
Abstract
This study explored the supportive relationships that former system youth (FSY; e.g., foster care) with mental health challenges identified as “key” in making the transition to adulthood. In-depth semi-structured interviews were conducted with 59 FSY, ages 18 to 25, with mental health challenges. Participants were asked to reflect on their relationships with a key helper or what the literature defines as a natural mentor, “an adult that has been particularly helpful, or supportive,” in this case with their mental health. Seventy-six percent (N = 45) of the participants identified a key helper. Relationship qualities that emerged as salient to successful transition included consistency, mutuality, and empathy. The nature of support received included emotional, informational, and tangible support. Implications for research, practice, and policy are discussed.
A successful transition to adulthood hinges on resources and opportunities, including consistent relationships with supportive adults. However, access to such resources may be limited for more vulnerable young adults, such as those who have moved in and out of mental health, child welfare, and juvenile justice systems. It has now been well documented that these young people, often referred to as “system youth” (see Grisso, 2004; Osgood, Foster, Flanagan, & Ruth, 2005), tend to have significant difficulties in a number of important life domains, including education, employment, and mental health (Collins, 2001; Courtney et al., 2007; Osgood et al., 2005). One important factor contributing to the poorer outcomes of former system youth (FSY) may be the lack of sustained and consistent connections with key supportive contacts they can carry forward from childhood (Osgood, Foster, & Courtney, 2010). Furthermore, FSY with mental health challenges and mood disorder histories often carry relational vulnerabilities rooted in their past experiences that can make it challenging for them to develop and maintain healthy relationships, such as trauma symptoms (Cecil, Viding, Barker, Guiney, & McCrory, 2014), mistrust related to negative experiences with public systems of care (Scott, McCoy, Munson, Snowden, & McMillen, 2011), insecure attachment styles (Marganska, Gallagher, & Miranda, 2013), and affect dysregulation (Dvir, Ford, Hill, & Frazier, 2014). The need for supportive relationships among FSY is recognized. For example, the Fostering Connections Act acknowledges that the state has the responsibility to act as guardians for system youth into early adulthood and providing services to help foster support, including relational connections, to become successful adults (Osgood et al., 2010). However, little is known about how prevalent such connections are among FSY or about the nature and quality of the relationships that FSY do form and sustain and what aspects of these relationships are considered to be most valuable and helpful in their eyes. To better support FSY in developing the critical connections needed to navigate well the transition to adulthood, a better understanding of the supportive relationships experienced by FSY with mental health challenges is needed.
The presence and quality of supportive relationships has a significant impact on whether or not individuals transition to successful and independent adult roles (Osgood et al., 2010). The importance of relationships with people who can offer various forms of aid and assistance more generally is well documented in the literature on social support, resilience (Masten & Coatsworth, 1998; Werner & Smith, 1992), and positive youth development (Leffert et al., 1998). The presence of supportive relationships with non-parent adults is associated with positive outcomes in multiple life domains. Social support research indicates that health and mental health outcomes improve when individuals are engaged in social relationships (House, Landis, & Umberson, 1988). Social ties may influence behavior, including specific health behaviors (i.e., going to a doctor’s appointment), emotionally by reducing feelings of stress and enhancing one’s sense of personal control over life choices and decisions, and physiologically by improving health and decreasing physiological responses to stress (Umberson & Montez, 2010).
Social support can be provided in the context of both informal and formal relationships. According to Gottlieb (1983), “social support consists of verbal and/or nonverbal information or advice, tangible aid or action that is proffered by social intimates or inferred by their presence and has beneficial emotional or behavioral effects on the recipient” (p. 28). Research that focuses explicitly on social support between youth with mental disorders and supportive others is sparse; however, research on resilience makes clear the importance of supportive ties for vulnerable youth. Wagner and Davis (2006) conducted a review on “exemplary practices” to help youth with emotional disturbances and identified relationships as one of the five principles that help them most in finding success in early adulthood. Also, a study of young adults hospitalized during adolescence reports that for a small group of “resilient” young adults, relationships were a key resource for them (Gralinski-Bakker, Hauser, Billings, & Allen, 2005).
Little is known about the prevalence and function of such relationships in the lives of FSY. One study (Samuels, 2008) examining social relationships and social networks among young adults transitioning from foster care found that although participants considered biological family to be important to them, these family members often did not provide much in the way of emotional or tangible support. More generally, participants reported a lack of emotional support and a lack of consistent relationships, and some participants reported a sense of distrust in relationships. Another study (Samuels & Pryce, 2008) revealed that not only were young adults “aging out” of foster care not receiving much support, they were often serving as a provider of social support for their family members. These studies suggest that FSY may have an even more heightened need for support from sources outside of the family, given that they tend to provide but not receive much support from family members.
Adults other than family members can play important roles in the lives of FSY, but here again, little is known about the prevalence and nature of these ties. Like young people more generally (Spencer, Jordan, & Sazama, 2004; Werner & Smith, 1992), research on transitioning foster care youth indicates that a wide range of adults may provide support, including teachers and other community leaders, but also that professional case workers also figure prominently as sources of support for these youth (Collins, Spencer, & Ward, 2010). Others (Werner & Smith, 1992) have observed that spouses can also serve as important sources of support for resilient young adults. Further research is needed to identify who these non-parent adult providers of support are in the lives of FSY with mental health challenges.
Research on social support relationships among more mature adults with mental illness and their supports suggests that peers, defined as others who have a shared lived experience, can offer positive outcomes (Davidson, Bellamy, Guy, & Miller, 2012). There has been less conclusive research on what the underlying mechanisms of this help is or “what precisely peer staff do—beyond disclosing their own history and recovery” (Davidson, 2013, p. 1); but peer support has been found to be related to positive outcomes for adults with mental illness, such as fewer rehospitalizations and fewer hospital days (Sledge et al., 2011). Furthermore, research on family support has shown that family psychoeducation can be effective in helping individuals with mood disorders and their families (Miklowitz et al., 2000), along with those living with schizophrenia (Dixon et al., 2001). Others have noted that through family interventions, such as Journey of Hope (JOH), family members may be provided with the support and knowledge to cope with their ill family members’ illness (Pickett-Schenk, Cook, & Laris, 2000). In light of the central role that relationships play in making a successful transition to adulthood, more research is needed to understand the key ingredients of supportive relationships needed to make them a key resource in the lives of FSY with mental health challenges. This can critically inform program development, training, screening, and the overall design of mental health and services.
Rhodes’s (2002) model of youth mentoring (see Figure 1) provides insight into how supportive relationships influence outcomes by explicating underlying mechanisms of mentoring relationships, along with empirically based potential moderators. Rhodes’s model posits a socio-emotional mediating path (based on attachment theory), a cognitive mediating path (based on learning theory), and a role modeling mediating path (based on social cognitive theory). The model suggests that more than one of these mechanisms may be activated in any given relationship. The model brought a theoretical emphasis to an area that had been predominately atheoretical, and it provides a starting point for scholars interested in understanding further the structure and process of supportive relationships among various sub-populations with special needs and their supportive others. The opportunity this study offers is to examine the supportive relationships of one such sub-population from the perspective of the youth, comparing their experiences with Rhodes’s model.
