
Abstract
The aim of this study was to explore the physical activity behaviors and body image of adolescent girls and their mothers. Adolescent girls (N = 44) and their mothers (N = 19) were recruited from three middle schools (two Colorado and one South Carolina). Girls qualifying for free or reduced-price lunches comprised 53% (South Carolina), 32% (Colorado), and 39% (Colorado) of participants. Focus groups with questions pertaining to body image and physical activity were conducted with daughters and mothers. The study was approved by the first author’s Institutional Review Board. Data were assessed using the five-step framework analysis. A thematic framework was identified, quotes were divided under the thematic content, and results were then interpreted by analyzing links among the whole data set. Four themes and eight subthemes emerged: (1) complex communication, with subthemes of daughter’s frustration and mother’s confusion, (2) societal expectations of women, with subthemes of social networks and women’s bodies, (3) high prevalence of social comparison, with subthemes of mother/daughter comparison and peer comparison, and (4) daughters’ awareness of mother’s health behaviors, with subthemes of weight loss and physical activity. Interventions aimed at improving adolescent girls’ health should include support for mothers as well as a psychosocial health and a mother’s educational component.
The relationship between mothers and daughters is complex and can have lifelong impacts on the development of adolescent girls’ health. As young girls develop, their body image (Clark & Tiggemann, 2006; Tatangelo & Ricciardelli, 2013) and physical activity levels (Leech et al., 2014) decrease. The intent of this study was to examine the influence of mother/daughter dyads on adolescent girls’ body image and physical activity behaviors using a qualitative approach.
Physical Activity
As of 2016, only 26% and 19% of men and women, respectively, met the physical activity guidelines for Americans (150 minutes of moderate-to-vigorous-intensity aerobic exercise weekly and 2 days per week of muscular strengthening exercises) as set by the U.S. Department of Health and Human Services (Piercy & Troiano, 2018). Worldwide, 80% of 13- to 15-year-old adolescents are not meeting the physical activity guidelines of 60 minutes of moderate physical activity per day (Hallal et al., 2012; World Health Organization, 2010) and this trend holds true in the United States, with only 25% of youth ages 12 to 15 meeting the physical activity guidelines (Fakhouri et al., 2014). Similar to adults, the prevalence of adolescents meeting the physical activity guidelines differs by sex. Adolescent girls are less physically active (Leech et al., 2014; Tudor-Locke et al., 2006) and more sedentary compared to adolescent boys (Cooper et al., 2015). A recent review article reported that, out of 18 empirical studies, 17 consistently reported boys being clustered in the high–physical activity group and girls being clustered in the low–physical activity group (Leech et al., 2014), one of which found that only 9% of girls, compared to 26% of boys, met the 60 minutes/day physical activity guideline (Gorely et al., 2007). Developmentally, it is important to note that as girls age their physical activity levels continue to drop; however, the greatest decline occurs during middle school years (a decline of 7.1% per year for girls 9–12 years vs. a decline of 5.1% per year for girls ages 13–16) (Dumith et al., 2011). The differences in physical activity behavior by age suggest that middle school may be an opportune time for tailored programming aimed at improving physical activity engagement and enjoyment in adolescent girls.
Early research on the relationship between mothers’ and daughters’ health reported greater lifelong physical activity participation in adolescent girls whose mothers were also highly physically active (Anderssen et al., 2006). In a diverse sample of older adolescent girls (mean age = 15.7), Bauer and colleagues (2011) found that, after controlling for education, age, and race/ethnicity, both family support and parent physical activity levels were significantly related to their daughters’ physical activity participation. However, a meta-analysis on the influence of parental behaviors on children’s physical activity reported that parental modeling (i.e., physical activity levels of the parents) is less influential on their daughter’s physical activity levels than once thought (Yao & Rhodes, 2015). Gustafson and Rhodes (2006) suggested that parental modeling may be more influential in early childhood, but as the child matures, parental modeling of physical activity becomes less important. As children transition into adolescence, parental support becomes more salient. Yao and Rhodes (2015) classified support behaviors as encouragement to be physically active, parent-child coactivity, praising the child’s activity, watching the child be active, informing the child that physical activity is beneficial, and providing transportation to physical activity venues, with parental encouragement having the greatest individual effect on the child’s physical activity levels. The greater influence of parental support compared to parental behavior modeling has been supported by others (Bauman et al., 2012; Trost & Loprinzi, 2011). Sebire et al. (2014) expanded upon this research by examining the impact of parental physical activity modeling and support on adolescent girls’ (age 11–12) psychosocial health (i.e., self-efficacy, self-esteem, and physical activity intentions) as well as their physical activity levels. Similar to Yao and Rhodes, Sebire and colleagues found that parental support was more predictive of adolescent girls’ health (self-efficacy, self-esteem, and physical activity intentions) than parental modeling, with maternal support being the greatest predictor of adolescent girls’ health. Compared to maternal modeling, maternal support requires more interaction and communication between a daughter and a mother. While it seems intuitive for a parent to discuss their child’s health directly with the child, it remains unclear if these conversations are taking place and whether they are productive.
Body Image
According to the “Tripartite Influence Model,” there are three sociocultural factors that influence the development of body image: (a) parents, (b) peers, and (c) the media (Van den Berg et al., 2002). The salience of each of these sociocultural factors depends on one’s age and developmental stage. During younger years, girls are more likely to spend time with their parents, particularly their mothers (Ebbert et al., 2019), which has been theorized to have a great impact on their body image development (Arroyo & Andersen, 2016). However, as girls age, they are less influenced by their mothers and care more about how their peers view them (Helfert & Warschburger, 2011). Michael et al. (2014) reported that in fifth grade girls body image was influenced by both a fear of poor evaluation by their peers as well how nurturing they perceived their mother to be. This demonstrates the importance of both peers and mothers in the transition stage of early adolescence. An additional and important contributing factor in body image development is the media. Older girls and adult women are exposed to more and varied sources of media, which has been shown to directly influence one’s body image (López-Guimerà et al., 2010). One of the reasons exposure to media negatively influences one’s body image is the overrepresentation of thinness or the “thin ideal” in mass media (Voelker et al., 2015).
During adolescence, many girls report a desire to be thinner (Clark & Tiggemann, 2006; Tatangelo & Ricciardelli, 2013), which is not surprising as adolescent girls tend to perceive themselves as more overweight than they actually are (Standley et al., 2009). Standley et al. (2009) found that, in a multiethnic sample of 14- to 15-year-old adolescents living in the United Kingdom, 43% and 24% of girls and boys, respectively, described themselves as being “too fat.” Moreover, those girls who reported wanting to be “fit” described this body type as “being and looking thin” (Phares et al., 2004), indicating that even healthy body types are being misinterpreted by adolescent girls. Most concerning, poor body image has been associated with disordered eating symptoms (Thompson & Smolak, 2001), depression, and decreased self-esteem (Phares et al., 2004). A recent study by Kenny et al. (2017) found that, in a sample of adolescents living in Ireland, most reported being aware of the unhealthy behaviors (e.g., suicide, self-harm, binge eating, and extreme weight loss attempts) that youth engage in as a result of body image concerns. This indicates that, despite an awareness of the possible physical and mental impacts having a poor body image can have, adolescents continue to struggle with their own self-perception and body image.
