urology 10 and multiple reasons can account for such differences. To begin with, this survey confirms a different working setting between specialists. Paediatric specialists often dealing with rare conditions, generally worked in small units located in few major academic centres. They were significantly more often trained both in paediatric surgery and general urology. These characteristics, together with the fact that UPJO is a congenital condition often diagnosed prenatally, may explain why paediatric specialists seemed to treat larger numbers of cases/year than the adult counterpart. The peculiar working setting of paediatric specialists might also involve a dipper interest and easier access to more sophisticated investigations such as the MRI compared to the CT scan.
The CT scan is considered useful in the management of adult patients or obtaining anatomical information about UPJO and to help identifying potential causes. 11 A major reason possibly accounting for the much less extensive use of this tool by paediatric specialists, might be the attempt to minimise X-ray exposure in children. This is also consistent with the preference given to the MRI scan, if additional diagnostic study of the urinary tract was deemed necessary preoperatively. 12 Similar arguments may apply also to the significantly less extensive use of preoperative retrograde pyelography in children compared to adults.
Apparently in contrast with such an attitude to avoid radiological and invasive investigations in children, paediatric specialists seemed significantly more likely than adult colleagues to recommend a VCUG during preoperative workup. This is due to the possible presence of a VUR in paediatric patients with HN. 13 This attitude, however, seems to be changing also in paediatric practice where nowadays this investigation is generally limited to cases with a visible ureter on the US scan. 13 It is increasingly accepted that the presence of VUR in patients with the typical signs of UPJO on US and dynamic renal scintigraphy is low and, when present, the VUR under these circumstances is usually of limited clinical significance due to a low risk to develop urinary tract infections and a high chance of spontaneous resolution. 14
Different attitudes with preoperative work-up can also depend on the different characteristics of the condition adult and paediatric specialists usually deal with. In adult practice, symptomatic HN seemed significantly more common. Under these circumstances, the indication for surgery is more clear-cut. Paediatric specialists, instead, often deal with asymptomatic HN. Under these circumstances, natural history series have shown a high chance of spontaneous resolution of the dilatation in the absence of treatment. 4 Therefore, a period of observation is generally recommended to assess the evolution of the dilatation before a decision about surgery is taken. For this reason, likely, a detection of a drop in function over subsequent dynamic nuclear scintigraphies was reportedly a significantly more common indication for surgery in children than adults.
During postoperative follow-up, specialists of both groups generally recommended to repeat the same investigations performed during preoperative workup and the first follow-up investigation was generally an US scan performed between 1 and 3 months after surgery. Postoperative investigations included also a CT scan that, as during preoperative work-up, was recommended significantly more commonly by adult specialists.
The dynamic renal scan was also recommended quite extensively but less than during preoperative workup. The most likely reason accounting for this is that, although a postoperative nuclear scan can give valuable additional information, 7 it is quite accepted that whenever an imaging of the urinary tract, like either an US or a CT scan, documents an improvement in the degree of HN, the risk of a persistent/recurrent obstruction seems very low. 15 According to this assumption, in clinical practice, a postoperative renal scintigraphy could be limited to patients showing no improvement of the dilatation postoperatively, or to assess any function recovery in patients with preoperative renal function impairment. 16 It should be said, however, that very few respondents declared to perform a nuclear scan based on the results of the ultrasound. Possible explanations are that this is unpractical to adopt such a flexible approach, or that having both exams provide a more comprehensive and reliable assessment of the results.
Controversies also surround the ideal timing of the follow-up nuclear scan. Adult specialists generally recommended performing this investigation earlier than paediatric specialist. Both attitudes have possible pros and cons. An early scintigraphy, in principle, allows for a timely detection of a failures thereby reducing the risk of renal damage due to a persistent or recurrent obstruction. 8 In addition, it can allow for an early patient discharge from additional follow-up.8,17 Nevertheless, an early nuclear scan can also be misleading. Pohl et al 17 reported a persistent obstructive excretion pattern in 20% of cases 3 months after pyeloplasty with a subsequent improvement at 1-year follow-up scintigraphy in 98% of cases. Therefore, a delayed renal scan can be more reliable particularly. This should also to be considered in light of the success rate >95% reported for the procedure. 1 It is finally possible that paediatric specialists usually dealing with a larger number of UPJO, could feel more confident in waiting longer before re-assessing the patients after surgery.
The major limitation of present survey is the low response rate. The latter could not be calculated accurately because many responders were members of both societies and also resident and non-urologist members of the societies were included in the mailing list of invitation. Nevertheless, we complied with the most common reconditions for this kind of studies 9 and our response rate is comparable to other similar surveys published recently.18,19
Conclusions
Present survey suggests quite a significant variation between adult and paediatric specialists in pre- and post-operative assessment of patients requiring pyeloplasty for PUJO. Adult specialists were significantly more likely to recommend a CT scan pre- and post-operatively, whereas paediatric specialists were more likely to include a VCUG in the standard preoperative workup and consider an MRI in patients requiring additional study of the upper tract anatomy. This may just reflect different attitudes that could be improved with appropriate studies, or unavoidable differences in the treated conditions or in patient characteristics. In any case, such differences are important and should be taken into account.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.