
Abstract
Life-space mobility (LSM) in older adults is influenced by physical, cognitive, and psychological states. However, the relationship between LSM and personality traits remains unclear. Thus, our cross-sectional study investigated this correlation, which included 144 participants aged ≥60 years. LSM was assessed using the life-space assessment (LSA), and personality traits were evaluated using the Japanese version of the Ten-Item Personality Inventory (TIPI-J). Physical data were also collected. Univariate analyses revealed that among young-older adults, extroversion in the TIPI-J showed a significant association with LSA scores in addition to handgrip strength. Among old-older adults, openness to experience in the TIPI-J demonstrated a significant association with LSA scores in addition to quadriceps strength. This study revealed correlations between personality traits (extroversion and openness to experience) and LSM, in addition to physical function. Considering older adults’ personality traits is crucial for designing support and interventions to maintain and expand LSM.
• Physical function and personality traits correlate with life-space mobility in older adults. • Biographical factors associated with life-space mobility vary with age. • Extraversion in young-older adults and openness to experience in old-older adults were significantly associated with enhanced life-space mobility.
• Personality traits along with physical strength should be assessed in older community-dwelling adults. • Interventions to improve life-space mobility in gerontological practice should consider personality traits and physical function. • Personality testing is not presently common in treatment plans but holds great potential for quality-of-life improvement for older adults in clinical settings.What this paper adds
Applications of study findings
Introduction
Maintaining an independent lifestyle and preserving mobility form the foundation for active aging (World Health Organization [WHO], 2023a). Mobility in daily life is assessed in terms of physical mobility, resilience to physical decline, and evaluation of social isolation among community-dwelling older adults. It is associated with factors including physical and cognitive function, history of falls, healthcare utilization, admission to care facilities, and mortality rates (Taylor et al., 2019). The utilization of medical care facilities and services directly affects social insurance costs. Achieving an active lifestyle while aging and sustaining mobility contribute not only to a healthier society but also to economic stability.
A conceptual framework defines mobility through seven zones: Room, home, outdoors, neighborhood, service community, surrounding area, and world. Several studies have investigated the factors related to mobility in older adults (Webber et al., 2010). Of the various comprehensive physical, cognitive, and psychosocial conditions, walking speed and driving are associated with mobility (Kuspinar et al., 2020). Among the factors influencing changes in mobility, walking speed was the most notable (Kennedy et al., 2019). In addition to walking ability, fatigue is associated with mobility (Moored et al., 2022), and exercise tolerance can influence the range of activities. Mobility is influenced by musculoskeletal pain, but the interpretation of the relationship between pain and mobility varies in research reports (Kuspinar et al., 2020; Uchida et al., 2020; Uhm et al., 2020). The frequency of going outdoors is related to both the gradual decline in physical function over time and the recovery of mobility function, and it is also associated with the physical function prognosis (Fujita et al., 2006). Psychological states including kinesiophobia (Uchida et al., 2020) (the fear of movement), psychological fatigue (Moored et al., 2022), and cognitive function (De Silva et al., 2019) also play a role in mobility. Social isolation can lead to a decline in daily functioning, especially in men (Fujiwara et al., 2017). Both social withdrawal and isolation increase the risk of mortality (Sakurai et al., 2019).
Mobility is influenced by several factors. Webber, in conceptualizing the theoretical framework for older adults’ mobility, identified five factors: Physical, cognitive, psychosocial, environmental, and financial. Additionally, sex, culture, and biographical influences are considered relevant (Webber et al., 2010). Previous research has predominantly focused on examining physical and cognitive factors.
When evaluating the mobility of older adults (Kalu et al., 2022), psychological factors, such as self-efficacy, fear of falling, depression, anxiety, and personality, are considered. Even if older adults are in good physical function, it is not necessarily guaranteed that they will have a wide range of mobility, and psychological evaluation is also necessary (Shimada et al., 2010). Even with similar physical and cognitive conditions, we believe that the life-space mobility (LSM) of older adults—how they move, engage, and participate in society—is associated with their personality traits. For example, driving skills can be influenced by human factors, such as attention, emotions, and stress (Fuller, 2005). Older adults with higher extraversion tend to have a broader range of mobility (Barnes et al., 2007; Ndubuaku et al., 2023). Moreover, older adults with more neuroticism are more prone to impaired mobility (Boyle et al., 2010). While there are some scattered studies focusing on factors related to personality and mobility in community-dwelling older adults, studies focusing on these factors are limited compared to studies focusing on physical and cognitive factors. Moreover, reports focusing on Japanese individuals are even more rare. Therefore, we aimed to introduce a novel perspective by focusing on personality as it relates to the LSM of community-dwelling older adults in Japan and elucidate the correlation between LSM and personality traits.