Influence of Mothers
Adolescents’ awareness of issues related to poor body image is partially a result of conversations they have had with their peers (Kenny et al., 2017). Girls are more likely than boys to discuss appearance with their peers (Lawler & Nixon, 2011), which leads to increased attention to body image–related issues, including the construction and acceptance of appearance norms (e.g., thin ideals; Clark & Tiggemann, 2006). Adolescent girls commonly compare their clothing size and weight with one another (Kenny et al., 2017) and their frequent social comparison and appearance conversations have been shown to significantly predict body dissatisfaction (Jones et al., 2004). Another source of comparison and appearance conversations, however, occurs between adolescent girls and their mothers. While girls’ body image is greatly influenced by their peers during adolescence, the impact of mothers may be more detrimental to the long-term development of girls’ body image as they transition into later adolescence and adulthood. Arroyo and Anderson (2016) theorized that the mother/daughter relationship has a greater impact on adolescent girls’ body image due to more time spent at home observing their mothers’ behavior than the time spent in school observing their peers’ behavior.
An adult woman’s body image has been socially constructed throughout her life and often consists of unattainable beauty standards (Fredrickson & Roberts, 1997). According to Bussey and Bandura (1999), people behave in ways that mimic their observations, thereby modeling the behaviors of others. The cycle of body dissatisfaction behavior modeling is difficult to break, particularly since mothers might not realize they are communicating such body ideals. Abraczinskas et al. (2012) found that mothers communicate body image ideals directly (via verbal communication) and indirectly (via behavior modeling), with indirect behavior likely the most influential. Cooley et al. (2008) found that daughters’ perceptions of their mothers’ behavior (in comparison to their mothers’ self-reported behavior) were a stronger predictor of the daughters’ health outcomes. When adolescent girls believe that weight status is important to their mother, they are more likely to express a desire to be thinner and engage in dieting behaviors (Field et al., 2005). Even though some mothers do not intend to communicate body image ideals, when mothers express personal body dissatisfaction in front of their daughters, the message of body dissatisfaction is reinforced (Wertheim et al., 1999).
Despite the intuitive influence of parental modeling on adolescents’ well-being, negative weight-related conversations are common between adolescent girls and their mothers (Berge et al., 2015; Eisenberg et al., 2006; Keery et al., 2005). Research indicates that mothers are more likely to encourage their daughters to lose weight when the mothers themselves are preoccupied with their weight, a trait associated with restrained eating behaviors (Francis & Birch, 2005). Keery et al. (2005) found that 13% of middle school girls reported receiving negative appearance–based teasing from their mothers. Further evidence demonstrates that, despite a mother’s “good intentions,” using negative weight-based talk with their daughters is commonly experienced as weight stigma (Berge et al., 2016) and leads to poor body image and dieting behavior in daughters (Francis & Birch, 2005; Vander Wal & Thelen, 2000). Other negative health outcomes associated with negative weight talk between mothers and daughters include daughters developing poor self-esteem, depressive symptoms (Eisenberg et al., 2006), loneliness, suicide (Eisenberg et al., 2003), and increased risk of becoming overweight or obese (Berge et al., 2015). More importantly, the harmful impacts of negative weight-based talk exist despite an adolescent girl’s weight status (Eisenberg et al., 2003; Keery et al., 2005), further exemplifying the influence of negative weight-based conversations between mothers and daughters on adolescent girls.
Conversations about weight between mothers and daughters may lead daughters to think that it is appropriate to evaluate their own bodies negatively and self-objectify since they have witnessed and participated in such conversations without any negative consequences (Arroyo & Andersen, 2016; Smith et al., 2016). Studies have shown that women often receive implicit rewards (compliments) for negatively discussing their body (Nichter, 2000) which subconsciously encourages them to continue such behavior. Therefore, a mother discussing her weight with her daughter may further perpetuate societal pressures, including desires to be thin.
This Study
Most parent/child negative self-talk research stems from self-report data from adolescents about their parents’ behaviors rather than self-report data from the parents about their own behaviors (Rodgers & Chabrol, 2009). Very little research has examined parent-reported behavior and its influence on adolescent health and studies that have yielded mixed results (Baker et al., 2000; Cooley et al., 2008; Keel et al., 1997). Therefore, this study’s inclusion of mothers’ and daughters’ perceptions of body image and self-esteem is an important contribution to the literature. Moreover, a majority of the current research on the relationship between mothers’ and daughters’ behavioral health (e.g., nutritional choices) has used quantitative methods, which has limitations in the depth of understanding (Ogle & Damhorst, 2000). Thus, the purpose of this study was to explore the physical activity behaviors and body image of adolescent girls and their mothers. Because this is a qualitative exploratory study, no hypotheses were made. Rather, the researchers used a phenomenological approach to gain a broad knowledge of mothers’ and daughters’ lived experiences (Creswell, 2013). The guiding research question was as follows: What relationship exists between mothers’ and daughters’ physical activity behaviors and body image.
Method
Research Design
Data for this study were drawn from the post-assessments (focus groups) of a larger study assessing the impact of Smart Fit Girls, an intervention designed to improve body image, self-esteem, and physical activity enjoyment in adolescent girls. After completing Smart Fit Girls, adolescent girls and their mothers (who received no intervention) participated in focus groups aimed at exploring the relationship between mothers’ and daughters’ physical activity behaviors and body image. Over a 2-year period, 44 girls and 19 mothers participated in seven and four focus groups, respectively.
Participants
Middle school girls (N = 44) and their mothers (N = 19) were recruited from three middle schools, two in Colorado and one in South Carolina (see Table 1). A greater proportion of girls than mothers participated in this study due to time restraints and scheduling conflicts with the mothers. An invitation for the mothers to participate in each focus group was sent home with each daughter (i.e., Smart Fit Girls participant). Other than their daughters’ participation in Smart Fit Girls, there was no additional benefit for the mothers to participate in the study. Prior to data collection, parent consent (for themselves and for their child’s participation) and child assent were obtained. Both the school district and the first author’s Institutional Review Board approved this study. Adolescent girls and their mothers were informed that participation in the study was voluntary and they could withdraw at any time.
Comparison of School Demographic Information.
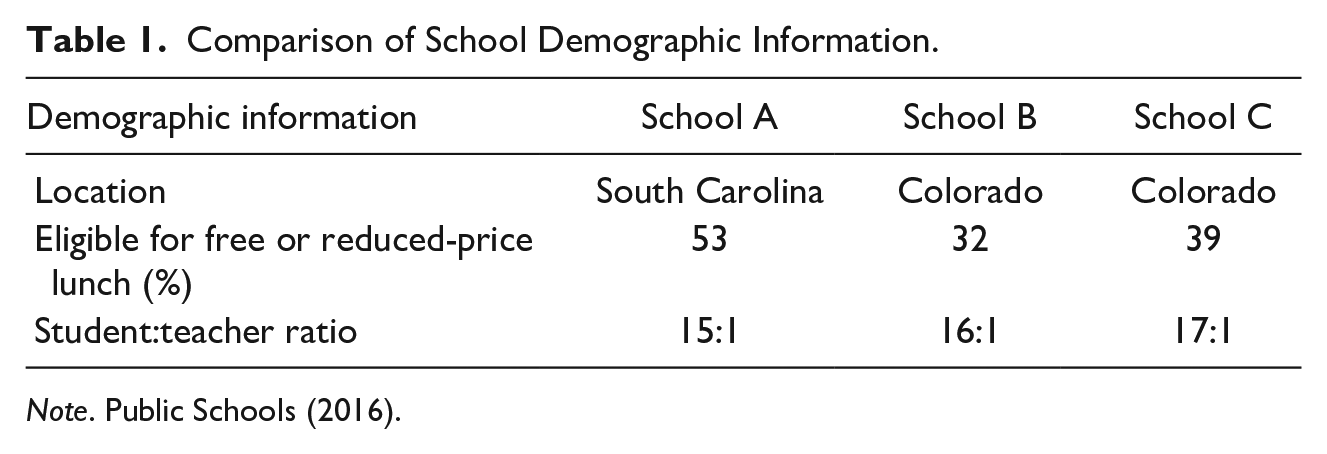
Note. Public Schools (2016).
