
Abstract
The tongue-in-groove technique in endonasal rhinoplasty is a commonly used method for making changes in tip rotation and projection. We examine the outcomes of absorbable and permanent suture tongue-in-groove technique in relation to maintaining postoperative tip rotation and projection. A retrospective review of the preoperative and postoperative photographs of 18 patients treated with endonasal tongue-in-groove technique were analyzed. Twelve patients were treated with nylon suture and 6 with polydioxanone suture (PDS). There were 9 females (50%) and 9 males (50%), with the age ranging from 17 to 49 years. The mean follow-up time was 12.1 months. All patients were treated by the senior author in a New York City hospital. All patients were treated with the tongue-in-groove technique in endonasal rhinoplasty; 5.0 clear Nylon suture was used on 12 patients and 5.0 clear PDS on 6 patients. Using an unpaired t test and an alpha value of 0.05, the difference between the preoperative and postoperative tip rotation and projection was statistically significant for nylon (P = .0069, P = .026) but not for PDS (P = .27, P = .15). Using permanent suture in tongue-in-groove technique during endonasal rhinoplasty seems to be a more reliable method for maintaining postoperative changes in tip rotation and projection.
Introduction
The tongue-in-groove (TIG) technique, first described by Rethi in 1934, has been widely used in the treatment of various nasal deformities. 1 This technique involves the cephalad repositioning of the medial crurae onto the caudal septum and can be used in both endonasal and open rhinoplasty. Originally described for the treatment of an elongated nose, success with the technique has now been reported for treating alar-columellar disharmony, as well as the improvement in tip rotation and projection.1,2
Suture choice has been an ongoing debate among rhinoplasty surgeons as permanent and absorbable sutures come with certain advantages and disadvantages. The ease of placement of an absorbable suture for TIG made it a preferred option initially when performing this technique via endonasal approach. In addition, absorbable sutures have the advantage of being resorbed, thus leading to a lower incidence of infection or extrusion, whereas permanent sutures, although not commonly, do have the theoretical risk of suture extrusion or infection. When dissolved, the structures originally bonded by an absorbable suture are supported only by the forces of fibrosis, which may or may not be sufficient enough to provide a reliable surgical outcome as time progresses. On the contrary, permanent sutures are not affected by the local environment and generally maintain their position and the level of structural support.
To date, we are not aware of any studies in the English literature examining outcomes of TIG technique performed with absorbable versus permanent sutures. In this article, we examine the long-term postoperative changes in tip rotation and projection in patients treated with TIG endonasal rhinoplasty with absorbable suture versus a permanent suture. The goal of the study is to compare the postoperative outcomes of absorbable and permanent suture material in maintenance of tip rotation and projection.
Methods
Approval was received from the New York Eye and Ear Infirmary Institutional Review Board (IRB) prior to conducting the study. We retrospectively identified 18 patients treated with TIG endonasally: 12 patients had TIG procedure using permanent (5-0 clear Nylon) suture and 6 patients had TIG procedure using absorbable (5-0 clear polydioxanone suture [PDS]) suture. Most of these patients had other rhinoplasty components performed at the same time, such as dorsal hump reduction, osteotomies, or septoplasty, but no other tip-modifying techniques were carried out except TIG. There were 9 males (50%) and 9 females (50%) in this group; all of the patients were treated by the senior author from 2008 to 2013 at an academic hospital in New York City. The patients’ age ranged from 17 to 49 years, and the follow-up ranged from 3 to 53 months, with a mean follow-up of 12.1 months.
