
Abstract
This study assessed mental health literacy in Irish adolescents (N = 187), and explored participants’ help-giving responses toward hypothetical depressed peers. Participants read five vignettes, each describing an adolescent experiencing a life difficulty; two of the characters met Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV) criteria for depression. The majority of participants could not identify depression or potential suicidality, but felt concerned for the depressed characters’ well-being. Most participants stated they would provide help if they were the depressed characters’ friends. Correct identification of depression did not influence the type of help offered. A significant proportion of participants did not mention engaging an adult’s assistance, and assessing for suicidality was not mentioned by any participant. Gender differences were found in mental health literacy and the type of responses offered. Education that emphasizes the importance of informing an adult and assessing for suicidal risk is recommended.
Young people’s mental health is a worldwide issue of acute concern. In a review of international research, Patel, Flisher, Hetrick, and McGorry (2007) estimated that approximately 20% of young people will experience at least one mental disorder in any given year. The adolescent period, in particular, is associated with a marked increase in the onset of mental disorders (Kelly, Jorm, & Wright, 2007). Depression is particularly concerning due to the link with suicide (Burns & Rapee, 2006). Suicide has been reported as the third leading cause of mortality in young people worldwide in the Global Burden of Disease Study (Patton, 2011), and Ireland has the fourth highest rate of youth suicide in Europe (National Educational Psychological Service, 2013). Overall, the picture is that approximately one in five adolescents suffers from clinically significant emotional distress, and the suicide risk among adolescents is high. Despite this, the majority of young people in distress are not seeking support from formal mental health services (Dooley & Fitzgerald, 2012).
Enhanced understanding of the pathways toward adolescents’ help seeking would help close this treatment gap. Help seeking is affected by several factors, including the young person’s knowledge of the symptoms of mental disorders, of appropriate avenues of support, and of treatment options (Cotton, Wright, Harris, Jorm, & McGorry, 2006). The concept of mental health literacy encapsulates this type of knowledge. The present study is concerned with understanding mental health literacy in Irish adolescents, and how they respond to peers with mental health difficulties.
Mental Health Literacy
Mental health literacy is defined as “knowledge and beliefs about mental disorders which aid their recognition, management, or prevention” (Jorm et al., 1997, p. 182), and includes knowledge and attitudes about appropriate sources of help (Jorm, 2000). Mental health literacy in the general population could lead to more positive and supportive interactions with individuals with mental disorders, which is important as the probability of close contact with an individual with a mental disorder is very high (Jorm, Morgan, & Wright, 2008). These interactions could have a significant impact on these individuals’ pathways toward receiving help. This is especially true of young people who are in need of mental health support for the first time.
Mental health literacy in members of an individual’s social network is a crucial component of the Gateway Provider Model (GPM; Stiffman, Pescosolido, & Cabassa, 2004), a conceptual lens through which help-giving processes can be viewed. This model posits that “gatekeepers,” such as friends and family members, often connect individuals with mental health services, as changes in a person’s functioning related to the development of a mental disorder are likely to be apparent to friends and others in their social network before professional help is sought (Jorm et al., 2008; Kelly et al., 2007; Lawlor et al., 2008). Mental health literacy research corroborates the GPM, as Stiffman et al. (2000) found that the gatekeepers’ assessment of the severity of the problem was the strongest predictor of recommendations for youth mental health services. In the GPM, the recognition of symptoms and endorsement of seeking help by peers are likely to significantly increase engagement with appropriate supports for young people with mental health difficulties.
The ability of an individual’s friends and family to identify appropriate professional help is particularly significant given that professional help is not a well-utilized source of help for young people. Access to mental health services in the Irish public healthcare system typically is initiated through a visit to a general practitioner (GP), and GPs have been named by young people as a primary source of formal help (e.g., UNICEF Ireland, 2011). However, research has shown that less than one fifth of adolescents with mental health difficulties access a GP service (e.g., Dooley & Fitzgerald, 2012). Given that young people name concerns about confidentiality as a prominent barrier to service use (e.g., Gulliver, Griffiths, & Christensen, 2010), the fact that caregivers of Irish adolescents under 16 years must be informed of any mental health treatment from a GP is problematic. The cost of a GP visit may also place a further burden on adolescents. However, the Irish public healthcare system is supported by some organizations that offer free services for young people (e.g., Headstrong: The National Centre for Youth Mental Health). Some young people can access support from a school counselor, but specialized school counselors are not present in most secondary schools. These barriers to service use, together with adolescents’ reluctance to engage with formal sources of support, reemphasize the importance of mental health literacy in the young person’s social network, of which peers are an important subgroup.
Peer Support
Jorm, Wright, and Morgan (2007) discuss how “in many ways it is unreasonable to expect adolescents to have the knowledge and skills to support peers” (Jorm et al., 2007, p. 69). Despite these concerns, research has consistently shown that while many depressed and suicidal adolescents are unlikely to seek help from any source, those who do seek help prefer peer support (Chambers & Murphy, 2011; Sullivan, Arensman, Keeley, Corcoran, & Perry, 2004). Furthermore, individuals suffering from depression are more likely to seek professional help upon recommendation (Vogel, Wade, Wester, Larson, & Hackler, 2007), and the fear of negative reactions from peers is a common reason given for not seeking help (Barney, Griffiths, Jorm, & Christensen, 2006). Particularly in late adolescence, young people are more likely to turn to peers than family as a source of information and support (e.g., Bokhorst, Sumter, & Westenburg, 2010; Swords, Hennessy, & Heary, 2011). Adolescents are also in a unique position to observe changes in their peers’ behavior before these changes may be noticeable to adults (Olsson & Kennedy, 2010).
Adolescents’ perspectives on their ability to help peers are extremely positive. The majority of adolescents report that they have a good understanding of how to help a friend going through a tough time (Chambers & Murphy, 2011). Adolescents are more confident in their ability to provide help to peers than are young adults, and girls are more confident than boys (Jorm et al., 2007). However, adolescents’ ratings of their help-giving abilities may not be reflective of the efficacy of this help. In one study, only 23% of adolescents stated that they would engage an adult’s support, and 20% named violence or recreational drug use as helpful measures to deal with mental health difficulties (Kelly, Jorm, & Rodgers, 2006). The current study extends our understanding of the types of support adolescents offer to their peers, which has not yet been adequately explored in an Irish context.