Procedures
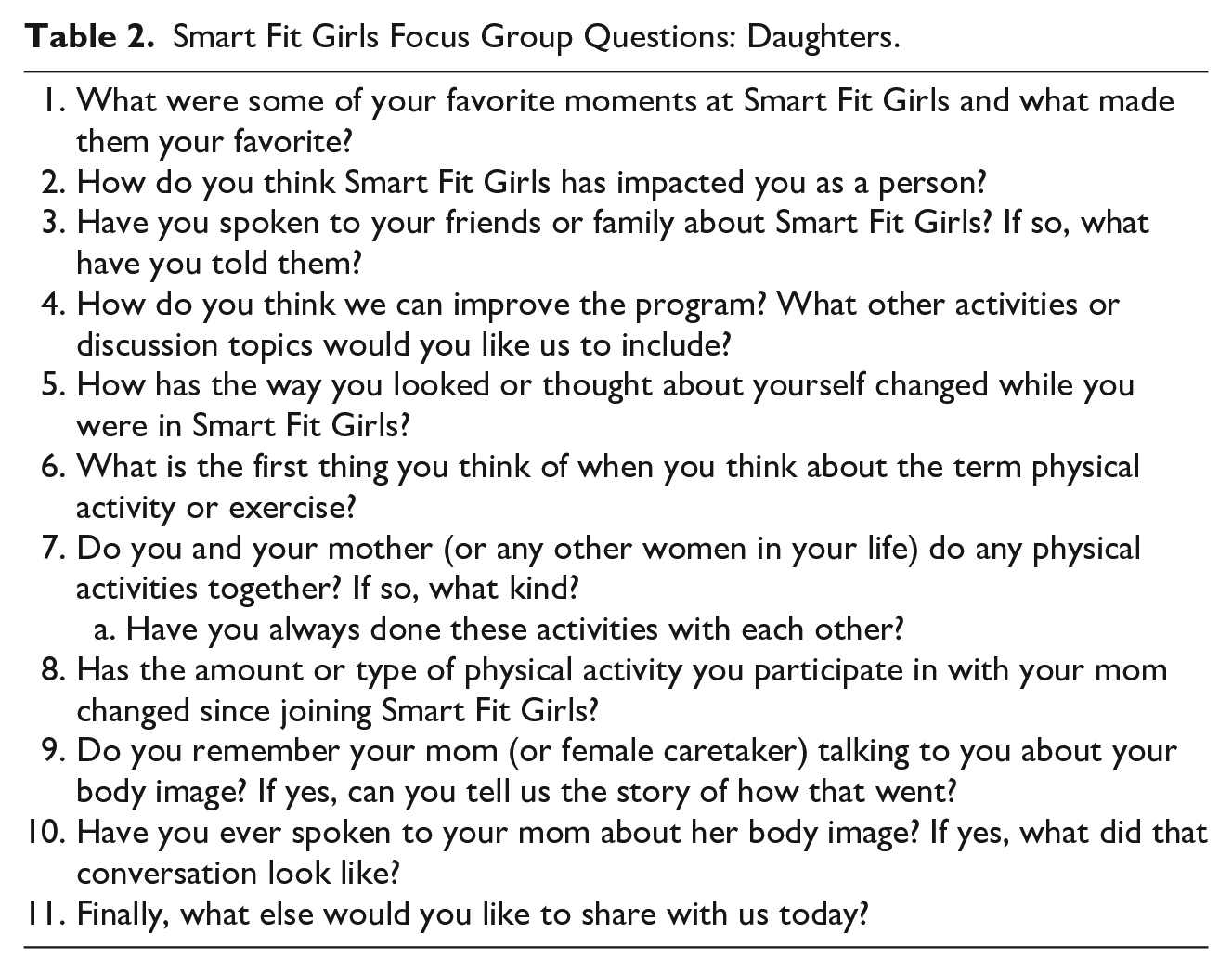
Focus groups (Tables 2 and 3) were used in this study due to the nonthreatening environment and subsequent comfortable discussion they often foster among participants (Rabiee, 2004). Focus groups allow researchers to observe group interactions and empower participants to drive the conversation, which has been shown to lead to new and unexpected results (Tiggemann et al, 2000). Three members of the research team administered the focus groups, all of whom had sufficient training and experience conducting focus groups. In addition to the focus group administrator, a second research team member attended each focus group and took detailed notes. Focus group questions were written by the first author and approved by additional study investigators who have experience in qualitative research. Pilot interviews were conducted with seven adolescent girls attending one of the school locations used in this study. These interviews were used to determine the appropriateness of the focus group questions, order of question administration, and approximate time needed to complete the focus group.
Smart Fit Girls Focus Group Questions: Daughters.
Smart Fit Girls Focus Group Questions: Mothers.