Surgical Technique
Following intubation and sterile preparation, patients were decongested using oxymetazoline-soaked pledgets. A preoperative photography was taken at this time to serve as a baseline prior to surgery (Figure 1A). Using digital manipulation, the columellar was cephalically advanced to demonstrate the degree of change needed to effect results (Figure 1B). Local anesthetic using 1% lidocaine with epinephrine 1:100,000 was injected in a standard fashion. A full transfixion and intercartilaginous incisions were made, exposing the caudal septum and nasal dorsum. Bilateral submucoperichondrial septal flaps were elevated exposing caudal aspect of the septal cartilage. If required, dorsal refinements, osteotomies, and septoplasty were performed at this point. The intercrural pocket was then dissected between the medial crurae of the lower lateral cartilages using tip scissor (Figure 1C). In cases of using a permanent suture for TIG, two incisions on each side of the lateral aspects of the columella through the columellar skin but not through the medial crural cartilages were made to bury Nylon sutures (Figure 1D). The incisions were approximately 2 to 3 mm in length. The columella was then manually inset onto the caudal cartilaginous septum in a manner as to achieve a desirable change in either the tip projection or tip rotation, or both. Two horizontal mattress sutures using either 5-0 Nylon or 5-0 PDS were placed to suture the medial crurae onto the caudal cartilaginous septum (Figure 1E and 1F). When using Nylon suture, the suture was buried within the previously made lateral columellar incisions; the PDS suture was placed through and through the columella in a horizontal mattress fashion and tied over the skin. Care was taken to ensure the symmetric placement of the mattress sutures on each side of the columella to avoid any postoperative columellar and tip asymmetries. Including the caudal septal cartilage into the TIG mattress suture