
Abstract
Background:
Following the Supreme Court of Canada’s Carter Decision, medical assistance in dying (MAID) became possible with individual court orders in February 2016. Subsequently, on June 17, 2016, legislation was passed that eliminated the need for court orders, essentially making physicians the arbiters of these requests. Canadian health-care facilities now face the challenge of addressing this unprecedented patient health-care need.
Aim:
To describe the manner in which London Health Sciences Center has approached local and regional requests for MAID, including the administration, ethics, privacy, and clinical process.
Design:
A health-care systems descriptive study.
Setting/Participants:
Between June 6, 2016, and May 30, 2018, London Health Sciences Center’s MAID Internal Resource Committee triaged and referred 260 cases. Ninety-six received the requisite assessments were deemed eligible for and received MAID.
Results:
The procedure was completed in hospital 59 (61%) times, and 37 (39%) times in the community (either private residence or long-Term Care facility). Nineteen patients did not meet MAID criteria and 63 patients died while awaiting the procedure. The median wait time between first request and referral was 1 day. The median time between referral and the procedure was 12.0 days. The ratio of referrals to completed cases is 96 of 260 (or 37% conversion rate).
Conclusion:
Our MAID processes, including our committee structure, referral triage process, and physical site have all undergone extensive review and improvement cycles throughout these first 2 years with the aim of ensuring that this procedure is managed in a respectful, confidential, safe, efficient, and patient-centered manner.
Background
Following the Supreme Court of Canada’s Carter Decision, 1 medical assistance in dying (MAID) became possible with individual court orders in February 2016 and later without court involvement when legislation 2 was passed on June 17, 2016. Medical assistance in dying in Canada includes both physician-assisted suicide (the prescription of lethal medication(s) by a physician to a patient for self-administration) and voluntary euthanasia (the administration of lethal medication(s) to a patient by a physician, typically by the intravenous route). The Provincial Physician, Nursing, and Pharmacy Colleges (among others), as well as Canadian hospitals, now face the challenge of addressing this novel patient care need that is unprecedented in Canadian health care.
These early days of managing a generational change in the practice of medicine continue to be met with uncertainty, 3 evident through the variability in practice and pace of adoption across the country. 4 Even among supporters of this transition, there are concerns with the implementation. Quality care requires a data repository from which to evaluate a practice and improve. Indeed, this quality assurance process has been undertaken in other jurisdictions such as the Netherlands. 5 In Ontario, the best data available come from the chief coroner’s office, who has been reporting monthly to the Ministry of Health and Long-Term Care. 6 The coroner’s office data are important for tracking case volume, procedure location, and types of diseases leading to MAID requests. Helpful as they are, these data do not help providers develop the infrastructure for their local programs. The purpose of this article is to share the experience of one tertiary care health-care center’s approach to developing the infrastructure to support and sustain a MAID program. Our Toronto colleagues recently described their approach to MAID. 7 Although sharing many similarities with the Toronto approach, our MAID infrastructure has several distinct differences, including our multidisciplinary committee, our Chair role being performed by our hospital ethicist, our providers’ willingness to perform procedures at patient residences, and our hospital’s dedicated physical space for MAID procedures. In addition to our health systems description, local quantitative patient data are shared for context setting, in the hope that it will inform future planning discussions and collaborations.
From the outset, our tertiary care hospital established dialogue and debate on MAID. Our most important governing principle is accepting the obligation to ensure that patients who desire MAID are able to access timely assessments and procedures. Recognizing our hospital, local and regional obligations, it was determined we would work to support community requests from patients and providers not affiliated with London Health Sciences Center (LHSC) where they were otherwise unable to find providers or institutions to support their requests. Where necessary, this included bringing patients to our hospitals for both assessments and for procedures.
As an organization, we encountered many early challenges including accurately predicting the number of requests and referrals to inform human resource and facility requirements. (Figure 1) An internal review committee was established, whose mandate is to receive requests from patients and physicians, (Figure 2) liaise with partners including hospital and community pharmacies, our Catholic Hospital counterpart, and our local homecare nursing organization to create a hospital policy and to report to the hospital medical advisory committee and senior leadership.
