
Abstract
Previous cross-sectional studies have shown that exposure to cleaning chemicals among health-care workers (HCWs) is associated with respiratory disorders and ventilatory function changes. This study aimed to further explore this association using a longitudinal approach. A prospective 2-year follow-up study was carried out at a tertiary care hospital in Saudi Arabia from June 2012 to June 2014 among 56 nurses who were responsible for disinfection and sterilization of medical instruments and equipment. The workplaces of the participants were assessed for engineering, environmental, and safety control measures. Self-administered questionnaires were distributed to all participants to assess their exposure to cleaning chemicals and their medical history. Spirometric parameters were measured for all nurses in 2012 (baseline) and again in 2014 (follow-up). The prevalence of work-related respiratory symptoms did not increase significantly over this time. Among all the spirometric parameters, only forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio decreased significantly, and only 10.7% of participants who were exposed to cleaning chemicals for more than 10 years had FEV1 and FVC less than their longitudinal normal limits at the end of the study. Smoking and gender were associated with statistically significant decreases in some of the spirometric parameters. Our 2-year follow-up study did not demonstrate significant association between exposure to cleaning chemicals among HCWs and changes in the prevalence of work-related respiratory symptoms, but indicated early effects on ventilatory function among them. The study highlights the importance of periodic spirometry, proper work practices, and effective control measures to protect HCWs against potentially harmful workplace chemicals for disinfection and sterilization.
Introduction
Health-care facilities use different cleaning chemicals such as disinfectants and sterilants to protect patients from infectious diseases by maintaining the cleanliness of the hospital environment and sterilizing medical equipment and instruments (Arif and Delclos, 2012). Hence, the health-care professionals, especially nurses, are exposed to various cleaning chemicals during disinfection and sterilization of medical instruments and equipment (Arif et al., 2009; Dumas et al., 2012).
Most of the cleaning chemicals used in the health-care facilities are irritating to the mucous membranes and skin, such as bleach, ammonia, hypochlorite, and quaternary ammonium compounds (Quirce and Barranco, 2010). Also, they contain sensitizers such as aldehydes (glutaraldehyde, formaldehyde, and ortho-phthalaldehyde), chlorhexidine, and detergent enzymes (Adisesh et al., 2011; Gonzalez et al., 2014).
Different epidemiological studies have reported associations between exposure to cleaning chemicals and adverse respiratory health effects among health-care workers (HCWs), including ventilatory function abnormalities, irritant acute or chronic bronchitis and asthma, caused by either irritating or sensitizing effects of the chemicals (Dumas et al., 2012; Lipinska-Ojrzanowska et al., 2014; Siracusa et al., 2013; Smith and Wang, 2006). However, most of these studies are case reports and cross-sectional and case–control studies (Adisesh et al., 2011; Jaakkola and Jaakkola, 2006; Makela et al., 2011). Hence, we have conducted a 2-year prospective study aimed to assess changes in ventilatory function and the prevalence of work-related respiratory symptoms among a group of nurses exposed to cleaning chemicals in a tertiary-care hospital in Saudi Arabia.
Materials and methods
Study design
A prospective 2-year follow-up study was carried out at King Fahad tertiary care hospital (Saudi Arabia) from June 2012 to June 2014. The study included 60 out of 80 nurses who agreed to participate in the study and who were responsible for disinfection and sterilization of medical instruments and equipment including endoscopies. The exclusion criteria for the study were pregnancy and past history of asthma or other chronic respiratory disease before working directly with disinfection and sterilization of medical instruments and equipment.
The study was approved by the King Abdullah International Medical Research Center ethical committee and the participants provided a written consent to participate in the study.
Environmental and safety assessment
At the start of the study in 2012, the occupational exposure to the cleaning chemicals among the participants as well as their work practices and workplace environment were assessed by an expert team which included environmental and occupational health specialists. The assessment included (a) the different types and names of the cleaning chemicals that were used by the participants, (b) duration of work in disinfection and sterilization of medical instruments and equipment including daily exposure to the cleaning chemicals, (c) accessibility of the material safety data sheets (MSDSs) of the chemicals in their work places and if they were evaluated and approved by their hospitals, (d) proper labeling and appropriate hazard warning and signs for the cleaning chemicals, (e) wearing the proper personal protective equipment (PPE), (f) safety training on the use, storage, and emergency spill procedures for the cleaning chemicals, (g) the ventilation system at their work places, (h) availability of safety and emergency measures for rapid flushing or drenching of the eyes and body within their work places such as eyewash and body shower, (i) history of acute exposure to splashes and spills of the cleaning chemicals, and (j) if they were mixing different cleaning chemicals during the disinfection and sterilization process. In 2014, the same team conducted a reassessment for the above items and the results did not vary from the previous assessment done in 2012.