is crucial as caudal septum serves as the main support for the resultant tip changes. This was ensured either by direct visualization of the suture passing through caudal septal cartilage or by pulling on the suture and observing for the mobility of the columella: Pulling on the suture that indeed passed through the caudal septal cartilage would not pull the columella away from the septum, and vise versa. The sutures were then tightened, and the resultant tip changes and symmetry were evaluated. In case of dissatisfaction, one or both mattress sutures can be redone until the desired result is achieved on the table. The excess membranous septum that commonly results from this maneuver is trimmed conservatively (Figure 1G). Full transfixion and intercartilaginous incisions were closed using 5.0 chromic suture. The columellar incisions do not typically require any closure; however, these can be sutured with 6.0 fast absorbing gut if desired. A final postsurgical photograph was taken at this time (Figure 1H). The nose is then taped and splinted with Aquaplast in a routine fashion.
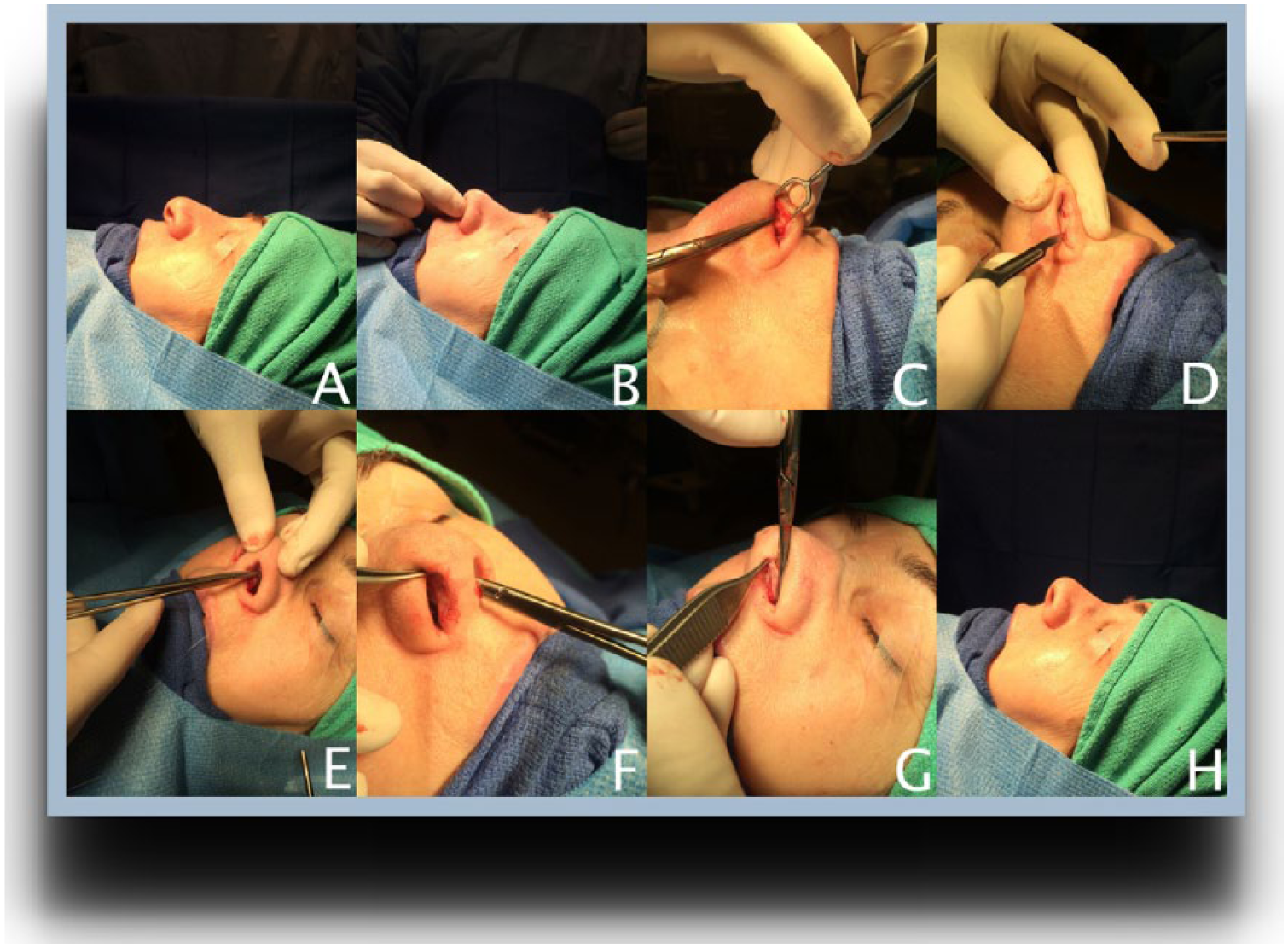
Tongue-in-groove procedure. (A) Preoperative photograph of the patient prior to making incisions. (B) Manually advancing the columella to assess the projected change by the tongue-in-groove maneuver. (C) Dissection of intracrural pocket following full transfixion and intercartilaginous incisions. (D) Two incisions are made lateral to the columella to bury the horizontal mattress sutures after securing the medial crurae onto the septum. (E) Horizontal mattress suture placed to secure the medial crurae onto the septum. (F) Horizontal mattress suture placed to secure the medial crurae onto the septum. (G) After securing medial crurae, excess vestibular mucosa is trimmed. (H) Final result displayed following completion of tongue-in-groove technique.
Analysis
