
Abstract
Objectives:
Evaluation of safety, efficacy, and feasibility of emergency extracorporeal shockwave lithotripsy (eESWL) in combating obstructing stones with colic on emergency basis.
Materials and methods:
From November 2019 to November 2021, 102 subjects underwent emergency ESWL for obstructing ureteric and renal stones with colic within 24 h of presentation.
Results:
Patients in this study belonged to age group of 18–67 years with mean being 39 years consisting of 85 males and 22 females (M:F = 85:22). Mean stone dimensions were 8.26 mm in length and 7.65 mm in width. A total of 42 patients had their stone in kidney or upper ureter while 24 patients had stone in mid ureter and remaining patients (n = 36) had stone in lower ureter. About 65 patients had their stone completely cleared after single ESWL session while 20 patients required multiple sessions to achieve complete clearance. Of these 17 patients (16.67%) were not rendered stone free even after three sessions and had to undergo ureteroscopic lithotripsy (URSL). Overall Stone Free Rate (SFR) was 83.33%. For stone attenuation of ⩽900 HU, SFR was 97.18% while for >900 HU it was only 51.61%.
Conclusion:
eESWL is safe, feasible, and efficacious noninvasive alternative for definitive management of obstructing ureteral and renal stones with colic as far as stone clearance and rapid and definitive pain relief are concerned and that too with very minimal morbidity without the need for admission and hence can reduce the prolonged waiting period for endoscopic stone surgery in any high-volume tertiary care hospital. Length, width, and attenuation of stone were found to be the main factors dictating the success of eESWL.
Keywords
Introduction
An ever-increasing global surge in the incidence of urinary stone disease has been noted, the bulk of which is constituted by upper tract urinary calculi. Patients present with acute ureteric colic as their chief complaint which has traditionally been quoted as acute flank pain radiating to groin and is quite often caused by ureteric calculi. A non-contrast computed tomography (NCCT kidney ureter bladder [KUB]) confirms the diagnosis. After initial relief of symptoms, obstructive uropathy is taken care of, either by ureteral stent insertion, ESWL, URSL, or open/laparoscopic ureterolithotomy.
ESWL, a non-invasive modality is the preferred modality to combat moderately sized, uncomplicated ureteric calculi.1,2 It is a simple and safe procedure for stones refractory to drug therapy provided there are no absolute indications mandating ureteral drainage. 3 It’s quite intriguing to note that the role of eESWL as front-line therapy, applied immediately after the onset of symptoms, has hardly drawn attention.
Success rate of ESWL is somewhere around 80%. 4 There is no consensus with regards to the time of ESWL for ureteric colic. Different authors have quoted it differently. Even without anesthesia, ESWL has been delivered successfully in patients with recurrent symptoms after initial medical therapy. 5 While others have advocated delivering ESWL under anesthesia, within 2 weeks of the onset of ureteric colic 5 or at the onset of acute symptoms 1 or even in the setting of acute renal insufficiency. 6 Moreover, a retrospective comparative study has already established the superiority of emergency ESWL over urgent nephrostomy or a double J stent. 7
Taking into account the towering incidence of urinary stone disease, it’s quite obvious to have a long waiting period at any tertiary care health center for it’s definitive management. While the patient’s wait for definitive management continues, the disease process doesn’t come to a standstill, rather it keeps on progressing and it’s not infrequent for the waiting patient to land up in complications like hydronephrosis, pyonephrosis, or urosepsis which ultimately leads to renal insufficiency and at times even complete loss of function of the concerned kidney. 5 This dreaded scenario compels us to look at emergency ESWL in an attempt to halt the disease progression at the outset. The idea of emergency ESWL is not something that’s unheard of, but there is only a handful of literature banking upon it.5 –8
The incidence of stone disease at our center is in the range of 3500–4000 cases per year and more than 95% of these patients harbor stones in their upper urinary tract. Out of these only about 1000–1200 patients undergo endoscopic stone retrieval annually as definitive management and that too after a minimum waiting period of 3–4 months. Rest of the patients are subjected to routine ESWL (provided they are candidates eligible for ESWL). Even the waiting period for routine ESWL at our center averages around 4–6 weeks.