Respiratory questionnaire
A self-administered questionnaire based on the medical research council questionnaire on respiratory symptoms (Cotes, 1987) was distributed to all participants both in June 2012 and June 2014. The questionnaire consisted of questions on demographics, smoking history, medical history (e.g. work-related respiratory symptoms, chronic respiratory diseases, asthma, and allergies), and family history (e.g. atopy and asthma).
Spirometric measurements
Spirometric parameters including forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, and forced expiratory flow at 25–75% (FEF25–75) were measured for all participants before the morning shift in June 2012 and 2014 by two trained spirometry technicians using a MicroLoop portable spirometer (Micro Medical Ltd, Rochester, UK) according to the recommendations of the American Thoracic Society (Redlich et al., 2014). All variables were also converted into the percentage predicted value for each person with the equations integral in the spirometer. The tests that were carried out in 2012 and 2014 were done by the same spirometry technicians who were trained on using spirometer to measure ventilatory function. Longitudinal normal limit (LNL) of FEV1 and FVC (from 2012 to 2014) was calculated for each participant according to the American College of Occupational and Environmental Medicine (ACOEM) (Townsend, 2011) and based on the American Thoracic Society recommended year-to-year decline limit of 15% considering the predicted age-related decline over years (Redlich et al., 2014). According to Hnizdo (2012), LNL is defined in terms of a critical value below which a longitudinal measurement should not fall from the baseline FEV1 (FEV1b) or the baseline FVC (FVC1b) values, using following equations:
Statistical analysis
Data were entered and analyzed using Statistical Package for the Social Science (SPSS), version 17.0. Qualitative data were presented as frequencies and percentages while quantitative data were presented as means and standard deviation (SD). Work-related respiratory symptoms in 2012 and 2014 were statistically analyzed using the McNemar test. Spirometric parameters in 2012 and 2014 were statistically analyzed using the paired t-test for all participants according to smoking and gender. The participants who had FEV1 and FVC values below their corresponding LNL (from 2012 to 2014) were presented as numbers and percentages.
Results
Out of the 60 nurses, 4 were excluded from the study (1 pregnant and 3 resigned before 2014). The remaining 56 nurses constituted our study participants.
Quaternary ammonium compounds were the cleaning chemicals used by most of the participants (92.9%) followed by chlorhexidine (87.5%) and then ortho-phthalaldehyde (78.6%). About half of the participants were exposed to gluteraldehyde and about quarter of them were exposed to formaldehyde and sodium hypochlorite bleach. Endozyme® exposure was reported by 19.6%, and only 8.9% of them were exposed to ethylene oxide. The mean daily exposure time to cleaning chemicals was 5 ± 1.5 h (range 2–7 h; these data were not tabulated).
The mean age of the participants was 43.00 ± 7.19 and most of them were males; 71.4% (40/56) were nonsmokers and the rest were current smokers (28.6%). More than half of them were exposed to cleaning chemicals for more than 10 years. The body mass index) of all participants did not change significantly from 2012 to 2014 (Table 1).
Demographic criteria of 56 nurses exposed to cleaning chemicals, a 2-year follow-up study (2012–2014).
