
Abstract
Objectives:
To evaluate the efficacy, safety, and patient-reported outcomes, including satisfaction and pain level, of electroconductive (EC) and electrohydraulic (EH) extracorporeal shock wave lithotripsy (ESWL) for the treatment of ureter and kidney stones in a randomized controlled trial.
Materials and methods:
A total of 56 patients were randomly allocated to the EC or EH groups. Patient and stone characteristics and treatment outcomes were compared.
Results:
The stone-free rates were not different between the groups. The EH group achieved the same stone-free rates as the EC group with less energy use. Pain scores were higher in the EH group (mean 4.76 ± 3.53) than in the EC group (mean 3.04 ± 2.84), with borderline significance (p = 0.063). Satisfaction scores and radiation exposure were significantly lower in the EH group than in the EC group, regardless of the stone location. Univariate and multivariate analyses identified the total number of shocks and stone location as significant predictors of stone-free status.
Conclusions:
EC and EH lithotripters demonstrated comparable efficacy and complication rates across different stone locations. While the EC group showed lower pain scores and higher satisfaction, these outcomes required greater energy use and resulted in higher radiation exposure. Patient satisfaction and pain level, as patient-reported outcomes, may be considered as additional measures alongside safety and efficacy in the evaluation of ESWL modalities.
Keywords
Introduction
Extracorporeal shockwave lithotripsy (ESWL) has attained broad recognition as a highly regarded minimally invasive approach for managing urinary stone disease. The treatment approach to urinary stone disease has undergone significant transformations since the clinical utilization of ESWL. 1 Advancements in ESWL technology have contributed to greater efficacy in its application, while minimal morbidity associated with the procedure has bolstered its effectiveness. Several factors influence the success of ESWL, including stone size, location, composition, the type of lithotripter employed, the operator’s level of experience, the utilization of repetitive sessions, and the shockwave delivery parameters, such as the number of shocks, energy level, and frequency. 2
Among these variables, the type of lithotripter may significantly influence treatment success. The core component of a lithotripter is its shockwave generator. Presently, electromagnetic (EM), electrohydraulic (EH)/electroconductive (EC), and piezoelectric generators are utilized. EH type generates shockwaves via electrode sparks. EC type, derived from EH, features electrodes in a conductive solution for consistent sparks and reduced wear. 3 In the early stages of development, EH-type lithotripters were prevalent due to their remarkable efficacy and lower retreatment rates. 4 However, research on EC-type lithotripters needs to be expanded, with studies yielding inconsistent results, including instances where the lithotripsy outcomes were comparable to or inferior to those of other types of lithotripters. 5 Furthermore, randomized controlled trials investigating the efficiency and safety of EC-type lithotripters are scarce, contributing to the current lack of comprehensive understanding.
Therefore, this study aimed to investigate whether comparable outcomes in stone-free rates and safety could be attained from two different lithotripters, specifically EC and the EH-type lithotripters, while evaluating the performance of the EC lithotripter equipped with an embedded ultrasound for targeting. In addition to safety and efficacy, patient-reported outcomes such as satisfaction and pain level were also evaluated, reflecting a broader perspective in assessing ESWL performance.
Materials and methods
Study design
The Institutional Review Board approved the study protocol of this randomized, controlled trial (IRB: 2003-046-1108). Between March 2022 and May 2023, 56 patients were prospectively enrolled and randomized to either the EC or EH groups at a single center. Only unilateral stones were included; patients with bilateral calculi were excluded. This study was designed as a pilot trial, with a target of 25 cases per arm. Allowing for a 10% dropout rate, 28 patients were allocated per group. The sample size was based on feasibility, as no formal power calculation could be performed due to limited prior data. All personal identifiers were removed prior to analysis. The study followed CONSORT guidelines.
