
Abstract
Background
There has been a rapid growth of technologies designed for people living with dementia and their care-partners. However, despite the proliferation of dementia care technologies, their person-centeredness is not guaranteed, and successful integration into care settings is inconsistent.
Objective
To better understand the relationship between technology and person-centered dementia care.
Methods
This article draws on discussions from two Alzheimer’s Association Dementia Care Provider Roundtable meetings to understand key issues related to technology and person-centered dementia care.
Results
Findings relate primarily to long-term care settings and suggest that technologies hold promise to facilitate engagement and improve care efficiency. However, concerns include the lack of person-centered design, potential for depersonalization of care, and challenges related to implementation. Drawing on provider recommendations, the Modified Hexagon Tool for Designing and Implementing Person-Centered Dementia Care Technologies is introduced as a practical framework for person-centered dementia care technologies in long-term and other care settings.
• Highlights providers’ perspectives on the design and implementation of person-centered dementia care technologies • Adds a dementia specific lens to the growing body of literature surrounding technology and person-centered care
• Identifies topics for further research surrounding the design and implementation of person-centered dementia care technology • Provides a novel framework for the design and implementation of person-centered dementia care technology for older adults in long-term and other healthcare settingsWhat This Paper Adds
Applications of Study Findings
Introduction
With a focus on meeting the unique needs and preferences of the individual through meaningful interpersonal relationships, person-centered care (PCC) is widely recognized as the foundation of holistic healthcare and engagement for the over seven million older adults living with Alzheimer’s disease and related dementias in the United States (Alzheimer’s Association, 2025; Fazio et al., 2018). While definitions vary, PCC is generally described as care where “individuals’ values and preferences are elicited and, once expressed, guide all aspects of their healthcare, supporting their realistic health and life goals” (American Geriatrics Society Expert Panel on Person-Centered Care, 2016, pg. 16). Person-centered dementia care additionally emphasizes preserving the individual’s identity and personhood through caring relationships built on love, comfort, attachment, and inclusion (Kitwood, 1997). Although person-centered dementia care shows promise in meeting both the psychosocial and physical needs of those living with dementia (Fazio et al., 2018; Yee et al., 2021), effectively implementing practices and principles across long-term, home-, and community-based care settings remains challenging (Bayly et al., 2020; Yee et al., 2021; Zimmerman et al., 2026).
To expand access to person-centered care for older adults, many organizations have embraced technological innovations including telemonitoring, self-management systems, and sensor-based programs (Leonardsen et al., 2023). For those living with dementia, applications of machine learning, big data, sensor technologies, and artificial intelligence (AI) may enable timely and accurate diagnoses, assess dementia progression, and assist in maintaining functionality in performing activities of daily living (Astell et al., 2019). Digital technologies have the potential to positively impact well-being through increased individualization of activities (Goodall et al., 2020), and GPS tracking devices can increase a sense of safety for both those wearing the device and their care-partners, and persons with dementia report experiencing improved independence when using trackers (Doyle et al., 2024). Additionally, in long-term care settings, technologies including robotics and multi-media computer programs have been implemented to promote engagement and social connection among residents living with dementia (Neal et al., 2020).
For dementia care-partners, internet-based interventions and educational programs have become widely available resources (Astell et al., 2019), ranging from therapeutic interventions (Contreras et al., 2022) to online peer-support programs (Yin et al., 2024). And although evidence varies, virtual reality (VR) has shown promise in increasing care partner dementia knowledge and the ability to understand the perspective of those living with dementia (Huang et al., 2024).