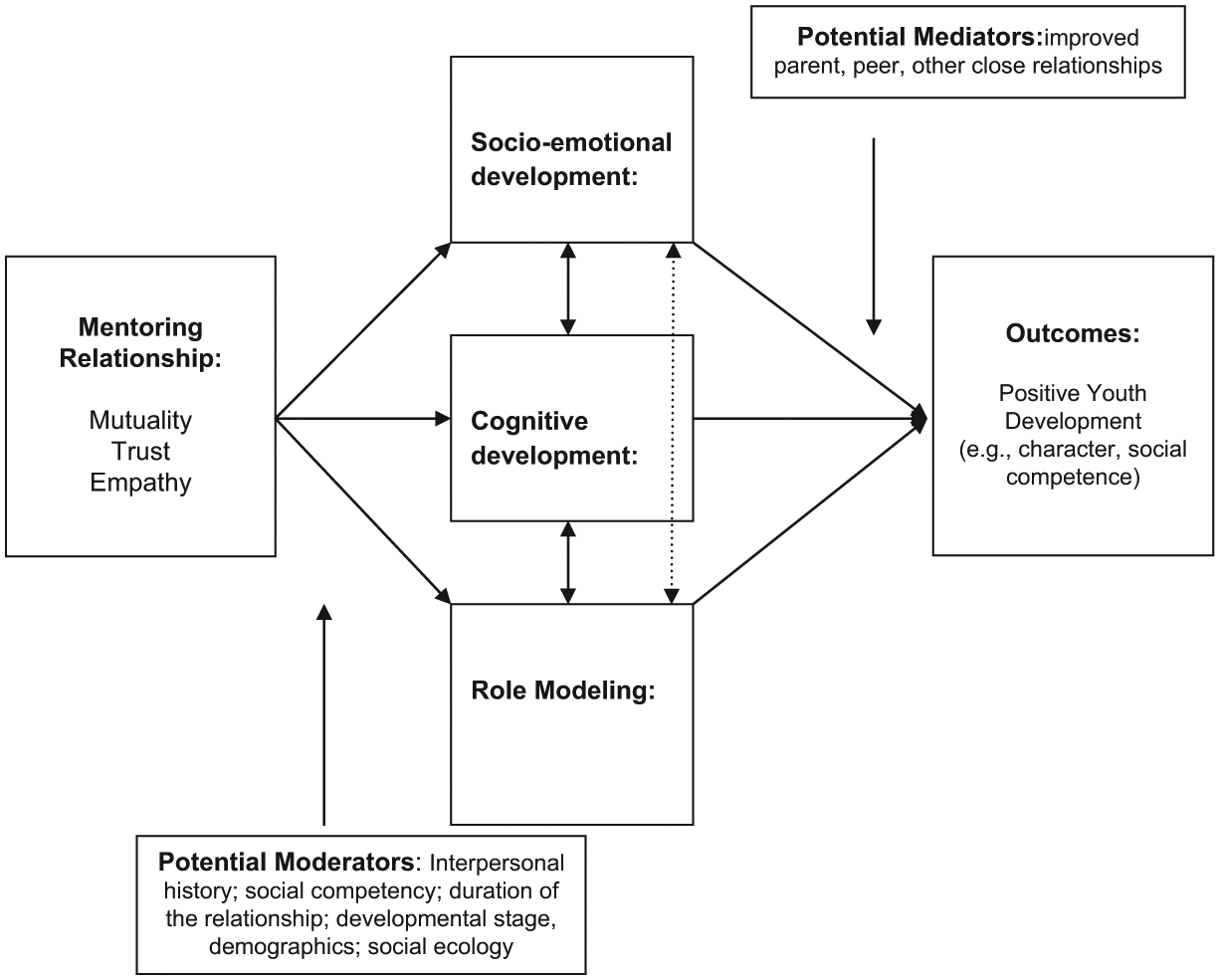
Rhodes’s (2002) model of youth mentoring.
Research on mentoring relationship success and failure, and factors contributing to that success (or failure), informed this study (e.g., Rhodes, Spencer, Keller, Liang, & Noam, 2006; Spencer, 2006, 2007). In one study, Spencer (2006) examined the relational process among adolescents and their mentors and reported that qualities such as authenticity (i.e., being real with each other) and collaboration (i.e., working together on skill development) are critical in the development of successful mentoring relationships. Equally important, Spencer (2007) examined factors that led community-based mentoring relationships between adolescents and their mentors to fail, for example, lack of mentee motivation and deficiencies in mentor relational skills. Studies such as these help build knowledge on specific relational qualities necessary to provide effective mentor-type programs and opportunities for our most vulnerable youth and young adults.
A few more recent studies have built on the research of Rhodes and Spencer and begun to examine the same question among older youth in foster care and former foster care youth (Ahrens et al., 2011; Munson, Smalling, Spencer, Scott, & Tracy, 2010). For example, Ahrens and colleagues (2011) examined data on 23 former foster care youth and their relationships with non-parental adults and found that unique characteristics of support, such as authenticity, respect, and “going beyond their prescribed role,” were significant qualities described as essential for developing relationships. They also reported that patience on the part of the adult was a key factor in relationship formation. And former foster care youth reported that fears of being hurt were barriers to relationship formation.
The present study aims to build on this previous research and explore who FSY with documented mental health needs nominate as their key helpers and how they experienced their relationships with these supportive adults.
Method
Participants
Purposive sampling methods were used to conduct information-rich interviews with young adults who had experienced a unique transition to adulthood, a transition that included three common experiences during childhood, namely, (a) being given a diagnosis of a mood disorder; (b) using Medicaid-funded mental health services; and (c) using at least one additional public system of care (e.g., child welfare, public welfare, juvenile justice). Participants, on average, were involved with 3.3 public systems of care during childhood. All participants were currently struggling with emotional difficulties, which we also assessed for in the telephone-screening interview using self-report. The sample was recruited from three counties in one midwestern state between 2008 and 2010, and participants had to be between 18 and 25 years of age (inclusive) and living in the community. Young adults were excluded if they were actively psychotic, using substances, had used services for developmental disabilities, and/or could not speak English or had communication difficulties that would hinder them from answering interview questions.
The final sample consisted of 59 young adults (M age = 20.97; SD = 2.09). Sixty-eight percent of the sample was female and 68% were Black, African American, or bi- or multi-racial (See Table 1). The present study is part of a larger study, which examined the mental health service use experiences of young adults over the transition to adulthood (see Munson et al., 2012).
Sample Characteristics of FSY (N = 59).