Eligible patients presented with stones located in the upper kidney or ureter, with diameters of 5–15 mm. Patients with musculoskeletal deformities, active urinary tract infection requiring immediate treatment, bleeding diathesis, or ureteral obstruction precluding stone passage were excluded due to technical challenges in performing ESWL. Written informed consent was obtained from all participants. The primary endpoint was the stone-free rate. Secondary endpoints were patient-reported outcomes, including pain (assessed by Visual Analog Scale (VAS)) and treatment satisfaction evaluated using a standardized 5-point Likert scale: 1 = very dissatisfied, 5 = very satisfied). Adverse events such as hematuria, steinstrasse, fever, infection, and bleeding were prospectively recorded and graded according to the Clavien–Dindo classification.
Treatment protocol
Patients were allowed to pause treatment if discomfort occurred, and shockwave intensity was adjusted accordingly. ESWL was performed without anesthesia; however, procedures were terminated early in cases of intolerable pain. Stone-free status and fragmentation were evaluated by non-contrast computed tomography (CT) performed 1–2 weeks post-treatment.
If patients experienced discomfort during the procedure, they were allowed to take a break, and the investigators had the flexibility to adjust the shockwave level accordingly. The ESWL procedure was performed without any specific anesthesia. However, if a patient complained of severe pain, the ESWL procedure was stopped early. Approximately 1–2 weeks after lithotripsy, a non-contrast kidney computed tomography (CT) scan was conducted to confirm fragmentation of the calculi and stone-free status. The level of pain experienced by patients was monitored throughout the ESWL process to ensure safety, and was also systematically assessed as a patient-reported outcome.
Comparison of two types of generators: Electroconductive and electrohydraulic
ESWL was performed using an embedded ultrasonic electroconductive Sonolith i-move® shockwave lithotripter (EDAP, Lyon, France) and an electrohydraulic Rifle lithotripter (HNT Medical, Seoul, Korea). A total of 2000–3000 shockwaves were administered per session, with a pause and subsequent resumption of the procedure to deliver up to 1300 shockwaves if a patient reported severe pain, resulting in early termination. We employed the ramping technique, and when increasing the energy, we proceeded with the intensity of the previous stage if the patient reported discomfort. A ramping protocol was applied, defined as a stepwise increase in shockwave energy beginning at a low level and raised every few 100 shocks according to patient tolerance and fragmentation progress.
Randomization
A random allocation list was generated for 56 subjects using a block randomization method to minimize imbalance between the patient groups. Block randomization was performed using an independent online randomization tool. Allocation concealment was ensured with sealed opaque envelopes prepared by a research assistant not involved in patient care. The envelopes were opened by the professional nurse upon the patient’s arrival in the ESWL suite. Patients were not stratified by stone location; however, subgroup analyses of ureteral versus renal stones were performed.
Shockwave energy levels
The shockwave intensity in the EC group is expressed as a percentage and could be adjusted in 20 steps, ranging from 5% to 100% at 5% increments. For the EH group, shockwave level adjustment was performed in 10 steps, ranging from levels 1 to 10. Lithotripsy was performed by gradually increasing the shockwave intensity from low to high while evaluating the fragmentation of the stones and assessing the patient’s pain levels. We adjusted the levels of both the EC and EH groups while gradually increasing the shockwave intensity to match the shockwave intensity at the same level. The ureter and kidney were treated with shockwaves at distinct energy levels (Supplemental Table 1). The initial targeting was performed using embedded ultrasound, with combined X-ray and ultrasound checks conducted every 500 cycles to evaluate stone fragmentation.
Data collection and outcomes
The following data were extracted from the patient’s medical records: age, sex, body mass index (BMI), stone location, maximum stone diameter, Hounsfield unit (HU) measured through CT scans, and number of stones. The volume of the stone was calculated by multiplying the length, width, and height, and then applying a constant of 0.523. As determined by kidney CT, stone-free status was defined as the absence of residual fragments or fragments smaller than 3 mm of the target stones. Treatment success was defined as achieving a stone-free status within 2 weeks after the single SWL session without requiring additional auxiliary treatment. The outcomes reflect single-session treatment results, which may partly explain the relatively lower stone-free rates compared to some published studies reporting multi-session outcomes. Visual analog scale (VAS) scores were used to assess pain intensity and safety assessment, with analgesics prescribed to patients experiencing severe pain. The total energy values of the lithotripters were obtained by multiplying the number of shocks with the energy values calculated from voltage and frequency.