Despite promising interventions and outcomes, current literature reflects ethical questions and concerns regarding the provision of person-centered dementia care as the intersection between technology and dementia care grows. For example, the collection of personal data (a necessary component of training artificial intelligence systems) may leave individuals vulnerable to breaches of privacy and misuse by third parties, and the effects of cognitive decline, combined with a lack of technological familiarity, pose challenges to informed consent (Chung et al., 2016; Hine et al., 2022). Programs designed for reminiscence may inadvertently become tools of interrogation (Goodall et al., 2020), and difficulties with technology can lead to disuse and frustration (Leonardsen et al., 2020; Møller, 2020). In healthcare settings, digitization and telehealth use risks creating distance between providers and those seeking care, diminishing the ability of providers to form meaningful relationships with their patients (Leonardsen et al., 2023). Further, some older adults have expressed concerns that smart home technologies designed to support aging in place may paradoxically foster dependency on the technology itself, creating an overreliance on technology to perform daily tasks (Chung et al., 2016).
This article deepens understandings of the implementation and use of technology in person-centered dementia care through the perspective of those often responsible for implementing it: care providers. As part of the NIH-funded consortium Leveraging an Interdisciplinary Consortium to Improve Care and Outcomes for Persons Living with Alzheimer’s and Dementia (LINC-AD), two in-person meetings of the Alzheimer’s Association Dementia Care Provider Roundtable (AADCPR) were focused on this topic. The first meeting, facilitated by LINC-AD members in June of 2023 included 41 dementia care thought leaders and focused primarily on the conceptualization and challenges inherent to person-centeredness, including questions related to technology. Participants included long-term and healthcare providers (n = 25), home- and community-based service providers (n = 6), dementia and long-term care workforce advocates (e.g., affiliates of the Alzheimer’s Association and the National Association of Health Care Assistants; n = 5), and members of the LINC-AD research team (n = 5). A follow-up meeting in December of 2023 focused on the future of technology and person-centered dementia care; 34 dementia care thought leaders, including long-term and healthcare providers (n = 17), home- and community-based service providers (n = 7), dementia care advocates (e.g., affiliates of the Alzheimer’s Association; n = 7), and technology pioneers and researchers (n = 3) attended this meeting. Both meetings were facilitated by researchers and focused on questions related to the concept of person-centeredness, the design and implementation of technology in dementia care, and its impact on person-centeredness (Appendix).
Discussions from both meetings were recorded with permission from AADCPR attendees and exploratory thematic analysis was performed on recordings and session notes. Common topics discussed by roundtable attendees were identified by a member of the research team and consolidated into preliminary themes. Preliminary themes were shared with and reviewed by the authorship team, including members of LINC-AD and AADCPR attendees. Three final themes, and related sub-themes, were agreed upon by the authorship team. Quotes and key points related to each were then extracted from recordings and are presented below.
Key Points
Roundtable discussions on technology and person-centered dementia care focused on three related yet distinct topics: recommendations for designing person-centered technologies, recommendations for the implementation of person-centered technology, and the impacts of technology on person-centeredness. Providers offered numerous suggestions while discussing a variety of technologies designed for long-term care staff, individuals living with dementia, and their care-partners. Although conversations centered primarily around dementia care in long-term care settings, many of the themes discussed are more broadly applicable, and collectively provide a roadmap for both providers and innovators to enhance the person-centeredness and effectiveness of care technologies.
Recommendations for Designing Person-Centered Dementia Care Technologies
The initial design of technology was widely recognized by participants as informing both its person-centeredness and effectiveness in implementation. Participants noted that to be person-centered, technology must account for the needs of not only the person living with dementia, but also those tasked with its implementation. Providers noted that poorly designed digital tools provide minimal contributions to workflow or care. They discussed strategies to design effective person-centered technology and noted that person-centered technologies (i.e., those that are founded in principles of person-centeredness, such as individualization and choice) must embrace collaborative design, and recognize “real world” environmental and individual limitations as well as the need for both efficiency and flexibility.
A collaborative design approach begins by “asking direct care staff, residents, and families what are the actual barriers [to quality care], and then from there look[ing] to implement innovations based on what the barriers are.” Providers noted that for individuals with dementia there are often discrepancies between the intended use of technology and the realities experienced by the population, such as wearable technologies that are immediately taken off or will not be worn. To bridge the gap between vision and reality providers stated that “dementia subject matter experts… people who know what really goes on in the real world” must be included in the technology design process to ensure that resulting interventions are acceptable and feasible for those they are intending to help.