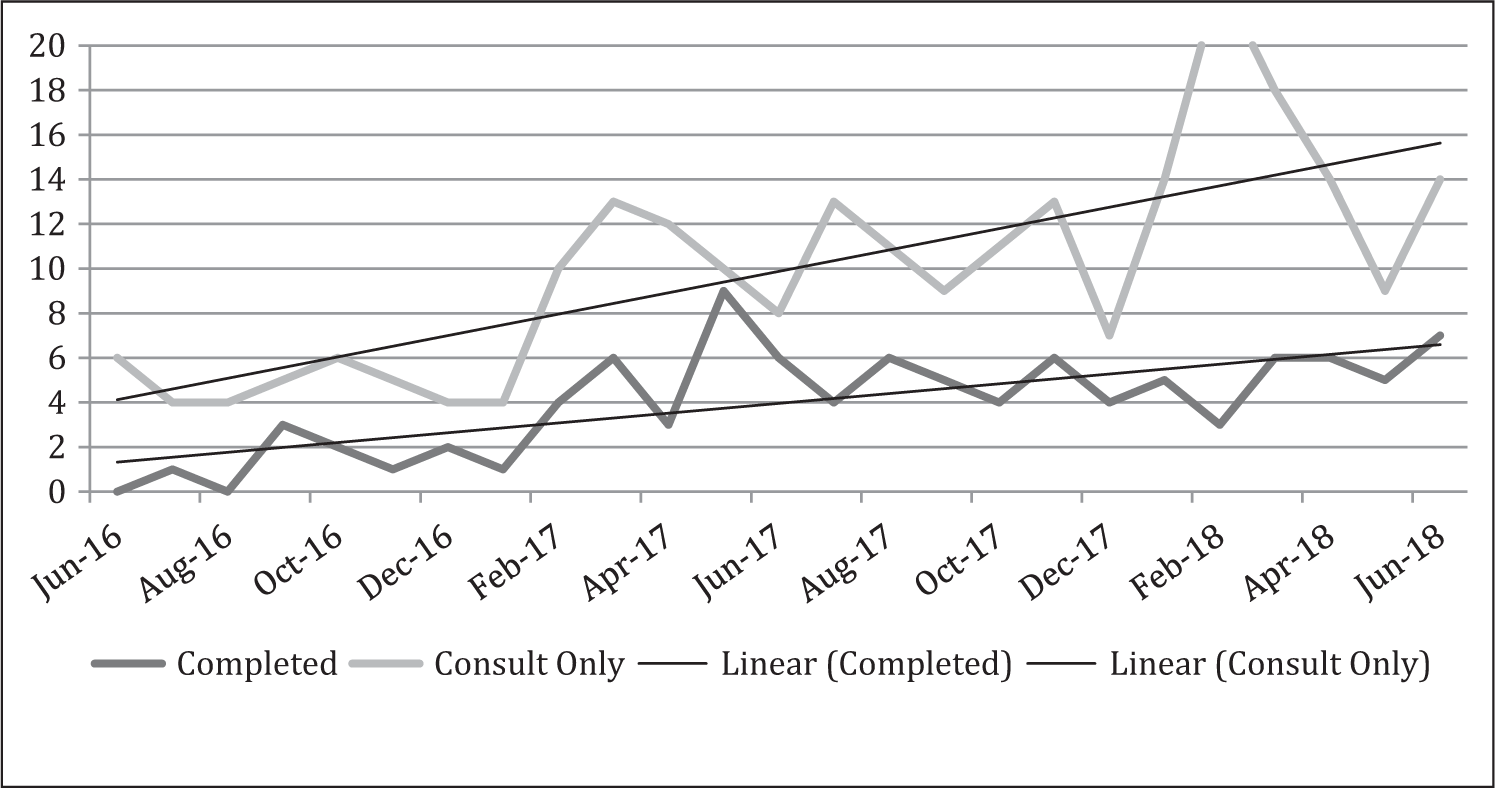
Volume of referrals, and completed medical assistance in dying (MAID) procedures (with projection).
