
Abstract
The measurements of beautiful buttocks have varied according to patient preference, different cultures, and ethnicity. There are great differences in the ideal aesthetic measurements of the buttocks among ethnic groups. In this work, the authors introduce an easy and versatile method for the assessment of “Gluteal-Related Aesthetic Subunits.” This method works as a tool to perform liposuction and lipoinjection, to treat the variety of differences in patients’ racial, cultural, personal preferences, and ethnic-related demands, thus improving the results of gluteal aesthetic surgery. This study was carried out on 148 patients, at plastic and reconstructive surgery department, Tanta University hospitals, and in private practice, in the period between 2010 and 2018. The aesthetic assessment and surgical planning were performed according to the criteria suggested by the authors of this work. Patient’s satisfaction showed excellent results in 104 (70.2%) patients, good results in 39 (26.4%) patients, fair results in 5 (3.4%) patients, and no poor results. Clinical assessment showed excellent results in 96 (64.8%) patients, good results in 44 (29.7%) patients, fair results in 8 (5.5%) patients, and no poor results were reported. (1) We believe that this classification of buttock areas is a valuable step that could help in achieving the required results that are more satisfactory to different types of patients. (2) Despite all the merits of this analytical tool and the advantages of the innovations in liposuction, some limitations remain. Fat transfer alone will not treat and even may worsen ptosis.
Introduction
The buttock is considered as one of the symbols of female beauty. Currently, the patient demand to improve the form and size of the gluteal region is increased. 1 The measurements of beautiful buttocks have varied according to patient preference, different cultures, and ethnicity. 2 The aesthetic attractiveness of a small waist and full buttocks is not a new concept, as these characters have been identified by many cultures and ethnicities. 3 Wong et al 4 considered the ideal waist-to-hip ratio as 0.6 and 0.65 compared with the previous 0.7, which was representing the ideal ratio. As a result of the new fashion trends, there is increased interest in gluteal augmentation, but this procedure is not without risk.5,6
In the earliest attempts of gluteal augmentation, breast implants were used, but a lot of complications occurred, such as dislocation, asymmetry, and capsular contracture, and the aesthetic outcomes were not satisfactory. These stimulated surgeons to search for a better technique. 7
Currently, plastic surgeons have numerous techniques for gluteal enhancement that can be broadly classified into 3 categories, including the use of implants (sub-fascial, sub-muscular, and intramuscular placements), autologous flap augmentation, and autologous fat transfer, which has been dramatically increased in popularity in recent years. 8 - 10
A proper scientific method to define the beautiful gluteal area was not reported until the study of Cuenca-Guerra and Quezada. 9 Centeno focused on the relations of the aesthetic subunits that surround the gluteal region and their effect on the aesthetics of the gluteal area itself. He recommended that the subunits must be analyzed before the performance of any type of gluteal augmentation surgery, to achieve the best results. He mentioned 8 areas (2 symmetrical “flank” areas, 1 “sacral triangle” area, 2 symmetrical gluteal areas, 1 “infra-gluteal diamond” area, and 2 symmetrical posterior thigh areas). 11
Mendieta 12 gave a simple classification for buttock shapes (round, A-shaped, V-shaped, square shaped and intermediate) and gave another classification for buttock ptosis. Mendieta 13 also defined 5 zones that directly surround the buttocks and determine its aesthetics, namely, the sacrum V-zone, flank, upper buttock, lower back, and outer thighs.
In this work, the authors introduce a modified extension to the work of Centeno and Mendieta for the assessment of “Gluteal-Related Aesthetic Subunits.” This method works as a tool to perform liposuction and lipoinjection, to treat the variety of differences in patients’ racial, cultural, personal preferences, and ethnic-related demands, thus improving the results of gluteoplasty.
Patients and Methods
This study was carried out on 148 patients, at plastic and reconstructive surgery department, Tanta University hospitals, and in private practice, in the period between 2010 and 2018.
Criteria for Patient Selection
Inclusion criteria
This study included all patients asking for gluteoplasty at different ages.
Exclusion criteria
The exclusion criteria included patients with blood disease coagulopathies, diabetic, unrealistic expectations, previous liposuction to the trunk area, and history of aesthetic enhancement of the gluteal area.
All Selected Patients Were Subjected to the Following
Complete history taking, including the use of hormonal drugs, history of previous interventions.
Condition-Specific Questions
Effect of the buttocks on general health, life style, and physical and social activity. All participants were subjected to general clinical examination to confirm their fitness for surgery. Informed consent forms were taken from all patients, including statements regarding scientific photography and the potential use of their data and photographs in scientific studies and publications. The aesthetic assessment and surgical planning were performed according to the criteria suggested by the authors of this work (Figure 1).
