
Abstract
Person-centeredness is instrumental to quality dementia care but is inconsistently defined and descriptions often reflect higher-income and Eurocentric perspectives. This paper addressed these limitations by surveying 39 member associations of Alzheimer’s Disease International regarding the global quality of dementia care, challenges and successes in providing person-centered dementia care, and definitions of person-centered dementia care in their countries. The economically and geographically diverse respondents described a common lack of both quality and person-centered dementia care and identified associated barriers. Results suggest that identifying shared perspectives is necessary to further the person-centeredness of dementia care, and should reflect five core tenets: individualize care, support and acknowledge caregivers, empower the individual, cultivate respectful relationships, and address dimensions of wellness.
• Utilizes a questionnaire to gain empirical knowledge surrounding the current state of quality dementia care and person-centered dementia care across the world. • Identifies fundamental tenets of person-centered dementia care representative of geographically and economically diverse countries.
• Identifies global barriers to person-centered dementia care for further study. • Presents fundamental global tenets of person-centered dementia care to be used by practitioners, researchers, and policy advocates to speak with a common voice. • Presents recommendations for practitioners, researchers, and policy advocates on how to embody global tenets of person-centered dementia care.What this paper adds
Applications of study findings
Introduction and Background
An estimated 55 million individuals live with dementia worldwide, a number expected to more than double by 2050 (Alzheimer’s Disease International, n.d.). The 2022 World Alzheimer Report developed by Alzheimer’s Disease International (ADI), a federation of 105 geographically and economically diverse Alzheimer and dementia associations, presented key recommendations to meet the care needs of this population, a fundamental component being universal access to person-centered care (PCC) (Gauthier et al., 2022). These recommendations align with the 2018 Dementia Care Practice Recommendations put forward by the US Alzheimer’s Association naming PCC the underlying philosophy behind quality dementia care (Fazio et al., 2018).
Modern conceptualizations of PCC originate from Carl Rogers’ person-centered therapy where the therapist takes a non-directive role, recognizing the client as ultimately responsible for driving the therapeutic process (Rogers, 1946). Throughout the 20th century person-centeredness became increasingly called for in healthcare; in the 1990s, Thomas Kitwood focused PCC on the relationship between caregivers and persons living with dementia. Kitwood’s ideal relationship focuses not on completing care tasks, but on meeting an individual’s needs through love, comfort, attachment, inclusion, and occupation; in so doing, the personhood, or retained identity of the person, is upheld (Kitwood, 1997). Brooker’s subsequent “VIPS” system defines four components of person-centered dementia care: Valuing the individual, Individualizing care based on the unique needs of the individual, understanding the Perspective of the person living with dementia, and maintaining a positive Social environment (Brooker, 2003). Today PCC is globally recognized as the basis of quality dementia care.