Sex Differences
Although sex differences in mental health literacy are given little attention in the literature, the limited research available has consistently suggested such differences exist. A large-scale Irish study recently found that female participants scored up to 20% higher than males on measures of mental health literacy (Chambers & Murphy, 2011). Lawlor et al. (2008) found that young Irish females were significantly more likely than males to recognize depression in a vignette; this pattern of results was corroborated by Cotton et al. (2006) with a sample of Australian young people. Adolescent girls have reported knowledge of a wider range of mental disorders than boys, and boys have been shown to be significantly less likely to believe that recovery from mental disorders is possible (Williams & Pow, 2007). The present study seeks to contribute to this limited body of research, by examining sex differences in both mental health literacy and help-giving responses.
The Study Purpose
The aim of the current study was to assess the mental health literacy of a sample of Irish adolescents, specifically in relation to their knowledge of depression. This study also explored the help-giving responses of adolescents toward their depressed peers. Sex differences in mental health literacy and help-giving responses were investigated.
This study focused on young people in late adolescence, as a decrease in utilization of mental health services among older adolescents has been found in previous studies (Leighton, 2010). The incidence of depressive disorders in adolescence has also been shown to increase with age (Health Service Executive, 2011; Thapar, Collishaw, Pine, & Thapar, 2012), and young people in late adolescence have been shown to prefer peer support (Bokhorst et al., 2010). Sex differences were explored, as previous research has suggested that adolescent girls and boys differ in their knowledge of mental disorders (Chambers & Murphy, 2011).
Vignettes were used, which require participants “to articulate their own beliefs and knowledge, [providing] an alternate method to investigate mental health literacy that taps more directly into declarative knowledge” (Burns & Rapee, 2006, p. 227). The use of vignettes has been effective for the exploration of sensitive topics and adolescents’ subjective definitions (Barter & Renold, 2000). Studies have suggested that responses to vignettes are very similar to those in real-life situations, and that the social desirability bias is reduced in comparison with direct questioning (Leighton, 2010). This study adapted vignettes developed by Burns and Rapee (2006) in order to render them suitable for use with an Irish population. Mixed methods were used in the form of a series of closed- and open-ended questions following each vignette, in order to address the following research questions: What knowledge of mental disorders, depression in particular, do Irish adolescents possess? What types of help-giving responses are offered to a peer suffering from mental health difficulties, and why is this help offered? If help is not offered, what are the reasons for this? Are there sex differences in this knowledge and these responses?
Method
Design
The current study is a quasi-experimental within-subjects design. The quasi-experimental variable is sex and the within-subjects variable is vignette type (depressed/non-depressed). All participants read the same vignettes before mixed-method questioning was used to assess their knowledge and beliefs. The sample was later disaggregated by sex.
Participants
Participants were recruited through purposive sampling of three secondary schools in rural counties Wicklow and Carlow in the Republic of Ireland. Approximately 400 students were provided with information sheets regarding the study, of which 187 consented to participate (47% response rate). There were 96 (51.34%) girls and 91 (48.66%) boys. Of these students, 61 (32.62%) were in fourth year, 66 (35.29%) were in fifth year, and 60 (32.09%) were in sixth year (final year of secondary school). The mean age for the sample was 17.04 years (SD = 0.949), while age ranged from 15 to 19 years. Data on participants’ ethnicity were not collected. However, the majority (over 87%) of the population in this region is White Irish (Central Statistics Office, 2012). Socioeconomic status was measured using the proxy variable of mothers’ and fathers’ highest level of education completed to date. The majority (61.7% of mothers and 61.7% of fathers) had completed second-level education (i.e., high school) or less, 22.3% of mothers and 21.3% of fathers continued their education to complete a (third-level) diploma or certificate, and 11.7% of mothers and 6.9% of fathers had completed a bachelor’s degree or higher.
Materials
An adapted version of the Burns and Rapee (2006) vignettes was utilized. Minor adaptations were made to the vignettes, to facilitate their use in an Irish setting. For example, girls’ and boys’ names were changed to common names used in Ireland, and names of school years were changed to reflect the Irish educational system. A pilot study was conducted to ensure the amended vignettes retained their comprehensibility. A clinical psychologist working in Child and Adolescent Mental Health Services also reviewed the amended vignettes, with no suggested changes.
There were five vignettes in total. Each described a young person going through a life difficulty. Three of the five vignette characters were dealing with normal life crises such as breaking up with a boyfriend, the death of a grandparent, and being caught drinking alcohol by a parent. The other two characters, Tony and Emily, displayed five of the nine Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV; American Psychiatric Association, 1994) symptoms of depression. Each vignette was followed by a series of nine questions. The first six questions were taken from the original Friend in Need Questionnaire developed by Burns and Rapee (2006). The additional three questions were developed for the current research, in order to assess help-giving behavior. Tony and Emily’s vignettes, together with the questions and response options, can be seen in the appendix.
Procedure
Following receipt of ethical approval, three secondary schools were recruited for participation in the study. Information sheets and consent forms were distributed to all potential participants in each school, and their parents. Consent forms included demographic questions regarding the age, sex, and school year of the participant, and parents’ highest level of education. Testing took place in schools during school hours. A webpage hosting the questionnaire was loaded onto school computers, and participants progressed through the vignettes and their accompanying questions online at their own pace. The average length of time for completion was 20 minutes. There were no incentives provided to students for their participation.
Statistical Analyses
Data were exported from the online survey tool to IBM Statistical Package for the Social Sciences (SPSS). Descriptive and frequencies analyses were performed, followed by analyses of variance (ANOVA) and chi-square analyses.
Results
Can Adolescents Label a Cluster of Symptoms in a Peer as “Depression?”