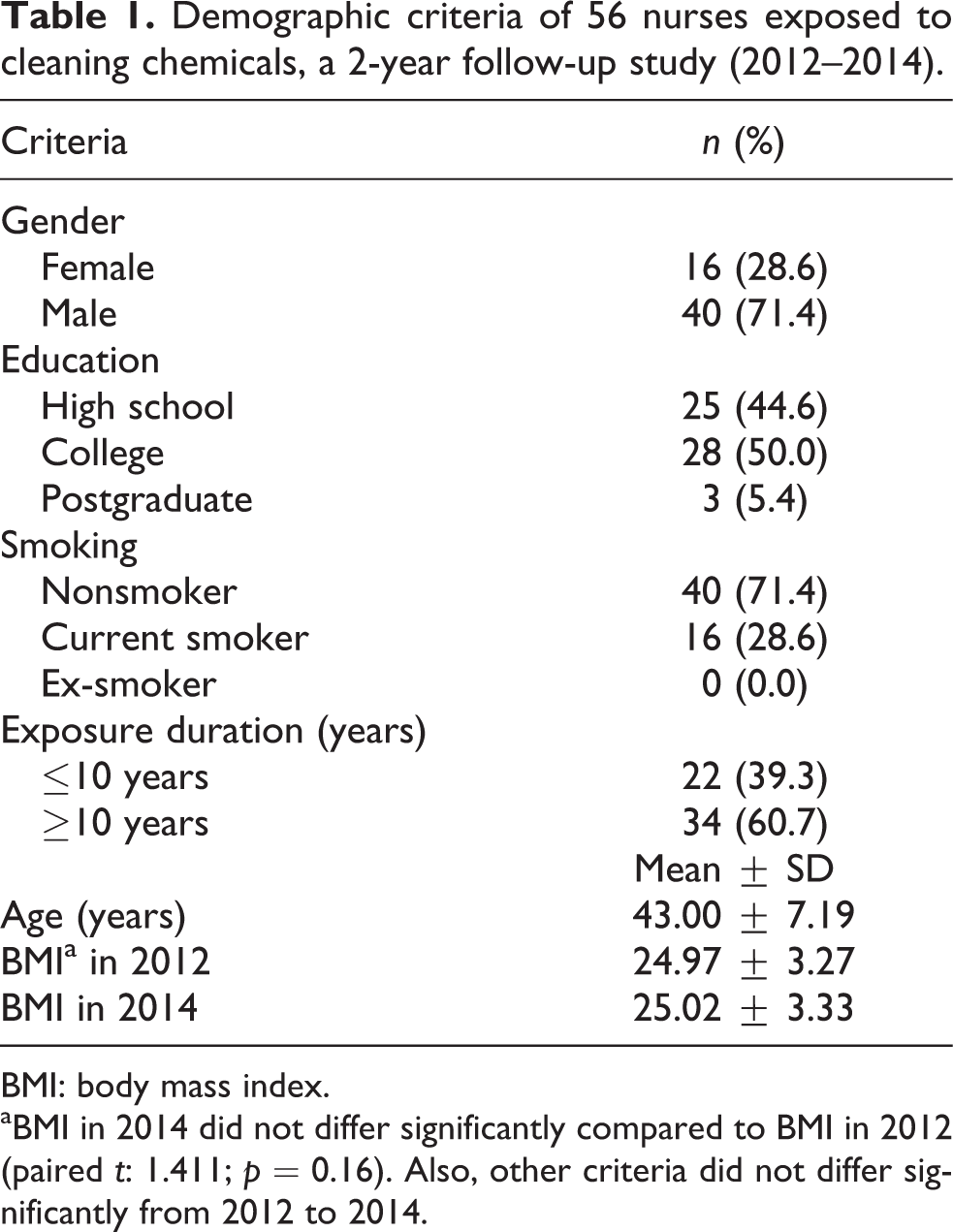
BMI: body mass index.
aBMI in 2014 did not differ significantly compared to BMI in 2012 (paired t: 1.411; p = 0.16). Also, other criteria did not differ significantly from 2012 to 2014.
While using cleaning chemicals, most of the participants (89.3%) were wearing PPE and 73.2% were trained on the use, storage, and emergency spill procedures for these chemicals. Also, most participants worked in areas with negative ventilation (96.4%) and suitable facilities for quick drenching or flushing of the eyes (89.3%). All of them reported that the cleaning chemicals they used were evaluated and approved by their hospital administration and were properly labeled. Most participants reported that MSDSs for the cleaning chemicals they used were readily accessible during their work shifts. Only 3.6% of the participants reported exposure to splashes and spills during use of cleaning chemicals and 16.1% of them were exposed to mists, vapors, or gases while using the cleaning chemicals. Also, 17.9% of the participants were mixing different cleaning chemicals during cleaning processes (Table 2).