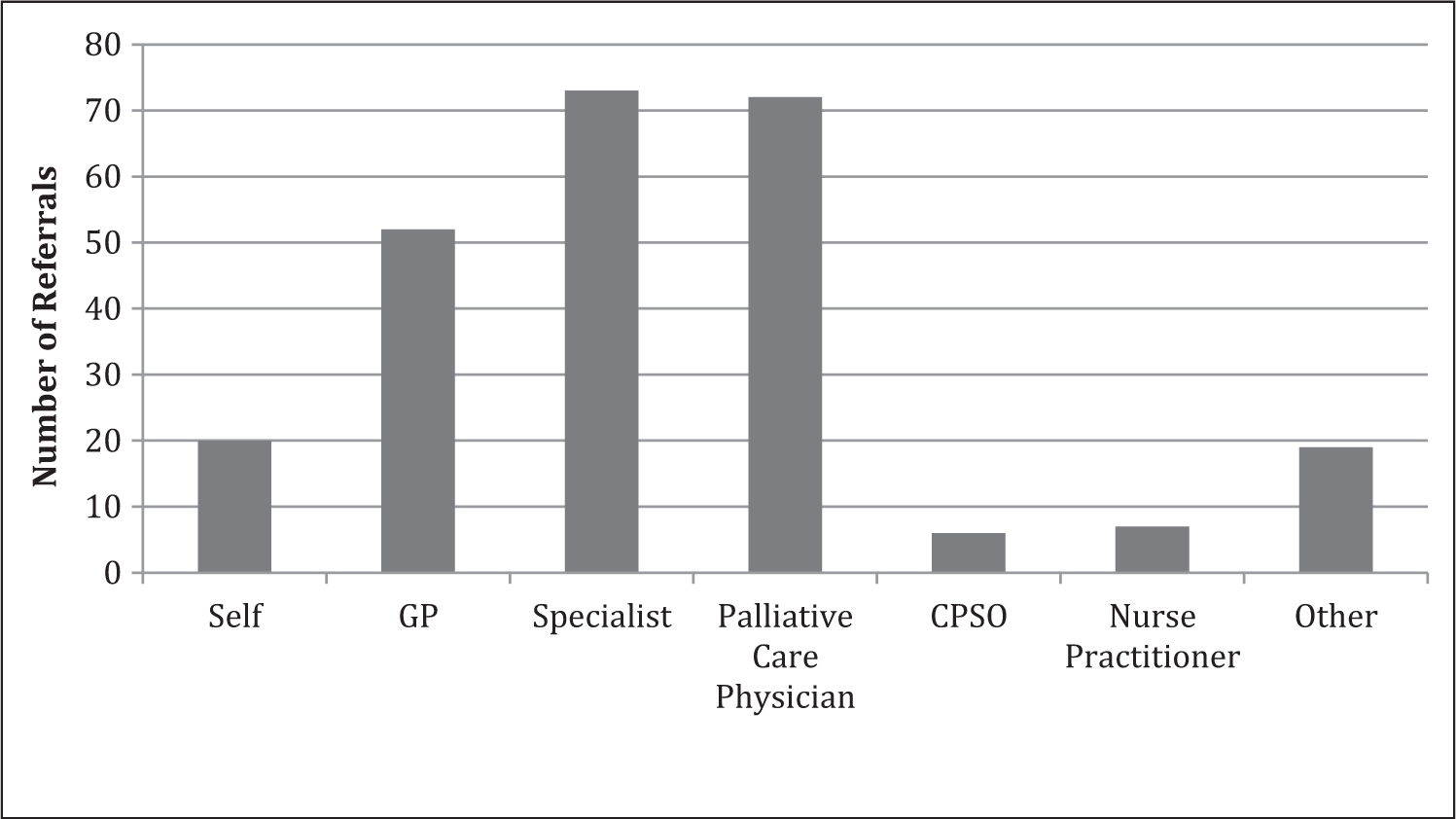
Referrals to internal resource group (IRG) for medical assistance in dying (MAID) by origin.
Hospital Internal Resource Group
Our internal resource group (IRG) supports referrals from patients and health-care providers from within our hospital, within London, and from within our region (Figure 3). In some cases, the committee establishes a connection between requestors and the physician provider group; in other cases, the IRG provides direct advice only.
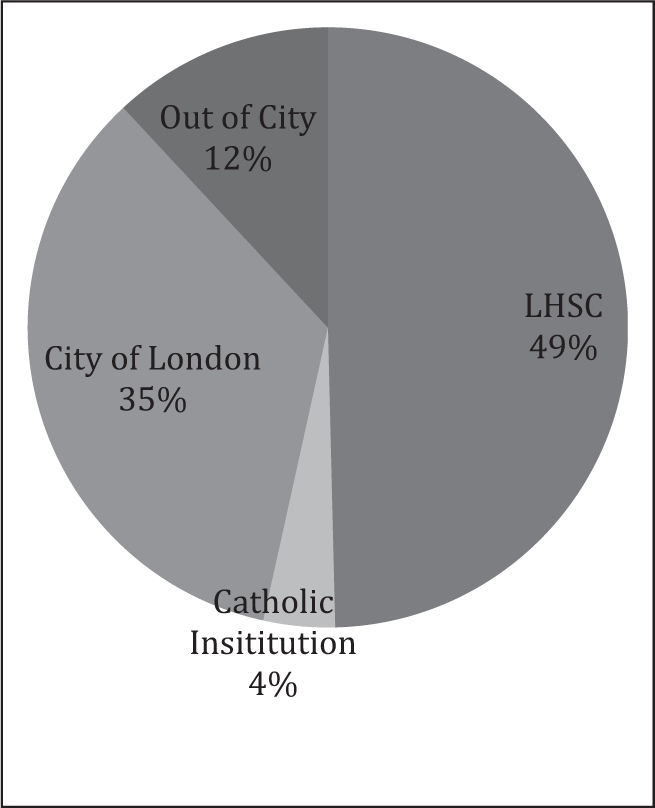
Requestor location at time of referral.