Participants explained in five words or less what they “think is the matter” with each vignette character. Three of the characters, Aoife, Sinéad, and James, were going through transient life crises (a break-up, being caught drinking alcohol by a parent, and the death of a grandparent, respectively). The other two characters, Tony and Emily, each displayed five of the nine DSM-IV symptoms of major depression; in Tony’s story, these symptoms are described in a meeting between his mother and his Year Head in school, and Emily’s symptoms become evident through interactions with a friend. Responses were coded as per the guidelines proposed by Burns and Rapee (2006): If the words “depressed/depression” or “suicide/suicidal” were present, the response was coded “Depressed.” In their absence, the response was coded “Non-Depressed.”
Over half (51.34%) of participants labeled Emily as “Depressed,” with no significant sex difference in responses, χ2(1, N = 187) = 3.383, p > .05. As Emily’s vignette made reference to suicidal ideation, responses were additionally coded solely for the presence of the word “suicidal” or a direct reference to suicide (e.g., “Going to kill herself,” “wants to die”). A small minority (9%) of participants identified Emily as suicidal, with no significant sex differences in responses, χ2(1, N = 187) = 0.773, p > .05. Almost a third (32.62%) of participants labeled Tony as “Depressed”; similarly, there was no significant difference in responses across the sexes, χ2(1, N = 187) = 0.276, p > .05. For the other three vignette characters, 8.02% labeled Aoife as “Depressed,” 3.74% labeled James “Depressed,” and no participants labeled Sinéad “Depressed.”
Do Adolescents Express Greater Concern for Peers Showing Signs of Depression Than for Peers Showing No Signs of Depression?
Participants expressed their level of concern about each character’s emotional well-being on a 4-point scale, ranging from 1 (not at all worried) to 4 (extremely worried). Each participant’s mean scores for the two depressed vignettes and the three non-depressed vignettes were calculated, and the differences between levels of concern shown for each group were examined using a 2 (vignette type) by 2 (sex) mixed between–within subjects ANOVA. An interaction effect between these variables was observed, Wilks’s λ = 0.978, F(1, 41.11) = 4.216, p < .05,
Do Adolescents Perceive Longer Recovery Times for Peers With Depressive Symptoms?
Participants estimated the recovery time for each vignette character, using a 4-point scale from 1 (one or two days) to 4 (longer than a few months). Participants’ mean responses to the two depressed vignettes were computed as one variable and the three non-depressed vignettes as another variable. A 2 (vignette type) by 2 (sex) mixed between–within subjects ANOVA was conducted to assess differences between estimates of how long it would take depressed and non-depressed vignette characters to recover. There was no significant interaction between vignette type and sex, Wilks’s λ = 1.00, F(1, 43.02) = 0.019, p = .889,
What “Symptoms” Do Adolescents Identify as the Strongest Hints of Problems in Depressed Peers?
Five of the nine DSM-IV criteria for depression were clearly referenced in both Tony and Emily’s vignettes. Fatigue/loss of energy, insomnia, weight loss/decreased appetite, diminished ability to think/concentrate, and diminished interest in activities were referenced in Tony’s story. Emily’s story referenced diminished interest, fatigue/loss of energy, depressed mood (sad/tearful), feelings of worthlessness, and suicidal thoughts. Participants were asked “Which parts of X’s story are the strongest hints to you that she or he might be experiencing emotional difficulties?” Responses were coded by the presence of words quoting or related to the sections of the vignettes referencing these symptoms.
Tony’s insomnia was considered the strongest hint of emotional difficulties, with 42.8% of respondents agreeing that this was a strong indicator. This was followed by his weight loss and decreased appetite (41.7%), lack of interest in activities (38.0%), fatigue and constant tiredness (27.8%), and finally his inability to concentrate (26.2%). Girls were significantly more likely to list Tony’s weight loss as a symptom of emotional distress, χ2(2, N = 187) = 12.59, p < .01. For Emily, participants most frequently rated her expression of suicidal thoughts as a strong sign of emotional distress (72.7%), followed by her feelings of worthlessness (56.1%), her sad and tearful mood (26.2%), and finally her lack of interest (23.5%) and fatigue (23.5%). Girls were significantly more likely than boys to list Emily’s fatigue as a symptom of emotional distress, χ2(2, N = 187) = 10.54, p < .01.
From Whom Do Young People Recommend Their Depressed Peers Seek Help?
Participants were asked “Do you think X needs help from another person to cope with his or her problem?” There were significant differences between male and female responses. In Tony’s case, 99% of female participants and 89% of male participants answered “Yes” to this question, χ2(2, N = 187) = 8.986, p < .05. In response to Emily’s scenario, 90.6% of female participants and 83.5% of male participants answered “Yes,” χ2(2, N = 187) = 6.664, p < .05.
Those who answered “Yes” were asked to state potential sources of help. Responses to Tony and Emily’s depressed vignettes were analyzed, and six categories were coded: Mental Health Professional, Friends, Family, School, Doctor, and Someone in Similar Situation. Responses were coded for all sources of help mentioned; for example, if both “doctor” and “friend” were mentioned in one participant’s response, this response would be coded for both categories. Mental Health Professional was the most frequently stated category, with 65.8% of participants giving this response. About 54.5% mentioned friends, followed by family (53.5%), school (16.6%), a doctor (8.6%), and someone in a similar situation (3.7%). In all cases, the difference between male and female responses was not statistically significant.
Are Young People Willing to Help Their Depressed Peers Access the Support They Need?
Participants were asked, “If you were friends with X, would you help him or her to access this help?” In Tony’s case, 78.6% of participants answered “Yes.” There were significant sex differences; 88.5% of girls and 68.1% of boys would help Tony, χ2(2, N = 187) = 11.594, p < .05. Over 80% (81.8%) of participants answered “Yes” in response to Emily’s scenario. Over 90% (90.6%) of girls and 72.5% of boys would help Emily access the support she needs; again, this was a statistically significant difference, χ2(2, N = 187) = 10.735, p < .05.
How Do Young People Help Their Depressed Peers?
If participants answered “Yes” when asked if they would help their peer, they were asked to explain how they would provide help. The responses to this open-ended question regarding the two depressed vignette characters, Tony and Emily, were analyzed using conventional content analysis, according to the guidelines set out by Hsieh and Shannon (2005). Seven types of help-giving responses were categorized: cheering, comforting, and reassuring; perspective-taking; advice from similar experience; distraction; physical activities; engagement with adults; and multiple types of help. It is noteworthy that no participant mentioned assessing for suicidal risk as a potential response.