In order to address the huge patient load and cut short the long waiting period, this present study was proposed.
Materials and methods
Urology department of a tertiary care center was the venue for this study conducted between November 2019 to November 2021. Ethical clearance for this study was obtained from the institutional ethical committee (IEC/2020/045). Patients having urinary tract infection (UTI), uncorrected coagulopathy, morbid obesity, radiolucent stones, bilateral ureteric calculi, renal insufficiency, bony deformities, and pregnancy were excluded. All patients presenting with acute ureteric colic in our emergency/urology department were recruited for this study after proper informed consent. Based on clinical diagnosis/suspicion urgent ultrasonography (USG) KUB (for initial diagnosis), X-ray KUB (for radio-opacity and also to aid in follow-up), and NCCT KUB (for stone characteristics) were done. On NCCT KUB-laterality of the stone, length (longitudinal diameter in case of ureteric calculus while the largest dimension in case of renal calculus) and width (transverse diameter in case of ureteric calculus while the shortest dimension in case of renal calculus) of the stone, stone attenuation, and the severity of hydroureteronephrosis were noted.
All patients underwent blood tests incorporating full blood count, coagulation panel, and renal function test. Urine was screened for routine and microscopy while awaiting culture sensitivity. After confirmation of clinical diagnosis by imaging, patients were scheduled for ESWL within 24 h of their presentation.
On conclusion of the session, patients were kept on observation for a few hours and were sent back home on the same day in the absence of symptoms mandating admission. However, if a patient had persisting refractory pain, vomiting, or gross hematuria they were admitted until their symptoms resolved.
Study technique
All patients underwent ESWL on an outpatient basis using Dornier sigma compact, Medtech lithotripter. Upper ureteric (UU) stones received ESWL in supine position while mid ureteric (MU) and lower ureteric (LU) calculi were fragmented in prone position (under c-arm guidance).
Shockwaves were delivered at a frequency of 60 pulse per minute without anesthesia (nevertheless subjects were given injection Diclofenac 75 mg, when required) with a gradual vamping from a–b–c–1–2–3 according to patient’s tolerability. The procedure was stopped once satisfactory disintegration was achieved as evidenced on fluoroscopy or after 3000 shocks. After ESWL, all subjects were put on tamsulosin (0.4), antibiotics, and analgesics.
In the follow-up period, patients were asked to get X-ray KUB done 21 days after first session. Absence of stone or any residual fragments on X-ray suggested successful ESWL. Insufficient or no fragmentation of calculus mandated further ESWL sessions. Stones refractory to disintegration or inadequate disintegration even after three sessions were stamped as failed ESWL and were subjected to endourologic modality. Any patient who developed complications like severe pain, UTI/sepsis was straightaway subjected to URSL.
Data collected at the end of the study duration were filled into a Microsoft excel sheet and were analyzed using SPSS (version 27: SPSS Inc., Chicago, IL, USA).
Results and analysis
About 102 patients (22 females and 80 males) were enrolled in this study. The final analysis of all these patients; their attributes and other parameters are depicted in Table 1.
Patient and stone characteristics in relation to ESWL.