Evaluation of ventilation and preventive measures among 56 nurses exposed to cleaning chemicals, at the start of the study in 2012.
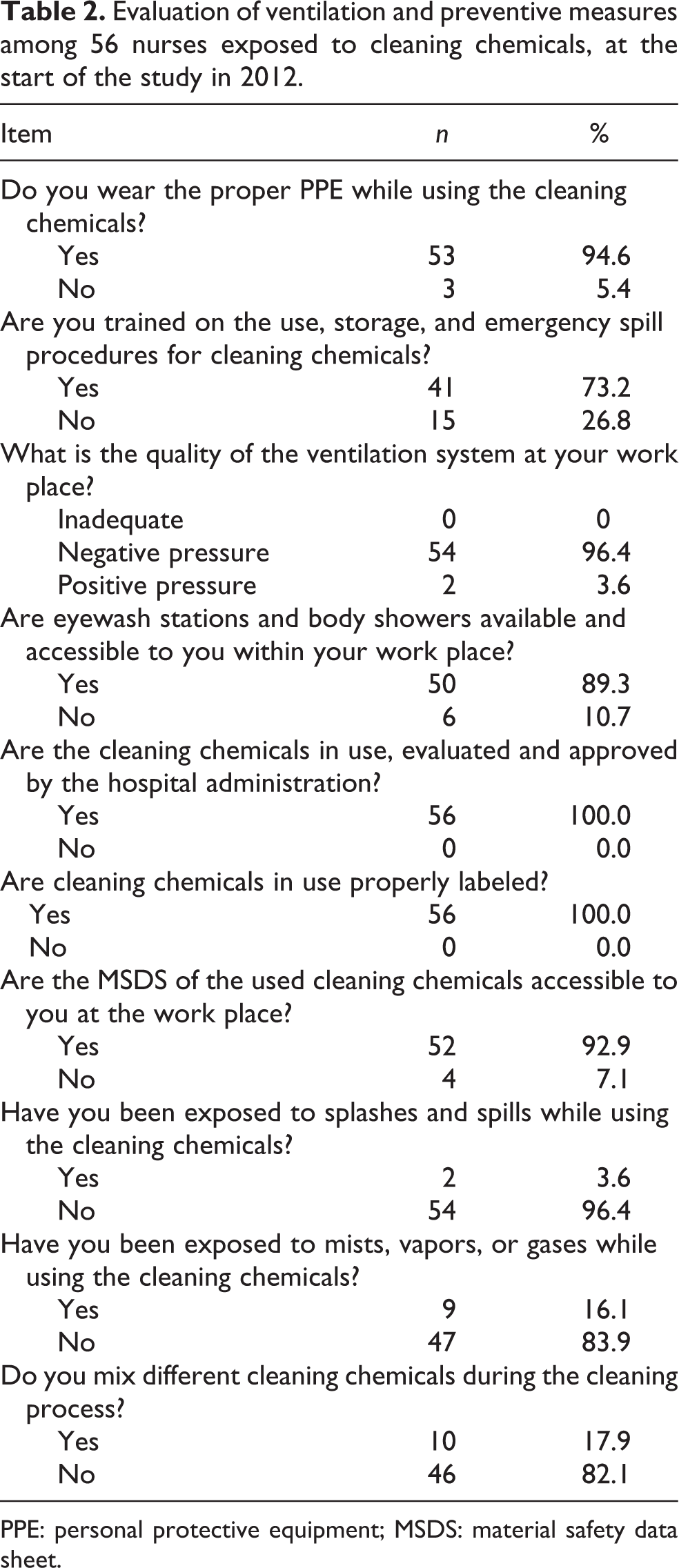
PPE: personal protective equipment; MSDS: material safety data sheet.