Chi-square analysis revealed significant sex differences in help-giving responses to both Tony’s vignette, χ2(7, N = 186) = 14.93, p < .05, and Emily’s vignette, χ2(6, N = 187) = 27.49, p < .001. These significant sex differences were found in responses in the “multiple” category for both Tony and Emily’s vignettes, and in the “engaging an adult’s help” category for Tony’s vignette only. Specifically, more girls than boys named multiple help-giving responses in relation to both Tony’s vignette (70.8% girls, 29.2% boys) and Emily’s vignette (85.7% girls, 14.3% boys). Of the participants who named engaging an adult to help Tony, 61.8% were girls and 38.2% were boys. Sample quotes from each category and the percentage of participants whose responses fell under this theme can be found in Table 1.
Responses Categories, Samples of Quotes Coded Under Each Category, and the Percentage of Participants Who Gave Such Responses to Both Tony and Emily’s Vignettes.
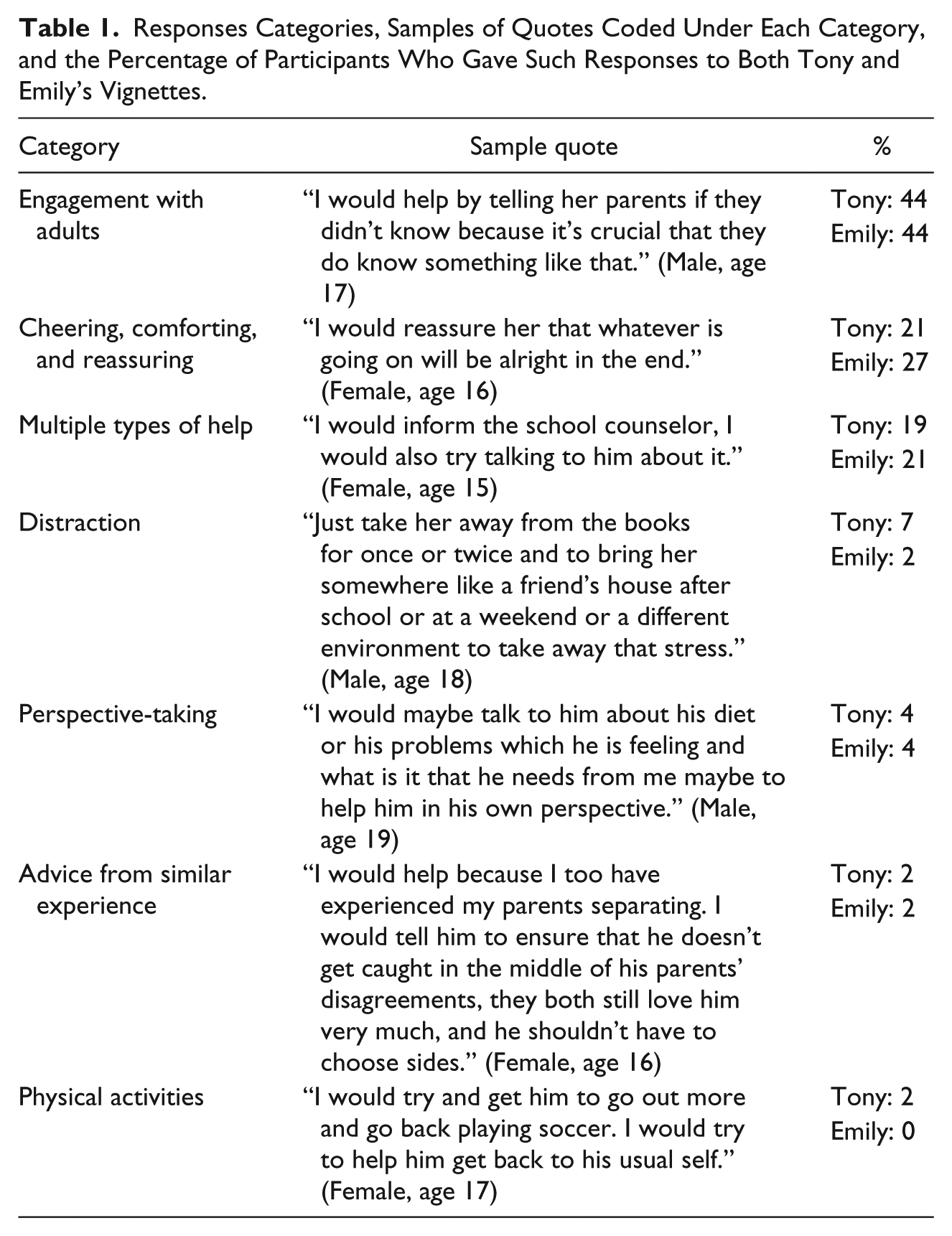
Further content analysis of participants’ responses was also conducted in order to assess the percentage of participants who discussed help-giving responses that involved solely the peer group, with no mention of engaging an adult’s help, and the percentage of participants who made some mention of adult help, either accessing both peer and adult help, or solely obtaining an adult’s help. In response to Tony’s vignette, 33.2% of participants’ help-giving responses involved the peer group only, and 66.8% of responses mentioned either both peer and adult help, or adult help only. In relation to Emily’s story, 29.4% of participants only mentioned help that involved the peer group, and 70.6% of responses mentioned both peer and adult help, or adult help only. There were no significant sex differences in these responses, in relation to either Tony’s vignette, χ2(1, N = 187) = 0.066, p > .05, or Emily’s vignette, χ2(1, N = 187) = 0.060, p > .05.
Finally, chi-square analysis was conducted to determine whether there were differences in the types of helping responses offered by participants who had correctly identified Tony and Emily as depressed, and those offered by participants who had not identified depression. No differences were found in relation to Tony’s vignette, χ2(7, N = 186) = 6.369, p > .05, or Emily’s vignette, χ2(6, N = 187) = 9.749, p > .05.
Why Do Young People Help Their Depressed Peers?