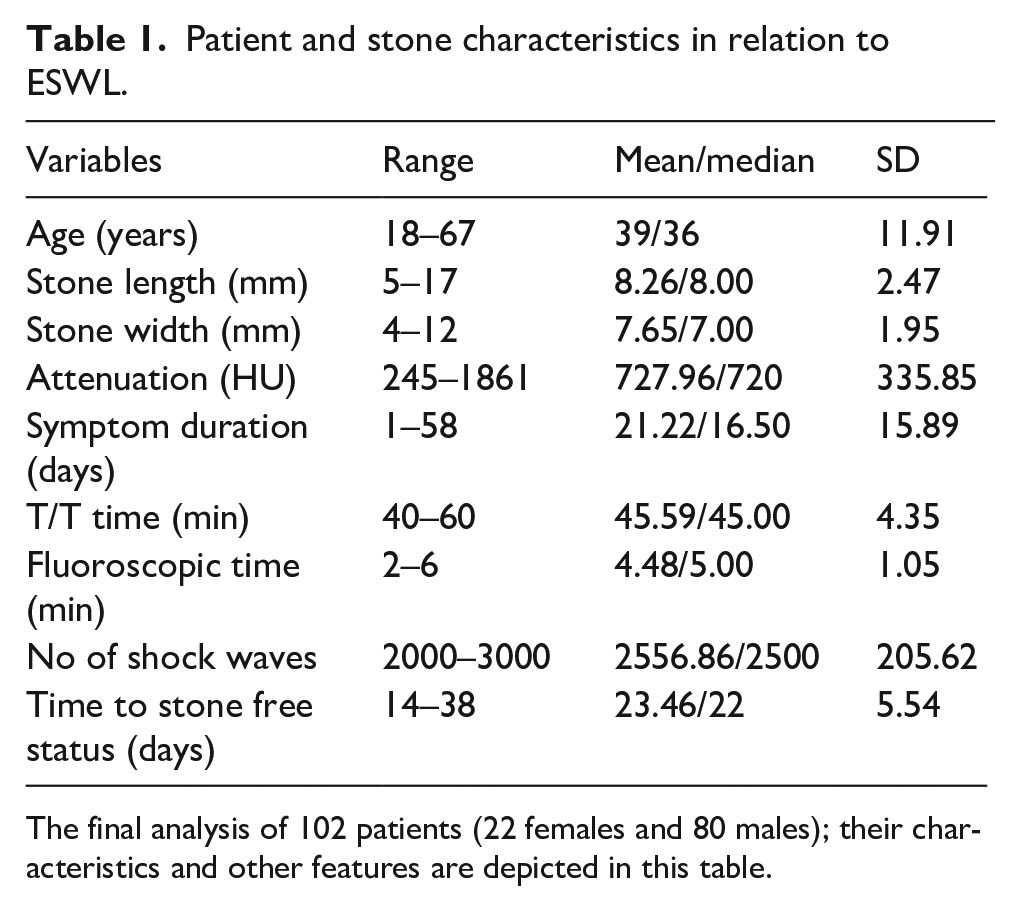
The final analysis of 102 patients (22 females and 80 males); their characteristics and other features are depicted in this table.
A 96.08% (98/102) of patients fell into the age group of 20–60 years. While less than 4% (4/102) of patients stood on either side of extremes of age.
Overall SFR was 83.33% (85/102). Of these 85 patients, 76.47% (65/85) had their stone cleared after one session while 23.53% (20/85) patients had to undergo multiple sessions. A 17 patients (16.67%) not rendered stone-free even after three sessions had to undergo URSL.
Mean stone length, mean stone width, and mean stone attenuation in stone-free and stone-not-free groups are depicted in Table 2.
Variables influencing stone-free rate.