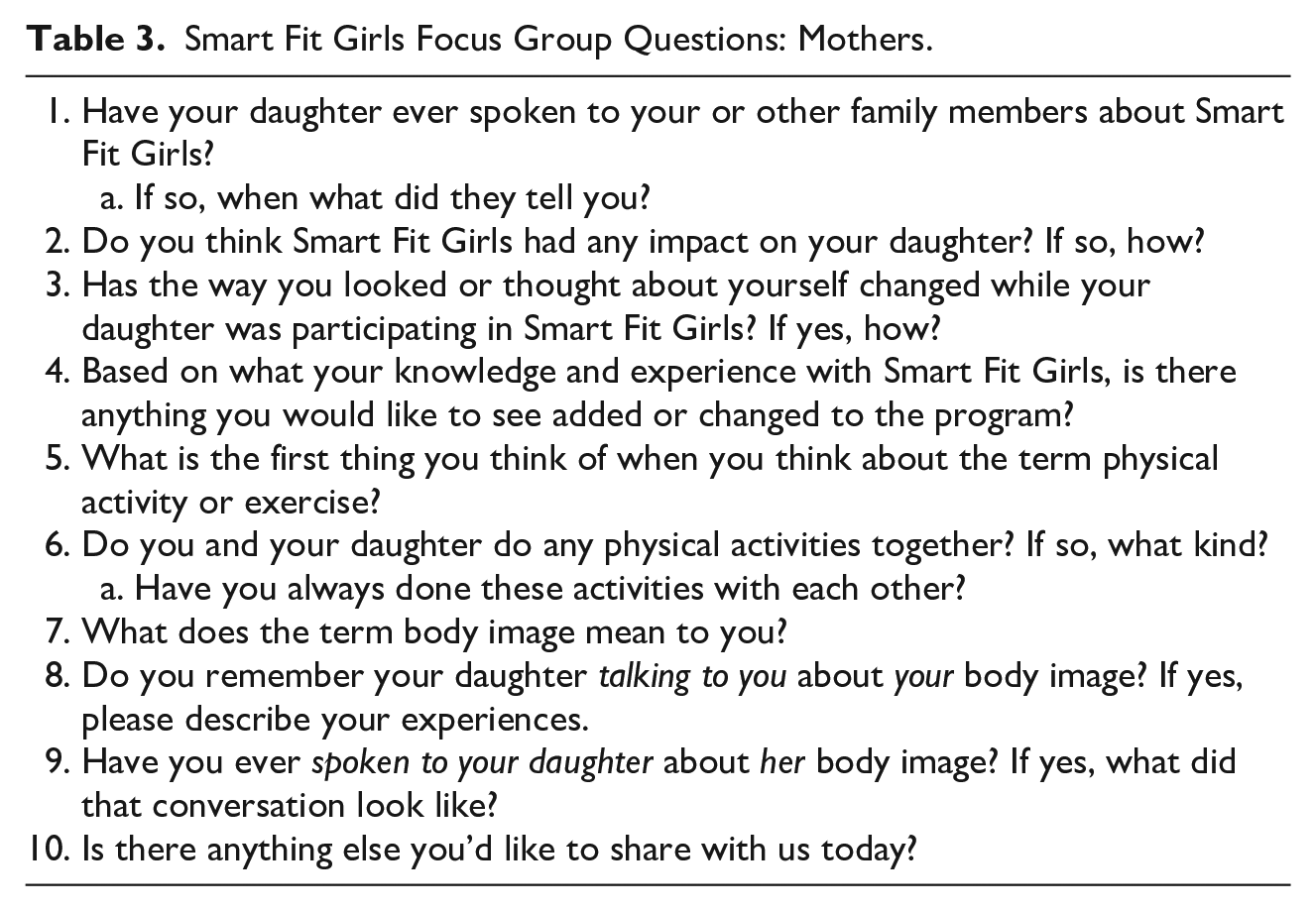
The focus groups were conducted after school ended in empty classrooms, except for one mothers’ focus group, which was administered in one of the mother’s homes due to time and logistical constraints. Each focus group lasted approximately 30 to 45 minutes and included an average of six girl participants or five mother participants. A total of 11 and 10 questions were developed for the daughters’ and mothers’ focus groups, respectively, with further discussion encouraged through supplementary probing or clarifying questions. Questions focused on body image and self-esteem (e.g., “Have you ever spoken to your daughter about her body image? If yes, what did that conversation look like?”) and physical activity behaviors (e.g., “Do you and your daughter do any physical activities together? If so, what kind?”).
Data Analysis
Focus groups were analyzed using the five-step “framework analysis,” outlined in Rabiee (2004). To start, all researchers familiarized themselves with the data by listening to audio files and reading transcripts and observational notes multiple times (Step 1). An inductive, open coding approach was used to develop a thematic framework. The authors individually wrote memos in the margins of the text containing ideas (e.g., mom realizes she needs to communicate her own health concerns differently with her daughter), codes (e.g., comparison), or short phrases (e.g., subconscious jealousy by mom) (Step 2). After completing Steps 1 and 2 independently, the researchers met twice more to discuss their individual memos. This process was done so the researchers could see which memos were agreed upon by all authors (including why and how those memos were representative of the data) and to discuss how those memos would be transformed into themes. Once Step 2 was complete, authors met again to identify an original draft of 14 themes. After indexing the data (i.e., sifting through the data, sorting and highlighting quotes, and making comparisons between focus groups (Step 3)), researchers organized the data by rearranging quotes under the previously developed thematic content (i.e., the 14 originally developed themes) (Step 4). The authors reviewed the quotes under each of the initially developed themes for quality, representation, and quantity and further discussed theme development. This discussion leads to a reduced number of themes: four primary themes, each with two subthemes. Once the final themes were agreed upon, researchers interpreted the results by analyzing links among the data sets as a whole (Step 5). Intercoder reliability was addressed through an iterative coding process (outlined above in Steps 1–5) whereby the authors developed and agreed upon the final themes. Using this repetitive process, researchers met several times to discuss themes that best represent the experience of the participants. To enhance trustworthiness, the authors reviewed the personal notes they took throughout the data analysis as well as the focus group notes taken during the actual focus groups (Creswell, 2009).
Results
The thematic analysis resulted in four major themes: (1) complex communication, (2) societal expectations of women, (3) social comparison, and (4) daughter’s awareness of mother’s health behaviors, each with two subthemes.
Theme 1: Complex Communication
Both the adolescent girls and their mothers reported that they found health communication (e.g., pertaining to body image, self-esteem, and physical activity) between one another challenging. Two subthemes emerged: (1) daughters’ frustration and (2) mothers’ confusion.
Daughters’ frustration
The girls reported feeling discouraged when talking to their moms about health for multiple reasons, including (a) a general awkwardness surrounding mother/daughter communication about their bodies and (b) frustration with their moms’ negative self-talk. Daughters perceived health-related communications as challenging and mostly negative, particularly those surrounding physical activity and nutrition. One of the daughters said, I used to get like huge portions, because I love food, and she would have this tone and it was like, “um you might want to go [eat] a little less” . . . and I would get really mad.
They also expressed not feeling comfortable talking to their moms about such topics and that previous experience doing so made them feel misunderstood. One girl said, “it’s kinda like you want to say something but you just don’t know what to say.” Another daughter said, “I talk to my friends about things like that all the time” and then followed by saying, “I have this weird issue with my mother where I have the hardest time talking to her about things, I’m always afraid I am going to get the worst response.”
Only a small number of daughters reported feeling “open” with their moms, and even when they did, they still expressed being uncomfortable with such conversations. One girl said, “I feel kind of open with my mom but it’s kind of awkward because we are always told to like, at school and stuff, not to talk about that sort of stuff,” indicating that the girls are receiving messages from their social network about the appropriateness of health-related conversations with their mothers. A possible contributing factor to the daughters’ uncomfortable feelings related to communication was their mothers’ negative self-talk. Mothers’ own negative self-talk was a source of frustration for many of the girls. They reported multiple examples of having to encourage their moms when their mothers spoke negatively about themselves (e.g., “when we go shopping together and she tries on stuff she’s, she always calls herself fat”), which resulted in the daughters feeling upset. When talking about her mom, one of the daughters said, “she kind of is a hypocrite because she would be like ‘you should feel good about yourself, you’re beautiful’ and then she’ll sit there and talk bad about herself.” This same participant followed by saying, “one day I confronted her about it and she just blew up on me and started talking bad about herself again.” Similarly, another daughter said, “my mom used to always like talk bad about herself and . . . I couldn’t tell my mom because she would always bring it in an opposite way and pull me down.”