Examples of Literature Based Definitions of Person-Centered Care (PCC).
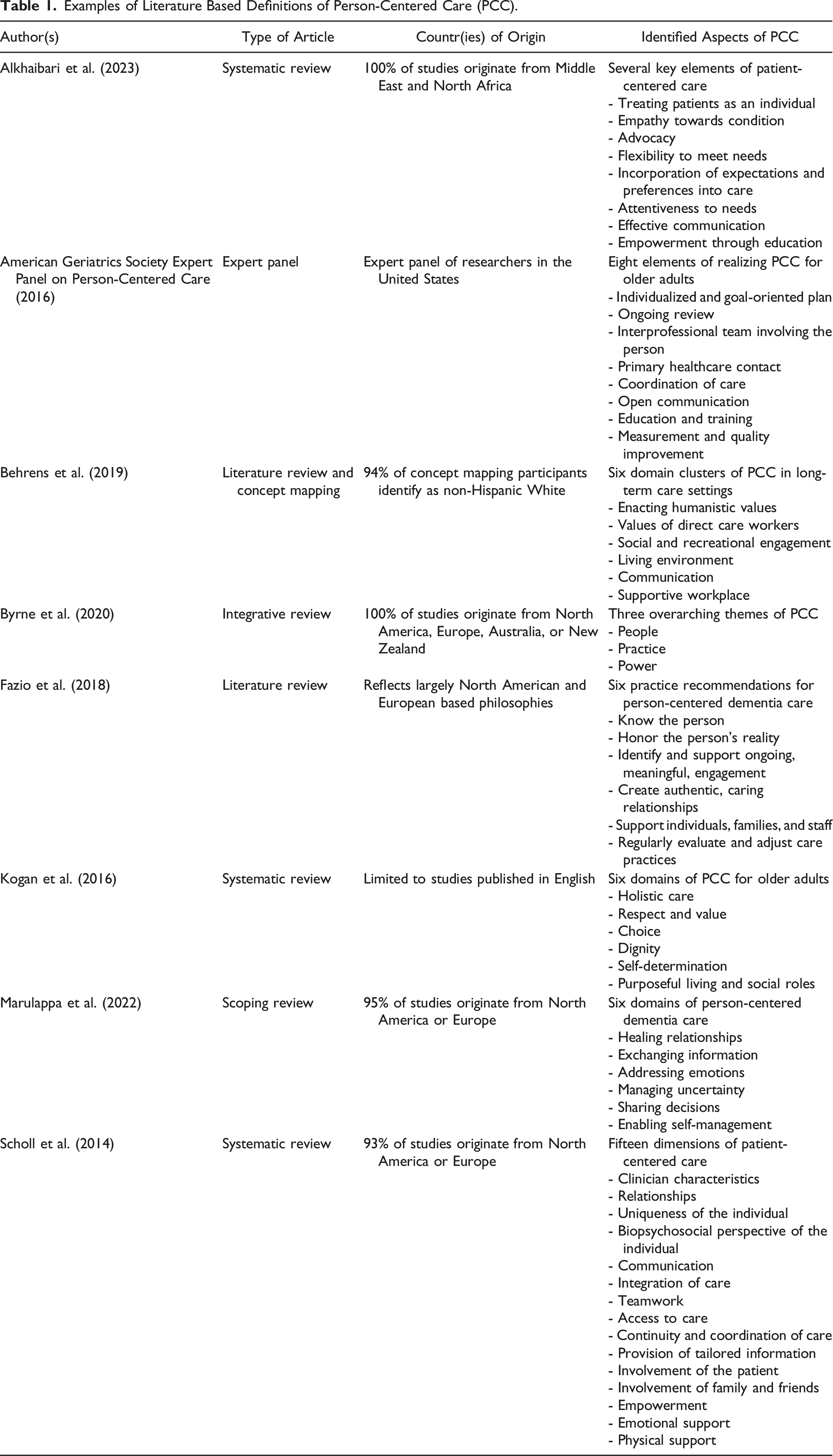
Common among the definitions of PCC captured in Table 1 are: individualization of care through the elicitation of values and preferences; the creation of respectful and empowering relationships between the individual, families, and providers; maintaining a biopsychosocial perspective of the individual; and supporting caregivers. PCC for those with dementia often involves meaningfully engaging individuals to optimize their independence and capabilities, and providing a sense of stability through routines and continuity (Fazio et al., 2018; Marulappa et al., 2022). Although commonalities exist, the variability surrounding what constitutes PCC leads to gaps between the theory of person-centeredness and its operationalization in healthcare and community based settings (Byrne et al., 2020; Gauthier et al., 2022), disparate terminology surrounding person-centered practices (The American Geriatrics Society Expert Panel on Person-Centered Care, 2016), inadequate standards of care (Kogan et al., 2016), difficulties in measurement (Scholl et al., 2014), and a heterogeneous landscape of dementia care interventions embodying varying degrees of person-centeredness (Mohr et al., 2021).
Attempts to conceptualize person-centered dementia care are limited by a lack of geographic and economic diversity in the literature. The reviews in Table 1 consist almost entirely of research from higher-income countries as designated by the World Bank, located in North America, Europe, and Australia/New Zealand. Although recent efforts have bolstered scholarship surrounding PCC in non-Eurocentric and lower- and middle-income countries, these studies often represent a small sample and are not specific to persons with dementia (Alkhaibari et al., 2023; Corazzini et al., 2019; Kim et al., 2021; Wang & Bowers, 2023). As a result, current definitions of person-centered dementia care lack a global and dementia sensitive perspective. To be sure, dementia care is and should be sensitive to cultural differences, and so differ between countries, but certain tenets may be common regardless of the country. Given that 60% of those living with dementia reside in lower- and middle-income countries (Wimo et al., 2018), the need to better understand common tenets of how person-centered dementia care is conceptualized in these nations is apparent.
Additionally, PCC for older adults with or without dementia is typically described and studied in clinical and long-term care settings (Behrens et al., 2019; Mohr et al., 2021), resulting in conceptualizations that focus primarily on relationships between providers and individuals (a recent exception being Marulappa et al. [2022]). With the majority of persons with dementia residing in the community—69% of those in higher-income countries and 96% of those in lower-income countries (Wimo et al., 2018)—the need to better understand PCC for those living in the community is evident.