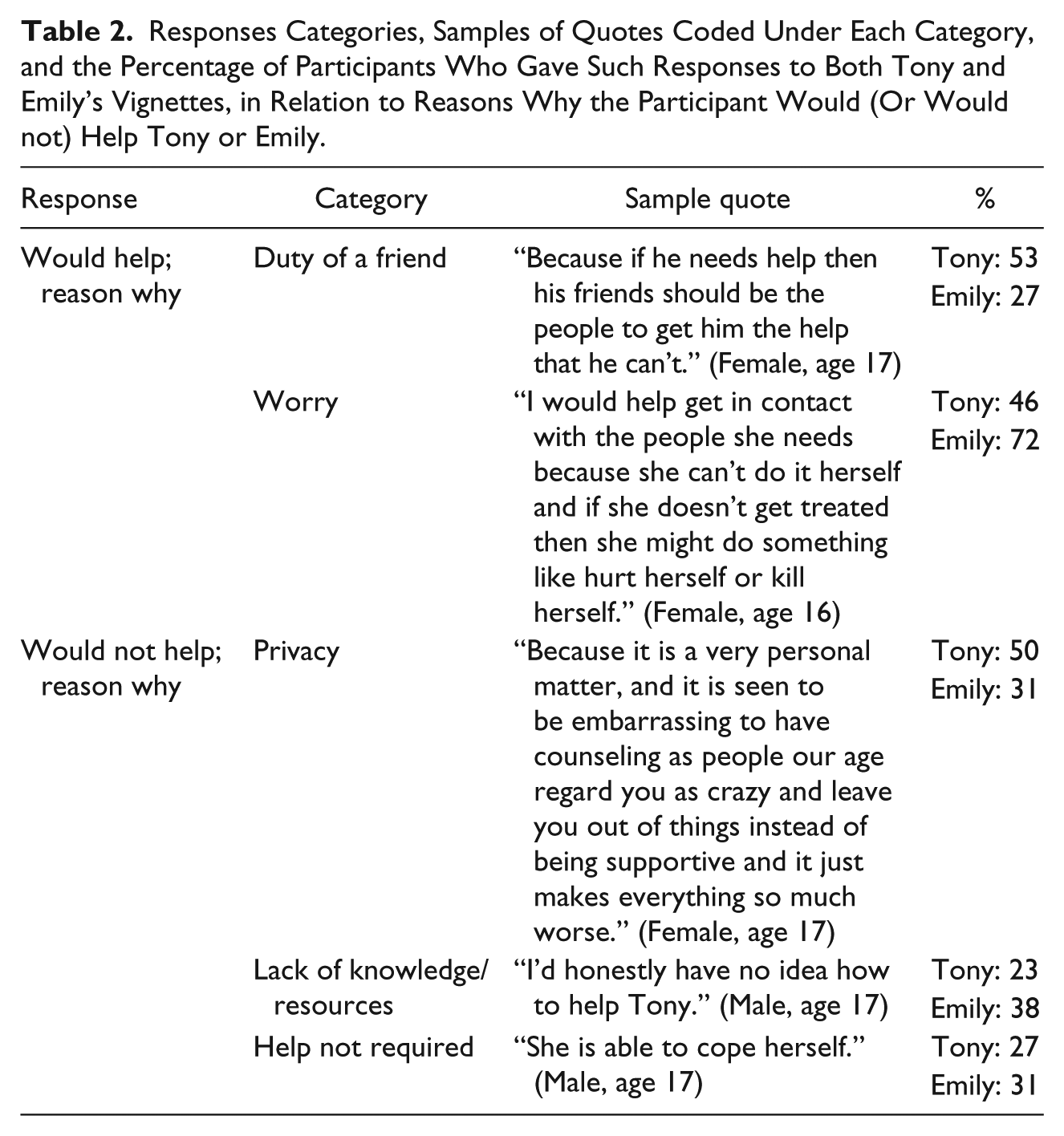
In terms of the reasons participants gave as to why they would help a depressed peer, two overarching categories were observed, “Duty of a Friend” and “Worry.” Sample quotes belonging to each category and the percentage of participants who responded as such to both Tony and Emily’s vignettes can be found in Table 2. Chi-square analysis revealed no sex differences between responses to either Tony’s vignette, χ2(1, N = 187) = 3.805, p > .05, or Emily’s vignette, χ2(1, N = 187) = 2.964, p > .05. There were also no differences in reasons given by participants who had identified depression and participants who had not identified depression in relation to either Tony’s vignette, χ2(2, N = 187) = 0.122, p > .05, or Emily’s vignette, χ2(1, N = 187) = 4.831, p > .05.
Responses Categories, Samples of Quotes Coded Under Each Category, and the Percentage of Participants Who Gave Such Responses to Both Tony and Emily’s Vignettes, in Relation to Reasons Why the Participant Would (Or Would not) Help Tony or Emily.
What Reasons Do Adolescents Give for Not Helping Their Depressed Peers?
A minority of participants answered “No” when asked whether they would help their peer: 21.4% in response to Tony’s vignette and 18.2% in response to Emily’s vignette. These participants were asked to explain why they would not offer help. Analysis of these responses yielded three categories: “Privacy,” “Lack of Knowledge and Resources,” and “Help Not Required.” The percentage of responses in each category and sample quotes can be found in Table 2. Chi-square analysis revealed significant sex differences between responses to Tony’s vignette, χ2(3, N = 187) = 9.224, p < .05, with 100% of responses in the “Help Not Required” category being provided by boys. No sex differences were found in responses to Emily’s vignette, χ2(3, N = 185) = 5.441, p > .05. No differences were found in reasons given by participants who identified depression and those given by participants who did not identify depression in relation to either Tony’s vignette, χ2(3, N = 187) = 7.066, p > .05, or Emily’s vignette, χ2(3, N = 185) = 6.670, p > .05.
Discussion
This study explored mental health literacy in Irish adolescents, specifically their knowledge of depression, and their help-giving responses to depressed peers. Sex differences in knowledge were also examined.
What Knowledge of Depression Do Irish Adolescents Possess?