Methods
Study Design and Participants
This cross-sectional study was conducted between January and November 2023 and was conducted following the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants. This study was approved by the Research Ethics Committee of the Takasaki University of Health and Welfare (Approval No. 2240).
The inclusion criteria for participants were: (1) aged ≥60 years; (2) independent in activities of daily living; (3) able to independently go out to places including community centers; and (4) able to walk indoors without the use of assistive devices including canes.
Measurements
All measurements were taken at the community centers. Information on age, sex, morbidity, need for support or care, and history of falls within the past year was collected as part of the assessment of participants’ general characteristics using a questionnaire.
Life-Space Assessment
The University of Alabama at Birmingham Study of Aging Life-Space Assessment (LSA) (Baker et al., 2003) and the LSA in institutionalized settings (Hauer et al., 2021) were identified as the most suitable LSM questionnaires for assessing individuals in community settings (Johnson et al., 2020; Ullrich et al., 2022), and the validated Japanese version of the LSA (Harada et al., 2010) was used in this study. In the LSA, participants indicated whether they had visited each of the five life-space levels: (1) their bedroom to other rooms, (2) the yard, (3) the neighborhood, (4) the town, and (5) beyond the town, by selecting “yes” or “no” (yes = 1, 2, 3, 4, or 5; no = 0). They also noted the frequency of such visits during the previous week (less than once a week = 1, 1–3 times a week = 2, 4–6 times a week = 3, and daily = 4) and their level of independence (independent = 2, using equipment = 1.5, and requiring personal assistance = 1). Life-space level-specific scores were computed by multiplying whether the participant visited that level, the frequency of visits, and the degree of independence. The scores for the five life-space levels were summed to generate the LSA score, with a range of 0–120. A higher LSA score indicated greater LSM. This information was collected using a questionnaire, with trained surveyors assisting in obtaining responses whenever there were doubts about the questions.
Ten-Item Personality Inventory
The Japanese version of the Ten-Item Personality Inventory (TIPI‒J) (Oshio et al., 2012) based on the Big Five theory was employed. The TIPI‒J is a Japanese version of the TIPI scale that (Gosling et al., 2003) measures personality and has demonstrated retest reliability and concurrent validity. According to the Big Five theory, personality is divided into five traits: extraversion, agreeableness, conscientiousness, emotional stability, and openness to experience. In this context, high extraversion is associated with sociability and optimism; high agreeableness is linked to a preference for cooperation with others and a strong tendency toward altruistic behavior; high conscientiousness is related to a strong sense of self-control and a preference for self-discipline; high emotional stability indicates relaxed, not anxious or easily stressed; and high openness to experience suggests a lack of restraint by existing values with a high level of intellectual curiosity. Each trait was scored on a scale ranging from 2–14 points, with higher scores indicating a stronger presence of that trait. This information was also collected using questionnaires, similar to the LSA.
Physical, Cognitive, and Psychological Assessment
Physical assessments included measurement of appendicular skeletal muscle mass index (ASMI), handgrip strength, quadriceps strength, comfortable walking speed (CWS), and the Brief Balance Evaluation Systems Test (BESTest) (Padgett et al., 2012).
We used a multifrequency bioelectrical impedance analyzer, specifically the InBody 270 (InBody Japan, Tokyo, Japan), to calculate the ASMI. The ASMI, a parameter commonly employed for the evaluation of sarcopenia (Chen et al., 2020), was determined by dividing the total muscle mass of all four limbs by the square of the participant’s height. Handgrip and quadriceps strength were measured twice, focusing on the dominant hand or limb, which was determined as the limb responsible for kicking a ball. A digital dynamometer (Grip-D, Takei Scientific Instruments Co. Ltd, Niigata, Japan) and a handheld dynamometer (μ-Tas F-1, Anima Corp., Tokyo, Japan) were used to record the stronger of the two measurements. Quadriceps strength was divided by the individual’s body weight. These measures demonstrated reliable results when applied to older adults (Bohannon, 2017; Schaubert & Bohannon, 2005). For the 4-meter CWS test, participants were instructed to walk at a comfortable pace over a 4-meter distance, with an additional 1-meter designated for acceleration and deceleration zones (Rydwik et al., 2012). Balance was assessed using the Brief-BESTest (Padgett et al., 2012), a condensed version of the BESTest (Horak et al., 2009) with proven reliability and validity for balance assessments (Viveiro et al., 2019). The maximum score on the Brief-BESTest is 24 points, with higher scores indicating better balance.
Moreover, recognizing the association of cognitive function and psychological state with mobility, we measured the Recognition of Deterioration in Senility Test (RDST) (Kalbe et al., 2003) as a brief cognitive function assessment, along with the Falls Efficacy Scale-International (FES-I) (Yardley et al., 2005) to evaluate self-efficacy regarding falls. Physical and cognitive function assessments were conducted by trained surveyors before the study, with careful consideration given to falls and pain during the assessments.