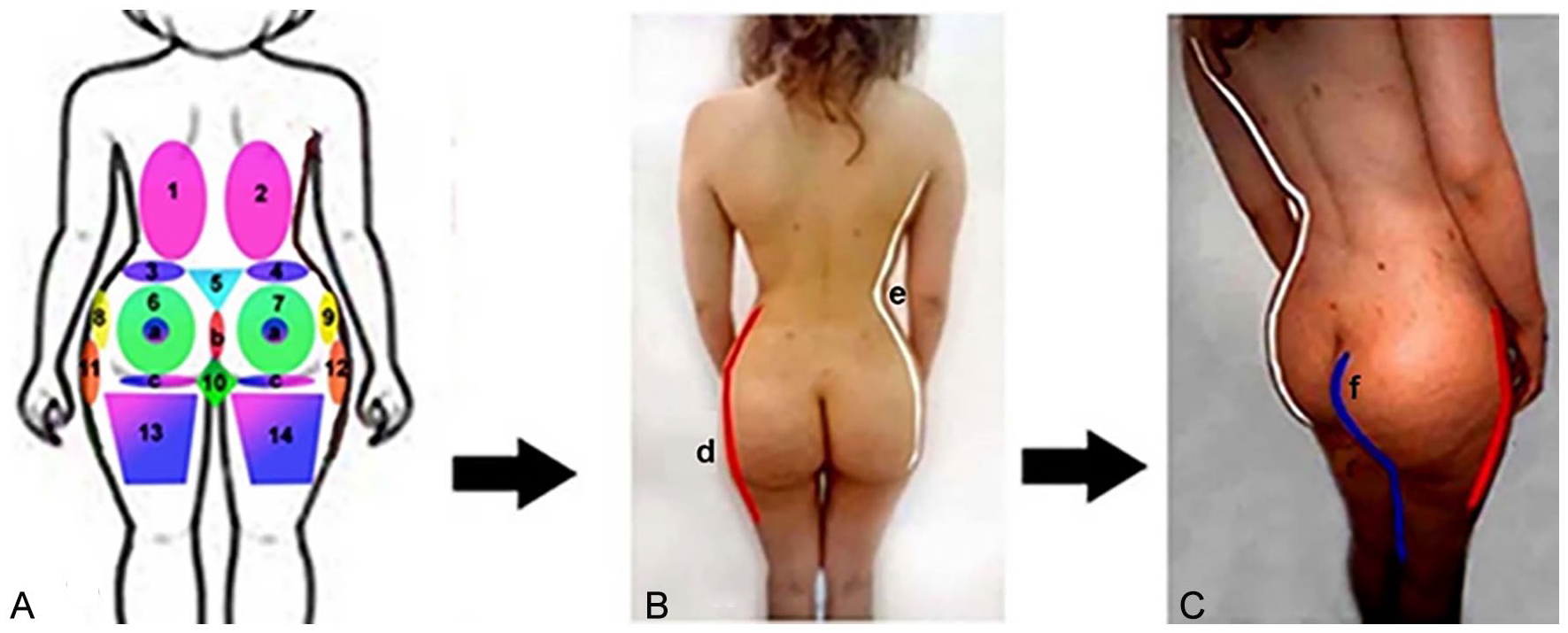
(A) Buttocks, and buttocks-related aesthetic subunits (areas), according to the plan adopted by the authors; areas 1 and 2 are the back; areas 3 and 4 are the flanks; area 5 is the sacral triangle: with its base superiorly with the line between the overt sacral dimples. Areas 6 and 7 are the proper buttocks. Areas 6 and 7 include a, b, and c, as described—“a”: overall fullness and location of the maximum projection point on the lateral view; “b”: the length of the intergluteal cleft; “c”: the infra-gluteal line. Areas 8 and 9 are the trochanteric areas. Area 10 is the infra-gluteal diamond area. Areas 11 and 12 are the lateral thighs and areas 13 and 14 are the posterior thighs. (B) and (C) The relationship between the aesthetic areas and the aesthetic curves of the buttocks, back, flanks, and thighs: the “d” curve, “e” curve, and “f” curve from the posterolateral view.
Operative steps
Under general anesthesia and complete aseptic technique, the operation was performed. The selected areas for liposuction were infiltrated using Klein 14 formula. Liposuction of the infiltrated areas was performed, using a 3-mm cannula. The aspirated Fat was left in sterile containers to be decanted. Fat was then transferred to a stainless-steel colander and washed repeatedly with normal saline till complete removal of any residual blood clots. Fat tissue was loaded into 20-mL syringes for transfer. The fat tissue was injected into the subcutaneous tissue of the buttocks using 4-mm gauge cannula with working length 15 cm, taking extreme care to avoid intramuscular injection.
The fat tissue was transferred to the buttocks according to the authors’ assessment criteria, the patient’s demands, or ethnic background. The liposuction ports were closed with 5/0 prolene. Immediately following the procedure, a special pressure garment was used by all patients for 3 months. The garment was designed to press over the liposuction areas and avoid the pressure over the lipoinjected areas.
Patients were instructed to perform limited activity and avoid pressure over the lipoinjection areas for 2 weeks.