Statistical analysis
Descriptive statistics were employed to analyze the characteristics of the patient group, and the Mann–Whitney U test was utilized for group comparisons. The variables were examined to assess associations with the actual values of age, gender, stone location, laterality, and procedural events. Chi-square analysis was employed to investigate associations among categorical variables. IBM SPSS Statistics ver. 26.0 (IBM Co., Armonk, NY, USA) was employed for statistical analysis, and a two-tailed p-value of <0.05 indicated statistical significance. Univariate and multivariate logistic regression analyses were performed to calculate odds ratios with 95% confidence intervals (CIs) for predicting the stone-free status, with adjustments made for potential confounding factors.
Results
A total of 56 patients were randomly allocated into the EC or the EH groups (Figure 1). Six patients were excluded from the analysis due to either the absence of visible stones during treatment, fever or the withdrawal of consent. No statistically significant differences were found in patient data or stone characteristics in the two groups, including the stone size and volumes, except for BMI values (Table 1).
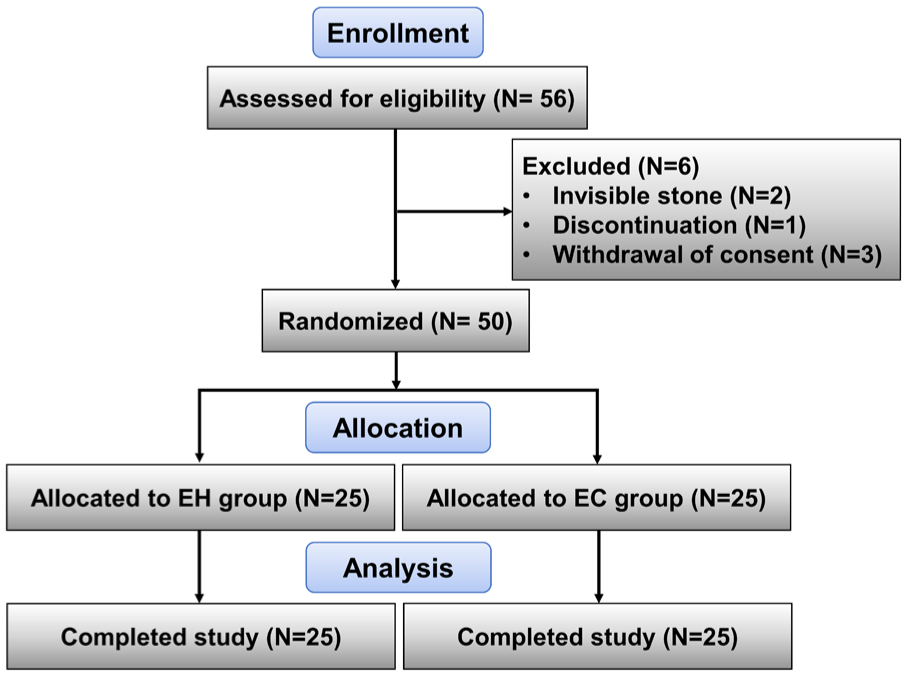
Flow diagram of the study.
Demographic data comparisons between EC and EH groups.