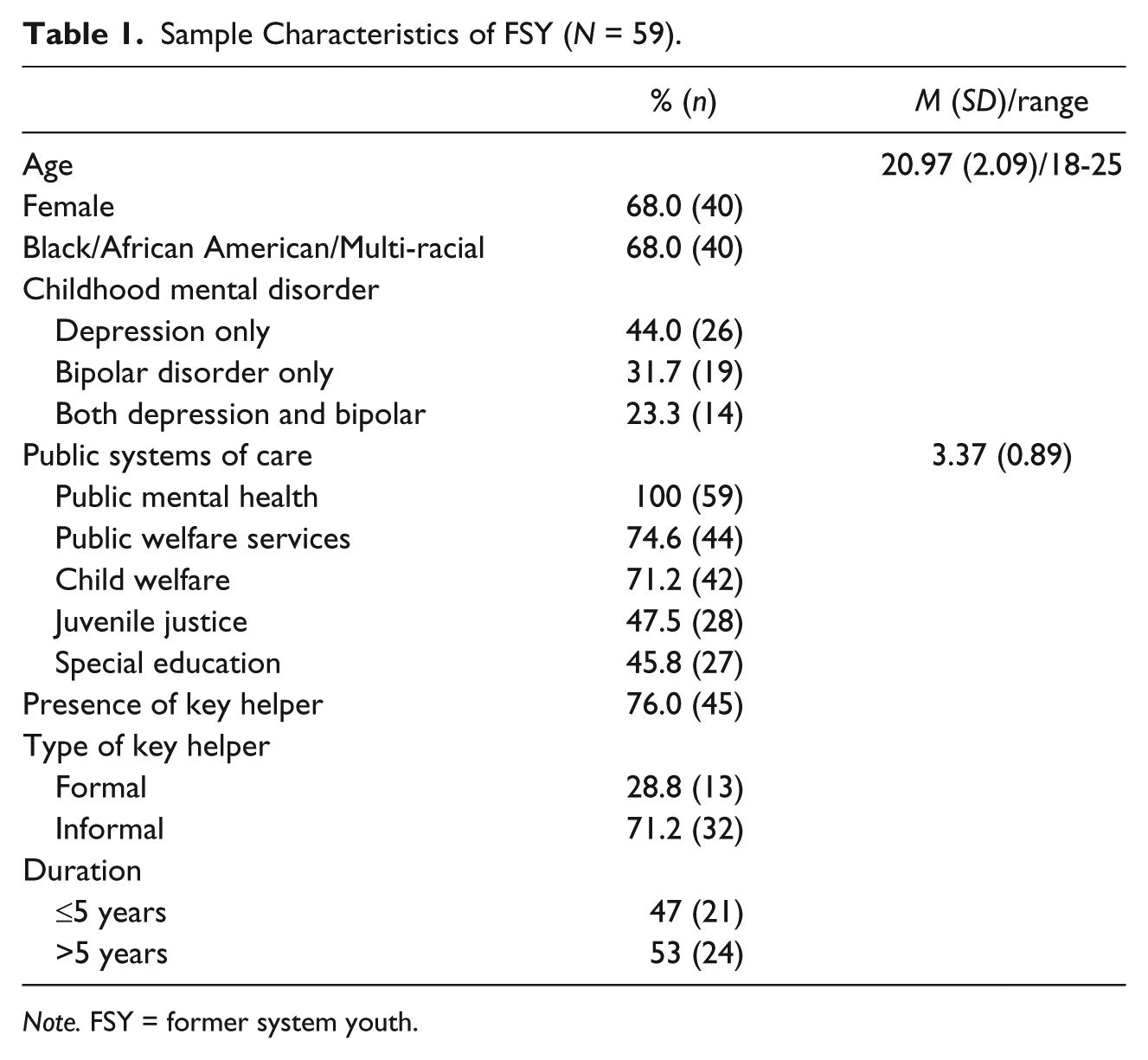
Note. FSY = former system youth.
Recruitment and Interview Procedures
The study used three strategies for recruitment: (a) study advertisements were posted at agencies/institutions serving the target population; (b) study advertisements were posted on telephone poles, in grocery stores, bus-stops, and at local eateries in the study areas; and (c) a variant of respondent-driven sampling. Potential participants contacted the project office and were provided information on the study. They were then administered a 15-minute screening interview. Just over 97% of those who met the study criteria participated in the study.
Face-to-face mixed methods interviews were conducted. Interviews were conducted at a site of the participants’ choosing, often their place of residence, the project office, or in community venues (e.g., social service agencies). The first author or doctoral students (with master’s degrees and training on the interview) conducted all interviews. Participants received an honorarium for completing the study interview. Interviews took between 2 and 3 hours. This research took place over a number of years.
Measurement
In order to most effectively assess for the respondent’s most supportive key helper we went through a series of steps. First, participants were asked whether they had a key helper in their lives, defined as, “an adult that has been particularly helpful, or supportive, in dealing with your mood and emotional problems, or [Fill in with words young adult uses to describe mood and emotional difficulties, i.e., anger, depression, bipolar, life struggles].” Young adult participants first were invited to discuss up to three individuals who met this definition. This was intentionally done to assist the participant in taking some time to think about up to three relationships in detail. After that process, interviewers asked participants to choose the person who they perceived as most helpful in dealing with their mood and emotional difficulties. A semi-structured interview protocol was developed consisting of a set of core questions (see Table 2), along with additional probes. Interviewers were free to adapt and add to these questions in response to participant experiences that emerged during the interview. Furthermore, some modifications were made to the formal protocol twice over the course of the data collection process in response to the principal investigator and research team’s initial analysis of collected interviews. The first modifications were made after examinations of the first few interviews highlighted questions that were more and less clear and relevant to the participants. The second modifications were made after 50 interviews were conducted. At this time, the overall protocol was shortened and approximately half the original questions on key helping relationships were retained. The team observed saturation in the qualitative data at this point as well (Morse, 1995).
Core Questions on Key Helping Relationships.
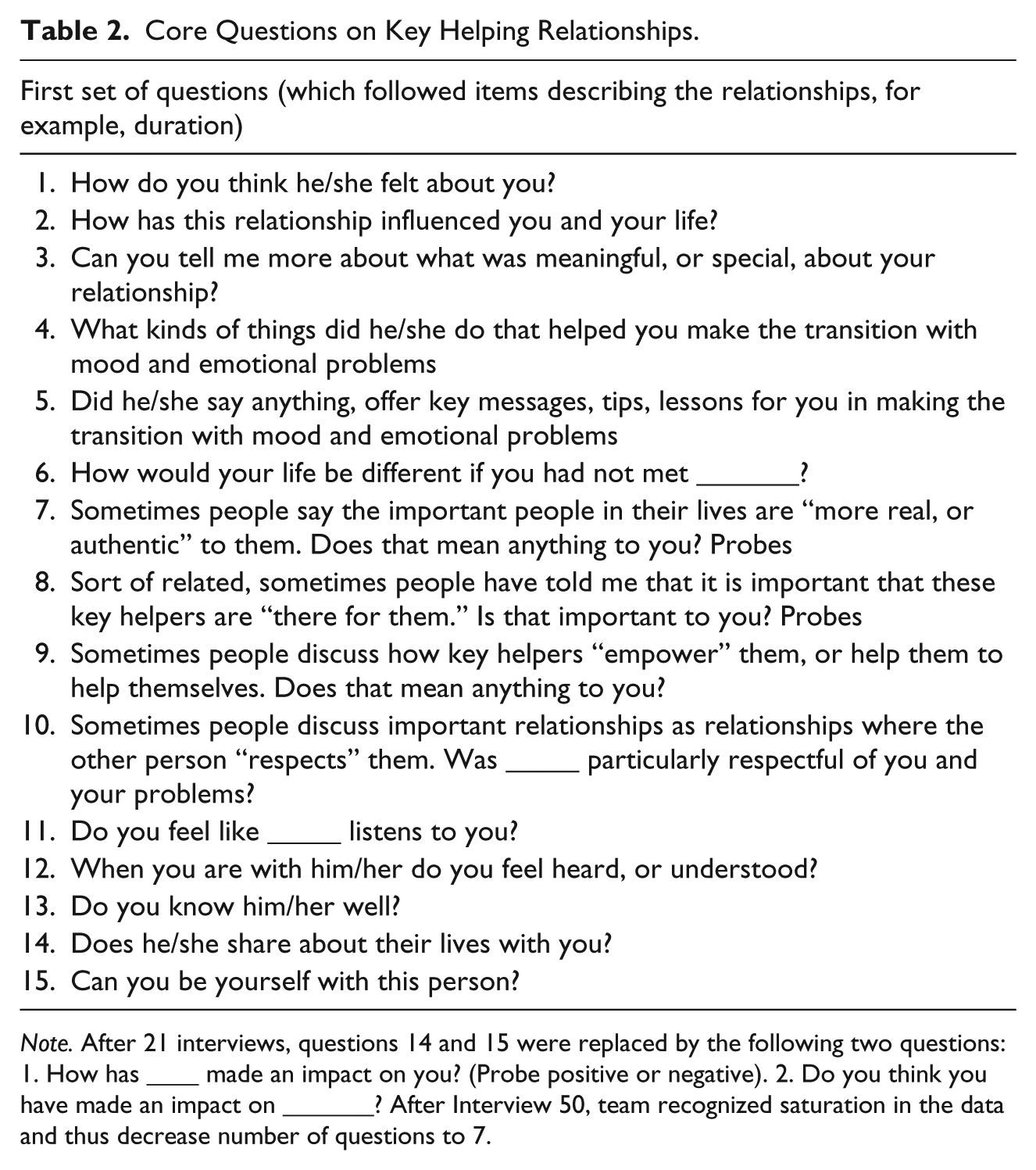
Note. After 21 interviews, questions 14 and 15 were replaced by the following two questions: 1. How has ____ made an impact on you? (Probe positive or negative). 2. Do you think you have made an impact on _______? After Interview 50, team recognized saturation in the data and thus decrease number of questions to 7.