Statistical Analysis
To identify factors influencing LSA and address potential biases resulting from missing data, the hot-deck imputation method was applied, assuming that the missing data occurred completely at random (MCAR). The MCAR condition was tested using Little’s test; however, it was challenging to definitively confirm the MCAR using only the observed data (White et al., 2011). Therefore, discrepancies between the imputed and complete data were assessed using the Mann–Whitney U test (Dong & Peng, 2013).
As the LSA score did not exhibit a normal distribution according to the Shapiro-Wilk test (p < .001), and the residuals in the multiple regression analysis were not normally distributed according to a quantile-quantile plot, non-parametric analysis methods and a generalized linear model (GLM) were used. Univariate analyses were performed to investigate the relationship between the LSA score and factors, including age, ASMI, handgrip strength, quadriceps strength, CWS, Brief-BESTest, FES-I, and RDST, using Spearman’s rank correlation coefficient. LSA scores were compared among sexes and those with and without multimorbidity/a history of falls using the Mann–Whitney U test. Multimorbidity was defined as having more than one chronic disease (WHO, 2023b).
A GLM with a gamma distribution and a logit link function was used to explore the association with the LSA score. Collinearity among the independent variables was assessed using variance inflation factors (VIF), under the condition that VIF should be less than five. We conducted a two-stage analysis to confirm whether the LSA is associated with physical and cognitive conditions in this population, as demonstrated in previous studies. Model 1 was based on this premise, while Model 2 included personality traits in the analysis. In Model 1, the LSA score served