By acting as an intermediary between MAID requestors and the provider group, the IRG provides an element of anonymity to the members of the physician provider group. This was felt to be of great importance to physician providers, some of whom were very hesitant to participate in the MAID process out of fear for the potentially negative impact on their careers and personal lives. Despite the fundamental differences between MAID and therapeutic abortion, the experiences abortion providers encountered in the early 1990s from activists suggest that caution is warranted.
Internal Resource Group Membership
Our IRG is chaired by the hospital ethicist and includes representation from the medical advisory committee and senior leadership, departmental leadership, and pharmacy leadership. Additionally, professional practice disciplines are represented, as well as legal counsel. Although family members are currently not represented on our MAID group, the Director of Patient Safety and Experience whose mandate includes patient- and family-centered care, also sits on the committee.
Medical Assistance in Dying Providers
In June 2015, our IRG chair began engaging physicians with both supportive and opposing views on MAID with the goal of creating a “MAID provider group.” An initial team of physicians from anesthesia, palliative care medicine, intensive care medicine, family medicine, oncology, psychiatry, and neurology were asked to support policy development and also provide 2-way communication between their respective disciplines and the MAID team. Out of this team, we eventually identified physicians willing to act as “MAID assessors” and/or “MAID providers.” The team initially included 7 physicians willing to provide medical guidance to the IRG and to participate in MAID assessments. A smaller number of clinicians were willing to participate as actual MAID providers. In at least 2 cases, despite being strong MAID advocates, physicians have been unwilling to step forward as providers out of fear of potential adverse personal and professional consequences. Professionally, the concern was primarily related to judgment by colleagues and peers (which was experienced by at least one of our members).
The IRG was responsible for developing a hospital policy for MAID. The IRG felt strongly that only clinicians experienced with anesthetic administration and the placement of central venous lines ought to be able to provide MAID within the hospital. The relatively infrequent nature of MAID prevents clinicians from developing expertise through direct experience. In light of this, it is the preference of our committee that providers must maintain competence through clinical experience in a non-MAID-related practice.
Collaboration
Pharmacy
Our hospital pharmacy leadership has membership on the IRG and has been involved in the development of our hospital protocols and policy since the beginning. Individual pharmacists are given the option of not participating in MAID procedures. Despite this option, several individual pharmacists have been extremely engaged in and supportive of the MAID initiative. In addition to pharmacy’s early role in contributing to the conceptualization of the MAID drug regimen, pharmacy has been extremely helpful at preparing a MAID “kit” for providers to use. The kit includes the requisite medications, syringes, lines, needles, and other supplies required for the procedure. In early cases where procedures were planned in the community, the hospital pharmacy provided medications and supports while community pharmacies worked to develop their own procedures (now in place). Pharmacy disposes of all left over medications and equipment at the end of the procedure. Pharmacy leaders in the IRG committee have helped to communicate with and educate, community pharmacists for MAID cases taking place outside of our hospital.
Local Homecare Nursing Organization
When developing our MAID program, we anticipated approximately a 4:1 home: hospital ratio, based on the Dutch experience. 8 Provincial data to date have instead demonstrated a 1:1 ratio, 6 fairly consistent with our own data (Table 1). This ratio reversal may be driven by an abundance of patients from within our region but outside our city (Table 2). As a referral center, we have a catchment area of 971 500 people, or 7% of our province’s population. Nearly, 40% of our region’s residents live in the city of London (population 366 151), its only large urban population center (100,000+)] MAID now comprises approximately 2% of all deaths in our health-care region.
Baseline Patient Characteristics.