Results indicated that participants showed more concern for the depressed vignette characters and felt that it would take longer for them to get better. Yet, a substantial proportion of the sample possessed insufficient knowledge to accurately label vignette characters as “Depressed.” Just over half of the participants correctly labeled Emily as depressed and just under a third correctly labeled Tony as depressed. It has been posited that the ability to label a disorder is secondary to the recognition that a problem exists and that help is needed (Leighton, 2009); this is supported by the finding in the current study that correct identification of depression did not have an effect on type of helping response offered. However, other research found that correct labeling is associated with the recommendation of appropriate help (Wright, Jorm, Harris, & McGorry, 2007). Burns and Rapee (2006, p. 232) also postulated that correct labeling “is likely to increase a young person’s urgency for seeking help and who they seek help from.” Therefore, the fact that a significant proportion of participants were unable to identify depression in these hypothetical peers is of concern. Although Social, Personal, and Health Education (SPHE) must be undertaken during the compulsory years of education in Ireland (i.e., Junior Cycle), detailed education on mental disorders is not provided (Department of Education and Science, 2000). These results suggest the inclusion of such education within the post-primary curriculum would be advisable.
Furthermore, less than 10% of participants identified Emily as suicidal. This discrepancy exists despite direct reference to suicidal ideation in Emily’s vignette, and the fact that three quarters of participants quoted the section of the vignette referencing these suicidal thoughts as the strongest sign of Emily’s emotional distress. In addition, assessing for suicidal risk was not mentioned by any participant when asked how they would help either Emily or Tony. These findings taken together suggest that young people may not be able to identify the links between depression and potential suicidality, and may not perceive assessing the level of suicidal ideation as a potential helping response. This is in line with Jorm et al.’s (2008) study, which presented participants with a vignette of a 15-year-old with depression and reported that a third of adolescents thought that asking the vignette character if they were feeling suicidal would be harmful, compared with less than 2% of GPs, psychiatrists, and psychologists.
Tony’s insomnia was perceived as the strongest hint that he might be experiencing emotional distress. Many participants expanded on this, implying that they interpreted his insomnia to be a direct function of worrying about his parents’ separation, rather than a physical symptom of depression. This attribution of the symptoms of depression to external causes is worthy of further investigation, particularly among young males.
Girls were significantly more likely than boys to list Tony’s weight loss and Emily’s fatigue as a symptom of emotional distress. Previous research suggests that girls are more likely than boys to present to mental health services with eating problems and fatigue, and therefore, these symptoms may be more readily recognized by girls as indicative of mental health problems (Bennett, Ambrosini, Kudes, Metz, & Rabinovich, 2005; Health Service Executive, 2011). Girls were more likely to list all of Emily’s symptoms as signs of emotional difficulties, corroborating previous findings of higher self-reported knowledge of depression in adolescent females (Williams & Pow, 2007). Overall, the current results imply that female participants had higher overall mental health literacy than males, which corresponds with the results of other Irish studies (e.g., Chambers & Murphy, 2011). In late adolescence, substantially more girls than boys are referred to Irish child and adolescent mental health services for depression (Health Service Executive, 2011). Thus, older adolescent girls potentially have more social experience of the presentation of depression in same-sex peers. It is important to highlight the concurrent yet conflicting findings in the present study, where girls appear to recognize depressive symptoms in a description of behavior, but cannot label these symptoms as depression. Similar findings were reported by a qualitative study with adolescent girls in the United States (Pinto-Foltz, Hines-Martin, & Logsdon, 2010).
What Types of Help-Giving Responses Are Offered to a Peer Displaying Symptoms of Depression?
The majority of participants thought both Tony and Emily required the help of another person, although significantly more girls than boys reported thinking this way. Jorm et al. (2006) also found that adolescent boys were more likely to believe in the helpfulness of dealing with depression alone. In contrast with findings from research conducted in the early 2000s (e.g., Sullivan et al., 2004), where older adolescents consistently recommend friends as primary sources of help for mental health difficulties, the present study found that both boys and girls favored the support of mental health professionals. Swords et al. (2011) reported similar results in an Irish sample of 16-year-olds, although other research conducted in Ireland in 2012 found only 28% of adolescent participants reported that they would be likely to use a psychologist, counselor, or therapist (Dooley & Fitzgerald, 2012). The current findings could demonstrate shifting attitudes about the usefulness or accessibility of mental health professionals, but further investigation is warranted. Furthermore, while participants in the current study endorsed mental health professionals as beneficial, responses to later questions indicated that they did not recognize their own ability to refer a peer to these sources of support. This is supported by the fact that when asked how they would help a depressed peer, approximately one third of participants’ help-giving responses to both Tony and Emily’s vignettes detailed help that involved only the peer group. This type of help-giving has been classified as “insular peer support” by Kelly et al. (2006).
The majority of participants agreed that they would help Tony and Emily if they were their friends. Girls were more likely to agree to help than boys, consistent with research that has shown girls to be more confident in their ability to provide help to peers (Jorm et al., 2007). Pertinently, the value of helping peers is emphasized in the participating schools, with the presence of their own youth leadership and peer support initiatives.
Why Is This Help Offered? If Help Is Not Offered, What Are the Reasons for This?
Participants’ accounts of how they would help a depressed peer varied across six categories: comforting and reassuring, perspective-taking, advice from similar experience, distraction, physical activities, and engagement with adults. Although engaging an adults’ support was the most frequently mentioned helping response, a sizable minority of young people did not recognize the importance of adult help for mental health difficulties. This is concerning, as the support of “one good adult” (Dooley & Fitzgerald, 2012) has been found to be one of the strongest predictors of good mental health among adolescents. Girls were more likely than boys to name multiple ways in which they would help both Tony and Emily. It could be inferred from this finding that girls have more knowledge of different alternatives for providing mental health support.