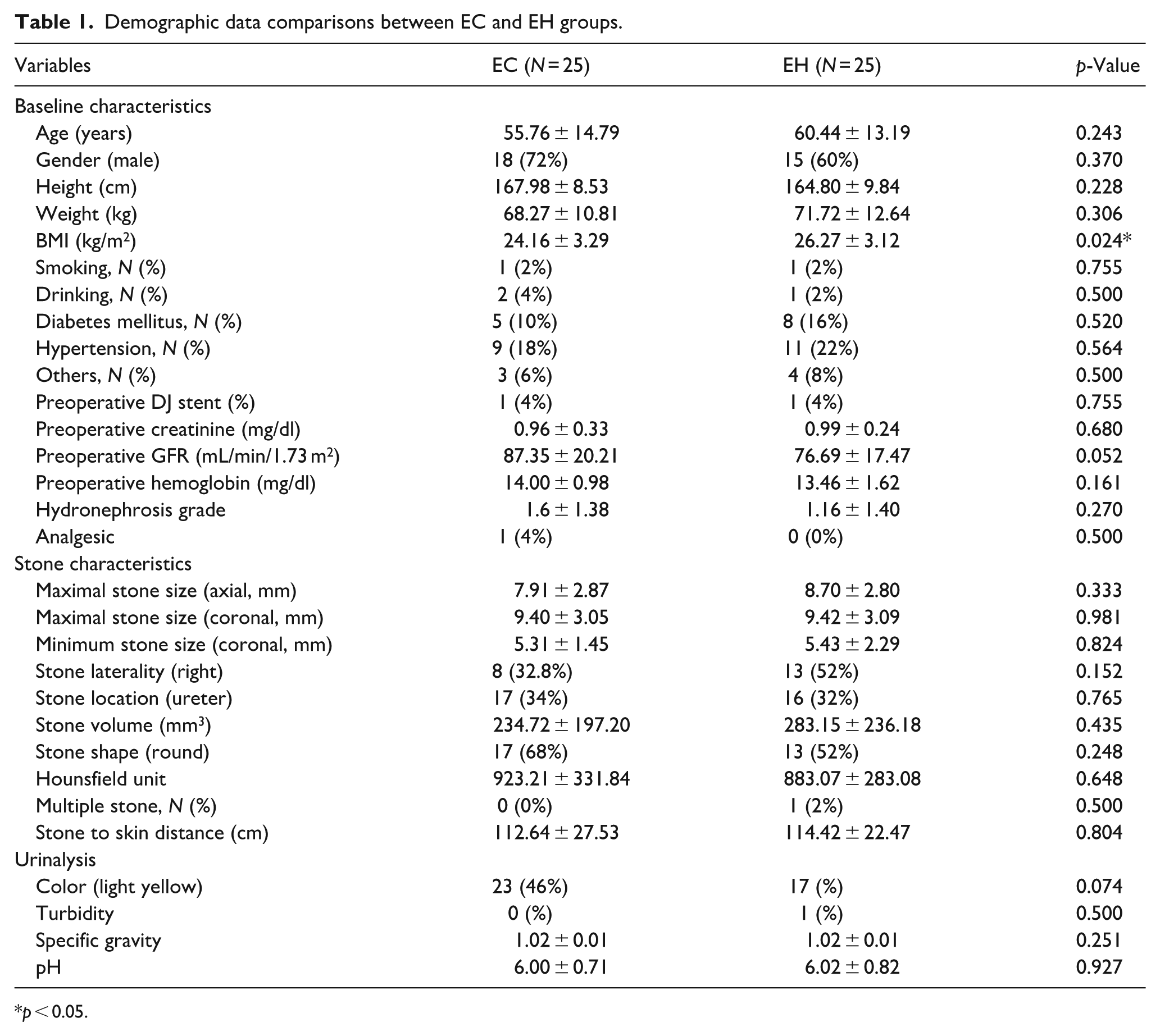
p < 0.05.
Baseline distribution of stone location was balanced between the two groups (p = 0.765). Both groups showed similar stone-free rates, indicating comparable stone fragmentation treatment outcomes (Table 2). After the single-session procedures, the stone-free rate in the EC group was 60% (15 out of 25 cases), while in the EH group, it was 52% (13 out of 25 cases; p = 0.569). In contrast, a statistically significant difference in total energy values was observed between the two groups. The total energy values were 681.96 ± 120.4 J and 513.08 ± 159.49 J for the EC and EH groups, respectively (p < 0.001). The EH group achieved the same stone-free rates as the EC group while using significantly less energy during the procedure. The total number of shocks in the EC group was 2776 ± 413.6, whereas it was 2584 ± 593.49 in the EH group, which was a slightly lower value (p = 0.192). Regarding VAS pain scores and satisfaction scores, the EC group had a lower mean score of 3.04 ± 2.84 versus 4.76 ± 3.53 in the EH group (p = 0.063) and a higher mean score of 3.80 ± 0.96 versus 3.08 ± 1.00 (p = 0.012). However, analgesics were prescribed for only one patient in the EC group and were not required for others. There were no complications, such as fever or bleeding, among the subjects analyzed.