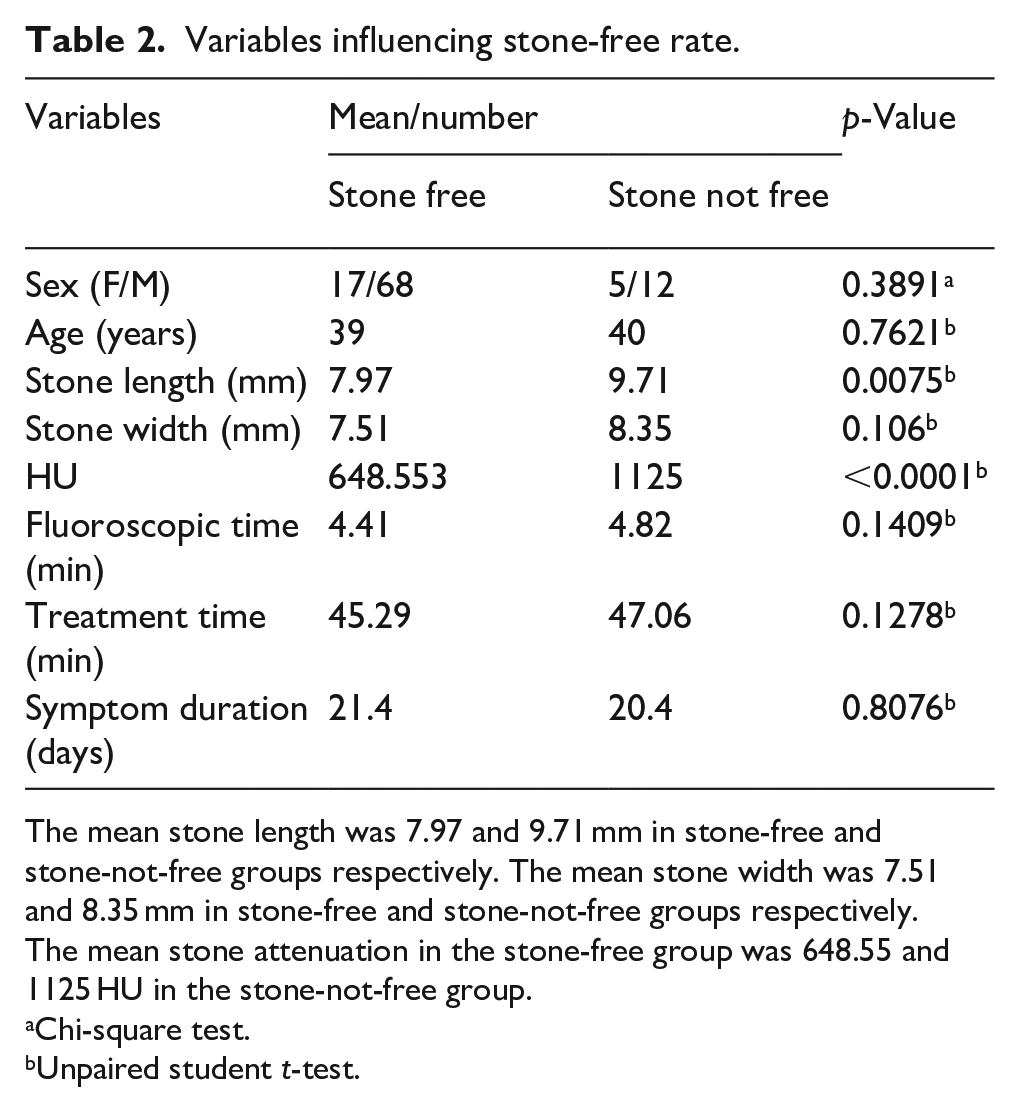
The mean stone length was 7.97 and 9.71 mm in stone-free and stone-not-free groups respectively. The mean stone width was 7.51 and 8.35 mm in stone-free and stone-not-free groups respectively. The mean stone attenuation in the stone-free group was 648.55 and 1125 HU in the stone-not-free group.
Chi-square test.
Unpaired student t-test.
For the purpose of result analysis based on stone dimensions, all volunteers were divided into three groups: based on length and width of stone (into groups of: ⩽7, >7–⩽10, and >10 mm) while on the basis of stone attenuation two groups were created (⩽900 and >900 HU) as these were the categorizations that yielded a significant difference on analyzing the compiled data at the end of study duration. Depending on the location of stone; patients were put into three groups, namely kidney/upper ureter (UU group), mid ureter (MU group), or lower ureter (LU group).
For stone length ⩽7 mm, SFR was 92.11% (35/38) compared to 82.93% (34/41) and 69.57% (16/23) for stone lengths of >7–⩽10 and >10 mm, respectively (p < 0.001).
For stone width ⩽7 mm, DFR was 86.79% (46/53) compared to 82.93% (34/41) and 62.5% (5/8) for stone widths of >7–⩽10 and >10 mm, respectively (p < 0.0001).