Follow-Up Sheet
Follow-up of the patients after discharge from hospital was performed after 1 week, 1 month, 3 months, 6 months, and 1 year or more. The following information was reported after at least 3 months:
Aesthetic outcome data
Functional outcome data and aesthetic outcome data were documented. Unfavorable aesthetic outcome data such as the degree of projection and deformity changes were also reported. Symptomatic pain, difficulty in daily work, difficulty to find sleeping position, improvement in quality of life (physical life–social life), and degree of patient satisfaction were reported.
Patient’s satisfaction was evaluated according to the patient’s reported outcome measures (PROMs) which were questionnaires that measured the patient’s views of Satisfaction about the following parameters: aesthetic shape, life style, comments of relatives, and general satisfaction degree. The collected data were organized and tabulated. The patients were asked to rate their degree of satisfaction at a 4-point score of 1 (poor), 2 (fair), 3 (good), and 4 (excellent) which was used for evaluating each parameter.
Photographic documentations were taken pre-operatively and at the end of the first 6 post-operative months (posterior and lateral views). During the last follow-up visit, photographic session was performed and considered to be the post-operative photographic result as long as it was taken 6 months or more post-operatively.
Clinical satisfaction was performed by 3 plastic surgeons not sharing in this work; through a score from 1 to 4, the results of the pre-operative and last follow-up photography were assessed as excellent, good, fair, and poor.
Results