Comparing outcomes in EC and EH groups.
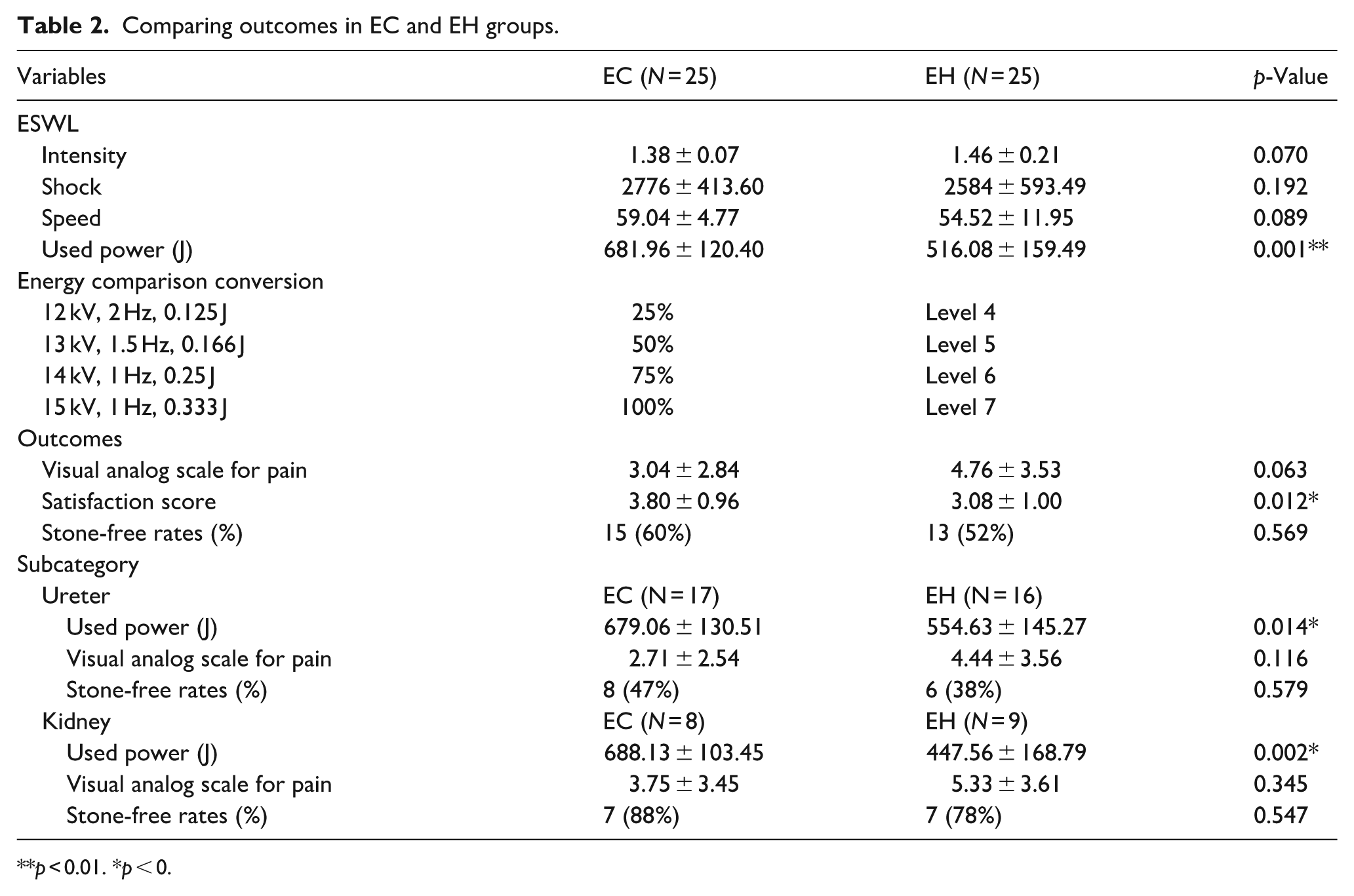
p < 0.01. *p < 0.