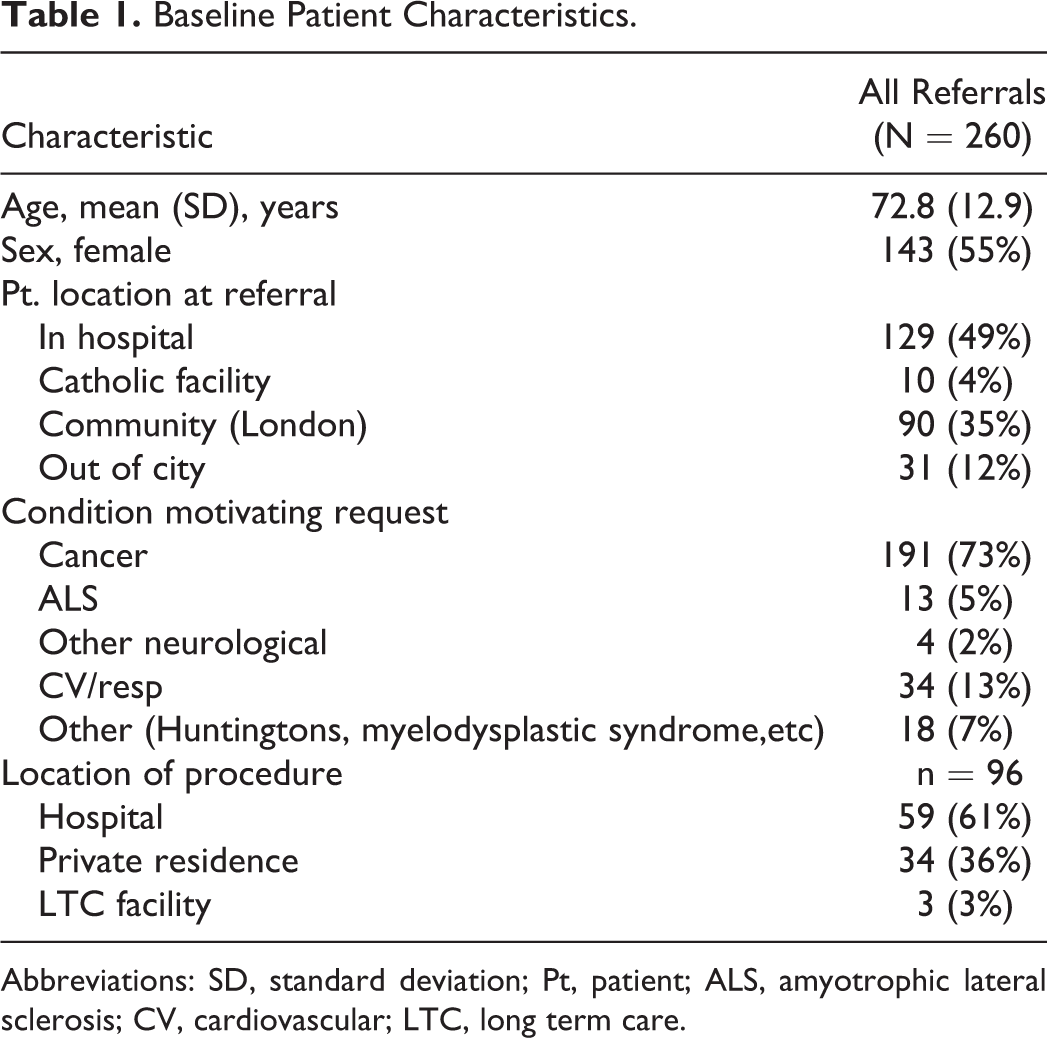
Abbreviations: SD, standard deviation; Pt, patient; ALS, amyotrophic lateral sclerosis; CV, cardiovascular; LTC, long term care.