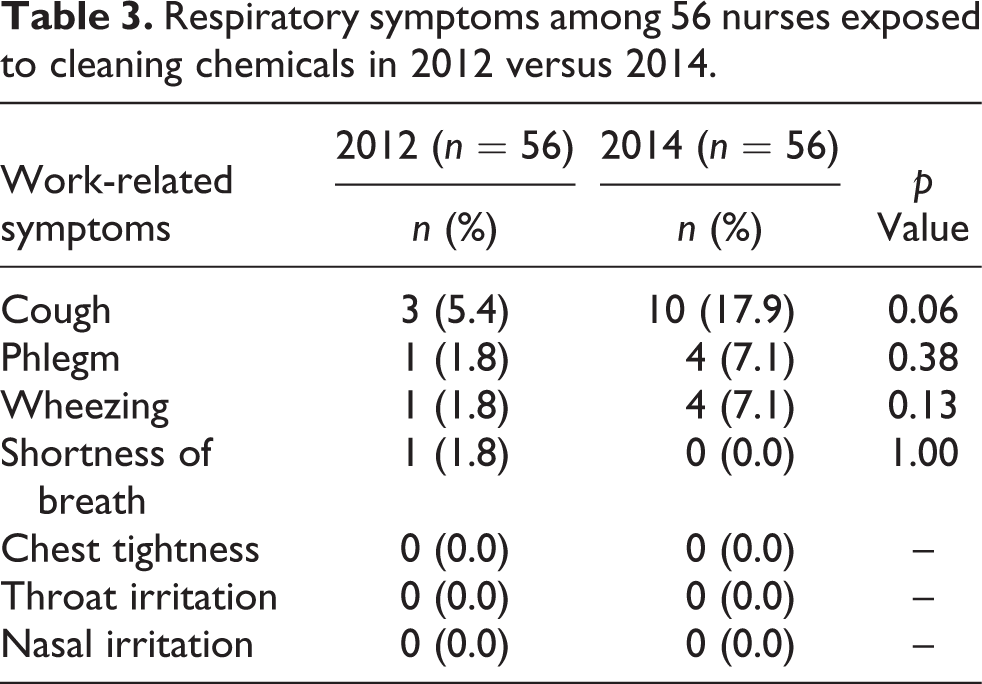
Work-related cough was the most common respiratory symptom (5.4%) among the participants in 2012 and its prevalence increased to 17.9% in 2014 with borderline significance (p = 0.06). The prevalence of both work-related phlegm and wheezing changed from 1.8% in 2012 to 7.1% in 2014, but the difference was statistically insignificant. Only one participant had shortness of breath in 2012 and none of the participants reported chest tightness, throat irritation, or nasal irritation either in 2012 or 2014 (Table 3).
Respiratory symptoms among 56 nurses exposed to cleaning chemicals in 2012 versus 2014.
Among all the participants, FEV1, FVC, FEV1/FVC ratio, and FEF25–75 in 2014 appeared to be decreased compared with 2012; however, the only difference that was statistically significant was for the FEV1/FVC ratio. All participants who had worked with cleaning chemicals for more than 10 years (60.7%) had significant decreases in FEV1, FVC, and FEV1/FVC from 2012 to 2014; however, no such decreases were observed for those who worked with cleaning chemicals for less than 10 years. Moreover, from 2012 to 2014, only 2 (3.6%) participants had FEV1 less than their LNL, and only 4 (7.1%) had FVC less than their LNL. All of these 6 (10.7%) participants were exposed to cleaning chemicals for more than 10 years. However, none of the participants exposed to cleaning chemicals for less than 10 years had FEV1 or FVC less than their LNL (data were not tabulated). Current smoking among the participants was associated with statistically significant decreases in FEV1, FEV1/FVC, and FEF25–75, from 2012 to 2014. Female gender was associated with statistically significant decreases in FEV1 and FVC from 2012 to 2014; male gender was associated with significant decreases only in FEV1/FVC ratio (Table 4).
Spirometric parameters of 56 nurses exposed to cleaning chemicals in 2012 versus 2014.