The results remained consistent when the two groups were divided into ureter and kidney subgroups. The total energy used in the EC ureter subgroup was 679.06 ± 130.51 J, whereas, in the EH group, it was 554.63 ± 145.27 J (p = 0.014), indicating that the EH group utilized significantly less energy. Regarding the stone-free rate in the ureter subgroup, there was no significant difference between the EC group (8 out of 17 cases, 47%) and the EH group (6 out of 16 cases, 38%; p = 0.579). Similarly, in the kidney subgroups, the total energy used was 688.13 ± 103.45 J and 447.56 ± 168.8 J in the EC group and the EH group, respectively (p = 0.002), highlighting the significantly lower total energy in the EH group. There was no significant difference in the stone-free rate in the kidney subgroups between the EC group (7 out of 8 cases, 88%) and the EH group (7 out of 9 cases, 78%; p = 0.547).
Univariate and multivariate logistic regression analyses revealed that the total number of shocks and stone location were significant predictors of stone-free status (Table 3). Finally, the cumulative radiation exposure dose in the EC group, which utilized the ultrasound-embedded lithotripter, was 0.41 mGy, whereas the EH group was exposed to 0.31 mGy. Thus, the EC group had a higher radiation exposure dose than the EH group.
Univariate and multivariate logistic regression analyses.
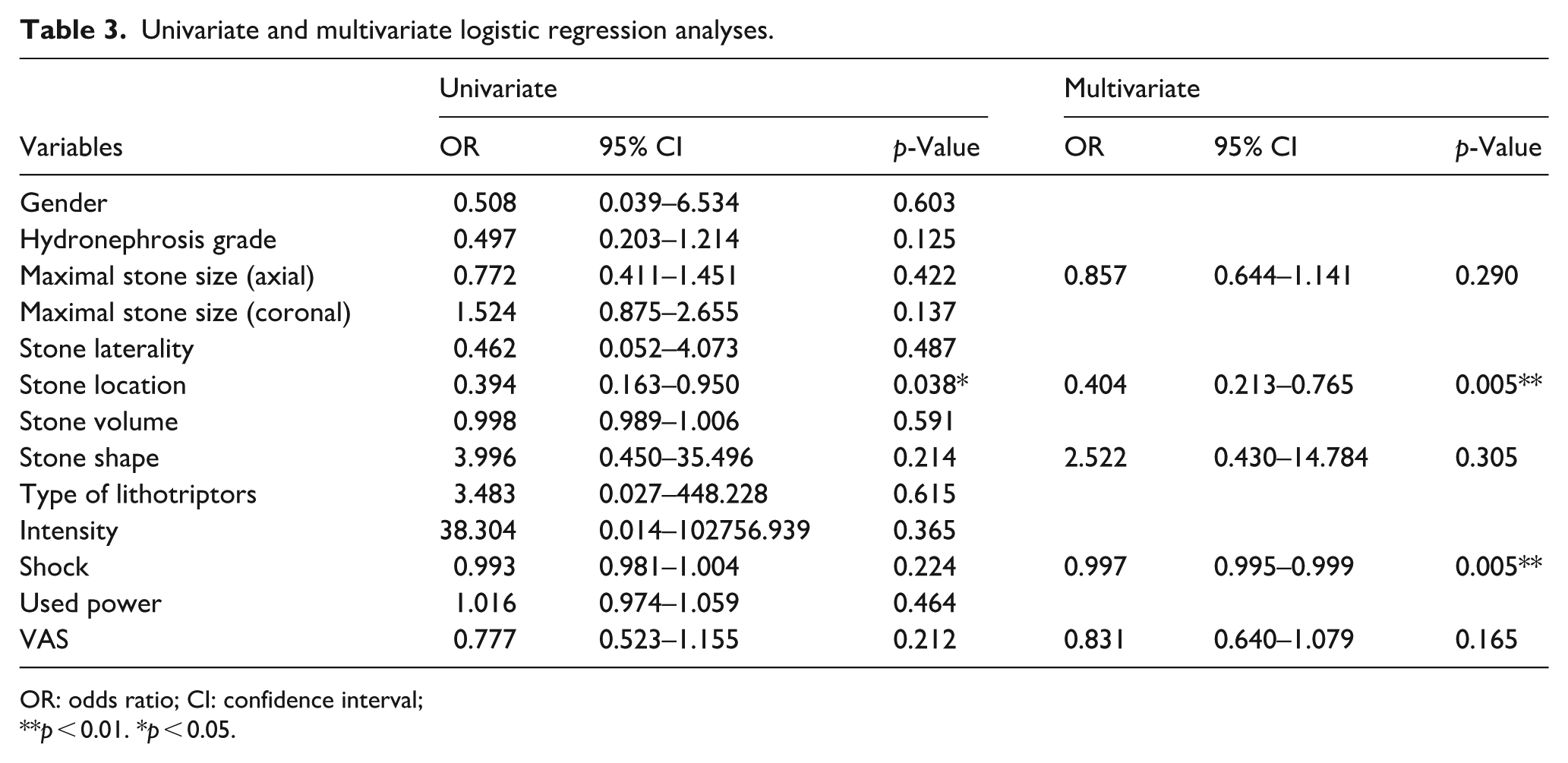
OR: odds ratio; CI: confidence interval;
p < 0.01. *p < 0.05.
Discussion
EH lithotripters have traditionally demonstrated favorable outcomes, with high stone-free rates and low retreatment rates. They have shown particular effectiveness in treating ureteral stones larger than 1 cm and in managing lower and mid-ureteral stones. 6 Experimental models further support their ability to fragment stones rapidly with minimal renal parenchymal injury, even under high-frequency shock waves. 7 With the development of newer EH lithotripters, stone-free rates and safety profiles have continued to improve. 8