This study was carried out on 148 female patients. Their age ranged between 23 and 58 years old, with the mean age 32 years. The body mass index at the time of surgery ranged between 23 and 34 kg/m2 (mean 26.8 kg/m2). The whole procedure took about 3 hours with a mean of 2 hours. The follow-up period ranged between 1 and 7 years, with mean follow-up 1½ years.
All patients were treated with fat injection once. The minimal amount of liposuction was 1.2 L and the maximum were 4.6 L with a mean 2.45 L. The total volume grafted in each gluteal region ranged between 320 and 650 mL (mean 420 mL). The downtime varied from 10 to 14 days. There were no cases of infection; 9 patients (6.1%) suffered from seroma at the donor area. They were treated with needle aspiration with uneventful course.
All the adverse effects like pain and edema were transient and cleared completely on follow-up. No patient required hospitalization or a blood transfusion. There were no cases of sciatic neuropathy or painful parenthesis. There were no cases of fat embolism. Clinical assessment was performed by 3 plastic surgeons not sharing in this work, using 4-point scale. It showed excellent results in 96 (64.8%) patients, good results in 44 (29.7%) patients, fair results in 8 (5.5%) patients, and no poor results were reported.
Patient’s satisfaction was evaluated according to PROMs; 4-point scale was used. It showed excellent results in 104 (70.2%) patients, good results in 39 (26.4%) patients, fair results in 5 (3.4%) patients, and no poor results. Three patients (0.94%) complained of decreased buttock volume 5 months post-operatively but better than the pre-operative size, and 2 patients (1.88 percent) asked to decrease their lateral trochanteric size (score 2). All underwent additional surgery 6 months after the first surgery, reaching better degree of satisfaction. All patients reported great improvement