As part of a broader effort to reconsider the concept of person-centeredness, the National Institute on Aging-funded Consortium known as Leveraging an Interdisciplinary Consortium to Improve Care and Outcomes for Persons Living with Alzheimer’s and Dementia (LINC-AD) sought to gain a better understanding of the tenets of person-centered dementia care on a global scale, and to learn the utility of developing a global definition of person-centered dementia care. This special article describes the results of an electronic questionnaire (Appendix A) distributed via SurveyMonkey to all 105 ADI member associations alongside 20 members of the ADI membership development program. ADI membership is limited to one per country and was chosen for this effort given ADI’s global role in providing emotional and practical support to people with dementia and their caregivers. The questionnaire, available only in English, consisted of 16 questions surrounding quality dementia care; key components, challenges, and successes of person-centered dementia care; and PCC resources. The questionnaire was developed by LINC-AD leadership and reviewed by ADI staff before being shared via email to all 105 ADI organizations. Organizations were given discretion regarding how to complete the questionnaire, resulting in 11 organizations having multiple respondents/surveys completed. Ultimately 59 individuals representing 39 geographically and economically diverse countries (Figure 1) provided responses, with respondents from 27 countries responding to the majority of the questionnaire. Exploratory thematic analysis of qualitative questions was completed and reviewed by the authorship team, and descriptive statistics (percentage and response frequency) were calculated for quantitative questions. The key points resulting from these responses highlight the varying perspectives, definitions, and status quo of dementia care throughout the world and identify five core components of global person-centered dementia care which are discussed in the context of the literature, followed by recommendations for research, policy, and practice. Countries represented by survey respondents and associated world bank income group designations. Note. Created with mapchart.net (MapChart, 2023).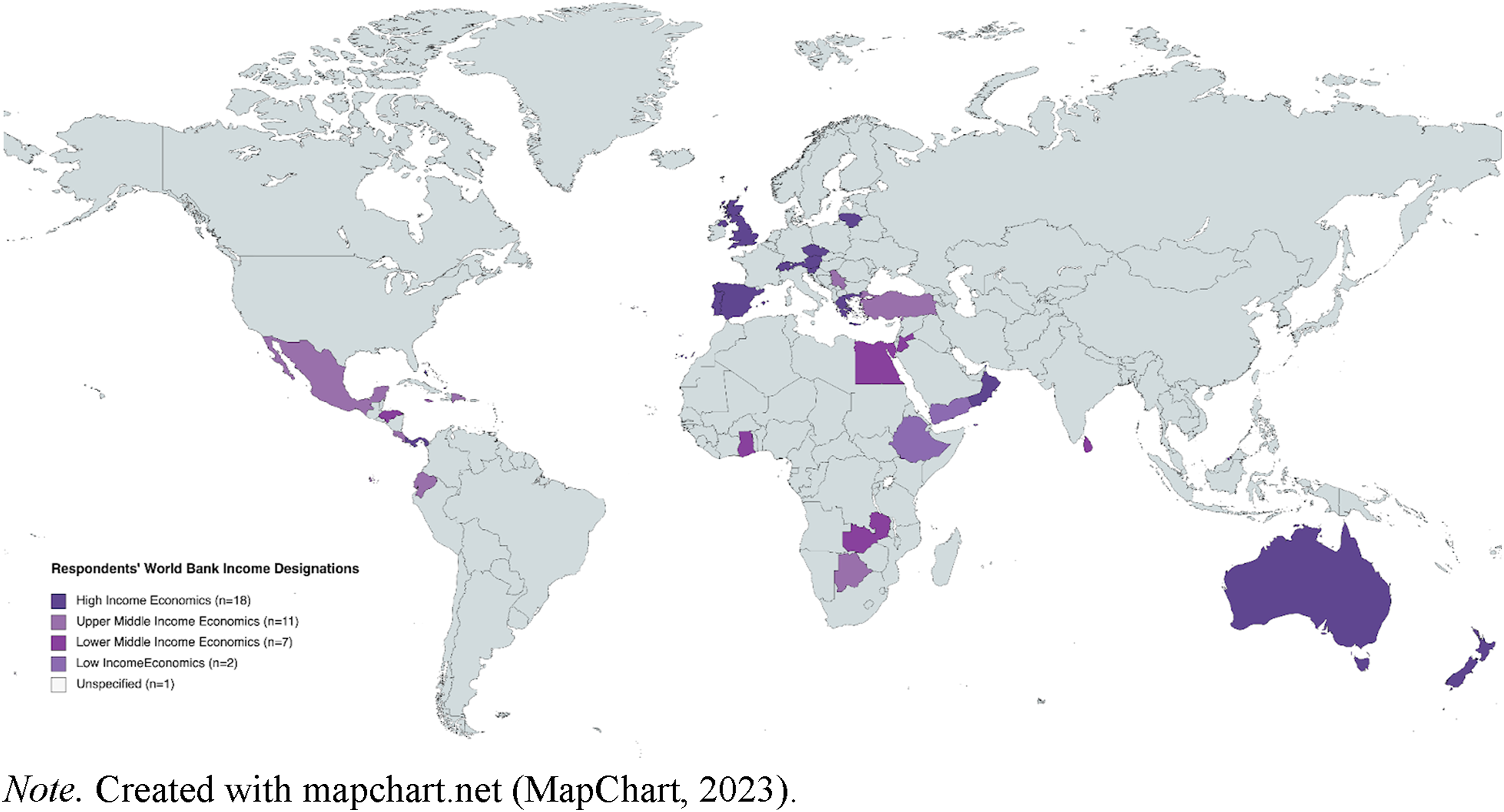
Key Points
Global Variations in Dementia Care for Individuals with Dementia
Respondents from all 39 countries answered the question asking what quality care for persons living with dementia looks like in their country, providing a range of responses. The majority of respondents, representing 24 countries, reported an immediate need to improve existing care systems for those with dementia, with one noting that “at its best [dementia care] is probably world leading, but there are low rates of diagnosis that hinder access to support and a ‘postcode lottery’ of what is available.” Respondents from 15 countries (34% of higher-income economies represented in this survey and 44% of lower-income economies) reported having little to no quality dementia care. Said one respondent “it [quality dementia care] is more in theory than in practice. Patients and their carers are not effectively and respectfully considered part of the care team: there are no clear guidelines of their involvement in the care process.” Ten respondents to this question explicitly described quality dementia care as embodying elements of person-centered care.
Respondents described numerous factors contributing to a lack of consistent high quality dementia care. There exists little public awareness surrounding dementia, and a “stigma of dementia, and belief that people affected can’t tell what they want or need.” Gaps in knowledge were described as leading to professional and familial caregivers experiencing challenges with communication, and difficulties navigating behaviors that challenge. In many countries family members provide the majority of dementia care, but often have “little to no health care training and [a] generally poor understanding of dementia.” Additionally, a general “lack of sufficient personnel and resources” was described as hindering quality dementia care and contributing to a lack of person-centered dementia care in both private and public services.