The daughters also described feeling poorly about their own bodies when their mothers used negative self-talk because they saw themselves in their mothers. When the daughters thought they looked like their moms, they questioned whether they should be worrying about their bodies the way their mom does. One daughter said, “when she says something about her [body], it makes me feel bad about it too . . . we’re built the same so it makes me think sometimes, ‘should I worry about this or do I look bad?’” Another daughter reported a similar experience and emphasized how upset the interaction made her: “When she says like she’s fat or she’s ugly or something like that . . . I get furious and I get depressed” and when asked why the daughter felt so upset, she responded, we look so much like her that it’s not funny and . . . so when she says things like “oh I’m fat, I don’t look good,” I’m all, “I look like you, does that mean I have to think that too?”
Mothers’ confusion
Results from the mothers’ focus groups complement and confirm the themes found in the daughters’ focus groups. The moms reported feeling confused in regards to how to adequately communicate with their daughters about body image, self-esteem, and healthy behaviors (e.g., physical activity and nutrition). One mother said that she would like to learn how to relate to her [daughter] on a level that would be sensitive enough so that she doesn’t think that I am blowing her off on certain types of things but at the same time how do I communicate to her in a better [way].
Similarly, one mom said, “I don’t want to say it’s not even flattering because it’s so tight because that’s insulting her body image or making her feel ‘fat’ or ‘heavy,’” while another said that “it’s really hard to watch what you say and how you say it.” Some moms reported trying to find a balance between helping their daughters have a positive self-esteem and at the same time staying modest. For instance, one of the girls said, I don’t want [my daughter] to feel like I did but I don’t want her to be too, like boastful about it either . . . I think it’s a big deal and it’s a hard balance to say one thing or another.
Similarly, another mom said, “there’s that boundary that we’ve always talked about, like not being too prideful but you know, being confident in who you are.”
Conversations pertaining to nutrition seemed to be the most challenging for moms. One mother claimed that her daughter is a “carb addict and we have had those conversations and they probably haven’t gone the best but I feel like I don’t know how to . . . respond to her because she’s a petite thing.” Another mom said that she tried to give her [daughter] advice that helped me when I did focus on eating better . . . but I didn’t want her to feel pressured because I remember what that was like being a kid and being overweight.
Even when moms have good intentions, conversations surrounding their daughters’ health remain challenging and often result in the daughters feeling poorly about themselves. One mother said, I’ve made comments to [my daughter] about “you can’t eat junk food you will put on weight” . . . I know that it’s coming from a place of protection because I don’t want people to ridicule her and hurt her.
This conversation also had an impact on the mother’s older daughter who “would get very angry at me for saying anything and she would be like ‘you’re always saying things, you’re critical.’”
The mothers also acknowledged speaking negatively about themselves in front of their daughters and expressed concerns in doing so. One mom said, “I realized I have to be careful of what I might say . . . she looks at me differently when I say ‘I’m gonna gain weight or something.’” Another mom reported her daughter saying, “momma, you’re being so hard on yourself.” Another mom said, “she has always been extremely supporting and she’s always like ‘you look great mom.’” Similarly, other moms reported that their daughters have “told me to be nice to myself and that I’m beautiful and that I’m not fat and stop saying it.” The mothers were also able to recall specific examples of how they used negative self-talk in front of their daughters. For example, one mom said, I probably say that I’m fat out loud every single day and my kids hear that. They’re always telling me “mom stop saying that about yourself, you’re not fat, stop saying that” and they’re correcting me all the time.
Another mom said, “I’m trying to be a little more conscious of saying ‘oh I’ve got bingo wings here instead of my arms’ because I don’t want them to be knocking themselves the way I sometimes do.”
Theme 2: Societal Expectations of Women
The second theme that emerged was the awareness of societal expectations of being a woman. Two subthemes emerged: (1) Social networks influence self-perception and (2) a woman’s changing body (e.g., puberty, pregnancy, aging) influences self-perception.
Social networks
The mothers reported feeling pressure to conform to a certain societal set standard of behavior and aesthetics. A clear distinction was made between the perception of expectations for men versus women in society. One mom stated, in society women are picked on more than the men and you know my husband [has] gained just as much weight over the years as I have but because I’ve had three kids I feel . . . the pressure to get it off.
Similarly, another mom stated, “I think society is so tough on women and girls . . . and especially mothers.” The perceived difference in expectations between men and women was confirmed in the daughters’ focus groups through the lens of their mothers. When asked whether their mother had ever talked to them about body image, one of the daughters responded with “my mom . . . feels like she has to look a certain way.” This conversation developed into the daughters discussing how girls experience physical activity differently than boys, indicating a frustration with not only how girls are viewed by boys but how girls view themselves. One of the girls said, “I hate it when boys say girls aren’t as strong as boys. It’s stupid because how do you know, you’re not a girl.” Similarly, another girl said that there are “some sports like that, they don’t allow girls to play . . . or the girls just don’t think they’re like able to, like they’re too big or they’re too skinny, or whatever excuse they have.”
The pressure to conform to societal expectations led mothers to feel as though they could not express how they really felt about their bodies. One of the mothers said, I freak out every time I think about having to go back and visit family because I was the “skinny one” and so I always have to kind of try to work out as much as possible . . . so I would almost feel pressure and embarrassment sometimes.
In addition to feeling distressed about the unrealistic body expectations for women in society, one of the mothers reported feeling pressured to be satisfied with her body as it was. This mother reported that after posting something on her social media about being fat, all these people came at me like “you need to love where you’re at,” so there’s that pressure of . . . acting as if you’re super comfortable with wherever you’re at. And then, there’s the pressure of the ideal.
Mothers also expressed concern over how societal pressures of being a woman will impact their daughters. There was an overall agreement between the mothers that their daughters, by virtue of being a woman, will experience societal pressures and expectations of being a woman, which will in turn impact how their daughters feel about themselves. Two moms stated, “obviously girls are just more, I think, insecure because of society” and “society is tough and especially in middle school, people are tough on kids.” Another mother said, guys can look however they want . . . they’ve got their beer bellies and no one comments but [people are] . . . making judgements about women so I don’t know how to make it with our girls to not get caught in that.
Interestingly, the conversation about societal expectations for women’s bodies and physical activity behaviors leads to a broader conversation about roles and responsibilities of women. One of the mothers said, “I think society is hard on mommas because we’re supposed to have it all together. We’re supposed to be the calendars, we’re supposed to be the organizers, [and] we’re supposed to be the housekeepers.” She continued with “we’re supposed to be the cooks, we’re supposed to have a job, we’re supposed to be really sexy for our husbands and, and keep it all together.” She also said, “if our kids aren’t smart we’re doing something wrong” and if they don’t have their homework turned in, they don’t think about the dad . . . if you come over to the house and it’s messy, you don’t think that the husband is a terrible housekeeper, you think that wife can’t keep her crap together.
This mom ended by saying, “I think girls see their mothers handle a majority of things . . . so I think it’s tough for girls to feel successful when . . . it’s kinda hard to be successful in all those realms.”