Waiting Periods Between Key Time Points in Process.a,b,c
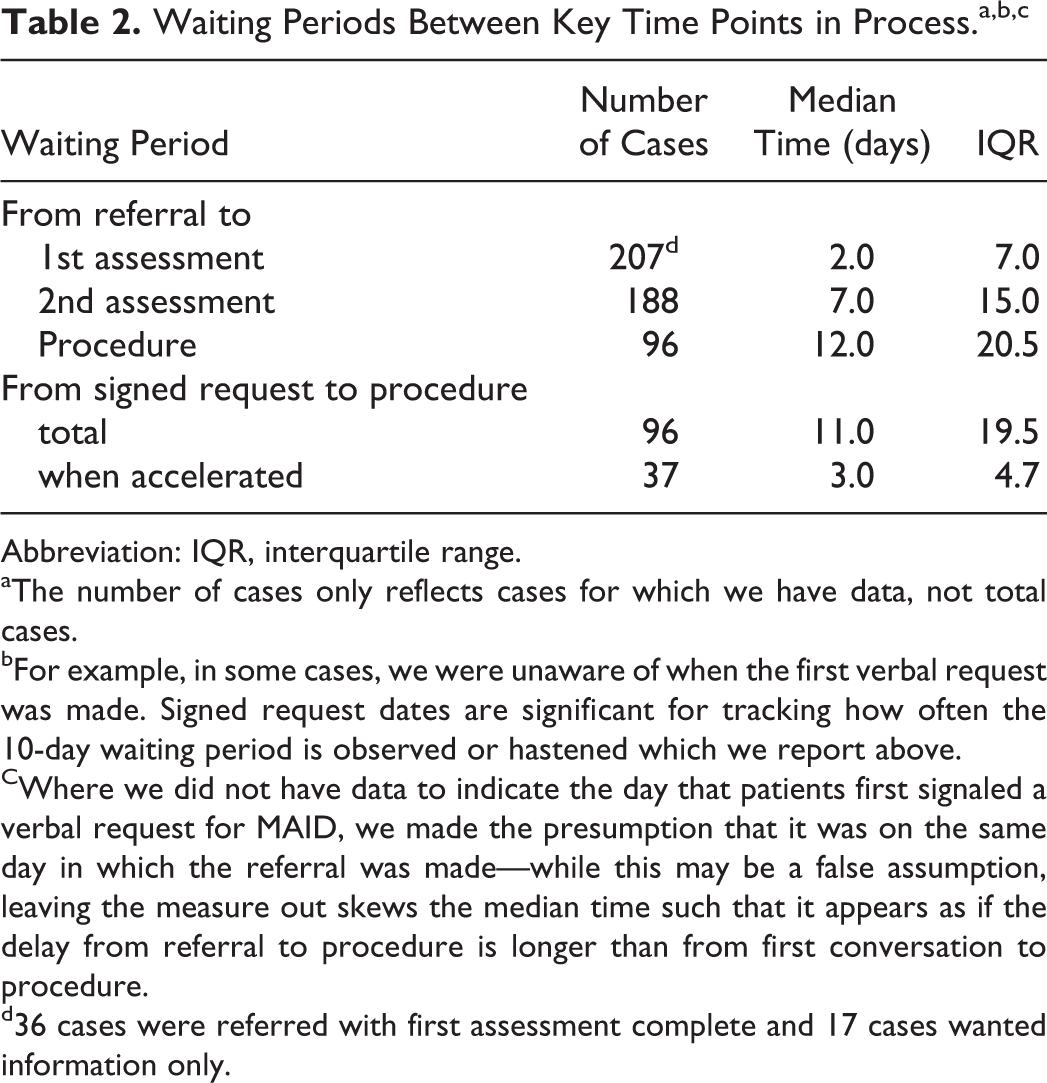
Abbreviation: IQR, interquartile range.
aThe number of cases only reflects cases for which we have data, not total cases.
bFor example, in some cases, we were unaware of when the first verbal request was made. Signed request dates are significant for tracking how often the 10-day waiting period is observed or hastened which we report above.
CWhere we did not have data to indicate the day that patients first signaled a verbal request for MAID, we made the presumption that it was on the same day in which the referral was made—while this may be a false assumption, leaving the measure out skews the median time such that it appears as if the delay from referral to procedure is longer than from first conversation to procedure.
d36 cases were referred with first assessment complete and 17 cases wanted information only.
It is logistically difficult for our small physician MAID provider group to perform home visits for these patients. In addition to the pharmacy support as described above, we have been very fortunate to have a strong relationship with our local homecare nursing organization. Its nurses have been instrumental at the following tasks: Arriving at the patient’s residence 1 to 2 hours prior to the procedure to establish 2 peripheral intravenous lines (in cases where peripherally inserted central [venous] catheter [PICC] lines are not already in situ). Reviewing any last minute patient or family questions about the procedure. Drawing up medications. Supporting patients, patient families, and the MAID provider during the actual procedure. Remaining with the body after the procedure until the coroner releases it to the funeral home. Transporting MAID medications to the pharmacy.
Local Catholic Hospital
In addition to LHSC, the city is served by St Joseph’s Healthcare, London, which includes St Joseph’s Hospital and Parkwood Hospital. Being a Catholic organization, both of these hospitals are unable to allow MAID procedures or assessments to occur on their grounds. London Health Sciences Center’s MAID IRG has worked effectively with our colleagues at St Joseph’s to facilitate the transfer of inpatients from St Joseph’s and /or Parkwood Hospitals to LHSC facilities for MAID assessments and/or procedures.