Regarding person-centered dementia care, respondents described difficulties “changing the culture of an organization from one that is task oriented to one that is person-centered/oriented” and the general misunderstanding of the term “person-centered” causing it to “used often to describe any care or support given to the person.” Difficulties quantifying the nebulous term “person-centered” also exist, with respondents from eight countries reporting being aware of tools used to measure PCC, and 14 explicitly stating that they were unaware of such tools. The challenge of implementing and measuring person-centered dementia care in lower-income countries is made difficult by inadequate scholarship, said one respondent “[person-centered care] is not well studied in low-income countries such as [ours] and little or not at all implemented.”
Despite global difficulties accessing person-centered dementia care, respondents described ongoing efforts to enact PCC for individuals with dementia in their country, including training caregivers to defocus tasks, and prioritizing “the needs and rights of a person living with dementia.” Others described advocating for increased social and health policies, privately developing services not provided by the public sector, and disseminating education to “raise the level of public awareness” surrounding dementia.
Extant literature mirrors barriers identified by respondents, with Marulappa and colleagues previously identifying several organizational and individual barriers to person-centered dementia care including human and material resource constraints, negative perceptions of dementia, and variations in knowledge of person-centered practices (2022). Other studies have pointed to the task-oriented environment of healthcare settings (Byrne et al., 2020), and measurements of care that focus on deficits and avoiding regulatory penalties instead of prioritizing person-centeredness (Corazzini et al., 2019) as contributing to difficulties in realizing PCC.
The Global Need for a Definition of Person-Centered Dementia Care
To determine the next best step to improve person-centered dementia care across the world respondents were asked to report on the relative importance of five components of PCC: having an agreed-upon definition, evidence that PCC improves outcomes, staff training and education, quality improvement resources, and technology. These components were chosen during a 2023 think-tank composed of LINC-AD Research Steering Committee members and other experts in person-centeredness as actionable steps representing person-centeredness. Respondents from 22 countries responded to this question; a majority (n = 12; 55%) reported having an agreed-upon definition of person-centered dementia care was most important to bolster the person-centeredness of dementia care, with evidence that PCC improves outcomes being chosen as second most important by respondents from eight countries (36%).
In a separate question asking if a universal definition of person-centered dementia care would be helpful to their organization, respondents from 22 countries (92% of those responding to this question [n = 24]) stated “yes”; many described a universal definition as helpful to resolve the previously described barriers to person-centered dementia care. One respondent noted that a universal definition would “help ensure consistent understanding of the terminology and support the argument for ensuring services and care and support were person-centered,” others stated that it could increase their organizations’ abilities to advocate with local governments for resources noting that “as combatants of the same disease it is important to speak with one voice and ‘language.’” Respondents identified a need to create standards for what constituted person-centered dementia care, stating that by “not having a definition [it] allows individuals to interpret it through their own lens”; additionally a universal definition could facilitate established and nascent organizations in educating their members and providing clear recommendations for “caregiver[s] in caring for a loved one who may exhibit challenges.”
The creation of a global definition of person-centered dementia care was endorsed by many respondents, however one stated that because care “must be adapted to the social and cultural realities of each country or region…[a universal definition] could be useful only for didactic purposes, although not so much for practical purposes.” In their paper Mitchell and colleagues vigorously agree with this argument, stating that “definitional exercises that are undertaken with an insistence on their finality and universal applicability create obstacles for implementing and understanding person-centered care” (pg. 13, 2022), arguing that maintaining a heterogeneity of frameworks allows for PCC to be responsive to differing contexts, groups, and ethical perspectives.