Multi-Phase Analytic Process
Three analysts individually engaged in constant comparison (Glaser, 1965) (a) conducting line-by-line initial coding, and (b) comparing and contrasting meaningful quotations within and between interviews. Analysts began this process with a subset of interview transcripts (n = 5). Beginning with a group of five interviews, each analyst developed initial codes and grouped or axial codes. Then, analysts met to discuss the initial codes and grouped codes, comparing and contrasting individual codes and quotations, while discussing and resolving discrepancies when they occurred. This led to the development of an initial codebook. Two analysts went back and individually coded another 35 interviews, comparing and contrasting new codes with quotations in the initial codebook. Project meetings were held to address unclear codes and codes that were not being applied in the same way. Discrepancies were resolved through consensus. Then, analysts coded the remaining 19 interviews, further refining codes and building reliability in the use of codes. A second stage of constant comparison was conducted on axial codes to derive categories and themes of salient dimensions of the supportive relationships.
Triangulation of analysts (three primary coders, two secondary coders) and data strengthened the reliability of the results. Finally, member and expert checking with one participant, clinicians, policy makers, and scholars further added to the validity of the data. In particular, early on, analysts modified some questions in order to elicit more rich data and narratives on the relationships. Also, the research team repeatedly presented the project in select settings in the community and discussed emerging preliminary results. Discussions added to the understanding of categories and themes that emerged. All of these meetings helped shape the results reported below.
Results
Seventy-six percent of the participants (N = 45) reported the presence of a key helper in their lives. Key helpers were predominately family members (n = 19) and professionals (n = 13), although a few nominated important friends (n = 5), significant others (n = 5), “god-family” (n = 2), and an ex who was their child’s parent (n = 1). Interestingly, the majority (53%, n = 24) of those with a key helper reported that they knew or perceived that their key helper also lived with mood and emotional difficulties. The duration of the relationships in the present study ranged from 1 year to the participants’ “whole life.” Almost half of the relationships had continued for over 10 years, and very few of the relationships cited were of fewer than 2 years’ duration.
The meaningfulness of the support provided was evident in many participants’ responses to a question about how their lives would be different if they had not met their identified helper. Some responded by saying that they thought they would be dead: “Probably I’d be dead, to be honest” (key helper [KH]: Family). Others reported that they would not have accessed help for mental illness: “If it wasn’t for her, I probably wouldn’t have started medication . . . counseling . . . It was my godmom who took me to counseling . . . and being involved and making sure I took medication” (KH: Godmother)]. One young adult thought she would be cycling in and out of the hospital: “I think I would be in and out of the hospital” (KH: Family). Some reported they would have been in prison longer: “Probably been in prison way longer. So I’ve kind of stayed out of trouble when I met her” (KH: Professional). No less important, one young adult reported, made it (life) easier . . . I mean I know I have to deal with the stressful situations, but instead of having to stay there and you know not be able to get out or get away from it for a little while, I know I can count on <key helper> and she just, she’s there. (KH: Friend)
In the sections below, both the characteristics of these significant helping relationships as identified by the participants are detailed followed by a delineation of the specific forms of social support they provided these FSY with mental health challenges.
Characteristics of Supportive Relationships and Nature of Support
Relationship characteristics
The features of the supportive relationships that were identified as being of importance to these participants were as follows: (a) consistency/availability, (b) feeling connected, (c) empathy, (d) conversations, (e) mutuality, and (f) acceptance.
Consistency and availability
Young adults placed great emphasis on “having regular contact” with a consistent person (“through thick and thin”) and spoke to how meaningful this was to them, especially with regard to helping them manage their emotions. As one FSY stated, That’s why I always tell them consistency is key. I have to have somebody I can see at least once a week because, if not, you know a lot can happen in seven days, and if I don’t have anybody to talk to, then that emotion stays bottled up inside. (KH: Professional)
Statements such as “always there” and “never leaves” were commonly made by these participants. For example, one FSY discussed the consistent presence of her mother, despite the trouble she thought she had caused her: “’cause I’ve put her through hell and she’s still there for me. I’ve put my whole family through hell and my mom is still there for me” (KH: Family).
Availability was also mentioned as an important aspect of these key helper relationships. As one participant said, You know some psychiatrists or some counselors, you have to make a date with, or more you have to come on your scheduled time or when they’re free, but <key helper>, you could call them. If they have a minute to talk to you, they’ll talk to you, or leave a message, they’ll call you right back. It’s just someone there besides family. (KH: Professional)
These descriptions illustrate the value that FSY place on consistency and availability, qualities that some of the participants perceived as difficult to find. One FSY suggests that their key helper would travel from another city to be there to make sure they are OK: She’s always there if I need her, and she’s all the way in [another city]. She’ll get here doing 90 to make sure that I’m all right. She’s just all around supportive, and fun-loving and caring, just a real cool person. (KH: Friend)
For some participants, the consistency of the relationship sustained them even through very difficult times when others have given up: It’s definitely gave me a sense of support, because everybody else said they were going to give up or did give up. She didn’t. That’s crazy ’cause I put her and everybody else in the world through so much crap, but she’s just always there waiting, like “Are you going to give me more crap or are you going to stop?” (KH: Significant other)
Another participant revealed how important it was to her that her key helper maintained a relationship with her, sticking with her through the difficult times: I mean I really appreciated him for just being able to stick it out with me through everything. That was really important to me that he stuck it, you know, no matter how many times I threw stuff at him, you know what I’m saying, he was there. So that was really important. (KH: Ex-boyfriend)
Key helpers nominated in this study offered supportive relationships that lasted a long time and provided consistency, which was especially important to most of these FSY. They felt they could count on their key helpers in tough times, and, for some, this relationship had become one that they had internalized and carried with them even when they were not physically with their key helper. Thirty-nine percent (n = 23) of the FSY in the present study, and 51% of those who nominated a key helper, spoke about one of these dimensions of consistency, many of them more than once. Furthermore, the key helpers nominated and perceived to be providing consistency for young adults represented each “type” of key helper described above.