as the dependent variable, and independent variables were selected from the univariate analysis results if their p-values <0.1 among measurements other than the TIPI-J. Furthermore, we employed a stepwise variable-selection method using the Akaike information criterion as an exploratory approach to determine the most crucial covariates. Next, we analyzed Model 2 by adding each TIPI-J trait as a dependent variable. In Japan, there is a noticeable decline in physical and cognitive conditions in individuals around 75 years old (Satake et al., 2017), leading to differences in healthcare insurance systems beyond this age threshold. Therefore, in addition to analyzing all participants, separate analyses were conducted for participants aged <75 and ≥75 years. A complete case analysis was performed as a sensitivity analysis for model validation.
In multivariate analyses such as GLM, it is recommended to have a sample size that is 10 to 15 times the number of independent variables. The dependent variable is LSA, and the following 11 variables—age, sex, history of falls, ASMI, handgrip strength, quadriceps strength, CWS, Brief-BESTest, FES-I, RDST, and TIPI-J trait—were considered as candidate independent variables. Consequently, a target sample size of 110 was set.
All statistical analyses were conducted using R version 4.3.1 (The R Foundation for Statistical Computing, Vienna, Austria), and statistical significance was defined as p < .05.
Results
Characteristics of study participants (n = 144).
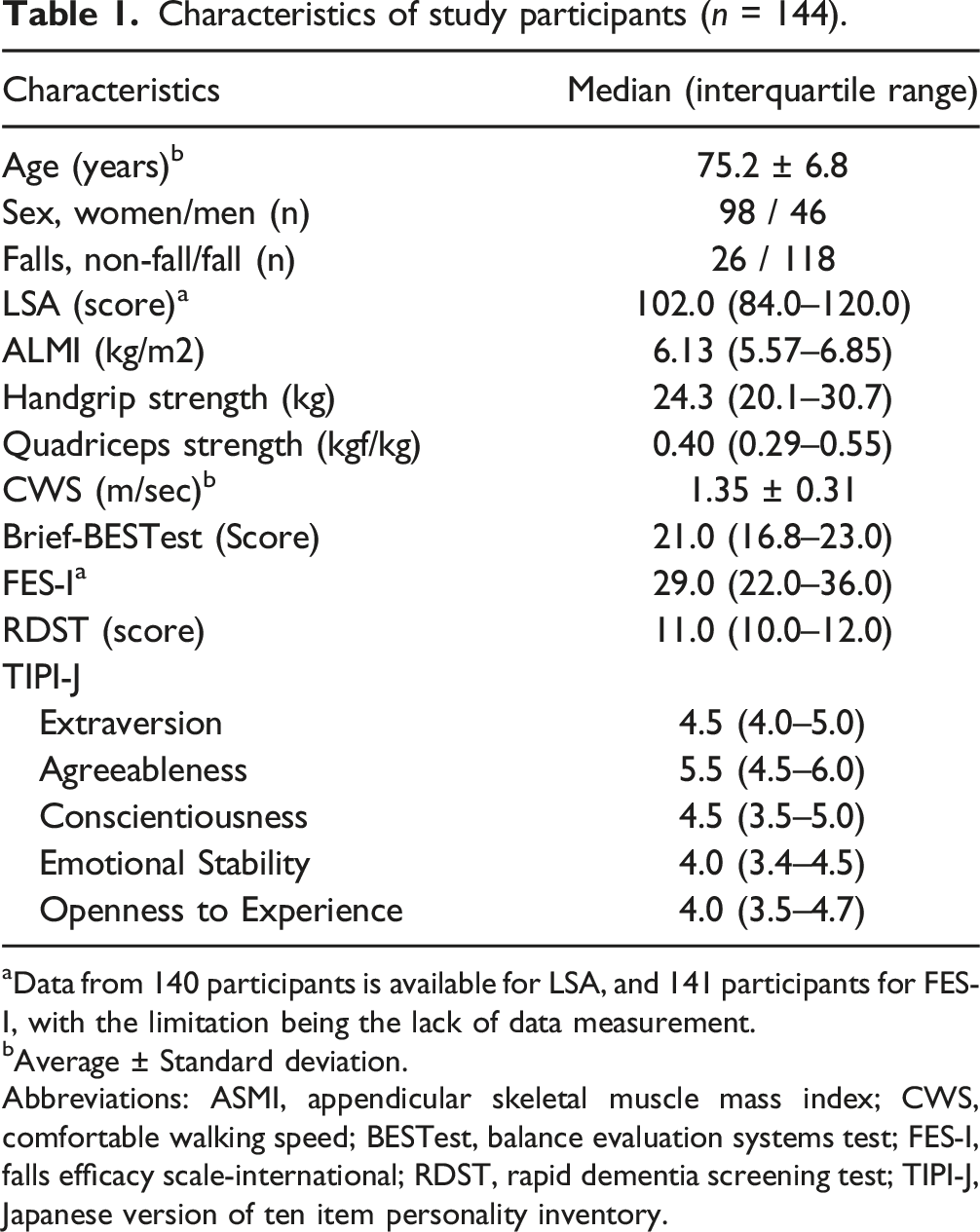
aData from 140 participants is available for LSA, and 141 participants for FES-I, with the limitation being the lack of data measurement.
bAverage ± Standard deviation.