Foundational Global Tenets of Person-Centered Dementia Care
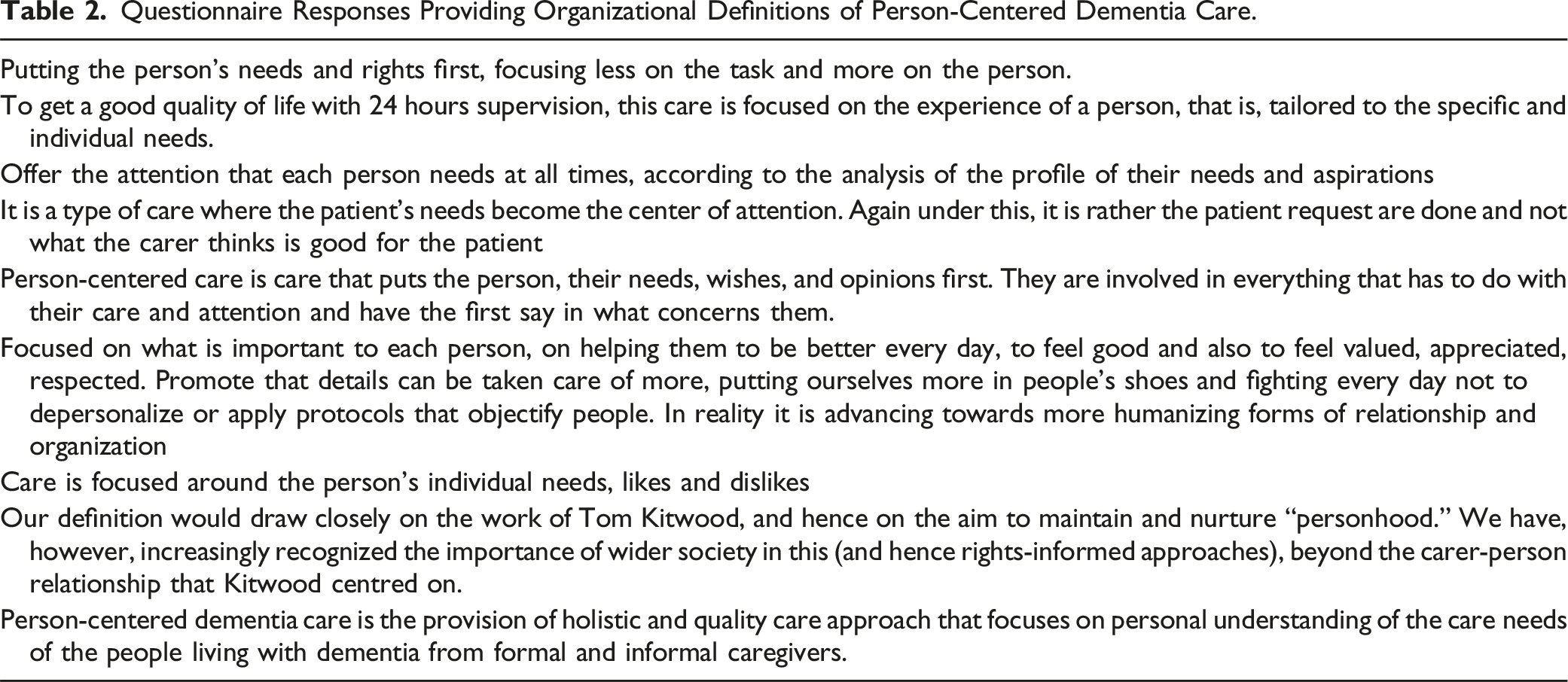
Questionnaire Responses Providing Organizational Definitions of Person-Centered Dementia Care.
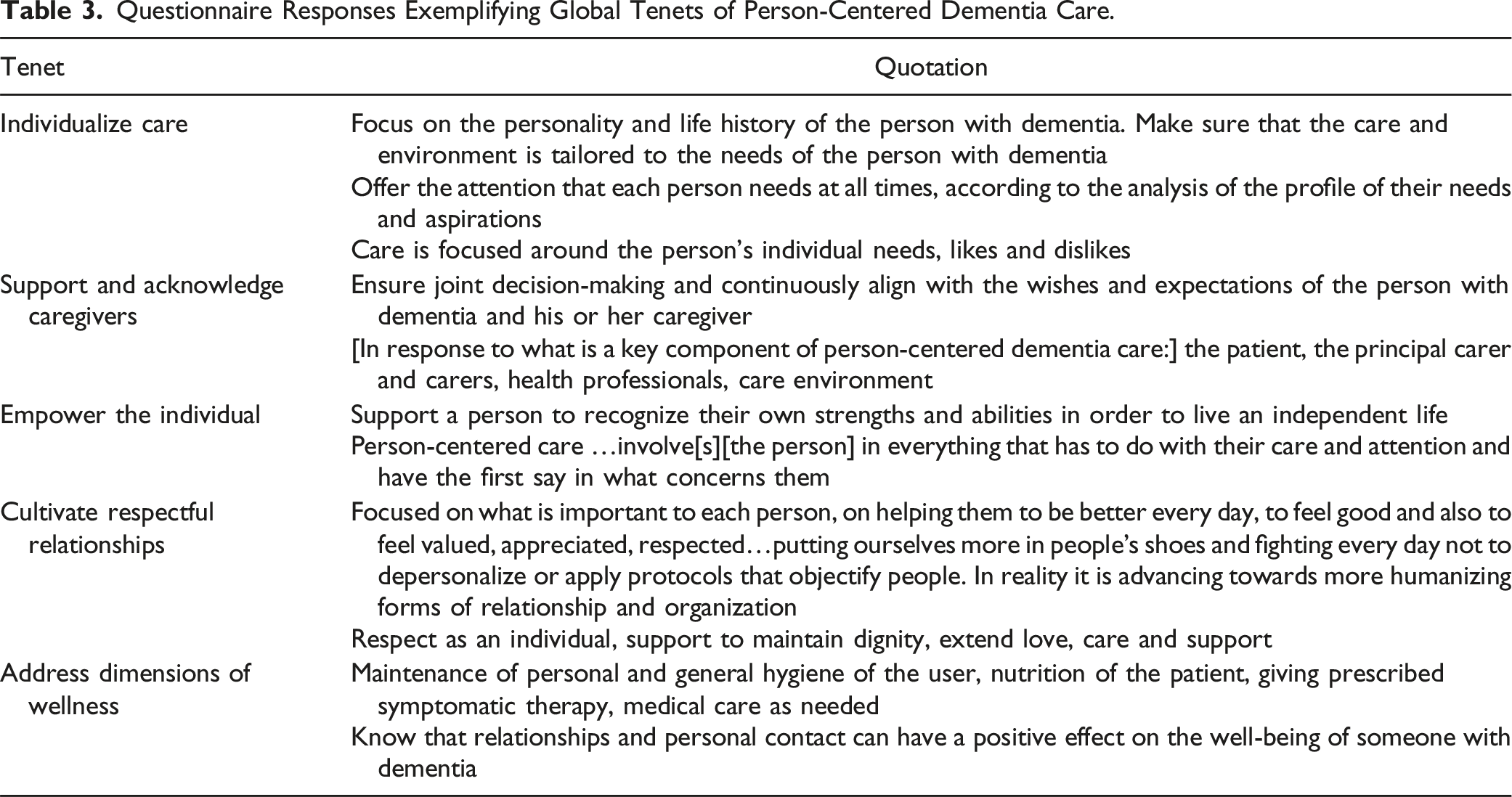
Questionnaire Responses Exemplifying Global Tenets of Person-Centered Dementia Care.