Preoperative and postoperative photographs were taken using Kodak D100 digital SLR camera. Using computer analysis software, the nasolabial angle and the Goode ratio were calculated in a standardized fashion for all preoperative and postoperative photographs.
An unpaired t test using an alpha value of 0.05 was used to compare the mean of the preoperative rotation with the postoperative rotation, as well as the mean of the preoperative Goode ratio with the postoperative Goode ratio for each suture type to test for statistical differences.
Results
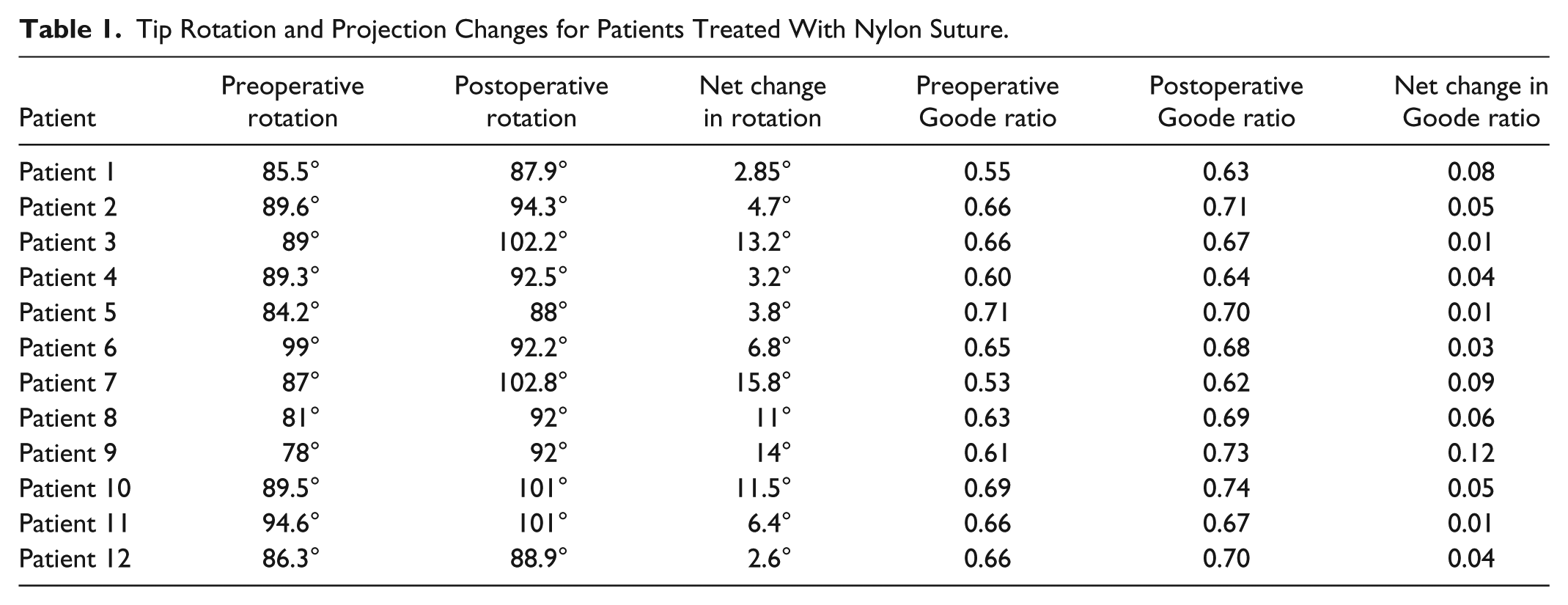
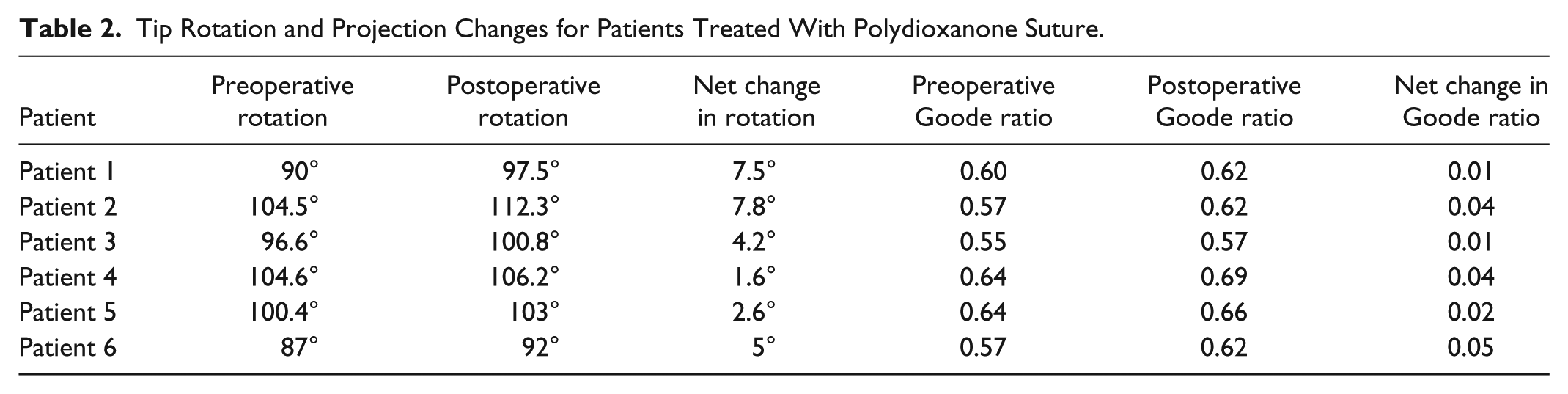
Table 1 shows patients treated with permanent (5-0 clear Nylon) suture, and Table 2 shows patients treated with absorbable (5-0 PDS) suture. Both tables demonstrate preoperative and postoperative tip rotation and projection along with corresponding net changes in both.
Tip Rotation and Projection Changes for Patients Treated With Nylon Suture.
Tip Rotation and Projection Changes for Patients Treated With Polydioxanone Suture.
For patients treated with permanent suture, the mean preoperative tip rotation was 87.7 degrees while the mean postoperative tip rotation was 94.5 degrees. The postoperative improvement in tip rotation was found to be statistically significant in this group (P = .0069). Individually, each patient in this group has shown certain degree of improvement in tip rotation. There were no patients in this group in who tip rotation remained unchanged or decreased postoperatively. The mean preoperative Goode ratio was 0.64 and mean postoperative Goode ratio was 0.68; this difference was also statistically significant (P = .026).
Examining the group treated with the absorbable suture, the mean preoperative tip rotation was 97.1 degrees and the mean postoperative rotation was 101.9 degrees, which was not statistically significant (P = .27). The mean preoperative Goode ratio was 0.60 and the mean postoperative Goode ratio was 0.63. These values were also not found to be significantly different (P = .15).