Cared for, loved, and “connected”
Many of these young adults described feeling a deep connectedness to their key helpers, both professionals and non-professionals. Feeling cared about and loved was discussed as an aspect of feeling connected. In discussing his connection to his key helper, one participant indicated that the fact that she made herself readily available showed that she cared about him: “You know she gave me her number. I can call her in emergencies or even not emergencies, and she just, she cares a lot” (KH: Therapist). Another FSY uses the words “caring” and “loving” when describing how she “can tell” that her former foster mother cares for her and the value placed on continued connection after leaving the system: I can tell. I know she loves me. I can tell you that much . . . She gets on my butt about it, but she does, she really does care about me, cause if she didn’t, even after I left from being in foster care with her, she wouldn’t still do half the things that she does for me now that she did when I was staying there. (KH: Former foster mother)
These expressions of caring and connection were important ingredients in relationships described by FSY with mental health challenges. In some cases, young adults perceived that their identified relationships led to important young adult outcomes, including motivation to pursue their goals and a desire to do better: Every child wants to be loved and to have somebody there, to know that they care about them, and I think that that’s what made me actually start wanting to do better for myself, because she actually showed that she cared about me, and she actually wanted to see me succeed in life. Like I said, she was always a big support in everything that I did. (KH: Former foster mother)
Empathy
Data suggest that FSY place great value on empathy, which was enhanced when key helpers possessed a shared understanding of specific experiences. Data reveal that for some FSY the understanding developed through shared experiences and/or common backgrounds. For example, one young adult describes how shared experience leads to understanding: “She is somebody who had a difficult growing up experience, and so she understands what that’s like to come from dysfunctional families and still try to become a productive citizen” (KH: Friend). Another young adult describes how similar experiences, such as living with a mental illness, leads to shared understanding and empathic responding: We’ll be talking about being depressed and I’ll be like, “Yeah, and you know how when you just want to shut yourself away and just not talk to anybody,” and she’s like “. . . I know what that’s like.” We have similar experiences. (KH: Friend)
For some of these young adults, sharing the same diagnosis was experienced as facilitating understanding, “. . . I think he understands because he was diagnosed bipolar too and ADHD too. So like he knows what I go through sometimes and how I feel the way I do” (KH: Family). This quality of shared experiences was central in the descriptions of key helping relationships among many study participants. It suggests that shared experiences and/or perceived similar backgrounds may heighten the helper’s ability to show empathy and/or their ability to provide support in more meaningful ways to FSY with mental health challenges.
Conversation matters
Some of the descriptions of key helping relationships highlighted conversations about meaningful topics, including talking about mental health challenges. These participants’ narratives indicate that they engaged in authentic dialogues with their key helpers. This is noteworthy in light of the fact that the great majority of young adults in this study had been through significant emotional struggles, had been depressed, abused and/or neglected, and struggled with trusting others. Such experiences can close individuals off from revealing their inner emotions; however, these young adults valued talking honestly with their key helpers: I don’t like things sugarcoated or I don’t like things swept under the rug . . . I like that she’s really honest. I like that she didn’t hold back about me wanting to go to <another state> . . . It was “If I was your counselor, I would tell you to go” . . . Be honest. I want to know, so that means a lot to me ’cause I’ve had a lot of liars in my life. (KH: Professional)
Young adults also discussed meaningful conversations and sharing opinions on topics important to them, such as Black history: “My Black History project, I worked with her on it. We read the books together. We wrote down our opinions about stuff and we put them together . . . She helps me. She tutors me . . .” (KH: Professional). As this example shows, in some cases, key helping relationships involved learning together.
Mutuality
Mutuality came up repeatedly in the interviews and may become increasingly important as youth become young adults. Young adults stressed the importance of these relationships “going both ways” and described both mutual sharing and giving back to key helpers in myriad ways.
One FSY shared how mutual help contributed to her capacity to conquer significant loss: “I helped him with his grandmother’s death. He helped me with my grandmother’s death . . . we conquered together. So that’s one of the key things. Like whatever, I felt like it’s me and him against the world” (KH: Significant other). While the key helper above is a significant other, mutual help was present in different types of key helping relationships as well. As one participant said, Because I know I want to do good for him too, though. Sometimes he gets thrown off track more than I do. Like he attention seeks more than I do, so that way I want to be a support system, like do more, so if he ever needs anything he could always come to me and then I won’t have to struggle even helping him out too. That’s what I want to do. (KH: Family)
Finally, in response to the question, “how do you think she feels about you?” another participant illustrated mutual helping in both positive and negative experiences: the same exact way, ’cause she knows I’m coming. I’m coming. If anybody do you wrong, I’m coming. Anybody do you right, I’m coming. Like she was telling me about her ex-boyfriend . . . She’s like “Yeah, if he told me he wants to get married right now, I’d be like yeah . . . Well what part am I playing in the wedding?” (KH: Godmother)
Mutual helping in this case involved “coming” (showing up to help) if somebody does her godmother wrong or wants to marry her godmother.
Some participants also described how they believed that the relationship had a positive impact on both them and their key helpers. One talked about how she and her key helper strived to keep moving forward together and stay positive: We both strive to be positive through it all . . . ’cause when one is a little bit lower, the other one might be a little bit higher, and so we try to pull each other up, Well it’s not so bad . . . we try to keep each other on this positive outlook, as opposed to letting each other just kind of spiral down . . . (KH: Friend)
Another shared about how she thought she had helped her key helper see her own life from a different perspective: “I don’t know, helped her look at things differently. That’s what I get from people that they look at things differently after talking to me. So maybe that helped” (KH: Professional).
Mutual sharing was one of the most frequently coded aspects of these relationships. Mutual sharing helped young adults feel connected to their key helpers and also less alone in the challenges they faced, which mattered greatly to them. As one participant said, She shares some of her own personal experiences, and not just things that are like, “Well you know, this happened to me and I overcame it by doing this,” but she’ll share “Well you know my mother-in-law did this and it really pissed me off,” and . . . stuff like that, and “The baby did this and I was scared out of my mind,” and . . . real experiences that aren’t just you know happy ending stories. They’re . . . you know real life “Other people feel this way” stories. (KH: Professional)
Mutual sharing helped participants realize that key helpers are “real” human beings with problems too. “I was like it just made me realize that she’s a real person and she grieves too” (KH: Professional). It is important to note that mutual sharing did not always lead to positive outcomes; for example, in describing her sibling, one young adult states, “. . . sometimes her experiences kind of bring me down. So I guess that would be kind of negative” (KH: Family). Many of the relationships discussed in the present study, including those with professionals, possessed mutuality. However, at times, these experiences of being burdened by the shared experiences of key helpers appeared to be far outweighed by the benefits of engaging in mutually beneficial supportive relationships.
Acceptance
These young adults described how meaningful it was to them that their key helpers accepted them for who they were and offered unconditional positive regard, even in the face of their mental health histories. For example, one participant revealed that even when she was scared and faltered in her trust of her therapist’s acceptance she did feel some acceptance from her: “I can be myself around her more than most people, but sometimes I get scared that she’s going to get mad at me, so I can’t be myself then” (KH: Therapist). Another example reveals the connection between understanding and accepting: “he knows that like I understand him and why he does the things he does, like and I accept him for who he is” (KH: Family). The battle for acceptance of self is common among young people with mental illnesses (Kranke, Floersch, Kranke, & Munson, 2011), and having a relationship with someone who provides a feeling of acceptance and unconditional positive regard can be critical to healing.