Individualize Care
Respondents from a majority of countries (n = 21) described intentional individualization of care as necessary for person-centered dementia care. This individualization puts “the person, their needs, wishes and opinions first” and “focus[es] on the personality and life history of the person with dementia, mak[ing] sure that the care and environment is tailored to the needs of the person with dementia.” It was noted that to achieve true individualization of care, person-centered dementia care must be based on an “analysis of the profile of their needs and aspirations.” One respondent stated that individualization of care occurs when “the patient requests are done and not what the carer thinks is good for the patient,” emphasizing that this individualization may result in outcomes undesirable to caregivers.
Individualizing care based on the unique needs of the individual with dementia is well established as a key component of person-centered dementia care (Brooker, 2003). This individualization of care is achieved in part when every interaction with the person is informed by knowledge of their current and historical values, interests, and capabilities (Fazio et al., 2018), and recognizes that no singular approach to care can capture the diverse cultural needs of every individual (Islam, 2024). Knowledge of the individual must move beyond superficial biographical information, and be gained through culturally sensitive meaningful exchanges, and an ongoing and intentional process of discovery (Zimmerman et al., under review). While some respondents described individualization of care as a continuous alignment with the wishes of the individual, other descriptions remained superficial focusing on needs and likes without discussion of an ongoing relationship.
Support and Acknowledge Caregivers
In addition to individualizing care, respondents from a majority of countries (n = 22) described the importance of supporting and recognizing informal and formal caregivers in providing person-centered dementia care. One respondent noted that person-centered dementia care must “continuously align with the wishes and expectations of the person with dementia and his or her caregiver” with others noting the need to respectfully and intentionally involve familial caregivers in formal care settings. Within healthcare settings respondents additionally noted the value of specialized interdisciplinary teams in realizing person-centered dementia care.
Respondents from several organizations described providing caregiver support, often in the form of education and training, as necessary for person-centered dementia care. Some reported that their organization’s primary role was to “work [with] caregivers and family of the person” with others being “tasked with training carers [on] PCC.” Some described educating caregivers using established conceptualizations of care, naming Dawn Brooker’s VIP system, Kitwood’s conceptualization of person-centeredness, and Naomi Fell’s Validation Method. Despite this focus on caregiver education and support, respondents from only 12 organizations reported maintaining educational materials on person-centered dementia care, with respondents from 21 organizations reporting that they did not.
Although partnership between formal and informal caregivers in the care planning process is an established element of person-centered dementia care (Marulappa et al., 2022), some have argued that the prioritization of the individual within person-centered dementia care risks minimizing the critical role played by family caregivers (Hao & Ruggiano, 2020). Others have noted that this prioritization embodies Eurocentric concepts of individualism that do not globally resonate (Wang & Bowers, 2023). Family-centered care, with its focus on forming meaningful partnerships with the family of those who live with dementia, has been proposed as a complementary approach to person-centered care (Hao & Ruggiano, 2020), and in collectivistic cultures where healthcare decisions are traditionally made by the family (Alkhaibari et al., 2023), may prove highly effective.
Empower the Individual
Respondents from 16 countries defined person-centeredness as intentionally honoring the agency and self-determination of individuals with dementia, “support[ing] a person to recognize their own strengths and abilities in order to live an independent life.” This support included modifying the format of information to increase its accessibility, modifying the environment to suit the needs of those with dementia, and extending “love, care and support to the extent necessary and/or expected by the client to carry out activities” Respondents also described empowerment in terms of ensuring that the person with dementia remains “involved in everything that has to do with their [own] care” and that their choices are respected and valued. However, others described challenges to prioritizing individual choices, such as behaviors that challenge or individuals refusing basic hygiene.
Empowerment for those living with dementia is described by Van Corven and colleagues (2021) as consisting of four domains: personal identity, choice and control, usefulness and being needed, and retaining worth; with fulfillment in these domains determined by the nature of interactions between the person with dementia and their social and physical environment. Fazio and colleagues (2018) similarly propose that person-centered dementia care must maintain an empowering perspective where every interaction is treated as an opportunity to support the individual through purposeful engagement, providing meaningful opportunities for choice and success. As discussed by respondents, opportunities for choice and success are best realized when all aspects of care, including the environment, provision of information, and available activities, are adapted to honor the individual’s strengths and maximize their involvement.