For stone attenuation ⩽900 HU, SFR was 97.18% (69/71) compared to 51.61% (16/31) for stone attenuation >900 HU (p < 0.0001).
Location of stone had no bearing on ESWL outcome as far as this study is concerned (p = 0.389) (Table 3).
Stone related factors influencing ESWL outcome.
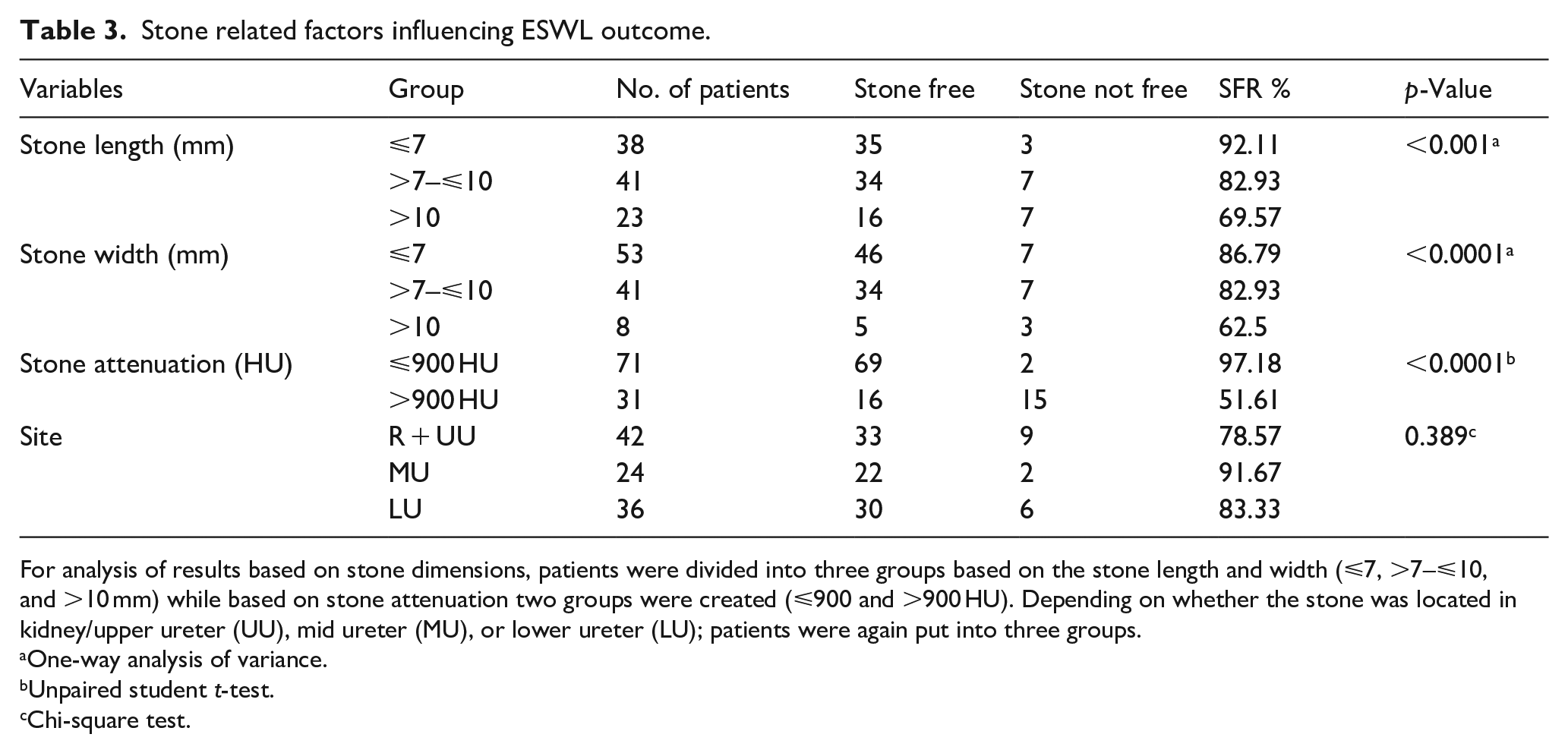
For analysis of results based on stone dimensions, patients were divided into three groups based on the stone length and width (⩽7, >7–⩽10, and >10 mm) while based on stone attenuation two groups were created (⩽900 and >900 HU). Depending on whether the stone was located in kidney/upper ureter (UU), mid ureter (MU), or lower ureter (LU); patients were again put into three groups.