Nature of the support
The relationships discussed offered participants various types of social support, including emotional, tangible, and informational support to them in their life more generally and also specifically related to their mental health challenges. In contrast to the relationship qualities described above, in this section the specific forms of support provided by key helpers are detailed. The nature of the support provided varied greatly, with some relationships providing more advice, others more tangible help, still others largely emotional support, and some providing all of these. As expected, based on the definition of a “key helper” in this study, a lot of support was discussed with respect to living with mental health challenges.
Emotional support
Many forms of emotional support were discussed by these participants. Particularly valued were messages of encouragement and acceptance and assistance with symptom management.
Encouragement
One young adult described how encouragement from her key helper motivated her to accomplish her goals. She said that her key helper would say things such as, “I know you could do it. Why are you always saying you can’t do it? You could do it” and went on to add that, “At the end of the day I always come out and I do it, because just her and her words, it just makes me just really want to go out and accomplish, which because it be powerful to me” (KH: Professional).
This kind of encouragement seemed to be especially helpful to some of these participants as they were making the transition to adulthood. Hearing their key helpers express their faith in them and in their abilities helped some to see themselves as having the capacity to do something positive and productive with their lives. As one participant said, She helped me with my writing, and she gave me confidence, ’cause like I’m good, so sometimes people, I guess they don’t want to tell me how good I am, don’t want to give you that power, but she would tell me like “This is good. This is really good,” and it just let me know . . . Okay, I do have something to offer the world. I have something besides selling drugs. So just she just helped me deal with reality pretty much. (KH: Friend)
Symptom management
Of particular importance to these participants were the ways that the emotional support provided by key helpers assisted them with the management of symptoms associated with their mental health challenges. The calming presence of key helpers and the listening ear they offered were noted by approximately half of the young adults. As one participant said about the way their key helper listened, “It’s just something about her that calms me down. I don’t know what it is” (KH: Significant other). Another young adult described this process in detail: When I tick, tick boom, she don’t tick, tick, boom . . . Like if I’m flipping out, she doesn’t join in and adds fuel to the fire. She actually says “Okay <Participant>, listen. Chill out. I’m hanging up.” She’ll tell me, and then I can be yelling at her on the phone and she’s “I’m hanging up now,” and then she’ll hang up on me for real, too, and then I’ll call her back like “Why you hang up on me?” “Because I told you I was going to hang up on you if you didn’t calm down,” and then it slowly calms me down. (KH: Friend)
Another participant spoke about how a key helper’s listening ear helped her refrain from yelling, screaming, and behaving destructively: I used to do stuff, go in the store and kick stuff over and just keep walking out like I didn’t see it, but I don’t do that no more. I just, I got like a normal person. In the movie, or riding, and if I feel down or feel like somebody’s watching me, I could tell her, you know “This is how I’m feeling right now” and she understands. (KH: Family)
Finally, key helpers were there for the young adults when they experienced serious episodes of mental illness: When my real mom called the Police on me and said I cut myself and the Police came to my house and took me. So they wouldn’t let me leave the hospital, so I called her on my cell phone. She came up there and she sat with me the whole time. She’s been there the whole time anyway. (KH: Family)
Others spoke about reductions in symptoms such as anger, sadness, and isolation, along with an increase in the ability to identify triggers, which they attributed in part to the emotional support these relationships provided them.
Informational support/advice
Participants also described receiving information and advice from their key helpers in a variety of important arenas, including finances and interpersonal relationships. One participant notes that her key helper influenced her financial decision making by encouraging her to think more carefully and intentionally about how she spent her money: She’ll talk me out of it, like “Girl, don’t do that. You know you got to pay your rent first. Think about having somewhere to stay. Them shoes ain’t good.” She talks me out of doing stuff that I be wanting to do a lot. (KH: Family)
Another talked about how her key helper encouraged her to think about money in new ways: “Growing up I really wasn’t money-oriented. I would just blow money . . . Just telling me like ‘Don’t blow your money. You’ve got to save your money’” (KH: Friend). Participants also described receiving advice from their key helpers regarding their important relationships. Key helpers were said to have encouraged participants to avoid relationships with individuals who could trigger their mental health symptoms or otherwise lead them in the wrong directions: I used to get mad and frustrated . . . I haven’t found that right girl yet, and you know I’ve been telling my grandmother . . . She’s been looking at all these guys who wear the pants sagging and stuff like that and she says, “You know what, son? You don’t have to be like that. You know if they want the gang-banging brothers who ain’t got nothing going for themselves, let them have them, because God will bless you with that person, put that person in your life.” (KH: Family)
Participants also stated that key helpers encouraged them to carefully select mental health professionals who will listen and spend time with them during their appointments. They also provided advice on mental health treatment, for example, the importance of getting evaluated, completing their program, and utilizing (or not utilizing) mental health services. Key helpers also gave spiritual advice related to mental illness and gave advice on how to cope with symptoms. Advice on coping was discussed in a variety of ways, such as meditation, taking walks, drawing, and using tools to manage anxiety and stress (i.e., hit a pillow, squeeze a stress ball). One participant described how the key helper encouraged self-talk as a way to cope: She’s like “Just talk to yourself, ’cause you know you . . . You know you, so if you feel like talking to yourself, and if yourself can help you, help it. Just help it. Breathe. Take a deep breath. Just if you got to squeeze something, squeeze something. If you’ve got to tap something, or talk on the phone, Like ‘Cope with it. Don’t just flip; cope with it. Find little methods,’” and I find little methods. (KH: Professional)
In these exchanges, the honesty of the key helpers was greatly appreciated by the young adults, even when the advice was difficult to hear: “She tells me what I need to hear. I mean it might not always be what I want to hear, but it’s what I need to hear” (KH: Friend).
Instrumental support
These young adults also identified times when their key helpers directly assisted them by providing them with some tangible necessity. One participant described the help received when first moving out on her own: The thing that’s most helpful about my mom is because when I first moved out . . . she bought me . . . groceries and everything . . . bedspreads, clothes, shoes. You know she’s not how they make out most foster parents to be, like she’s only in it for the money. (KH: Former foster mother)
Many participants noted that their key helpers provided them with a place to say when they needed it, even with food at times: “I had no food in my house when I lived on <street> and she came out just to give me food” (KH: Family) and also with child care: “If I’m tired, she always, always there to help out. Like if the baby might need a bottle wash and I’d been busy all day, she’ll help me” (KH: Family).
Critical help navigating the bureaucracies these young adults needed to interact with was also provided. Participants described how key helpers had helped them access services and benefits (e.g., Social Security Disability Insurance)) and higher levels of treatment, such as hospitalization when needed: “Like when I went to the mental hospital and I was so mad at her for like putting me in there, she kind of you know supported me that way. She came to see me” (KH: Professional). Key helpers also assisted FSY with obtaining their medications: “or if I’m out of medicine, then they get me more” (KH: Professional) and accompanied them to appointments.