Abbreviations: ASMI, appendicular skeletal muscle mass index; CWS, comfortable walking speed; BESTest, balance evaluation systems test; FES-I, falls efficacy scale-international; RDST, rapid dementia screening test; TIPI-J, Japanese version of ten item personality inventory.
The associations with the LSA score.
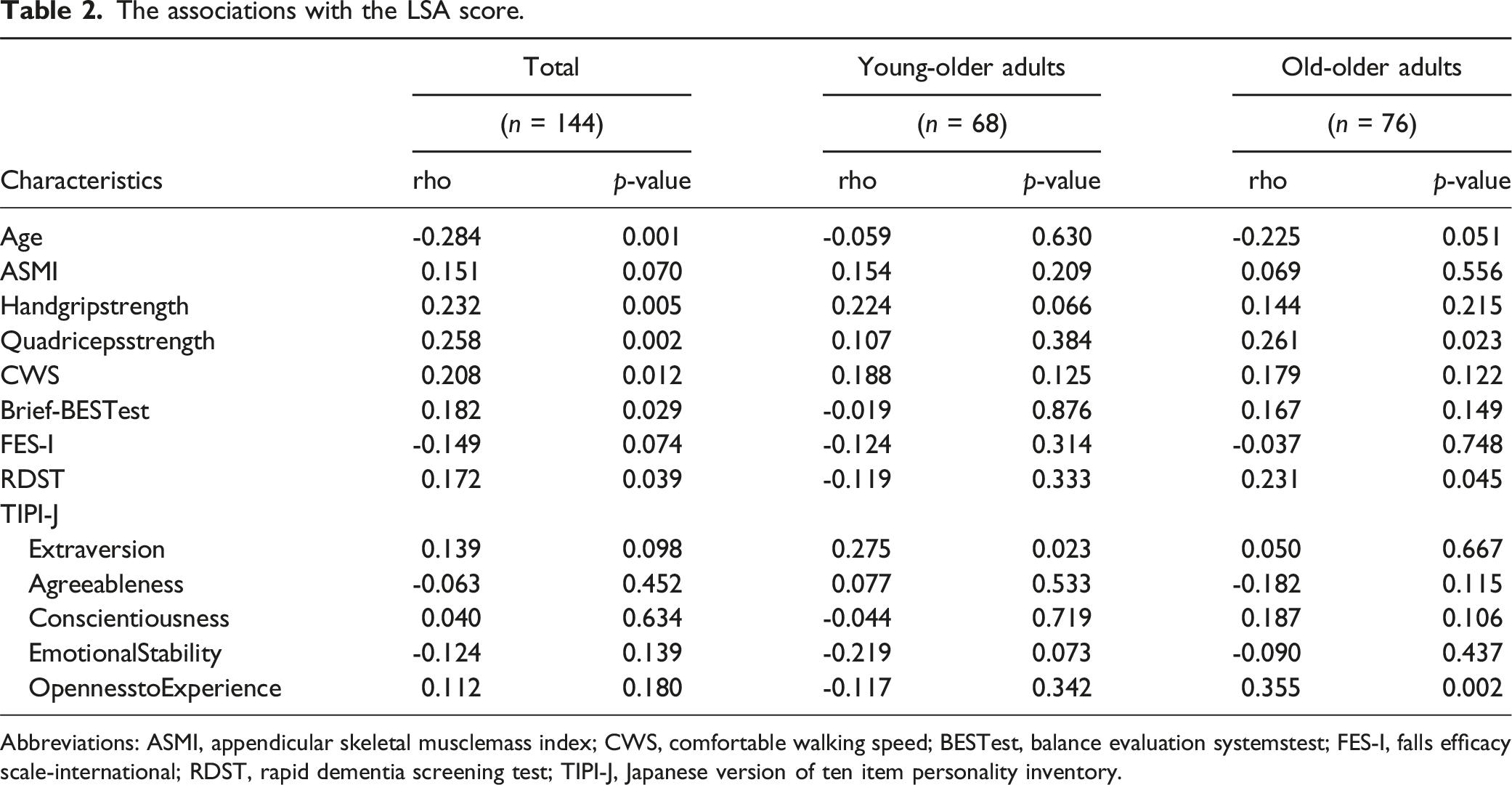
Abbreviations: ASMI, appendicular skeletal musclemass index; CWS, comfortable walking speed; BESTest, balance evaluation systemstest; FES-I, falls efficacy scale-international; RDST, rapid dementia screening test; TIPI-J, Japanese version of ten item personality inventory.
Among young-older adults, LSA did not significantly correlate with other measurements (Table 2). The median was 110.0 for males and females, with no significant difference (p = .940). The median was 110.0 for those without multimorbidity and 102.0 for those with multimorbidity, with no significant difference (p = .56). Regarding LSA based on the history of falls, the median was 116.0 for those without falls and 100.0 for those with falls, and there was a significant difference (p = .047).
Among older adults, The LSA score was significantly correlated with quadriceps strength (rs = 0.261, p = .023), RDST (rs = 0.231, p = .045), and openness to experience of the TIPI-J (rs = 0.355, p = .002) (Table 2). The median was 101.0 in men and 93.5 for women, without significant difference (p = .210). The median was 100.0 for those with and those without multimorbidity, without significant difference (p = .86). Regarding the LSA based on a history of falls, the median was 96.0 for those without falls and 102.0 for those with falls, with no significant difference (p = .366).
Factors associated with the LSA score according to the generalized linear model among older adults (n = 144).
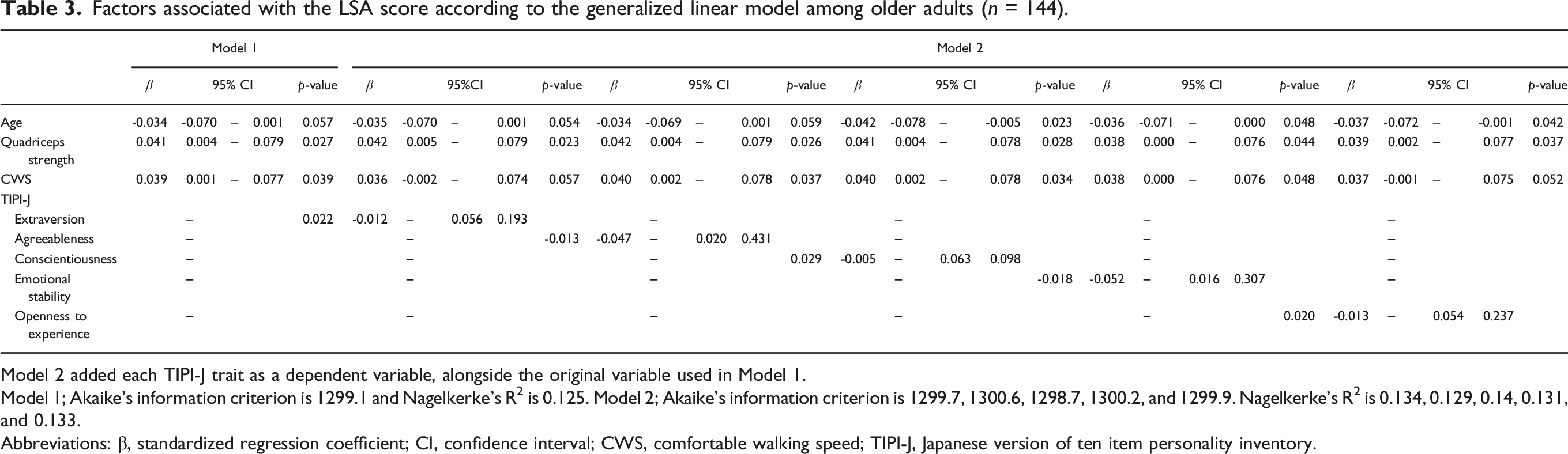
Model 2 added each TIPI-J trait as a dependent variable, alongside the original variable used in Model 1.