Participants’ reasons for helping a peer were related to either a sense of duty as a friend, or worry that not helping would lead to negative consequences. With increasing autonomy in late adolescence, it is likely that young people’s friendships grow closer, and the expectations of friendship, important even to pre-teens (MacEvoy & Asher, 2012), grow ever higher (Boldero & Fallon, 1995). As the quantitative findings of the current study imply, adolescents feel much concern for their depressed peers, and this worry can be seen to motivate their help-giving responses. It is interesting to note that while equal numbers of participants named each reason in response to Tony’s vignette, far more participants would help Emily due to worry rather than because Emily was their friend (72% compared with 27%). This suggests that when depressive symptoms reach the point of suicidal ideation, concern for a peers’ welfare may transcend friendship. This is important given the fact that research has found that in other forms of prosocial behavior, adolescents discriminate between friends and acquaintances (or “classroom peers”), with girls in particular more likely to help a friend (e.g., McMahon, Wernsman, & Parnes, 2006).
Those participants who stated they would not help Tony or Emily explained this decision by giving reasons that fell into three categories: that they felt the matter was private and it would not be “their place” to help, that they did not have sufficient knowledge or resources to help, and that help was not required. Again, it appears that these participants did not perceive their role as gatekeepers in the pathway toward accessing adult help, which reinforces the importance of educating adolescents about appropriate responses to help a friend experiencing mental health difficulties. Interestingly, all participants who felt that Tony did not require help were male, which again suggests that mental health literacy may be lacking in adolescent boys. Cognitive development has not yet been completed in adolescence, which may affect adolescents’ judgment processes regarding the need for help (Albert & Steinberg, 2011).
Limitations
In terms of this study’s assessment of mental health literacy, results must be interpreted with caution, as participants’ previous exposure to or experience with depression was not measured. Although participants demonstrated an awareness of the benefit of professional help, the source of their knowledge was not identified. With regard to help-giving behavior, one cannot assume with confidence that participants would apply the help-giving actions they described in similar real-life situations. As previously mentioned, the participating schools had youth leadership and peer support initiatives in place. This may affect the generalizability of the findings, as participants may be accustomed to the idea of helping others, given that this is promoted in these support initiatives.
The use of vignettes may be revised in future reiterations, as a previously acknowledged limitation of vignette-based research is that characters and situations may not seem real or relevant to participants (Leighton, 2010). However, this was hopefully minimized through the pilot study. It is also important to note that the order in which vignettes were presented was not randomized; therefore, there may have been order effects. The wording of some of the questions in the Burns and Rapee (2006) questionnaire is potentially leading; for example, “What do you think is the matter . . .” could lead participants to assume that there is something “wrong.” It is possible that without this prompt, participants would not detect that anything is the matter. In addition, the questions potentially constricted participants’ interpretation of the vignettes to issues of mental health, as the wording used was “emotional well-being” and “emotional difficulties.” As such, attributing symptoms to physical health or other problems could have been restricted.
Policy Implications
Adolescents in this study demonstrated fair levels of mental health literacy, and revealed their capacity and willingness to help peers. However, it is concerning that a significant number of young people in the current study could not identify depression or suicidal ideation in a peer, and would not assess for suicidality or engage an adult’s help. These findings have important policy implications in terms of training in mental health literacy and appropriate help-giving responses. Although concerns have been raised regarding placing too much responsibility on young people to provide early intervention and support for a friend in need, such training could teach young people to immediately acquire the assistance of an adult should they perceive emotional distress in a peer (Kelly et al., 2007). School-based programs that educate adolescents on mental health issues have already evidenced to be effective in Ireland (Power, Cleary, & Fitzpatrick, 2008). As current results show significant differences in male and female knowledge, this may need to be considered in the development of education programs (Burns & Rapee, 2006). For example, this study suggests that boys in particular could benefit from information on how to detect when help is required by a peer.
Conclusion
This research provides insight into adolescent mental health literacy in Ireland. The current research emphasizes the adolescent peer group as significant “gatekeepers” in the pathway toward service access in adolescents, as outlined in the GPM. Especially in late adolescence, it appears that peers are depended on as a primary source of emotional support, and adolescents perceive there to be certain responsibilities associated with being a good friend. The majority of adolescents in the current study showed great concern for a friend who they identified as being in distress, and were willing to provide help to this friend. However, specific knowledge around characteristics of mental disorders seemed to be lacking, in terms of the ability to label a cluster of symptoms, or the potential of suicidality. It was also demonstrated that adolescents do not always recognize the importance of engaging an adult’s help when a friend is in mental or emotional distress. The current research supports the proposal that providing adolescents with knowledge of appropriate sources of help, emphasizing the importance of engaging an adult’s help and assessing for suicidal risk, will help close the current service gap in child and adolescent mental health services.