in social life, social activity, and mood of the patient. In the early post-operative period, side-effects like difficulty in sitting, sleeping position, pain, edema, and ecchymosis were reported in all patients, but uneventful healing occurred within 2 weeks (Table 1 and Figures 2–7).
Descriptive Analytic Data of Different Variability in Age, Sex, Liposuction Volume, Lipoinjection Volume, Clinical Satisfaction, Patient Satisfaction. and Complications Encountered.
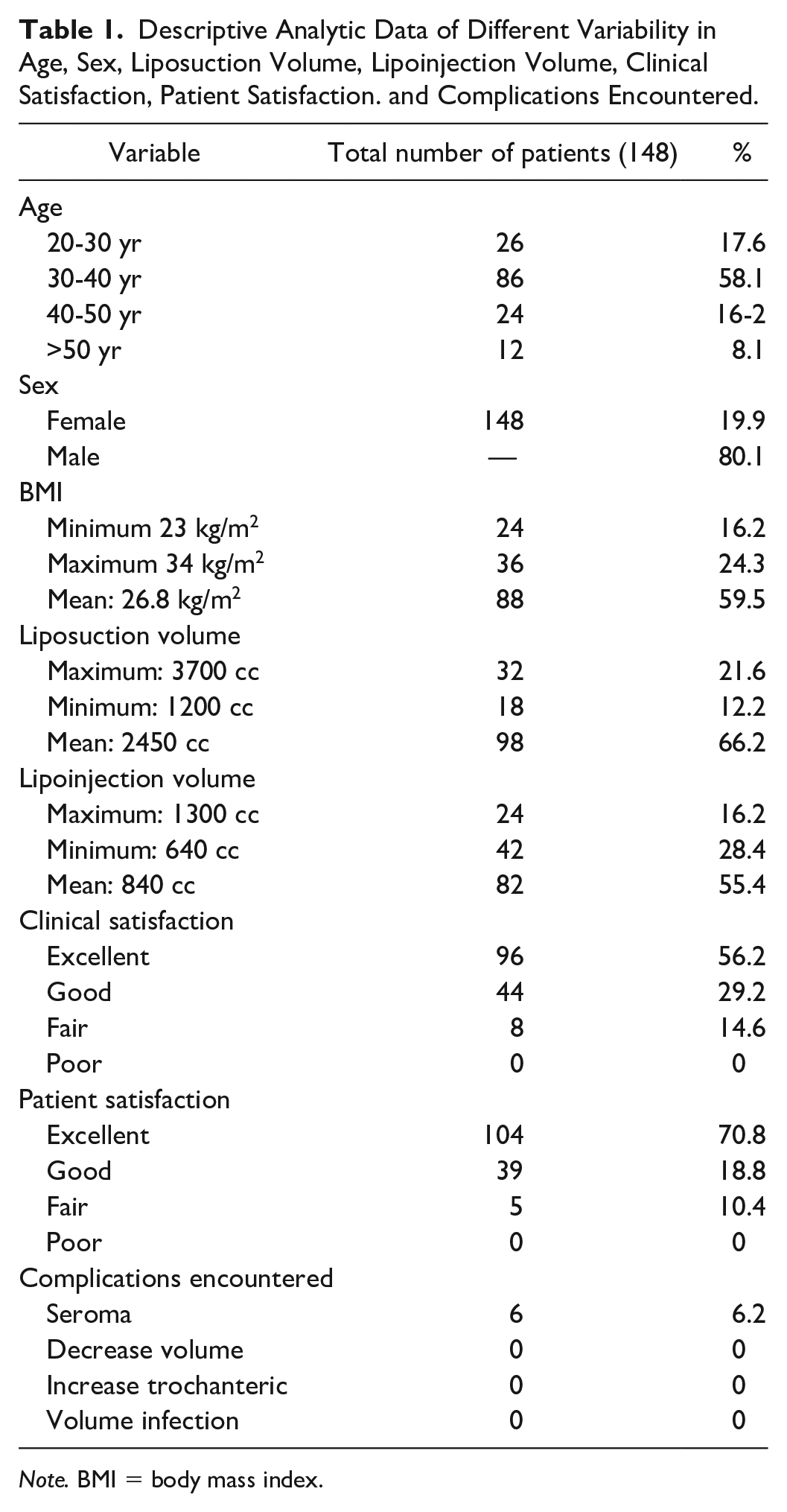
Note. BMI = body mass index.
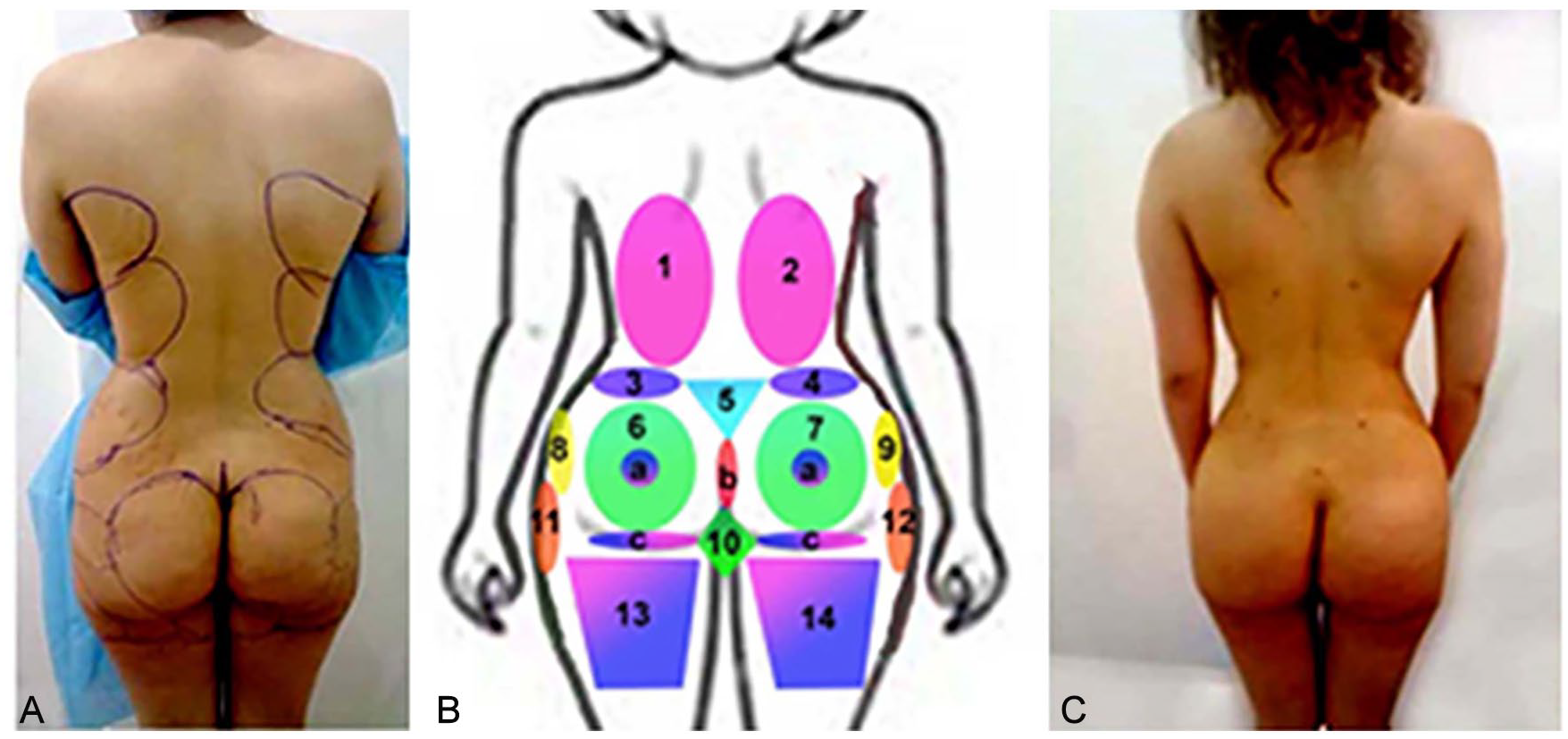
Example of the adopted extension put into practice. (A) Pre-operative diagnosis and assessment in posterior view of a 27-year-old patient. (B) Clinical diagnostic analysis showed fat excess in areas 1, 2, 3, 4, 5, 6b (the intergluteal cleft), 6c (the infra-gluteal line), 7b, 7c, and 10. The patient needs volume in areas 8 and 9. The patient was satisfied regarding areas 11, 12, 13, and 14. (C) the treatment plan view, 1 year post-operative after liposuction of 3.5 L from the abdomen and areas 1, 2, 3, 4, 5, 6c, 7c, and 10. Fat was transferred total 1200 mL to areas 6,7,8,9; that is, 600 mL per buttock.

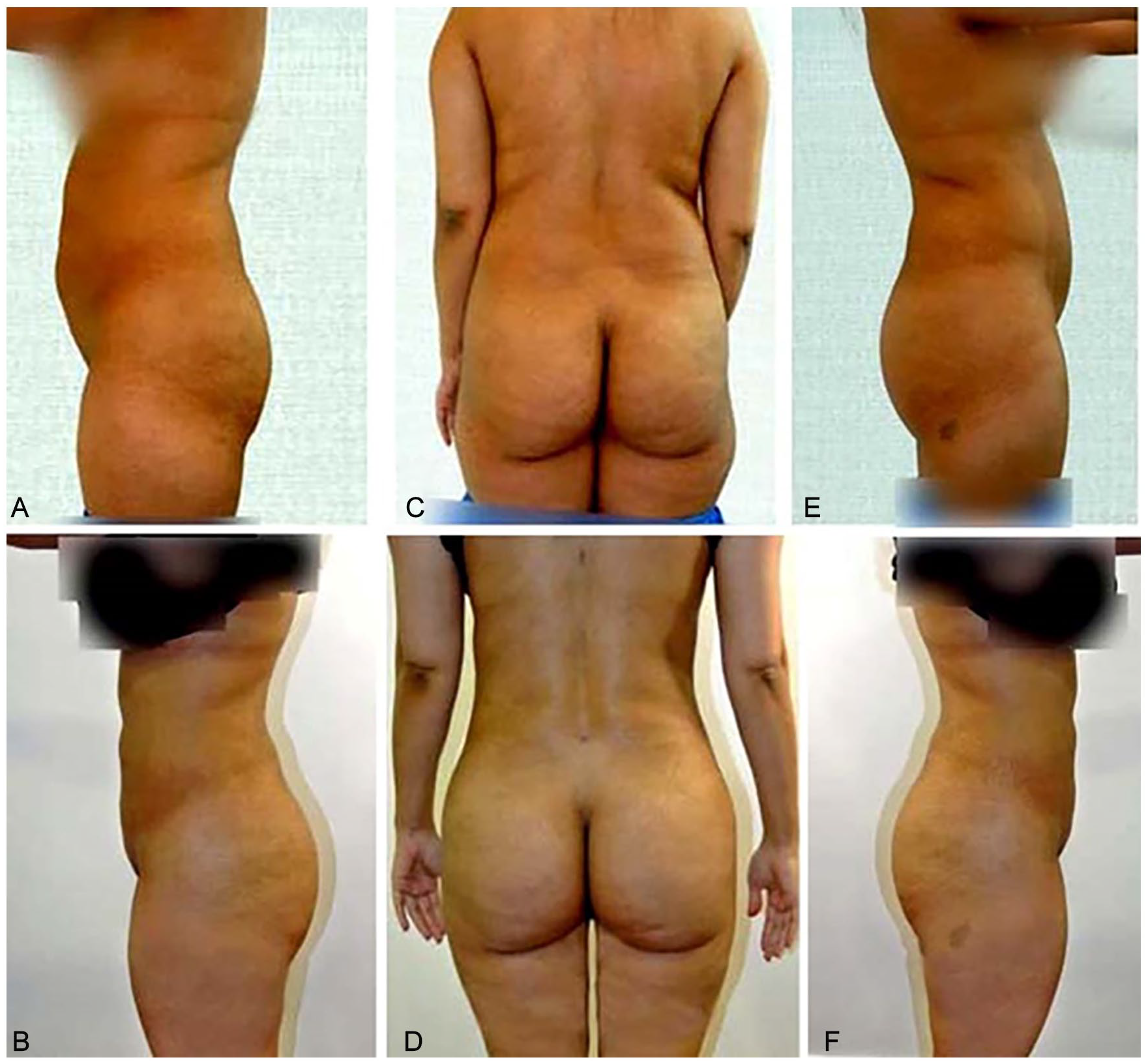
Patient, aged 27 years, from a Hispanic racial background (from Puerto Rico). (A, C, E) Pre-operative assessment and diagnostic views showing fullness in areas 1, 2, 3, 4, and 5, and emptiness in areas 6, 6a (location of the maximum projection point), 7, 7a (location of the maximum projection point), 8, and 9. (B, D, F) Post-operative views after the treatment plan using liposuction of 3.6 L of fat from the abdomen and areas 1, 2, 3, 4, and 5 and 900 mL of fat transfer to areas 6, 6a, 7, 7a, 8, and 9. The patient did not want a diamond zone (area 10).