Model 1; Akaike’s information criterion is 1299.1 and Nagelkerke’s R2 is 0.125. Model 2; Akaike’s information criterion is 1299.7, 1300.6, 1298.7, 1300.2, and 1299.9. Nagelkerke’s R2 is 0.134, 0.129, 0.14, 0.131, and 0.133.
Abbreviations: β, standardized regression coefficient; CI, confidence interval; CWS, comfortable walking speed; TIPI-J, Japanese version of ten item personality inventory.
Factors associated with the LSA score according to the generalized linear model among young-older adults aged 60-74 years (n = 68).
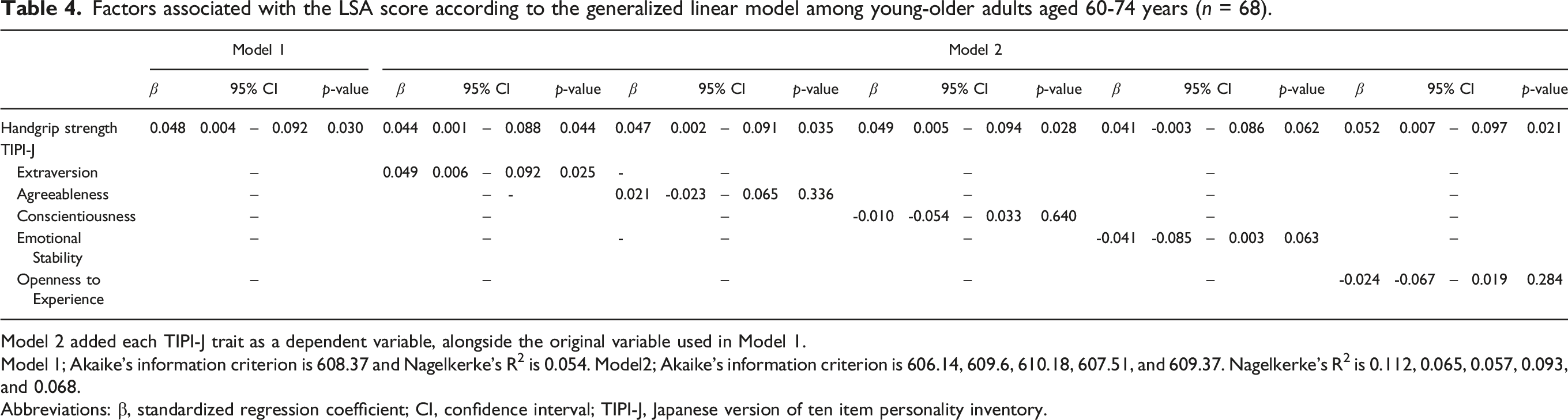
Model 2 added each TIPI-J trait as a dependent variable, alongside the original variable used in Model 1.
Model 1; Akaike's information criterion is 608.37 and Nagelkerke's R2 is 0.054. Model2; Akaike's information criterion is 606.14, 609.6, 610.18, 607.51, and 609.37. Nagelkerke's R2 is 0.112, 0.065, 0.057, 0.093, and 0.068.
Abbreviations: β, standardized regression coefficient; CI, confidence interval; TIPI-J, Japanese version of ten item personality inventory.
Factors associated with the LSA score according to the generalized linear model among old-older adults ≥ 75 years (n = 76).