Technology must be easy to use and complement existing workflows, such as digital portals that can give care staff readily accessible and up-to-date data prior to entering residents’ rooms. One provider noted that technology must be compatible with the setting’s existing infrastructure, stating “I would love technology that doesn’t take more wi-fi; I don’t have the wi-fi bandwidth for half of these really cool things that I need.” Providers noted that technologies designed to create care plans should use person-centered language emphasizing the agency of the individual living with dementia (e.g., “Ms E prefers a shower” vs. “Give Mr M. a bath”). By using person-centered language, technologies can prompt staff to involve persons living with dementia in their own care, honoring their agency and preferences. The flexibility and accessibility of technology was also discussed, and also the need for technologies to accommodate variations in age, education, income, technological literacy, culture, language, and cognitive capability; put simply, “we don’t want tech that is cookie cutter.”
The active involvement of the end-user in developing digital healthcare tools is well established as integral to the quality of care-based technologies (Leonardsen et al., 2020); many older adults express explicit interest in co-designing technologies, advocating for, among other features, larger fonts, fewer buttons, and voice activation capabilities (Wang et al., 2019). Unfortunately, current technologies do not always reflect a person-centered design approach (Ollevier et al., 2020), and while co-creation and participatory design of technology for persons with dementia is becoming increasingly prevalent, many still do not involve the end-user in design and/or implementation (Goodall et al., 2020). Consequently, many technologies fail to account for the physical and sensory impairments experienced by older adults and those living with dementia, requiring navigation of overly sophisticated and complex applications, or requiring competency across a fragmented landscape of platforms (Sweeney et al., 2021; Wang et al., 2019). For those living with dementia, poorly or non-dementia friendly designed technologies may often go unused, cause feelings of frustration, or foster increased dependence on their care-partners (Goodall et al., 2020; Møller, 2020; Sweeney et al., 2021).
Recommendations for the Implementation of Person-Centered Technology
Facilitators to Implementation
When choosing technologies, providers described a needs assessment as the first step to successful implementation, stating that oftentimes “organizations think they know what the barriers are, but they really don’t.” After the need has been identified, organizations must purposefully select vendors who will act as “tech partners, not just a vendor, you want someone who’s willing to adjust, and adapt, and be flexible with the constraints you may have.” Once the technology and vendor are chosen, obtaining staff buy-in “from the bottom up” and ensuring that those who will use the technology understand its significance are critical to sustainable use. One participant said “nothing is ever going to be adopted if we’re just saying this is what we’re doing now and not explaining the ‘why’ behind it.” Alongside initial buy-in, providers highlighted the importance of leadership in creating an environment for ongoing feedback from users and recipients, and the need to iteratively refine platforms and initiatives. Several participants described the identification of a “tech champion” as a key component behind sustaining new practices, noting that leadership can facilitate these champions by “celebrating team members who embrace the enhancements and are thinking innovatively.”
Choosing the appropriate technology for the correct setting or individual is important to its implementation (Cho et al., 2023). Similarly, the identification of a tech champion who can successfully advocate for the adoption of new technologies may help facilitate uptake of new initiatives (Miller et al., 2023). Existing literature also highlights the effect of social relationships on successfully implementing technology; technology must be introduced in a non-judgmental space and manner (Miller et al., 2023), and for those living with dementia, the “co-use” of new technologies with supportive care-partners can improve both engagement and enjoyment (Sweeney et al., 2021). However, further research is needed to better understand the impact of the dynamic between providers and vendors on the implementation and person-centeredness of dementia care technologies.