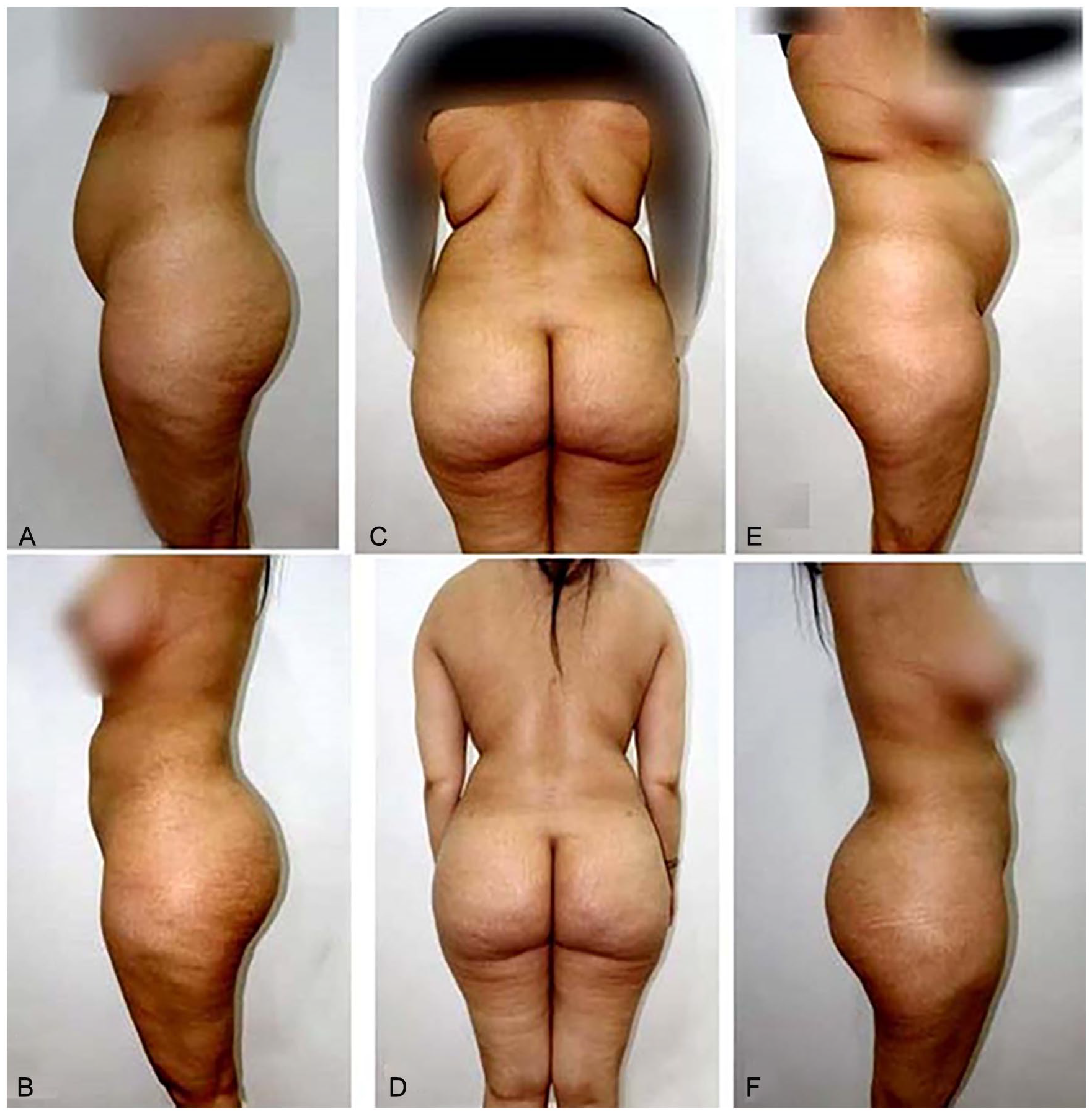
Patient, aged 32 years, from a white racial background (from Bosnia). (A, C, E) Pre-operative assessment and diagnostic views showing asymmetry between areas 11 and 12, and fullness in areas 1, 2, 3, 4, and 5. The patient asked for a narrow waist and fuller buttocks with a mild posterior projection and a diamond zone (area 10). (D, E, F) Post-operative views after the treatment plan using liposuction of 2.4 L of fat from the abdomen and areas 1, 2, 3, 4, 5, 10, and 12 and 700 mL of fat transfer to areas 6, 7, 8, and 9 with improvement of the asymmetry between areas 11 and 12.