One-way analysis of variance.
Unpaired student t-test.
Chi-square test.
None of the patients experienced respiratory distress or discomfort during positioning for ESWL. However, most patients did complain of transient hematuria and mild skin erythema. Four patients developed UTI post ESWL. Three of them were managed conservatively with culture-sensitive oral antibiotics while one patient was managed with iv antibiotics after admission. About 5 of 102 patients had refractory pain, and 2 of them needed inpatient treatment. None of these five patients needed endoscopic management.
Discussion
The various modalities available for ureteric calculi consist of conservative approach allowing spont aneous passage of stones, ESWL, URSL, and laparoscopic/open ureterolithotomy. Spontaneous clearance depends primarily on the dimension and site of calculus and also to a lesser extent, on the factors like observation time, severity of symptoms, degree of obstruction, etc. Spontaneous clearance of ureteric calculi falls in the range of 59%–69% for stones less than 5 mm. Incidence decreases significantly with an increase in stone size, with spontaneous clearance of stones measuring more than 5 mm being exceptional and are frequently apprehended by complications like persistent unrelenting pain, hydroureteronephrosis, and urosepsis.9,10
Ureteroscopy as a primary modality for ureteric calculi is hugely effective, with a success rate exceeding 90%. Its chief drawback lies in the fact that it is invasive, requires anesthesia mandating admission, and complications falling in the range of 1%–10%. 11
There has been an ongoing debate between ESWL and ureteroscopy for obstructing ureteral stones but still the value of eESWL to combat this situation has hardly been evaluated.5,6,12 To our utter surprise, even though ESWL is widely considered as one of the preferred options for ureteral stones, it’s use as an immediate therapeutic modality in emergency setting has not yet drawn much attention of investigators. Only a handful of investigators including Gonzalez et al., 7 Doublet et al., 5 Tligui et al., 6 and Tombal et al. 8 have published their studies advocating the utility of emergency ESWL.
Tligui et al. shared their experience of eESWL within 24 h in the year 2003. SFR fell in the range of 79%–83% depending on the site of stone and from 75% to 86% according to dimensions of the stone. On the basis of their results, they advocated a more rampant use of eESWL. Their results are in line with our findings. In our study, 76.47% of patients had their stones cleared after a single ESWL session while 23.53% had to undergo multiple ESWL sessions to achieve complete clearance.
Tombal et al. 8 in 2005 mentioned the reports of the first randomized trial addressing the role of eESWL in patients requiring hospitalization for ureteric colic. In their study they compared medical management versus eESWL. They concluded that eESWL is a valuable therapeutic option to improve elimination of ureteral stones and shorten the hospital stay, especially for stones located proximal to iliac vessels. In the present study, we delivered emergency ESWL on a daycare basis within 24 h of presentation and only 3 out of 102 patients required admission in view of urosepsis and refractory ureteric colic. Based on our results we strongly believe that it’s absolutely unnecessary to admit every patient of ureteric colic just for the sake of delivering emergency ESWL, only patients with some untoward complications mandate admission.
Various studies have worked on the factors predicting the outcome of ESWL upper urinary tract calculi. Almost all prior studies have documented an inverse relationship between stone dimensions and the ultimate outcome of ESWL for upper tract urinary stones.13 –15 In our study; length, width, and Hounsfield unit (HU) of stone turned out to be the three most important factors dictating the success of eESWL. Stones with length/width measuring <10 mm and attenuation <900 HU had a significantly better outcome in terms of SFR. Thus further emphasizing the fact that stone dimension by itself had an inverse impact on eESWL result.