Empowering the individual can be challenging when balancing an individual’s preferences with those of caregivers, or when actions potentially compromise health and safety. Empowerment is particularly complex in cultures where the power of decision-making traditionally belongs to family members and providers, a potential barrier to PCC (Alkhaibari et al., 2023). Although further study on the applicability of empowerment in these contexts is needed, adopting a stance of moral diversity and incorporating principles of relational autonomy into person-centered dementia care offers a promising path forward (Islam, 2024).
Cultivate Respectful Relationships
Alongside recognizing the agency of persons with dementia, respondents from 15 countries defined person-centered dementia care as a way of being that respects the inherent value of the individual. Embodying respectful relationships involves preserving the rights of individuals with dementia, affording them “respect as an individual, support to maintain dignity, [and] extend[ing] love, care and support,” and “helping them to be better every day, to feel good and also to feel valued, appreciated, respected.” By honoring the inherent worth of individuals with dementia, PCC is the antithesis of protocols that depersonalize and objectify individuals, it allows for “putting ourselves more in people’s shoes…[and] is advancing towards more humanizing forms of relationship and organization.”
Cultivating respectful relationships where the inherent worth of those living with dementia and those caring for them is valued is part of the first component of Brooker’s VIPS model (2003). These relationships honor the individual’s personhood, a “standing or status that is bestowed upon one human being by others, in the context of relationship and social being…[Implying] recognition, respect, and trust” (Kitwood, p. 8, 1997). Relationships where the person with dementia is treated with respect, compassion, and where their contributions are valued provide a crucial foundation for the maintenance of personhood; conversely relationships based on accomplishing care tasks, are unprofessional in nature, or lack compassion can diminish personhood (Smebye & Kirkevold, 2013). Person-centered dementia care therefore relies on non-task oriented environments (Byrne et al., 2020) which foster authentic, caring, relationships concentrating not on the fulfillment of tasks but on the interaction with the individual (Fazio et al., 2018). In addition, relationships that truly respect the individual embrace cultural differences (Du Toit & Buchanan, 2018), and value and validate the perception of reality held by the person with dementia (Brooker, 2003). In doing so, formal and informal caregivers must make a purposeful effort to respect the lived reality of the person with dementia, and as respondents stated, move towards “humanizing” relationships. Respecting the individual in this way supersedes a mere checklist of actions to take, and moves person-centered dementia care into a truly caring relationship, where respect, compassion, and love are genuinely expressed and felt.
Address Dimensions of Wellness
Amidst the varying definitions of person-centered dementia care respondents from 11 countries described the importance of maintaining various forms of well-being. Physical wellness was described as the “maintenance of personal and general hygiene of the user, nutrition of the patient, giving prescribed symptomatic therapy, [and providing] medical care as needed.” Social well-being was described as “know[ing] that relationships and personal contact can have a positive effect on the well-being of someone with dementia.” Others noted that the emotional and spiritual health of the person with dementia must be considered to provide truly person-centered dementia care.
To unify the diverse dimensions of wellness described by respondents, the model put forth by the International Council on Active Aging offers a valuable framework. This holistic model defines wellness as seven interconnected dimensions: emotional, physical, intellectual, vocational, spiritual, social, and environmental (International Council on Active Aging, n.d.). Wellness in one or more of these dimensions can promote healthier aging and maintain cognition (Strout & Howard, 2012), and recognizing their interconnectedness promotes culturally relevant person-centered dementia care. For instance, providing for physical wellness for individuals from Islamic communities also supports spiritual wellness, as religious practices emphasize diet and hygiene (Alkhaibari et al., 2023). Similarly, in cultures valuing filial piety, culturally sensitive support for familial caregivers can maximize the time older adults live with their children while also ameliorating caregiver strain (Shrestha et al., 2023), tending to the emotional, social, and spiritual wellness of both caregivers and individuals with dementia.
Limitations
It is important to acknowledge a major limitation of this work is its reliance on English as the language for the questionnaire. Given the international sample, this choice may have caused response bias with those countries with less facility with the English language being less likely to respond. Organizations from countries without an established definition of person-centered dementia care may also have been less likely to respond, which may have framed the tenets that were generated. It is also possible that language barriers lead to the variation in responses. Conflicting responses were obtained to a question asking if organizations maintained a definition of person-centered dementia care; eight organizations had at least one respondent report maintaining a definition of person-centered dementia care and another respondent of that same organization stated that they did not have a definition. Although reasons for these contradictory responses are unknown, as is the choice and identity of each respondent, it is possible that organizations may not prioritize upholding a singular definition, or may not prioritize the dissemination of a singular definition where one exists. The intra-organizational discrepancies regarding a definition of person-centered dementia care highlight the fractured and non-standard nature of person-centeredness within dementia care, and the value of this paper.
It is also noted that 39 countries/organizations were represented by this survey. Although respondents represented countries of varying economic designations throughout all six populated continents, it is likely that definitions of person-centered dementia care from countries and regions not represented by this survey exist, limiting the comprehensiveness of the definitions provided. Additionally, 12 countries had no respondents answer the majority of the questions. Due to this missing information, respondents from only 27 countries/organizations (69%) responded to the majority of the questionnaire, further limiting the generalizability of its results.
Finally, this special article presents findings from an initial survey, not a systematic research study. Future research including more countries is needed to corroborate these findings and to deepen the understanding of the global implementation and conceptualization of person-centered dementia care as presented here.