Barriers to Implementation
Discussions surrounding barriers to implementing person-centered dementia technology largely centered around resources and turnover. One participant noted that “constant staff turnover, turnover in residences, move-ins and move-outs change the semantics of the whole neighborhood.” This fluidity results in frequent onboarding and retraining and was described as a barrier towards innovation and consistent use of technologies. Others noted the persistent lack of funding as limiting the purchase of new technologies or upgrading existing infrastructure to accommodate them. To ease this financial burden, providers discussed marketing benefits to potential residents and family members to increase occupancy rates. One participant noted “if I was choosing a community, it would absolutely be [a] priority for me [about] how are you keeping mom or dad engaged…market the heck out of it.” Another described showcasing stylistic technology such as large TV screens when providing tours for prospective residents noting that you “have to be creative because you’re caring for people but you’re also selling your space.” Still, others described a general lack of familiarity and even fear of new technologies among both older adults and those who care for them, with innovations such as AI being extremely foreign to many individuals, limiting their uptake.
Extant literature similarly reports the impact of resource limitations and stigma on technology uptake. Limited financial resources can reduce the accessibility of person-centered technology (Chung et al., 2016; Goodall et al., 2020). And, while older adults may be willing to share personal data with medical professionals and family, concerns remain that the data collected by technology will cause a loss of privacy and be misused (Chung et al., 2016; Wang et al., 2019). To reduce stigma and fears over the misuse of technology, principles of informed consent offer a path forward. Examples include providing accessible and relevant information about the technology to older adults, ensuring comprehension regarding the use and purpose of the technology, providing opportunities for peer mentoring (Chung et al., 2014), and allowing older adults and their families to opt out of the use of the technology.
Impacts of Technology on Person-Centeredness
Positive Impacts
When describing person-centered dementia care, regardless of setting, providers stated that knowledge of the person such as “knowing whether or not they are huggers, whether they like a soft voice, or whether they need a little more volume” was a key aspect to person-centered care. It was widely agreed that digital care platforms can increase effective and timely communication of preferences and needs between staff, care-partners, healthcare providers, and individuals. By providing knowledge “about that person before you even consider providing some kind of care” and allowing the quick transfer of data from one care setting to another, these platforms may facilitate greater individualization and person-centeredness in dementia care. Additionally, providers noted that emerging AI models have the potential to scan care notes, flag individuals with an elevated risk for falls or other safety concerns, and provide individualized preventive plans.
For persons with dementia, providers discussed the potential of technologies designed to increase resident engagement to reduce the use of antipsychotics and other pharmacological interventions. One provider hypothesized “by increasing engagement we’ll see decreases in behavioral expressions … result[ing] potentially in a decreased use of psychotropic medications.” Others noted that technological monitoring can increase autonomy and independence for long-term care residents with dementia, giving staff tools to unobtrusively ensure the continued safety and well-being of residents while allowing residents “to be able to move about freely…[providing] a perceived sense of independency, autonomy, and choice.”
Other technologies were described as “taking the things that are repetitive and boring” off staff workloads and increasing staff’s capacity for engagement through the streamlining of non-resident facing tasks, such as cleaning. While increasing staff efficiency was perceived as a positive, providers noted that technology should not be designed to replace human interaction but instead enhance programming already in place; “we want tech that enhances our programming but doesn’t take away us doing it, we want it to work with us and help us and not just do it for us.” This goal could be achieved by pairing digital experiences “with a programmatic element like … an event and creating a better, larger, more integrative experience and stimulating a resident living with dementia’s ability to share their experiences and have a more joyful experience.”
Literature surrounding the role of technology in person-centered communication and engagement is well established, with technology providing older adults the means to engage with both others and their own past self in new and innovative ways, such as through digital storytelling programs (Goodall et al., 2020) or virtual reality visitations to childhood haunts (Miller et al., 2023). Within long-term care, technologies can facilitate resident engagement by providing a structure for staff to organize resident programming (Neal et al., 2020). While the evidence surrounding the effectiveness of technology on reducing behavioral expressions of persons with dementia varies (Chan et al., 2021), a recent meta-analysis of non-pharmacologic information and communication technology-based interventions found statistically significant effects of these technologies on both depression and agitation (Cho et al., 2023). Additionally, the use of video platforms containing messages recorded by family members has the potential to reduce resistance to care and improve the mood of individuals living with dementia (Goodall et al., 2020).