EC lithotripters, developed as a modification of EH technology, were designed to generate more consistent sparks and reduce electrode wear through the use of a conductive medium.9–12 However, their clinical performance has been variably reported. For instance, Ng et al. 13 demonstrated that slower shockwave delivery (60 vs 120 shocks/min) with EC devices improved fragmentation for stones >10 mm without increasing pain or analgesic use. In contrast, Faragher et al. 14 reported that EC lithotripters were less effective than EM or piezoelectric devices in vitro. A more recent comparative analysis showed no statistically significant differences in fragmentation efficacy among EH, EC, and EM devices, although EH was associated with higher pain scores. 15
The variance in fragmentation efficacy among lithotripter types may be partially explained by differences in electrode design and performance. One drawback of the EH generator is the requirement for electrode replacement before each procedure, which increases cost and can be cumbersome in clinical practice. 14 Nevertheless, EH lithotripters remain widely used because they consistently achieve robust fragmentation effects.
In the present randomized trial comparing EH and EC devices, we found that the EC group reported slightly less pain and higher treatment satisfaction, but also experienced greater radiation exposure, likely because the EC device used in this study was equipped with built-in ultrasound that required frequent combined focusing with X-ray. While we expected differences in fragmentation efficiency related to the integrated ultrasound system, these differences were not statistically significant, most likely due to the limited sample size of this pilot trial. Stone-free rates were similar between the two devices. However, the absolute stone-free rates observed in our study (60% vs 52%) were lower than those reported in many previous series. Several factors may explain this discrepancy. First, our outcomes were based on a single ESWL session, whereas many published studies report cumulative results after multiple treatment sessions.4,16,17 Second, our follow-up evaluation was conducted at 1–2 weeks, while many prior trials assess outcomes at 4–6 weeks or longer, providing more time for the spontaneous passage of residual fragments. 2 Taken together, both the single-session design and the short follow-up window may have contributed to an underestimation of the true stone-free rate in our study population.