Venous Access Support Team
Another important contributor to the LHSC MAID effort is our venous access support team (VAST). As previously mentioned, the loss of intravenous access mid-procedure is one of our providers’ greatest concerns. Whenever possible, LHSC providers are using central access, generally in the form of a PICC. When our program launched in the summer 2016, we allowed a broad interpretation of conscientious objection to include mostly any aspect of care associated with a MAID case. It is clearly stated on the requisition that certain PICCs were being placed to facilitate MAID, and individuals can excuse themselves from being involved in the line placement in accordance with their personal beliefs. Unfortunately, over time a number of VAST technicians have declared themselves to be conscientious objectors. A sufficient pool of VAST nurses has been identified and have been able to meet our needs to date, though at times requiring movement of staff between campuses.
London Health Sciences Center MAID Medical Protocol
The LHSC MAID protocol was adapted from the Belgian and Quebec protocols with input from our physician provider group.
Oral Medication Administration
Our provider group was extremely reluctant to provide MAID by oral medication administration. The Dutch experience describes that approximately 90% of the MAID cases are performed with intravenous medications. 8 Many patients have abdominal involvement of their malignancies or other medical reasons that make enteral absorption unreliable or unpredictable. Of great concern is the potential for a patient to vomit doses mid-procedure creating uncertainty as to the effectiveness of the regimen. Our group did concede that in the case of a patient wanting assisted suicide at home, we would be willing to prescribe oral medications for this purpose, with the explicit understanding of the patient that the scenarios described above are possible. Our current data demonstrate that 100% of our cases have been voluntary euthanasia (intravenous medications administered by the physician), whereas we have not performed a single case of physician-assisted suicide (the prescription of lethal medication(s) by the physician for patient self-administration).
Intravenous Access
Another significant concern articulated by the provider group regards intravenous access. The group recommends that central venous access be established (PICC lines are ideal). Cases have been completed successfully with peripheral intravenous access only, but similarly to the concern with oral medications, the group wants to avoid a “half-dose” scenario, where intravenous access is lost mid-procedure due to an interstitial peripheral intravenous.
Medication Protocol
Midazolam 10 to 20 mg IV for anxiolysis, repeated once PRN. Propofol 300 to 1000 mg IV, repeated once PRN. Rocuronium 50 to 100 mg IV, repeated once PRN. Midazolam10 to 20 mg IV PRN for tachycardia or hypertension.
Our group discussed the use of potassium chloride (KCl), but it was felt to be unnecessary. The same decision was made with respect to the administration of intravenous lidocaine. The patients being treated with this protocol are typically elderly patients, having a terminal disease, and are dehydrated in most cases. The medication protocol has been effective in this patient population.
Confirmation of Death
Another significant concern raised by the provider group is the extremely unlikely possibility of auto-resuscitation. Providers monitor the patients’ vital signs for 10 to 20 minutes after the absence of a palpable pulse and respiratory efforts to ensure that auto-resuscitation has not occurred. This step may seem overly conservative given the rarity of this event, but the possibility of a partial auto-resuscitation in a private residence after the physician’s departure is an event that cannot be left to even the most remote chance.
Ongoing Challenges
Delays
The median interval from time of referral to second assessment was 1 day (Table 2). Although this feels like a very timely response, 63 patients died prior to being able to receive the procedure (Figures 2 and 4). We are aware of several cases where patients perceived that their request was not referred until having expressed it several times. In 1 case, a patient claimed to have requested MAID for 25 consecutive days prior to being referred for an assessment. All of the examples above stress the need for improved public and health-care worker MAID awareness, to facilitate more prompt referrals.