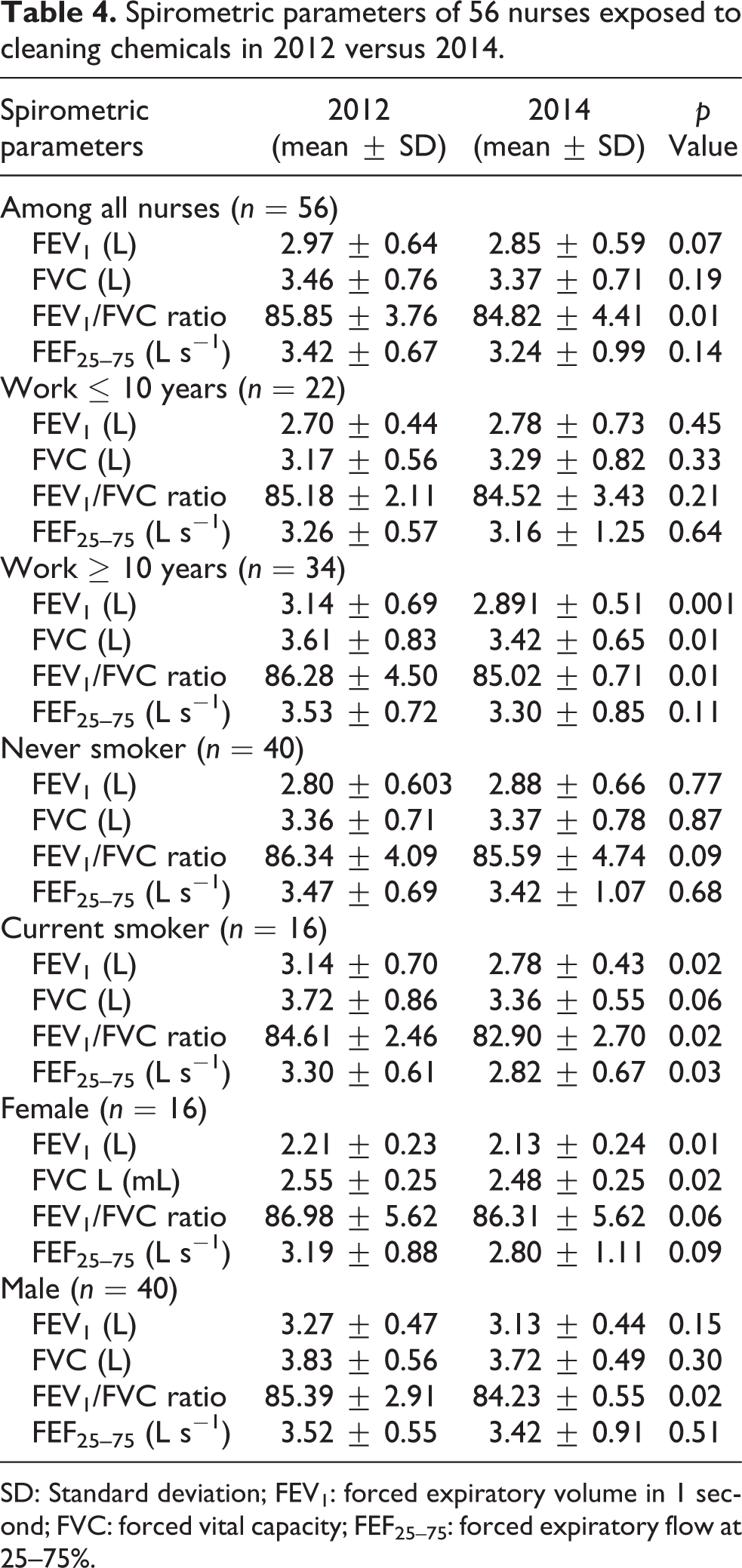
SD: Standard deviation; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; FEF25–75: forced expiratory flow at 25–75%.
Discussion
The result of this follow-up study did not demonstrate significant increases in the prevalence of work-related respiratory symptoms among the study participants who were exposed to cleaning chemicals. Concerning the spirometric changes, only the FEV1/FVC ratio showed a significant decrease among the participants from 2012 to 2014.
We studied the engineering and environmental control measures in addition to safety measures at the workplaces where the participants used cleaning chemicals. Based on the results of this study, it was noticed that most of the nurses worked with cleaning chemicals at well-ventilated workplaces with proper engineering and environmental controls and available safety measures. This may explain why apparent increases in work-related respiratory symptoms during the study period were minimal to insignificant. Hence, our study confirms the importance of engineering and environmental control measures to protect the health of HCWs while using the cleaning chemicals that might cause occupational respiratory disease such as asthma. This is in agreement with other studies (Gonzalez et al., 2014; Nayebzadeh, 2007; Siracusa et al., 2013; Tarlo and Liss, 2010).