We also observed that the EH group achieved comparable stone-free rates while using significantly lower total energy than the EC group. This finding is in line with prior experimental evidence that high energy and higher shock counts can enhance fragmentation but are also associated with increased risk of renal parenchymal injury. 9 Previous randomized trials have shown that stepwise ramping of energy can reduce acute renal damage while preserving fragmentation efficacy.16,17 Our findings similarly emphasize the importance of balancing fragmentation efficiency with safety considerations. Indeed, excessive shockwave exposure has been associated with acute kidney injury and biochemical alterations. 18
Multivariate analysis in our study identified stone location and the total number of shocks as significant predictors of stone-free status, which is consistent with prior predictive models. 2 Interestingly, our data showed that stone-free outcomes were achieved at lower shock counts than might be expected, suggesting that optimized energy delivery and stone characteristics may play a greater role than shock count alone.
Pain control during ESWL also deserves consideration. Although the procedure is typically performed without anesthesia, patients often experience variable discomfort. In our trial, the EC group reported lower mean VAS scores and higher satisfaction, underscoring the value of integrating patient-reported outcomes into evaluations of ESWL modalities. Patient comfort and acceptance are key determinants of treatment success and compliance.
Finally, subgroup analysis revealed that fragmentation was more favorable in the kidney stone group compared to the ureter stone group. This finding is consistent with previous comparative studies.6,19 Anatomical differences in tissue support, stone mobility, and calyceal structure may partly explain these results. Interestingly, in our cohort, technical parameters such as excitation energy intensity and radiation dose were not major determinants of success, suggesting that stone-related and anatomical variables may exert stronger influence on fragmentation outcomes.
Limitations
This study has several limitations. First, it was a pilot study with a small sample size and no formal power calculation, restricting the robustness of subgroup analysis. Second, it was conducted at a single center, which may limit generalizability. Third, randomization was not stratified by stone location, although baseline balance was confirmed and subgroup analyses were performed. Fourth, follow-up was limited to 1–2 weeks, which may underestimate stone-free rates compared to longer-term assessments. Finally, our study included only EH and EC lithotripters; exclusion of EM devices prevented a complete comparison across all available modalities. Future multicenter studies with larger cohorts, longer follow-up, and inclusion of EM devices are warranted to provide more definitive guidance for device selection.
Conclusions
EC and EH lithotripters yielded similar stone fragmentation, complication rates, and overall safety, regardless of stone location. The EC group showed lower pain scores and higher patient satisfaction, although more energy was used and radiation exposure was higher. These patient-reported outcomes were evaluated alongside efficacy and safety in the assessment of ESWL modalities.
Supplemental Material
sj-docx-1-urj-10.1177_03915603251390743 – Supplemental material for A randomized controlled trial comparing efficacy, safety, and patient-reported outcomes of electroconductive and electrohydraulic extracorporeal shockwave lithotripsy
Supplemental material, sj-docx-1-urj-10.1177_03915603251390743 for A randomized controlled trial comparing efficacy, safety, and patient-reported outcomes of electroconductive and electrohydraulic extracorporeal shockwave lithotripsy by Hyeji Park, Christine Joy Castillo and Sung Yong Cho in Urologia Journal
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
This study was approved by the institutional review boards of Seoul National University Hospital (IRB: 2003-046-1108). All methods were carried out in accordance with relevant guidelines and regulations.
Consent to participate
Informed consent was obtained from all patients.
Consent for publication
Not applicable.
Author contributions
Christine Joy Castillo was involved in data acquisition. Hyeji Park was responsible for statistical analysis and interpretation, while Sung Yong Cho participated in data acquisition, analysis, and interpretation, conducted statistical analysis, drafted the manuscript, contributed to the study’s concept and design, and supervised the entire study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health and Welfare, the Ministry of Food and Drug Safety; Project Number: 1711194216, RS-2020-KD000010) and partially SNUH funding (HI20C2092).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used during the current study available from the corresponding author on request.
Trial registration
ClinicalTrials.gov, NCT06144372. Registered November 20th, 2023 – Retrospectively registered.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.