Many practice recommendations for person-centered dementia care such as getting to know the individual, building authentic relationships, and providing meaningful opportunities for engagement, require substantive time spent with the person (Fazio et al., 2018). For home care organizations, digital planning and registration systems can reduce workload related to manual scheduling and recording of time spent on care delivery, negating the need for hand-written forms and subsequent data entry, and in long-term care settings the digitalization of administrative processes and resident records can facilitate documentation processes (Thoma-Lürken et al., 2015). While organizations report anecdotal labor-saving effects related to these technologies (Thoma- Lürken et al., 2015), there is a need for further research on both their cost-effectiveness and the impact of increasing efficiencies on relationship building and person-centered dementia care.
Negative Impacts
Although technology was discussed as having potential to increase the person-centeredness of dementia care, there was a consensus that organizations and individuals must use caution that they do not lead to depersonalization and poorer quality of care. Examples included care planning software, which, while useful, may result in a one size fits all approach producing non-person-centered “overly prescriptive” interventions. Other interventions, such as robotic pets for persons living with dementia “may calm one person…and at the same time become very agitating for the person sitting next to them.” Participants also discussed concerns that technology may replace human interactions among dementia care, stating, “it can be problematic if staff members start thinking of [technologies] as a way to be the sitter instead of having direct care provided by a human.”
Current literature reflects the need for person-centered decision making when implementing technologies. For instance, while the use of robotic pets for those living with dementia may have positive impacts for some, there remain concerns that certain individuals may find the use of these pets demeaning, and that they may increase agitation for those experiencing more advanced stages of the disease (Chan et al., 2021; Neal et al., 2020). Others have highlighted concerns that technology may hinder person-centeredness by removing the opportunity for human-human contact (Leonardsen et al., 2023), or reduce social engagement by replacing meaningful personal interactions with browsing the web or playing digital games (Kiselica et al., 2024). Another concern is that many technologies focus on providing functional assistance or maintaining safety with little emphasis on supporting self-esteem, agency, or the personhood of the individual (Koo & Vizer, 2019). A potential solution to some of these issues is designing technologies that align with theoretical approaches to person-centeredness, creating interventions focused on increased engagement and cultivating a greater sense of self-identity (Goodall et al., 2020).
Implications for Practice Policy and Research
Roundtable discussions provided several avenues for future research surrounding technology and person-centered dementia care: the dynamic between providers and vendors; the effectiveness of marketing non-care-related “stylistic” technologies to increase financial sustainability for care-related technologies (such as medication dispensers and care platforms); and the link between technology enabled efficiencies and person-centered dementia care. Future exploration of these and other topics could provide meaningful data to both providers and innovators and assist advocacy efforts for the continued investment in person-centered dementia care technology.
As demonstrated by roundtable discussions and current literature, a wide range of barriers, facilitators, and considerations exist when designing and implementing person-centered dementia care technology. It is at this juncture where implementation science, and its focus on translating research and implementing evidence-based practices, is most fruitful to translate technological innovation into practical application. Implementation science recognizes the impact of numerous complex factors and barriers on intervention adoption, including those related to the innovation itself, system-level characteristics, the implementation process, and more (Bauer et al., 2015; Zimmerman et al., 2021).