The outcome of present study very well corroborate with prior studies further emphasizing the fact that age, gender, laterality, and nature of stone had no bearing on the final result.16,17
In the past few years, quite a few investigators have probed into the effect of symptom duration on the outcome of ESWL and have concluded that early ESWL may yield a better SFR. 18 The results obtained in our study were also on the same lines, further establishing the safety and efficacy of emergency ESWL both in terms of pain relief and stone clearance with minimal morbidity without the need for admission or any invasive procedure and thus reducing the cost and fewer absences from work.
The minor complications in the form of regional redness and transient hematuria were of similar magnitude to prior conducted studies. Although five patients had refractory unrelenting pain not relieved even after ESWL, by and large most patients (80/102, i.e. 78.43%) reported a satisfactory pain relief. This could be owing to better stone disintegration in initial session.
Results obtained in this study are at par with the routine ESWL delivered at our center in terms of SFR. The SFR at our center for routine ESWL is around 75% (which is by and large at par with the AUA meta-analysis report 4 ) while in this study the success rate of eESWL is over and above the success rate of our routine ESWL, possibly because of lesser degree of ureteral edema and inflammation in the emergency setting.
It’s been reported that renal stones have a sparingly better ESWL outcome as compared to ureteral stones but many others could not appreciate any such difference.19,20 However Pace et al. 21 did demonstrate a more favorable outcome for proximal and mid ureteric stones in contrast to distal calculi. In our study, location of stone had no bearing on the ESWL outcome.
AUA meta-analysis reports best stone clearance rate of 74% for stones measuring <10 mm in contrast to 46% for stones between 11 and 20 mm. 4 Our study reported similar findings with slightly better results. This may be confounded by the fact that our sample size was small and ESWL was given on an emergency basis. Also, we used both supine and prone positions to deliver ESWL depending on the location of stone to improve the stone localization and efficiency of shockwaves.
Many patients are compelled to undergo multiple shockwave sessions in order to achieve complete stone clearance. 4 No general consensus exists, dictating the optimal number of ESWL sessions prior to switching over to other existing modalities. Subsequent repeat ESWL sessions after failed initial treatment have reported a marginal improvement as substantiated by Pace et al. 21 Owing to minimal improvement in subsequent cumulative SFR, Kim et al. 22 advocated a maximum of three ESWL sessions. On comparing the outcome of single session of ESWL for ureteral calculi to subsequent sessions in order to determine the justification of multiple sessions, we found our results to be in line with the prior reported series. Hence we recommend not to deliver more than three ESWL sessions.
Limitations
The present study was carried out to determine the safety, efficacy, and feasibility of eESWL for obstructing ureteric and renal stones with colic. The entire study was carried out at an apex tertiary care center with a relatively small sample size and the study duration was also a bit short. A large multicenter study incorporating a large number of patients over a longer duration is required to further validate these results in various multiple strata.
Conclusion
Emergency ESWL is a feasible, efficacious, and safe alternative for definitive management of patients turning up with obstructing ureteral and renal stones with colic. This simple, non-invasive modality imparts a satisfactory outcome as far as stone clearance and rapid and definitive pain relief are concerned and that too with very minimal morbidity without the need for admission. It’s quite prudent to mention that it can certainly bring about a paradigm shift in reducing the prolonged waiting period for URSL/RIRS (which in turn may lead to significant morbidity in the form of hydronephrosis, pyonephrosis, and loss of renal function) in any high-volume tertiary care hospital. The length, width, and attenuation of stone are the main parameters dictating the success of emergency ESWL.
Footnotes
Author contributions
Ashutosh Kumar Tiwari: materials, data collection and processing, analysis and interpretation, writing, and literature review; Debansu Sarkar: conception, design, supervision, materials, analysis and interpretation, literature review, and critical review; Dilip Kumar Pal: conception, design, supervision, analysis and interpretation, literature review, and critical review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approved by Institutional ethics committee: Institute name: Institute of Postgraduate Medical Education and Research, Kolkata, India. Approval number: IPGME&R/IEC/2020/045. Date: 04/02/2020.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.