Patient, aged 32 years, from a North African racial background (from Morocco). (A, C, E) Pre-operative assessment and diagnostic views are showing fullness in areas 1, 2, 3, 4, and 5; shortness in areas 6b and 7b (the length of the intergluteal cleft); and excess in areas 6c and 7c (the infra-gluteal line). The patient asked for more posterior projection in areas 6 and 7 and a slight reduction in the posterior thighs areas 13 and 14. (B, D, F) Post-operative views after the treatment plan using liposuction of 3.8 L of fat from the abdomen and areas 1, 2, 3, 4, 5, 13, and 14; and 1 L of fat transfer to areas 6, 7, 8, and 9; and improvement of the intergluteal cleft. The patient did not want to have a diamond zone (area 10).
Patient, aged 24 years, from a North African racial background (from Egypt). (A, C, E) Pre-operative assessment and diagnostic views are showing fullness in areas 1, 2, 3, 4, and 5. The patient asked for more posterior projection areas of 6, 6a, 7, and 7a, and a slight reduction in the posterior thighs areas of 13 and 14. (B, D, F) Post-operative views after the treatment plan using liposuction of 3.8 L of fat from the abdomen and areas 1, 2, 3, 4, 5, 13, and 14, and 1 L of fat transfer to areas 6, 6a, 7, 7a, 8, and 9. The patient did not want to have a diamond zone (area 10).

Patient, aged 36 years, from a white racial background (from Turkey). (A, B, C) Pre-operative assessment and diagnosis showed fullness in areas 1, 2, 3, 4, and 5; emptiness in areas 8 and 9; and asymmetry in the intergluteal cleft areas 6b and 7b (the length of the intergluteal cleft). The patient asked for rounded buttocks with an enhanced posterior projection. (D, E, F) Post-operative views after treatment plan using liposuction of 4.4 L of fat from the abdomen and areas 1, 2, 3, 4, 5, 11, and 12, and 1 L of fat transfer to areas 6, 6a, 7, 7a, 8, and 9, and improvement of the asymmetry of the intergluteal fold. The patient did not want to have a diamond zone (area 10). She is the only patient in this series with intergluteal cleft asymmetry.
Discussion
There are great differences in the ideal aesthetic measurements of the buttocks among ethnic groups. white Americans prefer buttocks with greater definition of the muscular and bony anatomy, with maximum projection at the level of the plane connecting the greater trochanter and the symphysis pubis (the distance of the most projecting point to the greater trochanter is nearly double the distance between the greater trochanter and the symphysis pubis in the lateral view). They also prefer lateral thigh depression. 15
The Asian American culture prefers the short buttocks, with a point of maximum projection higher than the symphysis pubis–greater trochanter plane. This gives the visual illusion of longer lower limbs and thus, giving better proportion between the extremities and the trunk. African American and Hispanic cultures favor buttocks having more projection than either white or Asian Americans. The point of maximum posterior projection is higher than the symphysis pubis–greater trochanter plane. Fullness of lateral thigh and deeper lumbosacral curve also appear to be favored by African Americans. 16
The ideal measurements of the buttocks-waist was evaluated in mass population with consideration of age and sex. They found greater differences in the ideal hip-waist ratio. There were a good percentage of women who preferred the ratio values of 0.65, 0.7, and even 0.5 to 1. 17 In our study, we introduce a descriptive analytic method which can accommodate these different racial preferences and patients’ requirements.
In recent years, the media has focused on the importance of the buttocks area in female beauty, and so the patient demands for buttock reshaping and augmentation have been increased. This necessitated a more structural approach to define the gluteal anatomy and the development of surgical approaches to enhance its beauty. The proposed classification of gluteal area by Centeno was accepted in a recent study by Mendieta and Sood. 18 In our opinion, the classifications of Mendieta and Centeno are very similar to each other. In both studies, they did not refer to the importance of the back, posterior thigh, and trochanteric areas and their role in esthetic interaction with the buttocks. They also did not stress upon the importance of the highest point of posterior projection, inter-gluteal fold, and infra-gluteal fold.