Conclusion and Implications for Practice, Policy, and Research
Through engaging with ADI organizations based in 39 economically and geographically diverse countries this paper provides a snapshot of the status of quality dementia care and person-centered dementia care throughout the world. Respondents from numerous countries representing higher- and lower-income economies reported a significant lack of both quality dementia care and person-centered dementia care, caused in part by limited resources, inadequate government support, a lack of research into person-centeredness in lower-income economies, and a lack of public awareness and sensitivity towards those with dementia. Future advocacy efforts should continue to focus on addressing these barriers to person-centered dementia care. Additionally, research examining the unique socio-political pressures affecting these factors within different countries and regions is needed.
When discussing measurement of PCC, respondents from 14 countries stated they were unaware of such tools, similarly, respondents from a majority of countries stated they do not maintain educational materials regarding person-centered dementia care. These results indicate a global need for the increased availability and proliferation of culturally sensitive and reliable materials for person-centered dementia care and future research. Respondents also noted a need for evidence that PCC improves outcomes for those with dementia and increased scholarship surrounding PCC in lower-income economies. Future research examining PCC approaches in these regions and populations would provide crucial evidence needed for ADI members to advocate with their respective governments for increased support, programs, and funding.
Nearly all respondents named the creation of a universal definition of person-centered dementia care as a necessary next step, however, current definitions are patchwork, and there is apparent intra-organizational misunderstanding regarding their existence. Some respondents described highly nuanced and theory-based definitions, while many did not move beyond the fundamental tenets of person-centeredness that are the individualization of care and supporting caregivers. Recognizing that no singular definition or framework can capture the intricacies of every culture and population, yet honoring the clear need for a unified global approach to what constitutes person-centered dementia care, this paper proposes that there exist five globally shared tenets informing the person-centeredness of interactions with those who live with dementia. These tenets: individualize care, support and acknowledge caregivers, empower the individual, cultivate respectful relationships, and address dimensions of wellness allow for a shared voice amongst those seeking to provide person-centered dementia care, and form a foundation for organization and population specific definitions of person-centered dementia care, promoting advocacy, education, and standards of care. Although future research is needed to examine how these, and potential other, tenets can be adapted and operationalized to meet the specific needs of individual countries and populations, a summary of suggested community practices derived from the responses and existing literature is provided below:
Individualize Care
- Tailor the care environment to the needs of the person with dementia based on knowledge of their personality, cultural background, and life history. - Continuously re-evaluate need by remaining actively engaged with the individual. - Honor the uniqueness of each person and avoid using labels, and depersonalizing or dehumanizing protocols.
Support and Acknowledge Caregivers
- Honor the role of, and support, informal caregivers in providing dementia care. - Provide culturally specific person-centered education and training to informal and formal caregivers. - Involve informal caregivers in professional settings and foster relationships between care providers and family caregivers.
Empower the Individual
- Provide meaningful opportunities for the person with dementia to engage with and make decisions regarding their own care and activities. - Modify the environment and approaches to maximize the strengths of the person with dementia. - Remain attuned to the role of culture and social relationships in decision-making.
Cultivate Respectful Relationships
- Honor the personhood of individuals with dementia through relationships built on compassion, dignity, respect, and warmth. - Prioritize meaningful interaction with the individual over accomplishment of the task at hand. - Embrace cultural differences and respect the lived experience and perspective of the person with dementia and meet them in their reality. - Destigmatize dementia through education.
Address Dimensions of Wellness
- Consider the individual holistically, addressing and providing opportunities to maintain all dimensions of wellness: emotional, physical, intellectual, occupational, spiritual, environmental, and social.
Supplemental Material
Supplemental Material - Global Perspectives on Person-Centered Dementia Care: Results of an International Survey
Supplemental Material for Global Perspectives on Person-Centered Dementia Care: Results of an International Survey by Sam Fazio, Walter Moczygemba, Lauren Stratton, Katie Evans, Wendy Weidner, Sube Banerjee, and Sheryl Zimmerman in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors thank the ADI members for their willing participation in the surveys and Laura Aubert at ADI for distributing and facilitating the surveys to the ADI members
Author Contributions
Sam Fazio, PhD; Lead author
Walter Moczygemba, MSW; Drafted the article, interpretation of data
Lauren Stratton, PhD; Methodology, review of article
Katie Evans; Review and approval of article
Wendy Weidner; Methodology, review of article
Sube Banerjee, MD; Concept, review of article
Sheryl Zimmerman, PhD; Concept, methodology, review and revision of article.
Declaration of Conflicting Interest
Sube Banerjee declares grants from National Institute for Health and Care Research (NIHR), Economic and Social Research Council, Engineering and Physical Science Research Council, Canadian Institute for Health Research, the Alzheimer’s Association, the Alzheimer’s Society, Health Education England, Alzheimer’s Association, Alzheimer’s Society, and Health Education England. He has provided consultancy/educational input to Lundbeck, Axovent and Lilly. He has held the following positions: Trustee Alzheimer’s Society, Non-Executive Director Somerset NHS Foundation Trust, Trustee of the Alzheimer’s Society, Executive Dean at the University of Plymouth, and Pro-Vice Chancellor of the University of Nottingham. No other authors declare conflicts of interest related to the authorship or publication of this paper.
Funding
The authors disclosed receipt of the following financial support for this article: This work was funded by the National Institute on Aging [R24 AG065185].
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.