Women’s bodies
The second subtheme that emerged within the theme of societal expectations was that a woman’s changing body (e.g., puberty, pregnancy, aging) influences her self-perception. Mothers reported feeling frustrated with their bodies throughout their lifespan (e.g., “I was tough on myself at that age [and] I wish I wouldn’t have because now I can be tough because I’m seeing changes”), many of them pointing out pregnancy as an event that shifted their body perception. One mother said that she realized “after three kids that [she] can’t eat as much and that things change.” Similar reports were made by other moms such as your body image probably started changing about the time you had children . . . your body never goes back to how it was and there is nothing . . . you can do to put it back . . . you become a mom and that changes everything
and “I have worked out for years and I have had to come to realize that my body just isn’t what it was.” The idea that pregnancy is a catalyst for body dissatisfaction was identified by the daughters as well. When asked whether her mom had ever talked to her about her mother’s body image, one daughter said, “she had three children so she has that extra skin I think that it’s from having children, so she thinks she’s overweight and she has to get back in shape.” This same daughter reported feeling confused about how to talk to her mom about her pregnancy for fear of making her mom feel bad: “It’s really hard for me to talk to her about that because I like don’t want her to think she’s too overweight.”
The moms expressed feeling challenged with how to handle their daughters’ changing bodies. One mom stated, “teaching your kids not to want to be an object . . . because that’s exactly what happens but they feel proud, they’re like ‘I’m known as like the booty girl,’ you know, so it’s tough.” Another mom said that there is a fine line of being proud of who you are but not being too boastful of like, that you’re skinnier or whatever, you know? . . . How you dress and stuff, it’s very hard to like to have that balance.
Similarly, one of the mothers reflected on a conversation she had with her daughter about her daughter’s changing body and clothing choices, telling her that “you need to not wear the little bitty shorts. You can wear them in the bed but you’re getting older . . .” and when you are walking around . . . being aware of that your body is changing and even though I know you’re not trying to get that kind of attention . . . just have that mindset I am going to be proper and appropriate at all times.
The mothers also reported feeling dissatisfied by the clothing options available for young girls, noting that their daughters struggle trying to fit into certain clothing styles and sizes. One of the mothers stated, “it was always a big deal when they’d change sizes and they were worried about the sizes,” while another mother reported that her daughter would “get really frustrated about shopping, ‘I can’t wear these skinny jeans because they don’t look right on me’ or ‘I can’t wear this because this doesn’t look like it does on the model.’” Similarly, another mom described her daughter as “skinny and tall” and because of that she doesn’t fit into little kids clothes anymore but she’s not in the junior’s section either so it is very hard to find things that fit appropriately and look nice and not too short . . . she struggles with that, you know?
The struggle of feeling pressured to fit into certain clothing styles and sizes was confirmed in the daughters’ focus groups. One girl brought up a conversation she had with her grandmother (her primary caretaker) about clothing and body image. The daughter said that “one day I couldn’t fit [in] these jeans because the zipper was stuck but she [my grandmother] thought it was just because I was so big.” Her grandmother responded with “you are getting fat and you need to fix this now” which made the daughter feel “very badly.” The daughter then reported that “I didn’t even want to be seen with her [my grandmother] because like I wasn’t even comfortable like I was just now starting to accept myself and then she put me back down, like ‘thanks.’”
Theme 3: Social Comparison
The daughters and mothers reported comparing themselves against other girls and women frequently, which lead to negative perceptions of themselves. These negative perceptions of themselves included how they viewed their own and others’ bodies and their personal life success (in work, school, and/or relationships). Two subthemes emerged: (1) Mothers and daughters compare themselves to their peers and (2) mothers’ comparison of themselves to their daughters influences their daughters’ perception of self.
Peer comparison
Social comparison between the mothers was common. One mother stated, “I went on vacations with like other women and if all the women looked good in their bathing suit I would just feel so inferior just because my body was different or I wasn’t in a healthy state.” Similarly, another mom said, if “you’re not the prettiest one in the room, you’re gonna cut down the woman that is prettier than you. You’re gonna find something wrong with her.” The comparison between mothers extended beyond body image to perception of success. One of the mothers stated, you see someone that looks like they’ve got everything going on and then you think “oh well they’ve got a house cleaner and they’ve got a personal chef” . . . that are helping them along the way you know?
The moms also reported that their daughters were high social comparers as well. In response to her daughter comparing herself to female peers, one mother said, “I remember like a year ago [my daughter] was comparing herself to [her friend] and we had to sit down and say ‘you two are perfect the way you are but you’re different.’” Their daughters’ social comparison episodes seemed to center around social media use (“girls get on their phones and ‘oh my gosh, look at her’ and just there’s all this negative stuff going on with comparing people and who’s pretty and who’s not” or “she’s sitting there on Instagram worrying about what people are wearing and how they look”) and clothing (“I know a lot of girls are talking [about] what size jeans they wear”). Mothers also reported that their daughters’ experience with peer social comparison had resulted in their daughters trying to lose weight: her friends that I have met are extremely thin compared to her and they were telling her to do crazy stuff . . . like “here’s this diet” and I was like “you are 10!” but [she] has asked to do that [try the diet].
Mother/daughter comparison
The mothers frequently mentioned comparing their bodies to their daughters, articulating that they wish they would have had more appreciation for their bodies when they were young. One mother said, when you get to be . . . this age . . . it’s a difficult thing and then you have a young girl who, you used to look like that is, it’s really hard to watch what you say and how you say it.
Similarly, another mom reported that her daughter is “built like me and growing up I always felt so different because not many girls have body types, like very powerful legs, and so it was something that I had always struggled with.” In addition to comparisons to their daughters, the mothers wished they would have been more accepting of their bodies when they were young. One of the mothers said, if I would have known so many years later that I was going to be like this . . . really wanting to hide when I thought about putting on a swim suit . . . I wish I would have worn the nicer swim suit.
This same mother followed by saying that her daughter is very tiny and I used to look like that . . . I look back and I’m like “dang it! Why didn’t I wear that bikini?” but it was because my hip bones stuck out and people made fun of it.
The daughters confirmed this finding with statements like “she says she’s jealous of me because I’m so skinny and I’m like ‘well I’m jealous of you because you’re so skinny.’” The daughters highlighted that when their mothers speak negatively about their bodies, they felt poorly about their own body image because “most of your moms look like you, or you look like your mom, and when they are saying something about themselves it means they are kind of saying it about you, so it’s bringing both of y’all down.” How the moms talked about themselves in front of their daughters also impacted their daughters’ self-image. One daughter said, she’s my role model so when she says things like . . . “Oh I’m fat, I don’t look good” I’m all, “I look like you, does that mean I have to think that too?” . . . that’s why I have such a bad self-esteem.
As a result of what their mothers said about themselves, girls also reported feeling poorly about areas of their bodies that are typically not scrutinized by society (e.g., not liking her ears). When asked why the daughters felt frustrated about their moms’ poor body image, one girl responded with because of genetics . . . when she’s saying that to herself, she’s saying that to me as well because I’m her daughter . . . we might have like funny ears too and so she is saying the same thing to us,
while another said, “because some bits of our bodies we take after hers.” The daughters reported feeling sad as a result of hearing their mothers speak negatively about their bodies because the daughters thought they looked like their mom. When their moms say something negative about their own body, the daughters question whether they should be worried about their own bodies since they look like their mothers. One of the daughters said that her mom used to always like talk bad about herself and I couldn’t . . . talk to her about the stuff I wanted to . . . I couldn’t tell my mom because she would always bring it in an opposite way and pull me down.