Footnotes
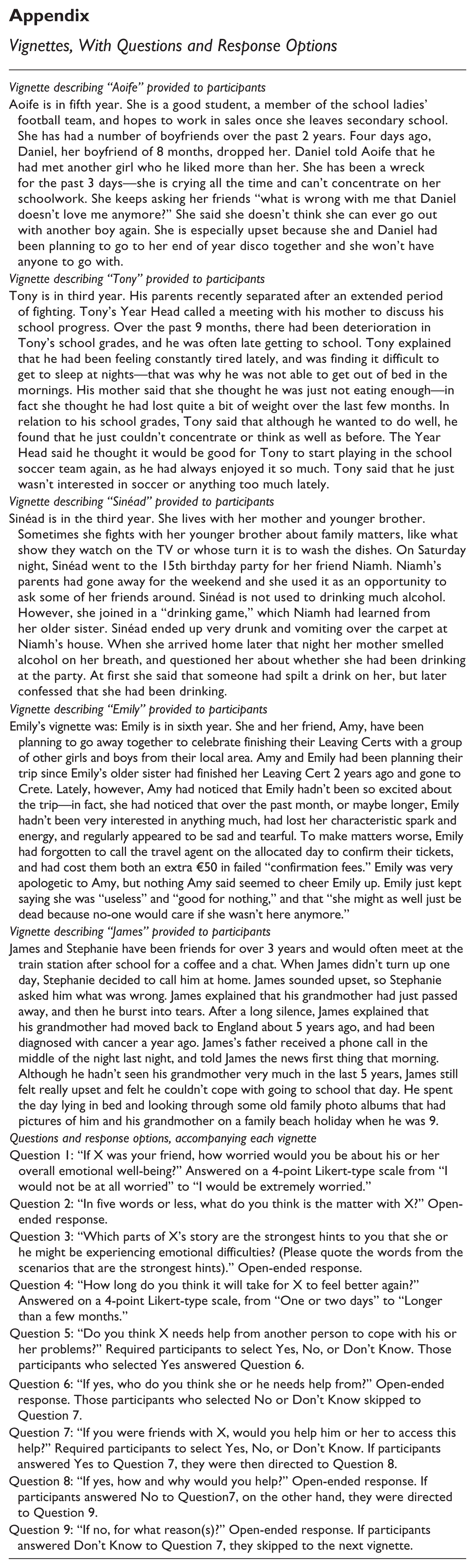
Appendix
Vignettes, With Questions and Response Options
| Vignette describing “Aoife” provided to participants |
| Aoife is in fifth year. She is a good student, a member of the school ladies’ football team, and hopes to work in sales once she leaves secondary school. She has had a number of boyfriends over the past 2 years. Four days ago, Daniel, her boyfriend of 8 months, dropped her. Daniel told Aoife that he had met another girl who he liked more than her. She has been a wreck for the past 3 days—she is crying all the time and can’t concentrate on her schoolwork. She keeps asking her friends “what is wrong with me that Daniel doesn’t love me anymore?” She said she doesn’t think she can ever go out with another boy again. She is especially upset because she and Daniel had been planning to go to her end of year disco together and she won’t have anyone to go with. |
| Vignette describing “Tony” provided to participants |
| Tony is in third year. His parents recently separated after an extended period of fighting. Tony’s Year Head called a meeting with his mother to discuss his school progress. Over the past 9 months, there had been deterioration in Tony’s school grades, and he was often late getting to school. Tony explained that he had been feeling constantly tired lately, and was finding it difficult to get to sleep at nights—that was why he was not able to get out of bed in the mornings. His mother said that she thought he was just not eating enough—in fact she thought he had lost quite a bit of weight over the last few months. In relation to his school grades, Tony said that although he wanted to do well, he found that he just couldn’t concentrate or think as well as before. The Year Head said he thought it would be good for Tony to start playing in the school soccer team again, as he had always enjoyed it so much. Tony said that he just wasn’t interested in soccer or anything too much lately. |
| Vignette describing “Sinéad” provided to participants |
| Sinéad is in the third year. She lives with her mother and younger brother. Sometimes she fights with her younger brother about family matters, like what show they watch on the TV or whose turn it is to wash the dishes. On Saturday night, Sinéad went to the 15th birthday party for her friend Niamh. Niamh’s parents had gone away for the weekend and she used it as an opportunity to ask some of her friends around. Sinéad is not used to drinking much alcohol. However, she joined in a “drinking game,” which Niamh had learned from her older sister. Sinéad ended up very drunk and vomiting over the carpet at Niamh’s house. When she arrived home later that night her mother smelled alcohol on her breath, and questioned her about whether she had been drinking at the party. At first she said that someone had spilt a drink on her, but later confessed that she had been drinking. |
| Vignette describing “Emily” provided to participants |
| Emily’s vignette was: Emily is in sixth year. She and her friend, Amy, have been planning to go away together to celebrate finishing their Leaving Certs with a group of other girls and boys from their local area. Amy and Emily had been planning their trip since Emily’s older sister had finished her Leaving Cert 2 years ago and gone to Crete. Lately, however, Amy had noticed that Emily hadn’t been so excited about the trip—in fact, she had noticed that over the past month, or maybe longer, Emily hadn’t been very interested in anything much, had lost her characteristic spark and energy, and regularly appeared to be sad and tearful. To make matters worse, Emily had forgotten to call the travel agent on the allocated day to confirm their tickets, and had cost them both an extra €50 in failed “confirmation fees.” Emily was very apologetic to Amy, but nothing Amy said seemed to cheer Emily up. Emily just kept saying she was “useless” and “good for nothing,” and that “she might as well just be dead because no-one would care if she wasn’t here anymore.” |
| Vignette describing “James” provided to participants |
| James and Stephanie have been friends for over 3 years and would often meet at the train station after school for a coffee and a chat. When James didn’t turn up one day, Stephanie decided to call him at home. James sounded upset, so Stephanie asked him what was wrong. James explained that his grandmother had just passed away, and then he burst into tears. After a long silence, James explained that his grandmother had moved back to England about 5 years ago, and had been diagnosed with cancer a year ago. James’s father received a phone call in the middle of the night last night, and told James the news first thing that morning. Although he hadn’t seen his grandmother very much in the last 5 years, James still felt really upset and felt he couldn’t cope with going to school that day. He spent the day lying in bed and looking through some old family photo albums that had pictures of him and his grandmother on a family beach holiday when he was 9. |
| Questions and response options, accompanying each vignette |
| Question 1: “If X was your friend, how worried would you be about his or her overall emotional well-being?” Answered on a 4-point Likert-type scale from “I would not be at all worried” to “I would be extremely worried.” |
| Question 2: “In five words or less, what do you think is the matter with X?” Open-ended response. |
| Question 3: “Which parts of X’s story are the strongest hints to you that she or he might be experiencing emotional difficulties? (Please quote the words from the scenarios that are the strongest hints).” Open-ended response. |
| Question 4: “How long do you think it will take for X to feel better again?” Answered on a 4-point Likert-type scale, from “One or two days” to “Longer than a few months.” |
| Question 5: “Do you think X needs help from another person to cope with his or her problems?” Required participants to select Yes, No, or Don’t Know. Those participants who selected Yes answered Question 6. |
| Question 6: “If yes, who do you think she or he needs help from?” Open-ended response. Those participants who selected No or Don’t Know skipped to Question 7. |
| Question 7: “If you were friends with X, would you help him or her to access this help?” Required participants to select Yes, No, or Don’t Know. If participants answered Yes to Question 7, they were then directed to Question 8. |
| Question 8: “If yes, how and why would you help?” Open-ended response. If participants answered No to Question7, on the other hand, they were directed to Question 9. |
| Question 9: “If no, for what reason(s)?” Open-ended response. If participants answered Don’t Know to Question 7, they skipped to the next vignette. |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.