Discussion
The present study provides detailed and contextualized examples of 45 supportive relationships between FSY with mental health challenges and nominated key helpers that they perceived supported them during the transition to adulthood. Key helpers in this study were both informal and formal helpers. Participants stressed the value of consistency, mutuality, empathy, acceptance, and “feeling cared for, connected, and loved” in key helping relationships. Also, specific forms of emotional, informational, and instrumental support were identified as being valuable, including encouragement, advice about relationships and mental health services, help with symptom management, and assistance with temporary housing, food, and child care when needed. Figure 2, which is based on Rhodes’s model (see Figure 1), explicates specific ways the more general processes outlined in Rhodes’s model played out in these key helping relationships.
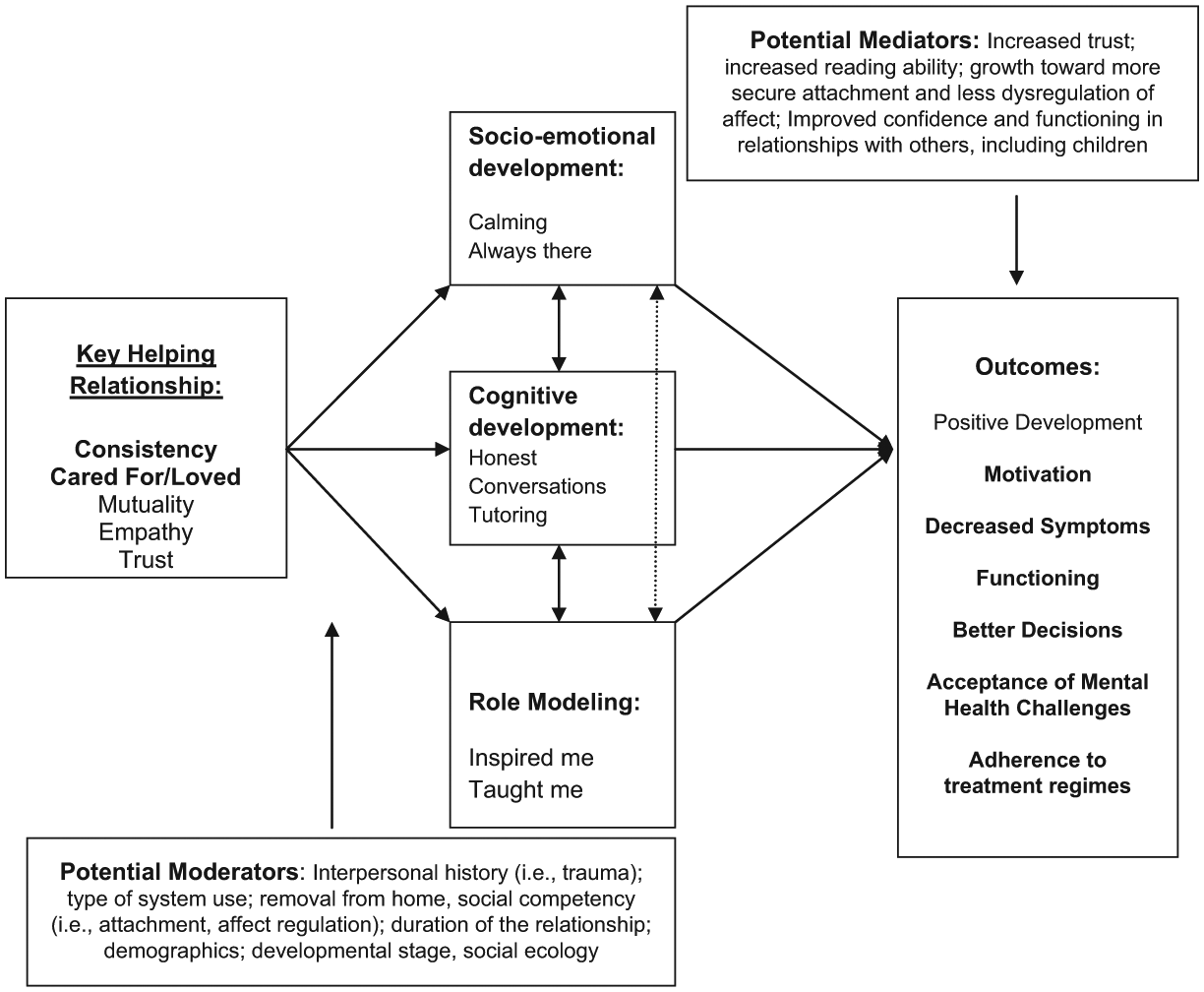
Supportive relationships between former system youth and key helpers.
In addition to mutuality, trust, and empathy, these participants emphasized the importance of consistency in their supportive relationships and especially consistency over extended periods of time and through major life transitions. Such consistency in relationships is something that these FSY find hard to obtain, making the support their key helpers provided especially meaningful. This consistency also appeared to contribute to participants developing a sense of trust in their key helpers, a dimension of relationships that can also be all too rare among FSY (i.e., Sparks, 2004). Histories of maltreatment and high levels of transience may work against consistency and can erode trust, and maltreatment has been found to be strongly associated with insecure attachments (Marganska et al., 2013). Such relational experiences can make it challenging for FSY to trust themselves and others, and thus make it difficult to effectively engage in and maintain relationships (Karen, 1994). Being removed from home, and/or another placement(s), which is common for system youth, can also further contribute to early insecure attachments (Troutman, Ryan, & Cardi, 2006). Supportive relationships with key helpers, in contrast, may provide a safe connection within which FSY youth may reappraise and restructure their representational models of self and others. The findings here indicate that the fostering of these kinds of “corrective emotional experiences” that Rhodes (2002) has posited can occur in mentoring relationships and may depend on a high level of consistency on the part of the key helper and the larger program the relationship develops within. Adding to the significance of this finding in the present study, consistency and availability has been reported in other recent studies on the qualities of supportive relationships among youth transitioning from foster care. For example, Collins et al. (2010) identified aspects of consistency (i.e., constant encouragement, reliability) and availability (i.e., provide assistance when needed) as important in the relationships they studied. Although the young adults in our study were older, specifically 18 to 25, they were still expressing a central need for consistency. Together, these studies strongly suggest a need to develop programs that can provide consistent supports to young adults, bolster the consistency of already existing natural supports, and/or help young adults identify and invest in relationships that have the features that undergird consistency. A specific aspect of consistency that was present in our data was being there during crisis situations or situations when mental health symptoms emerge. This suggests a need to assist supportive key helpers in preparing to address crises that come up for these FSY with mental health challenges. For formal helpers, this finding calls for continued training in crisis management and support, and for informal helpers it suggests a critical element of training on crisis management for any program model initiating new or supporting already existing supportive relationships with important natural supports or informal helpers.
Furthermore, the results of this study point to the desire FSY have to be in relationships that possess mutuality. Young adults described the importance of “giving back” to their identified key helpers in some way. It is important to note that professionals and informal key helpers were reported to engage mutually in these relationships, which was a key facet to the relationships being effective from the perspective of the FSY. The study participants indicated that a more bidirectional relationship helped them to feel normal, purposeful, and good about themselves. This is in keeping with other research on naturally occurring mentoring relationships among transitioning youth (Liang, Spencer, Brogan, & Corral, 2008). This is developmentally significant for professionals designing mentoring programs for young adults. Training modules and specific activities should offer healthy opportunities for young adults to be able to provide something for, or give back to those who help them, in ways that are both meaningful and ethical, particularly when considering professional helpers. Indeed, mutuality has been discussed in studies of youth (i.e., Munson et al., 2010), but the amount of data in this study on mutuality suggests that this quality becomes increasingly salient when providing relational interventions to those in early adulthood. It is important to note that mutuality was discussed in relationships with both informal and formal supporters. This finding is important to remind the mental health field that great care should be taken when attempting to facilitate a supportive relationship that is clinically healthy and healing for FSY with mental health challenges and consideration should be given to how, when, and in what ways to introduce appropriate and safe experiences of mutuality in the helping relationship. While some types of mutuality can go against traditional training for mental health professionals (Lazurus & Zur, 2002), an emerging clinical theory, relational-cultural theory (Miller & Stiver, 1997), can inform the fields on strategies of using mutuality in clinically relevant and ethical ways for growth in connection.