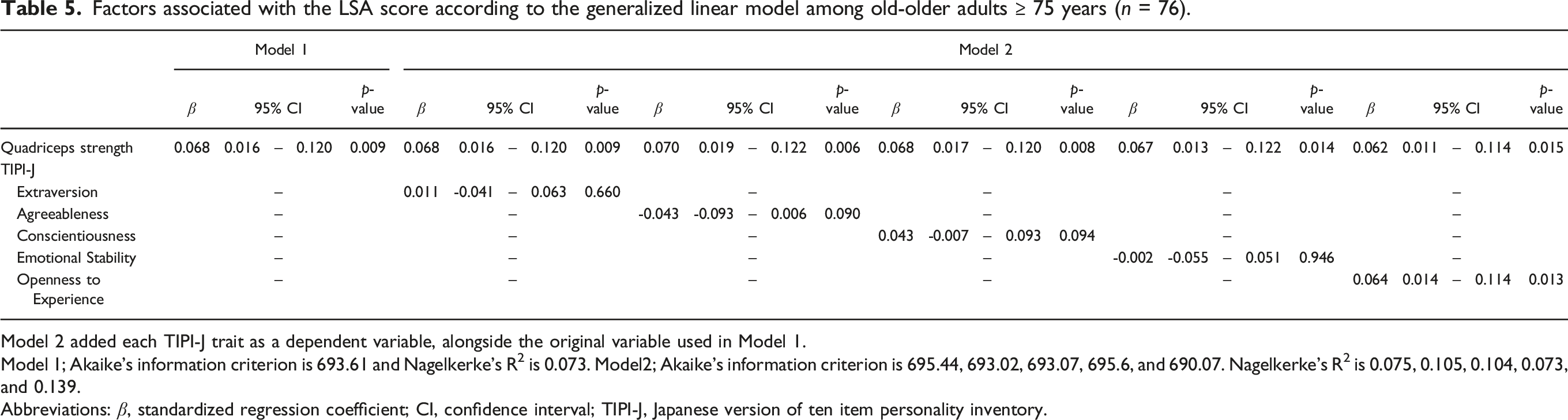
Model 2 added each TIPI-J trait as a dependent variable, alongside the original variable used in Model 1.
Model 1; Akaike's information criterion is 693.61 and Nagelkerke's R2 is 0.073. Model2; Akaike's information criterion is 695.44, 693.02, 693.07, 695.6, and 690.07. Nagelkerke's R2 is 0.075, 0.105, 0.104, 0.073, and 0.139.
Abbreviations: β, standardized regression coefficient; CI, confidence interval; TIPI-J, Japanese version of ten item personality inventory.
As a sensitivity analysis for model validation, in all older adult data, handgrip strength emerged as a significant variable in both Models 1 and 2. Additionally, within the TIPI-J, a significant association was observed with extraversion (β = 0.034, p = .046, Table S1). Among adults <75 years, a significant association was found with extraversion (β = 0.053, p = .016, Table S2). In older adults, a significant association was found between openness and experience (β = 0.064, p = .013, Table S3).
Discussion
This study assessed LSM using the LSA to explore whether personality traits were related to LSM beyond the previously validated physical and cognitive functions associated with LSM. For the study’s participants, univariate analysis showed significant correlations with many measurements, but in the GLM, quadriceps strength and walking speed were significantly associated with LSM. For those aged 60–74 years, extraverted personality traits and grip strength, and for those aged ≥75 years, openness to experience and quadriceps strength, were significantly related to LSM. In the sensitivity analysis, the personality traits associated with LSM were consistent, supporting the robustness of the present results.
The short physical performance battery, which includes an assessment of walking speed and handgrip strength, has been reported to be significantly associated with LSM (Fristedt et al., 2022). Gait function, including gait speed, made a more substantial contribution than age and sex (Suri et al., 2021). Furthermore, among the comprehensive assessments, including psychosocial and cognitive determinants as well as pain, fatigue, driving status, nutrition, body mass index, smoking status, and vision, walking speed, were identified as being most strongly associated with LSM (Kuspinar et al., 2020). Similarly, the LSM of community-dwelling older adults was reported to be associated with walking speed, as well as with pain and cognitive function (Shinohara et al., 2024). The correlation between lower limb muscle strength and walking speed is not difficult to predict, and this holds true for both men and women (Inoue et al., 2017). In longitudinal observations, quadriceps strength contributes to postoperative LSM expansion in patients undergoing total knee arthroplasty (Tobinaga et al., 2019). In this study, the association of walking speed, quadriceps strength, and grip strength with LSM supports previous findings. When dividing the older adults into those aged ≤74 and ≥75 years, grip strength was associated with the former, while quadriceps strength was related to the latter. The discernible decline in lower limb strength and individual variation, especially in individuals aged ≥75, might contribute to such differences.