The entire back is very important, as it forms the curves (Figure 1) that define the feminine beauty in the eyes of the beholder. 19 In our proposed method, we found that the relation between the back, trochanteric areas (1, 2, and 8, 9), and the buttocks were very crucial in gluteal aesthetic appearance. In this way, we could choose the best aesthetic treatment for the racial, euthenics, and personal preference differences in the shape of the buttocks. We believe that our new classification is a valuable addition to the classification set by the work of authors such as Mendieta and Centeno.
In our study, seroma occurred in 9 patients (6.1%), which is higher than that reported by Sinno et al 20 ; we attributed this to closure of all wounds without the use of drains. However, we were not confronted with other adverse effects of implants, as we used fat transfer at the subcutaneous plane in our entire study.
Some authors improved the gluteal aesthetic appearance by removal of tissues from the trochanteric region and gluteal fold and other authors performed lifting procedures, achieving good improvement but resulting in large and visible scars. 21 In our technique, we used fat transfer which resulted in good aesthetic appearance without visible scars.
In a study performed by Shah about the rate of complications after the use of Implants, or Local Flaps and Autologous Fat Grafting, they reported implants as being the least safe of the gluteoplasty techniques, as its complication rate was found to be 31.4%. They also reported that Flaps had a rate between the two (implant and fat grafting), but closer to implants, at 23.1%. When it came to the most documented complications, implants were at the top in asymmetry, capsular contracture, hematoma, infection, seroma, wide scar formation, and wound dehiscence. They advocate that fat grafting is the best option when it comes to preventing post-operative complications, in which there is a low 6.8% rate of complication. 22 This is in accordance with our study as we have not confronted with any serious complications, except seroma at the donor site in 6.1% of cases, which were treated with aspiration and uneventful healing occurred.
Stabilized hyaluronic acid (HA) gel has been used for volume augmentation by occupying space within the tissue. Being biodegradable, the treatment effects of the gel are not permanent and may require retreatment as the body changes with time. Also, they reported that the incidence of infection was high. 23 In our study, we used autologous fat transfer. We did not report any case with infection. Autologous fat was found to be of long durability and lower cost if compared with other types of fillers.
The most dangerous complication of fat transfer to the buttocks is pulmonary fat embolism, which occurs mainly due to intramuscular injection of fat. The incidence of mortality is 3% and in 1 of each 3000 procedures according to the Multi-Society Task Force for Safety in Gluteal Fat Grafting (ASAPS, ASPS, ISAPS, IFATS, ISPRES), which recently issued a global online warning. 24
Fat embolism was also reported by Cárdenas-Camarena et al, as a result of deeper level injection of fat. Their autopsies showed macroscopic fat embolism to the right heart and lungs. The authors recommend that, during the injection of fat, the direction of the cannula must be parallel to the gluteal surface to avoid entering the sub-piriformis or supra piriformis channels where the gluteal vessels are located. 25 Mofid et al 24 found that the risk of fat embolism was significantly increased when surgeons injected fat into the deep muscles or angled the cannula downward during fat grafting. We were not confronted with any case of fat embolism at our series, as we used large pore cannula 4 mm, no intramuscular injection, and injection was performed at the subcutaneous level during withdrawal of the cannula.
Sozer et al 26 reported the limitations of using fat in transfer in buttocks ptosis and very thin patients. This was also our limitations, as we found great difficulty to get fat from thin individuals and we found also that fat injection did not correct buttock ptosis.
Conclusions
We believe that this classification of buttock areas is a valuable step that could help in achieving the required results that are more satisfactory to different types of patients.
Despite all the merits of this analytical tool and the advantages of the innovations in liposuction, some limitations remain. Fat transfer alone will not treat and even may worsen ptosis.
Liposuction and fat injections are not an ideal treatment for very thin women with low subcutaneous fat amounts.
Footnotes
Acknowledgements
I acknowledge the efforts of Professor Dr Ahmed Hegazy, Professor Dr Mohammed Elhaddi, Professor Ahmd Bahaa, and Professor Omar Showman, Head of Department, Plastic and Reconstructive Surgery Department, Al Mansoura University, Egypt, and the Department of Plastic Surgeons for giving their valuable objective opinion in the assessment of the results of this work. I acknowledge my colleges and nursing staff at Tanta University hospitals for their help during all steps of this work.
Author’s Note
This article was approved by Tanta University’s Ethical Committee (2009/12/23).
Author Contributions
The author did the study design, performance of surgery, and manuscript preparation.
Availability of Data and Materials
The author confirms that the data supporting the findings of this study are available within the article and at the hospital also.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
All the steps of the procedures performed in this study were following the requirements of the institutional, national research committee, and with the 1964 Helsinki declaration and its later amendments or ethical standards. The rules and principles of ethical and professional conduct have been followed in this study. This article was approved by Tanta University’s Ethical Committee (2009/12/23).
Informed Consent for Publication
Informed consent was taken from all patients who participated in the study and additional informed consent was obtained from all individual participants for whom identifying information is included in this article.