Fortunately, there is a tool to unify these factors into an actionable framework: the Hexagon Tool developed by the National Implementation Research Network at the University of North Carolina at Chapel Hill (Metz & Louison, 2018). The Hexagon Tool assists organizations to evaluate new and existing programs along six contextual fit and feasibility factors composed of three implementing site indicators—Capacity, Fit, and Need—and three program indicators—Evidence, Usability, and Supports (Metz & Louison, 2018). Drawing from the literature, the Hexagon Tool has potential related to person-centered dementia care technologies. To better organize and translate the provider recommendations presented in this article into practice, Figure 1 presents a novel Modified Hexagon Tool for Designing and Implementing Person-Centered Dementia Care Technologies. Similar to the original Hexagon Tool, this modified version organizes provider recommendations related to person-centered dementia care technologies into three considerations for implementation—Capacity, Fit, Need and three factors relevant to the technology itself—Evidence, Design, and Supports. This tool offers providers and technology developers the opportunity to consider factors impacting the effectiveness and person-centeredness of dementia care technologies in long-term and other healthcare settings. Further research related to the Modified Hexagon Tool for Designing and Implementing Person-Centered Dementia Care Technologies is needed to validate this framework and related recommendations. Adapted with permission from The Hexagon Tool © 2018 NIRN – University of North Carolina at Chapel Hill (Metz & Louison, 2018)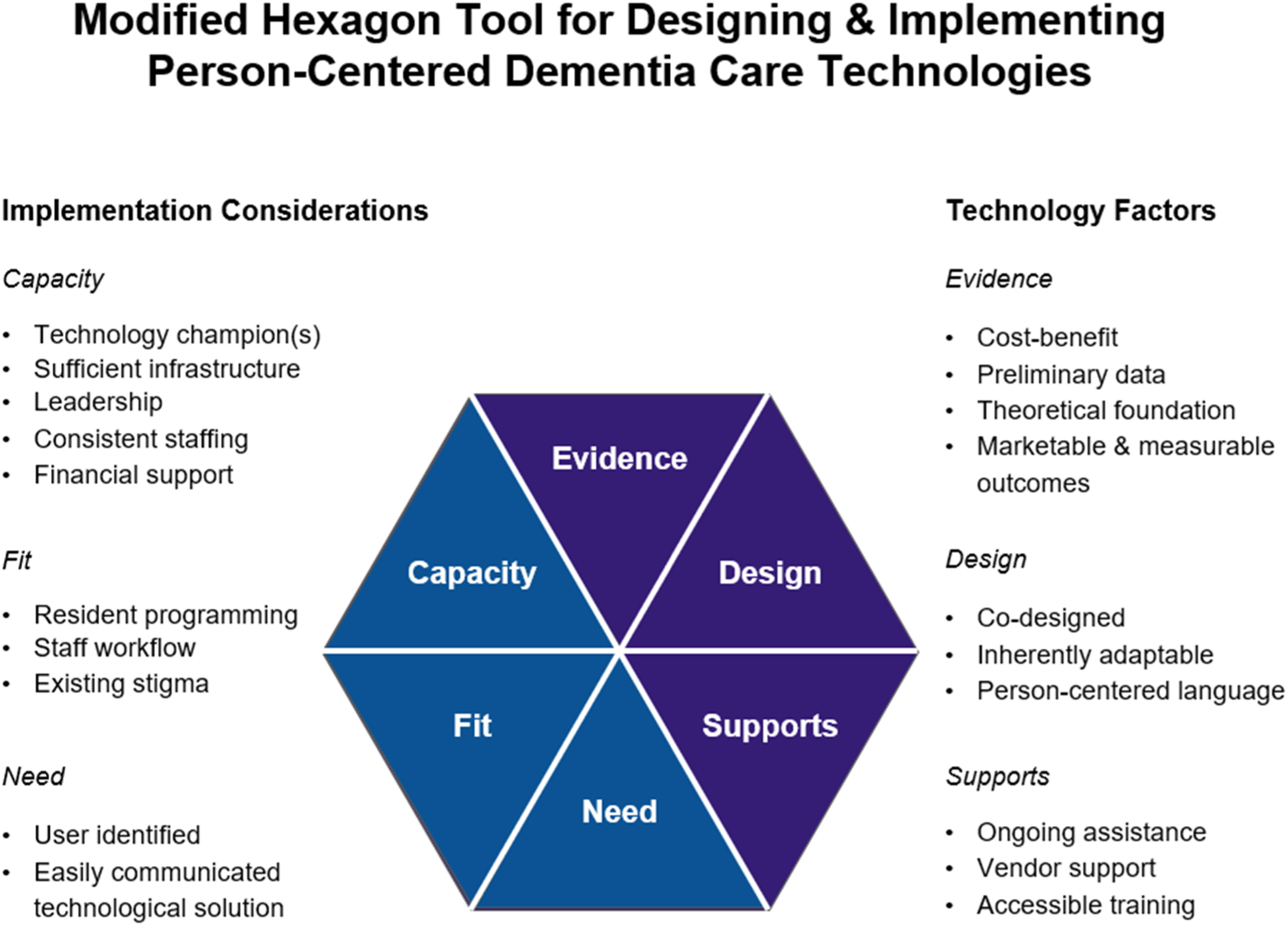
When considering this article’s findings, it is notable that much of the discussions and related recommendations were specific to long-term care settings, despite the presence of home- and community-based providers. While perhaps reflecting the language of the questions themselves being commonly associated with long-term care settings (e.g., “organization” and “culture-change” [Appendix]), additional work is needed to explore topics relevant to home- and community-based settings. Such topics may include the impact of intergenerational living on digital literacy, and the difference in costs associated with acquiring technology for individuals versus groups living in congregate settings. It is also noted that although providers represented a variety of settings and organizations, the sample size (n = 75) when compared to the vast array of existing services and organizations, may impact generalizability, and individuals living with dementia were not directly included in these conversations. Finally, while this special article contains findings from two AADPCR meetings, it does not constitute a systematic research study. Future research is needed to validate and explore this article’s perspectives and recommendations.
Conclusion