Finally, thinking broadly about the results through the lens of Rhodes’s (2002) model of youth mentoring, the present study offers some specificity on the underlying mechanisms of supportive relationships for FSY with mental health challenges (see Figure 2). Our data suggest that the majority of FSY are in need of, and yearning for, healthy socio-emotional connections. Young adults’ descriptions of key helpers that mattered to them were characterized as caring, emotionally close, consistent, and available. These data indicate that having someone who is there for FSY emotionally, encouraging them, and “showing up for them” helped these young adults feel connected and more motivated to pursue their goals and adhere to their treatment regimens as they made their way into adulthood, carrying difficult pasts and often children and families of their own.
Our data also suggest that some young adults valued supportive relationships for the chance to have someone to talk to, learn from, and engage in meaningful conversation with about important topics. Having someone listen to was repeatedly noted as well, suggesting that there is also a cognitive dimension to key helping relationships. Young people talked about some of their key helpers, often those who were professionals, as helping them see their worth and as promoting positive self-talk that in turn served to help them manage their difficult symptoms and negative thoughts about themselves. This appeared to help them see their own potential.
Finally, in some cases, young adults discussed the importance of shared experiences and of key helpers showing them how to do things or making suggestions on parenting, coping with their health challenges, and managing young adult tasks (i.e., finances). In these empirical data elements, it becomes clear that young adults are looking for role models—individuals that they trust that can provide a positive example for them as to how to be a productive adult, and further a productive adult with a mental health condition. In both our study as well as a similar study by Ahrens et al. (2011), it has become clear that taking time and showing young adults that some adults can be trusted is critical. It takes time to rebuild trust in relationships, and these factors must be considered when designing programs for FSY. These young people have often experienced very painful relational pasts, which include significant violations of trust, and these factors must be considered in program design and implementation.
Although only a start, these data add to the findings from previous studies regarding the specific relational needs of FSY and suggest that the relational needs of FSY with mental health challenges may be similar to those of youth transitioning out of foster care (Ahrens et al., 2011). More research examining the dimensions of relationships that do exist is essential for developing social service programs that are tailored to meet the unique needs of sub-groups of FSY.
Last, data on types of support provided by key helpers is extensive and spans both basic needs, such as food and shelter, and mental health needs. In these data, family key helpers were noticeably providing the general tangible and informational support, with professionals more often providing the support related to mental health. Interestingly though, with regard to emotional support, all types of supports were providing both general and mental health–related emotional support. This is important to understand in more detail. The findings here can inform the efforts of social services as they develop alternate avenues to reach young adults who are vulnerable and make every effort to connect with them, provide various forms of support, and encourage them to seek professional help as needed.
Conclusion and Implications
Developmentally, young adults are in the midst of innumerable changes, including changes in their relationships. Data from this study suggest that the transition to adulthood is a time when FSY are counting on supportive relationships with key helpers to provide important functions in their lives. The present study is one of only a few qualitative examinations of the relational lives of young adults with mental health and social service histories. There is a dearth of research on the relational lives of FSY with mental illness who are arguably distinct from adolescents and adults with mental health challenges in important ways. For example, when compared with adolescents, these FSY are increasingly becoming the decision makers in their lives. Furthermore, caregivers often will have less influence on their decisions as the important adults of their own choosing become more influential. And, compared with more mature adults, FSY are less likely to have moved into relationship commitments and routines about how they will engage in relationships in their adult lives. Thus, understanding the qualities and needed supports specific to young adults is paramount to best help them make a successful transition, including a successful transition to mental health services if needed.
This study examines the supportive relationships between FSY with mental health histories and their nominated key helpers through the lens of both social support and Rhodes’s (2002) model of youth mentoring. The field of mentoring, and social support more generally, can benefit from studies such as this one that specifies the types of relational supports and the qualities of relational supports that are valued by specific sub-groups of young people.
These findings suggest important practice considerations. First, it is clear that developing program structures and processes that will allow for the greatest amount of consistency must be paramount. Strategies must keep in mind the transience many of these young adults have experienced and make every attempt to provide services that embed consistency at every level, for example, providing consistency of the person (i.e., key helper), the place (or setting of the program), and the community (Munson, 2013). Furthermore, when considering relational interventions for this population, training must include detailed lessons on their relational needs and steps for addressing crises if they occur. Studies such as this one can inform training modules for mentoring programs designed for youth and young adults with mental health challenges involved with or aging out of public systems of care (Munson, 2013). A potential feasible strategy is to incorporate key helpers, both informal and formal, into programs delivered at mental health clinics. This would further support assisting if crisis situations were to emerge.
In addition, these data can inform the development of an assessment tool for youth and young adults recruited for mentor-type programs to help understand more about what type of relational support they need (i.e., role modeling, tutoring, attachment), what type of qualities program staff should look for in a potential mentor match (i.e., patience, shared experience of parenting), and what type of training modules can be helpful in preparing to support the match.
It is also important to note that while approximately 25% of participants named a professional as a key helper, 75% identified family or friends. While recognizing that adults with mental health issues often need professional services, it appears that assisting them in identifying, enhancing, and maintaining natural supports within their environments is also an important goal. Recent research has investigated a new strategy, called youth initiated mentoring (YIM), which calls on natural supports to provide more support (Schwartz, Rhodes, Spencer, & Grossman, 2013; Spencer, Tugenberg, Ocean, Schwartz, & Rhodes, 2013). YIM encourages young people to reach out and ask their potential natural supports to engage with them more and be in a relationship with them as a mentor. This strategy could be applied among young adults with mental health conditions.
The present research, of course, has limitations that must be kept in mind when interpreting the results. First, the study purposively sampled young adults from one midwestern state with a specific set of experiences, and while qualitative inquiry is not designed to be generalizable, one must exert caution relative to the limited sampling that was used. Second, a limitation discussed by leaders in the field of understanding the transition to adulthood among vulnerable populations is the heterogeneity of experiences among each sub-group of young people in transition. Our sample is indeed a group of young adults with mood and emotional difficulties that have experienced varying constellations of public system service use during childhood. Third, qualitative research is subject to the limitation of investigator biases in the process of coding and identifying themes. All analysts have had clinical training and have worked directly with individuals similar to the respondents. Biases were limited by using multiple coders and using the participant’s words as much as possible. Limitations notwithstanding, the data advance the discussion on how supportive relationships identified by FSY with mental health challenges can help facilitate a more successful transition to adulthood.
Footnotes
Acknowledgements
The authors would like to thank both New York University and Case Western Reserve University for their institutional support during the preparation of this article. We would also like to especially thank the young adults who participated in this study. Finally, we would like to thank the Ohio Department of Mental Health.
Authors’ Note
The authors Michelle R. Munson and Suzanne Brown participated equally in the development of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support was provided through a research grant to Dr. Munson from the Ohio Department of Mental Health 09.1240.