Another daughter said that her mom “looks so much like [me] that it’s not funny” so when her mother “says like ‘oh my God I look really fat,’ she’s kind of like my role model so when she says that I’m all ‘Oh God, what if she is right, what if I look like that too.’”
The association the daughters drew between their feelings about their body and their mothers’ body dissatisfaction led to feelings of depression and sadness. One daughter said, “when she says like she’s fat or she’s ugly or something like that, I get really um, I get furious and I get depressed,” while another said, “it makes me feel upset, it makes me feel depressed . . . it makes me feel like it’s my fault sometimes.” Other girls expressed frustration and anger, saying things like “I hate when I hear her say that because it’s like ‘dude, you’re skinnier than me and [friend] combined’ and ‘It makes me feel . . . upset . . . that she doesn’t like her own body.’” Similarly, another daughter said, “it upsets me because I feel like my mom is skinnier than me. When I hear her talking about how much she is fat . . . it upsets me because it makes me feel like I’m that way.”
Theme 4: Daughters’ Awareness of Mothers’ Health Behaviors
The daughters’ focus groups revealed that the girls were quite aware of their mothers’ health behaviors, including previous dieting experiences and physical activity participation. Two subthemes emerged: (1) Daughters reported that their mothers have tried multiple different weight loss methods and (2) daughters noticed the level of physical activity participation their mothers engaged in.
Weight loss
When the girls were asked to recall times their mothers spoke to them about body image, many of the girls brought up examples of weight loss attempts their mothers had made, often mirroring the negative self-talk described previously. One daughter mentioned that her mom “goes through phases. Like a lot of the time she has like all these friends that go on diets and are always really active and healthy but that can be like a good thing or a bad thing.” Similarly, another daughter said, “most of the stuff that my mom has for her diets are just pills and all that, and she has like stuff that are smoothies which don’t do anything.” Many of the girls mentioned that their mothers participated in multiple weight loss attempts, often disapproving of them because they were perceived as unhealthy. For example, one girl said that her parents are always complaining about how they’re overweight . . . they say they, that they are going to go out there and do something about it, like they are going to start eating healthy and all that stuff, but that didn’t really change my mom.
A few of the daughters were able to recall specific diets their mothers had been on, with one daughter saying, “my mom like goes on diets, like she’s done Weight Watchers twice . . . [and] Slimgenics.” This same daughter also said that her mother has “done like three different ones because she thinks she is fat and then she makes us join in it just since their, their food is healthy, when really it’s not.” This daughter’s negative emotions surrounding this memory was evident when she ended her statement with it’s not really doing anything except changing the way they think of themselves . . . it kind of makes me feel depressed just for their sake since they’re not fat or anything. Yeah, they have curves but that’s a good thing.
Physical activity
The daughters were also very aware of their mothers’ physical activity habits; some daughters reported that their mothers were frequently physically active, while others reported their mothers were mostly sedentary. However, what was consistent across the daughters was the awareness, and often disappointment, of their mothers’ exercise behaviors. One daughter said that when her mother “gets off working out on the machine thingy, she feels good for like the first ten minutes and then right before dinner it’s always like, ‘my legs are fat’ and she doesn’t like her butt.” Another daughter stated, you’re supposed to look up to your mom . . . and have that one woman in your life you have to look up to? Sometimes I can’t look up to her because she has low self-esteem . . . she’s just not exercising anymore.
When the daughters were asked if they were physically active with their moms, many of them responded by giving examples of times they were physically active with other family members (fathers, siblings, etc.) rather than examples of times they were physically active with their moms (“I do it with my brothers a lot and we’ll just dance to songs,” “me and my sister . . . usually walk the dogs together,” and “I either go on walks with my dad or I . . . do the seven minute workout thing”). Being physically active as a family was a more common response than being physically active with their mom exclusively. For example, girls reported playing sports, going to the gym, and going on bike rides as a family.
Responses related to specifically being physically active with their moms ranged from simple “no, but I encourage her to [be physically active]” to me and my mom used to go up to the Sandy Springs track and walk up there but now she don’t walk up there as much because . . . she gets really sore . . . so she doesn’t want to do anything anymore.
The most common form of physical activity that the daughters reported doing with their moms was walking and some girls expressed a sense of frustration with their experiences. One girl stated, “she is like making excuses like ‘I’m too old. I’m too fluffy’ and I tell her excuses don’t get results, you actually have to take the time to do something to get results.” Similarly, another daughter said, I used to work out with my mom a lot . . . but it aggravates me because I’m like a grumpy person so she’s always like “come run with me” and I’m like “no, you get on my nerves.”
Discussion
This study set out to explore the relationship between daughters’ and mothers’ physical activity behaviors and body image. As girls transition into adolescence, how their peers view them becomes more salient. However, mothers remain an influential source of a daughter’s body image development (Arroyo & Andersen, 2016; Michael et al., 2014). The findings from this study reveal that there is a strong relationship between the mothers’ and daughters’ physical activity behaviors and body image. The mother/daughter dyad seems to struggle with health communication, both through direct and indirect means. The societal expectations of women also influence self and body image that mothers and their daughters have. Social comparisons of the mothers and daughters to their peers, and the mothers to their daughters, are quite common and can create negative perceptions of themselves. Finally, the daughters’ awareness of mothers’ health behaviors shows to be quite influential on how daughters perceive their own body image and also physical activity. This is important as daughters will view their body image and physical activity more negatively if their mothers have this perception.
As girls transition from early (Grades 5 and 6) to middle adolescence (Grades 10 and 11), they begin to perceive communication with their mothers as less friendly (Beaumont, 1996) and report frequent conflict with their mothers (Laursen, 2005). Between the ages of 12 and 14, adolescent girls report a greater desire for autonomy and independence, which is characterized by a reduction in the frequency and quality of communication with their mothers (Keijsers & Poulin, 2013). Results from this study are similar to previous findings reporting that mothers communicate their weight concerns to their daughters and do so more commonly through indirect communication rather than direct communication (Arroyo & Andersen, 2016). Conversations among women about their body image concerns are commonplace and negative self-talk is often rewarded with positive compliments about one’s appearance (Salk & Englen-Maddox, 2011). Many women participate in such conversations in an effort to make themselves and other women feel better about their own body image (Salk & Englen-Maddox, 2011). By watching their mothers’ interactions with society, daughters learn that partaking in such conversations is socially “appropriate,” accepted, and, at times, encouraged. This is particularly problematic due to the strong correlation between frequent “fat talk” and depressive symptoms in adolescent girls (Chow & Tan, 2018).
Expanding on previous research, results from this study highlight the type of health communication that mothers and daughters perceive as most challenging; mothers and daughters found conversations surrounding mental and physical health (e.g., body image and physical activity) complex and uncomfortable. The daughters were frustrated with indirect conversations with their moms about health (e.g., moms talking about their own health concerns around their daughters), whereas their mothers disliked and struggled with direct communication about health (e.g., speaking directly to their daughters about their daughters’ health). This demonstrates a disconnect between mothers’ and daughters’ health communication, which has been corroborated by previous literature (De Los Reyes et al., 2016).