The integration of technology into person-centered care for older adults, particularly those with dementia, holds significant promise and challenges. The insights gathered from two Alzheimer’s Association Dementia Care Provider Roundtables indicate that while technological innovations may potentially enhance communication, increase engagement, and provide non-pharmacological solutions, they must not replace human interaction or become overly prescriptive. The person-centeredness and effectiveness of these technologies begins with a person-centered design approach, one that ensures accessibility, usability, and adaptability and directly involves those living with dementia and their care-partners. Roundtable discussions emphasized that effective implementation requires choosing supportive tech partners, obtaining comprehensive buy-in, and overcoming resource constraints. As the number of older adults living with dementia continues to grow, continued research and development, guided by frameworks such as the Modified Hexagon Tool for Designing and Implementing Person-Centered Dementia Care Technologies may help ensure that technological advancements truly support the holistic well-being of those living with dementia and their care-partners.
Supplemental Material
Supplemental Material - Provider Perspectives on the Design, Implementation, and Impact of Technology on Person-Centered Dementia Care: Insights From the Alzheimer’s Association Dementia Care Provider Roundtable
Supplemental Material for Provider Perspectives on the Design, Implementation, and Impact of Technology on Person-Centered Dementia Care: Insights From the Alzheimer’s Association Dementia Care Provider Roundtable by Lauren Stratton, Walter Moczygemba, Sheryl Zimmerman, Maggie Cattell, Lakelyn Eichenberger, Merle Griff, Sam Fazio in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors thank the members of the Alzheimer’s Association Dementia Care Provider Roundtable for contributing their expertise and time.
Ethical Considerations
This special article presents information gathered from two Alzheimer’s Association Dementia Care Provider Roundtable meetings, and not a systematic investigation. Such effort does not meet the Code of Federal Regulations (CFR) definition of research and IRB approval was neither sought nor required.
Author Contributions
Lauren Stratton; Lead author, methodology, review and revision, facilitated discussion
Walter Moczygemba; Drafted article, interpretation of data
Sheryl Zimmerman: Methodology, wrote prompts for discussion, facilitated discussion, and provided input on and approved article
Maggie Cattell; Review and approval of article
Lakelyn Eichenberger; Review and contribution to the roundtable discussion
Merle Griff: Review and contribution to the roundtable discussion
Sam Fazio; Methodology, review of article
Funding
The authors disclose receipt of the following financial support for this article: This work was funded by the National Institute on Aging grant R24 AG065185.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.