Discussion
The TIG technique is an effective method for correcting excessive columellar show, improving tip rotation and projection, and improving support of the nasal tip.3,4 This technique affords decreased operative time, predictable and reliable results, and increased tip stability. In a study of 2286 patients treated with the TIG technique, also known as the septocolumellar suture, 98% of patients were noted to have a satisfactory improvement in tip projection and rotation. The authors of the study reported that successful use of the septocolumellar suture is influenced by straightness of the caudal septum, as well as the height, length, and thickness of the septum. The septocolumellar suture counteracts downward forces on the nasal tip acted on by upper lip movements. 5
To date, there has been extensive debate among surgeons regarding the use of various suture materials in rhinoplasty. In the English literature, there are no known studies examining rhinoplasty results based on suture type. To our knowledge, this is the first study examining postoperative outcomes in patients treated with the TIG technique in endonasal rhinoplasty comparing the use of nylon suture and PDS.
Although studies examining suture materials are not present in the rhinoplasty literature, several studies examining suture materials in otoplasty and microtia repair do exist. In a 2012 study of 122 patients who underwent auriculoplasty for microtia, Sakamoto et al reported 2 patients treated with nylon suture who experienced suture exposure and deformation of the inferior helix from suture loosening. As such, they recommended the use of an absorbable suture such as PDS for fixation of the cartilage framework. 6 Iamphongsai et al in 2009 studied long-term otoplasty outcomes in rabbits treated with permanent and absorbable suture. In their study of 36 rabbits, otoplasty was performed with nylon suture in the right ear, while the left ear was repaired with an absorbable suture such as PDS, monocryl, or plain gut. At a follow-up of 3 months, the cartilage folds were harvested and analyzed. They reported that nylon was superior to plain gut or monocryl; however, no differences in nylon and PDS were found. Based on their results, they recommend the use of either nylon or PDS for cartilage reshaping and do not feel that one is superior to the other. 7
The obstetrics and gynecology (OBGYN) literature has examined suture use for the closure of fascial defects in cesarean section. A 2014 study by Rezaie Kahkhaie et al examined 120 women who underwent cesarean section; 60 of these women were repaired using nylon and 60 repaired with an absorbable suture such as PDS. Comparing both groups, there was no difference in hernia, wound dehiscence, or wound infection. The group closed with nylon reported more incisional pain than the PDS group. Overall, they recommended the use of an absorbable suture for closure of fascial defects to minimize postoperative pain. As this study examined fascial closure as opposed to cartilage approximation, the reader can appreciate the similarity in outcome but must keep in mind the possibility of variation in the healing on various tissue types. 8
With more widespread application of TIG in closed rhinoplasty surgery, the technique was initially more commonly performed using absorbable sutures, such as PDS or Chromic gut. The most plausible explanations of this suture type selection, in our opinion, were the ease of placement of an absorbable suture through the columella without the need to burry the suture, avoiding potential complications related to the use of a permanent suture material such as infection or extrusion, and a belief that TIG creates sufficient degree of scarring and fibrosis to adequately resist gravitational forces affecting nasal tips over time.
In our study, we examined a total of 18 patients, 12 in whom Nylon suture was used and 6 in whom PDS suture was used. Our results suggested that in patients treated with Nylon suture, the postoperative rotation and Goode ratio were both significantly improved compared with the preoperative (P = .0069, P = .0026). In the group treated with PDS suture, these preoperative and postoperative results were not significantly different (P = .27, P = .15). Our findings suggest that the use of a permanent suture may be more efficacious in providing an improved and lasting change in tip rotation and projection. It is reasonable to consider that the resorption of the PDS suture may lead to results which are not significantly different from the preoperative. Moreover, the resulting fibrosis may not provide sufficient tip support to maintain the immediate postoperative changes over time.
In conclusion, the TIG technique is an effective and reliable way to change nasal tip rotation and projection while maintaining or improving tip support. Our results suggest that the use of a permanent (nylon) suture may be a more effective and reliable option than the use of an absorbable suture (PDS) in achieving long-lasting changes in tip rotation and projection when used in the TIG technique in endonasal rhinoplasty. The results of this study indicate that the forces of scarring and fibrosis alone may not be sufficient enough to withstand gravitational forces invariably affecting nasal tip over time. The tensile strength of a permanent suture may be a necessary component in assuring longevity and reliability of the TIG procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.