Results from this study also demonstrate that mothers’ and daughters’ social networks (peers and family members) influence their perceptions of self and body image satisfaction. These results correspond with those of Clark and Tiggemann (2006) who found that peers have a significant impact on one’s body dissatisfaction. McCabe and Ricciardelli (2001) reported that, contrary to popular belief, girls’ body dissatisfaction was influenced by mothers and female friends but not media. Results from this study demonstrate that mothers and daughters feel discouraged as a result of trying to live up to society’s expectations for women and girls. Particular anguish was expressed when discussing times in their lives when their bodies were changing (e.g., puberty and postpartum). This corroborates previous literature demonstrating body image concerns of women during pregnancy. Evans et al. (2016) demonstrated that, during pregnancy, a woman’s body image is affected by “pregnancy police” (members of a woman’s social network that voluntarily tell a pregnant woman what behaviors are appropriate for her). Both the mothers and daughters in this study felt that, regardless of one’s age, there is a “right” way to look, demonstrating their perceived, often unrealistic, body image ideals.
While people may not perceive themselves as social comparers (Hemphill & Lehman, 1991), evidence suggests that a majority of people compare themselves to others (Gibbons & Buunk, 1999). Adolescence represents a time period when individuals are particularly preoccupied with their social images (Gerrard et al., 2002; Oyserman & Markus, 1990) and are therefore more likely to be high “social comparers.” Developmentally, the act of social comparison continues into adulthood and research indicates that adult women compare themselves to their peers significantly more than adult men (Gibbons & Gerrard, 1995). Similar to Jones (2001) and Jones and Crawford (2006), the daughters and mothers in this study reported using information gathered from their peers’ behaviors and values to judge their own behaviors and values. This study’s results support previous findings, demonstrating that mothers and daughters compare themselves frequently to women/girls their age.
Our study expands upon previous research that demonstrates a strong relationship between mothers’ and daughters’ body image concerns (Abraczinskas et al., 2012; Arroyo & Andersen, 2016; Hill et al., 1990) by demonstrating how adolescent girls are negatively impacted by their mothers. When mothers say negative things about their own bodies, daughters wonder if they should feel negatively about that same body concern because they feel they look like their mothers. Daughters reported feeling sad, depressed, and angry as a result of their mothers’ negative self-talk and their own self-comparison to their mothers. It is likely that, in addition to negatively impacting a daughter’s body image, indirect negative health communication likely influences other components of her health, including self-esteem and anxiety levels. For example, adolescent girls who experience high levels of alienation and distrust in their mothers during middle school are more likely to experience anxiety in Grade 12 (Ebbert et al., 2019). This is a developmental transition worth noting and actively working to mitigate.
Finally, results from this study demonstrated that daughters were very aware of their mothers’ health behaviors, often expressing frustration regarding their mothers’ dieting and physical activity history. It is important to highlight the girls’ complex reactions to their mothers’ behaviors and negative self-talk, as it is representative of the duality of their experience. The daughters simultaneously internalized the negative messages from their mothers while also feeling frustrated as a result of those messages because they did not mirror how they perceived their mothers. The level of awareness and subsequent frustration daughters had of their mothers’ behaviors is consistent with previous research (Haines et al., 2008; Keery et al., 2006) and the mostly negative impressions from their mothers likely explain the high prevalence of dieting and weight concerns of adolescent girls (Hill et al., 1990). This finding expands on previous research, demonstrating that adolescent girls are not only aware of their mothers’ nutritional choices but are also very cognizant of their mothers’ physical activity habits. The level of frustration daughters expressed when describing their mothers’ relationship with physical activity suggests that their perception of physical activity is impacted by their mothers’ personal experiences. This is supported by previous literature that demonstrates how influential a mother’s personal relationship with physical activity can be (via parental support of physical activity and physical activity modeling) on her daughter’s physical activity behaviors, particularly as the daughter transitions into adolescence (Gustafson & Rhodes, 2006; Yao & Rhodes, 2015).
This study expands upon the current literature by providing a more in-depth perspective of the health of the mother/daughter dyad. Research indicates that health care professionals are unaware of how to best advise parents on how to discuss healthy behaviors (eating, physical activity, and weight) with their children (Foster et al., 2003). In addition, conversations between parents and adolescents regarding healthy behaviors (healthy eating and weight talk) have been associated with both negative (e.g., more screen time) and positive (e.g., greater intake of vegetables and fruit) adolescent behaviors (Berge et al., 2015). This demonstrates the complexity of health conversations between parents and their children. Since a majority of these conversations are between mothers and daughters, a particular focus should be placed on how to best facilitate health communication between both groups. Results from this study also demonstrate the influence of mothers’ weight-related talk (indirect and direct) on adolescent girls’ self-perception. Therefore, a possible implication of this study includes support for targeting mothers, in addition to adolescent girls, in interventions aimed at improving adolescent girls’ health. Other possible implications include targeting psychosocial health (e.g., body image) and including an educational component for mothers in programs aimed at improving adolescent girls’ health.
Limitations and Future Directions
There were multiple limitations to this study. First, the number of focus groups for each cohort (mothers and daughters) was uneven. However, the researchers all agreed that data saturation, defined as “the point in coding when you find that no new codes occur in the data” (Urquhart, 2012), was reached. In an effort to increase validity, future research should aim to include the same number of focus groups per cohort. Second, the use of focus groups has limitations as well (Bryman, 2012). Some participants may dominate the discussion, while others may feel uncomfortable discussing sensitive issues in front of others (Barbour, 2007). Trained focus group facilitators were used to avoid and/or navigate such situations. To enhance trustworthiness of the data, each focus group transcription was coded by three individuals separately and trained qualitative researchers facilitated the focus groups. Third, the generalizability of the findings is somewhat constrained given the use of the relatively small convenience sample. It is also possible that maturation (various stages of pubertal development) influenced research findings. Usmiani and Daniluk (1997) found that the association between mothers’ and daughters’ body image existed when their daughters reached menstruation; however, this relationship did not exist pre-menstruation. In the future, researchers should expand the age range of girls and collect longitudinal data to explore whether maturation influenced such findings. Finally, since data used in this study came from a larger study where daughters were participating in a health intervention, it is possible that the intervention had an effect on the mother/daughter relationship. However, when the mothers were asked, “Has the way you looked or thought about yourself changed while your daughter was participating in Smart Fit Girls?” the overwhelming response was “no.” This suggests that the intervention likely had neither “domino effect” nor influence on the mother/daughter relationship.
Due to the high prevalence of body dissatisfaction in adolescent girls (Abbott et al., 2012) and associated health consequences (e.g., depression, obesity, increased likelihood of eating disorders) (Byely et al., 2000; Johnson & Wardle, 2005; McCabe & Ricciardelli, 2001), it seems necessary for more research to be conducted to better understand girls’ body image. Even more pressing is the need to educate mothers on how to best communicate (both verbally and nonverbally) with their daughters about their own and their daughters’ body image. It is the authors’ hope that results from this study will advance the literature on the relationship between mothers’ and daughters’ body image as well as positively influence communities through the application of this study’s findings (e.g., creation of mother/daughter programs aimed at decreasing body dissatisfaction through improved communication).
Footnotes
Acknowledgements
The authors would like to acknowledge Esmeralda Castro for her assistance in the final stages of this manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.