In occupational settings, the purpose of periodic spirometry for workers is to detect any changes in lung function over time compared to LNL, to prevent work-related respiratory injuries, and to maintain workers’ general health (Hnizdo et al., 2011; Redlich et al., 2014). Periodic spirometry is a more useful tool in preventing work-related decreases in ventilatory function than a single spirometry test (Hnizdo, 2012), that is because using a single spirometry test, a worker with lung function values equal to or greater than their lower limit of normal, may show lung function decline with periodic spirometry monitoring (Hankinson and Wagner, 1993). Based on that, we used longitudinal spirometry approach in the present study to monitor the change in the lung functions of a sample of HCWs exposed to cleaning chemicals during 2-year follow-up period as ACOEM recommends that spirometry should be conducted every 1–2 years when indicated because of workplace exposures (Townsend, 2011). However, increasing the follow-up time increases the accuracy of identifying the rate of lung function change (Hnizdo et al., 2011; Townsend, 2005; Wang et al., 2006).
Although the follow-up period of our study was 2 years, FEV1/FVC ratio was the only spirometric parameter that decreased significantly. Moreover, 10.7% of nurses had FEV1 and FVC less than their LNL after 2 years of the start of the study. These results may indicate early effects on lung function associated with exposure to cleaning chemicals, which indicate the importance of periodic spirometry for monitoring HCWs exposed to cleaning chemicals as a secondary preventive measure (Tarlo and Liss, 2010). Smoking and gender were also associated with decreases in some of the spirometric parameters among the participants and this was also reported by other studies (Dumas et al., 2012; Lipinska-Ojrzanowska et al., 2014). Among our participants, being female was associated with a significant decrease in FEV1 and FVC and a nearly significant decrease (p = 0.06) in FEV1/FVC ratio, from 2012 to 2014; however, being male was associated only with a significant decrease in FEV1/FVC ratio. This is in agreement with Lipinska-Ojrzanowska et al. (2014), who reported that gender is considered a risk factor for occurrence of respiratory symptoms during cleaning activities and that gender differences may explain greater airways susceptibility to nonspecific stimuli in women than in men (Obadia et al., 2009), which may be related to different geometry of airways and difference in cholinergic irritability and many hormonal factors, as explained by Paoletti et al. (1995).
In the present study, most of the cleaning chemicals used by the participants were less sensitizing agents, such as, quaternary ammonium compounds, chlorhexidine and ortho-phthalaldehyde, which are widely used in health-care settings (Bello et al., 2009; Gonzalez et al., 2014), frequently to replace aldehydes (Gonzalez et al., 2014). In addition, ortho-phthalaldehyde is considered an effective alternative to glutaraldehyde for the disinfection of endoscopes (Franchi and Franco, 2005). This change avoids the sensitizing effects of glutaraldehyde (Nayebzadeh, 2007), which was used by an estimated quarter of the participants as a disinfectant for endoscopes.
In spite of the relatively short period of our study, the results indicated some early effects on certain spirometric parameters among nurses who were exposed to cleaning chemicals despite the engineering, environmental, and safety measures that were in place. Hence, our study highlights the importance of periodic examination including periodic spirometry and respiratory questionnaires for early diagnosis of respiratory diseases among HCWs exposed to cleaning chemicals.
Our study has certain limitations including a relatively small sample size and a short period of follow-up, no controls were selected and no air monitoring was conducted for the cleaning chemicals used by the participants at their workplaces. Also, we did not assess the sensitizing effect of the cleaning chemicals among the examined HCWs such as measuring general and specific serum immunoglobulin E.
Conclusion
Our 2-year follow-up study indicated early effects on ventilatory function among HCWs exposed to cleaning chemicals. Additionally, the study confirms the importance of strict engineering, environmental, and safety control measures and proper work practice to keep them safe and healthy. The study also highlights the importance of ongoing medical surveillance including periodic respiratory questionnaires and spirometry to detect any changes in lung function or presence of respiratory diseases for early intervention. Health education and smoking cessation programs should be conducted to prevent the combined effects from smoking and exposure to cleaning chemicals on ventilatory function in this worker population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.