This study demonstrated the correlation between the LSM and personality traits. In the young-older group, extraversion showed a significant association, whereas in the old-older group, openness to experience was significant. The higher the extraversion, the faster the walking speed, and the less likely an individual is to experience a decline in gait speed (Stephan et al., 2018). Moreover, expanded mobility has also been reported (Barnes et al., 2007; Ndubuaku et al., 2023), and this study’s results based on a Japanese population support that notion. While there are few reports regarding openness, existing reports show no association between openness and walking speed (Tolea et al., 2012). High openness indicates not being constrained by existing values and having high intellectual curiosity, which correlates with a broader LSM. In both cases, the evaluation of beta and 95% confidence intervals were comparable to grip strength and quadriceps strength, indicating that personality has an impact equivalent to that of physical function. As has been emphasized regarding the importance of psychological conditions and biographical factors (Shimada et al., 2010), assessments and interventions in the mobility of older adults should encompass physical and cognitive conditions and personality traits. Intrapersonal risk factors that increase the risk of mobility limitation include advanced age, female sex, low socioeconomic status, comorbidities, lifestyle factors, physiological factors, and lack of motivation (including dependent personality and decreased self-efficacy) (Yeom et al., 2008). The barriers and facilitators to physical activity participation involve six major themes: social influences, physical limitations, competing priorities, access difficulties, personal benefits of physical activity, and motivation and beliefs (apathy, irrelevance, inefficacy, and maintaining habits) (Franco et al., 2015). While not explicitly mentioned here, personality is believed to be associated with multiple themes, particularly those directly linked to motivation and beliefs. Cognitive decline, diagnosis of late-life depression, and its progression in older adults are linked to personality traits (Sadeq & Molinari, 2018).
The personality traits examined in this study, unlike physical functions that can be altered through interventions, are not easily changeable. We believe that they should be understood as individual attributes rather than intervention targets, serving as valuable considerations for designing interventions or support strategies. In clinical settings, formal personality assessments are not commonly incorporated into clients’ treatment plans, despite the potential impact of personality traits on treatment effectiveness and outcomes (Sadeq & Molinari, 2018). Interventions and engagement considering the personality of the individuals are desirable for maintaining and expanding LSM in community-dwelling older adults. LSM is associated with multiple factors, and future research should investigate personality as a factor, in addition to others.
Limitations
This study had limitations. First, while the overall analysis aimed for the target sample size, the age-specific analysis fell short. Verifying that data collection is sufficient is essential to ensure an adequate sample size for conducting subgroup analyses. However, the number of variables in the final model obtained was within a reasonable range. Second, although variables related to physical function, cognitive function, and psychological aspects were included in the investigation, not all LSM assessments including those related to environmental and financial aspects were included. Third, a short-form personality assessment, the TIPI-J, was used to ensure feasibility. However, for a more thorough analysis of personality correlations, a detailed personality assessment may be necessary, even if it requires more time for evaluation. Fourth, the analysis was limited to a cross-sectional examination using LSM. In this study, although a significant association with personality traits was identified, a longitudinal analysis is anticipated to explore how the degree of personality traits with significant associations relates to changes in LSM over time.
Conclusions
This study demonstrated that both physical function and personality traits are associated with LSM in community-dwelling older adults. Extraversion in young-older adults and openness to experience in old-older adults were significantly associated. These findings indicate that the personality traits associated with LSM vary with age. While previous research has reported various aspects of LSM, this study highlights personality as a psychosocial factor associated with LSM. Therefore, future LSM studies should include assessments and analyses that incorporate personality traits.
Supplemental Material
Supplemental Material - The Life-Space Mobility of Community-Dwelling Older Adults is Associated With Personality Traits
Supplemental Material for The Life-Space Mobility of Community-Dwelling Older Adults is Associated With Personality Traits by Tomoyuki Shinohara, Rina Yamauchi, Yuta Yabana, Ayumi Maruyama, and Shota Saito in Journal of Applied Gerontology.
Supplemental Material
Supplemental Material - The Life-Space Mobility of Community-Dwelling Older Adults is Associated With Personality Traits
Supplemental Material for The Life-Space Mobility of Community-Dwelling Older Adults is Associated With Personality Traits by Tomoyuki Shinohara, Rina Yamauchi, Yuta Yabana, Ayumi Maruyama, and Shota Saito in Journal of Applied Gerontology.
Supplemental Material
Supplemental Material - The Life-Space Mobility of Community-Dwelling Older Adults is Associated With Personality Traits
Supplemental Material for The Life-Space Mobility of Community-Dwelling Older Adults is Associated With Personality Traits by Tomoyuki Shinohara, Rina Yamauchi, Yuta Yabana, Ayumi Maruyama, and Shota Saito in Journal of Applied Gerontology.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to Shizuko Nakajima, Masami Ashikaga, Noriko Takizawa, Kazuhiro Suto, Yoshiko Yamada, Hiroshi Akiyama, Jinko Aoyagi, Akemi Yoshii, and Katsumi Goto.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (Grant Number JP22K11154).
IRB Approval
This study was approved by the Research Ethics Committee of the Takasaki University of Health and Welfare (Approval No. 2240).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.