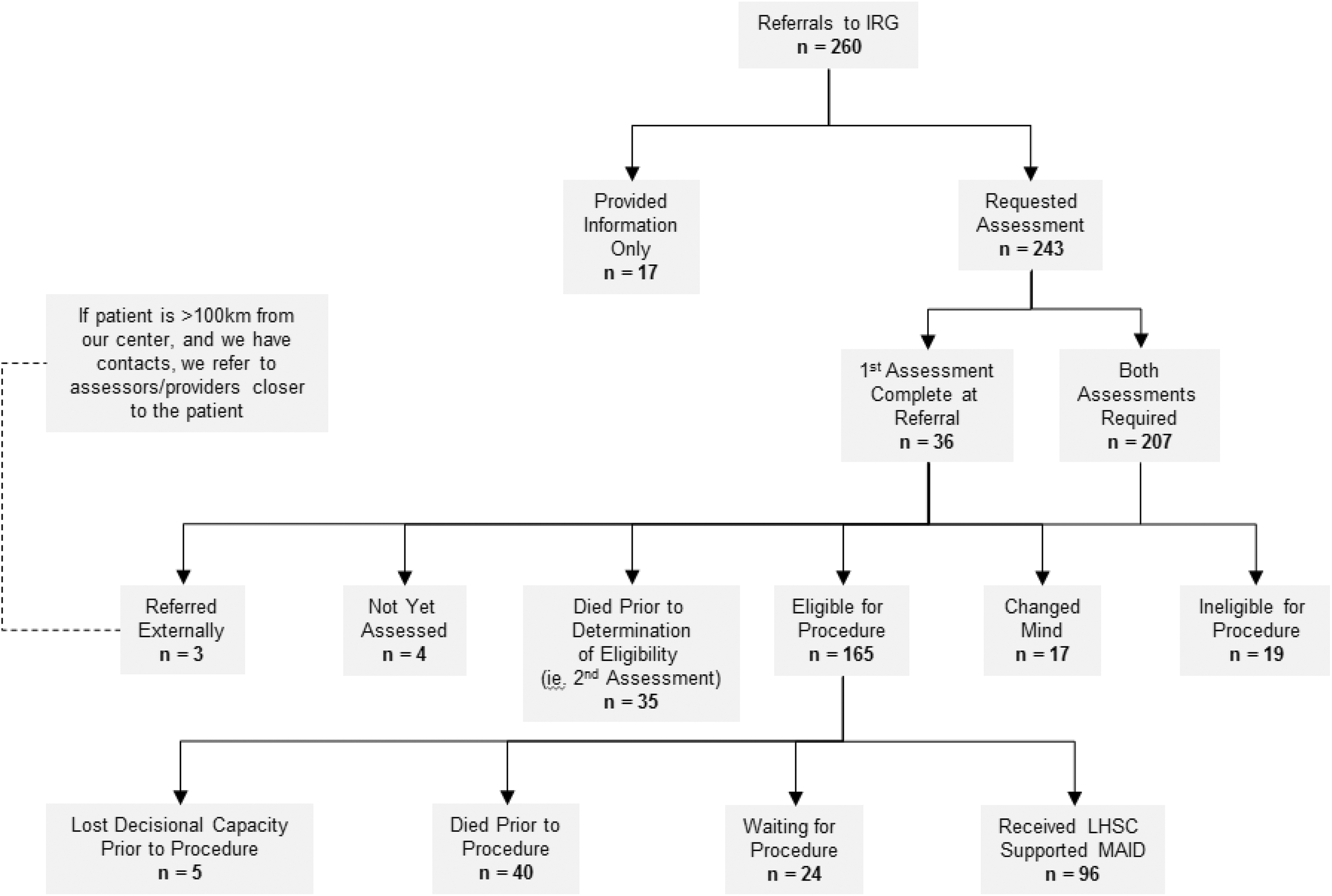
Outcomes of Referral to internal resource group (IRG).
Some of our patients were referred to us through a provincial hotline for physicians to register and refer patients for MAID assessments. This is a convenient resource, but there can be a delay of 5 to 7 (in at least 1 case we experienced a 10+ day delay) days before the service connects a willing MAID assessor to the patient. The province has responded by opening this resource to the public who can now self-refer (http://www.health.gov.on.ca/en/news/bulletin/2017/hb_20170529.aspx). Once the initial contact is made, a mutually acceptable appointment time needs to be determined. Many patients requesting MAID have already waited until they are close to losing capacity, or death, prior to approaching a health-care professional. The majority of our referrals come from GPs, palliative care physicians, and other specialists (Figure 2).
Current Canadian legislation mandates a 10-day waiting period between a patient’s written MAID request, and the performance of the procedure. This can be waived if clinicians believe the patient is at risk of losing capacity (or dying) during the waiting period.
Provider Knowledge Gap
We have encountered cases where providers have seemingly failed to adhere to our provincial medical college’s policy of providing an effective referral. We often encounter poorly informed physicians who are unaware of either their referral obligations or how to complete them. Physician misinformation and misunderstandings have led to patients being misinformed about location options, process, and even procedure eligibility. Locally, we have been concerned that even within our hospital; physicians are still unaware that they can complete their duty to refer internally through our IRG process.
Proposed methods for streamlining the process include public forums to improve awareness of patients and care providers in areas where MAID requests are likely to originate and to coordinate referrals through a regional, rather than provincial, service. Our provider group has been very responsive to requests, often completing first assessments within 24 hours of the IRG receiving the request. In 36 out of 96 cases, we have had to waive the 10-day waiting period because clinicians believed there was a high risk of patients dying or losing capacity. The median waiting period between referral and receipt of the procedure is 12 days (IQR 20.5), except in those where the 10-day waiting period is waived, in which case it is 3.0 days (IQR 4.7; Figure 5).
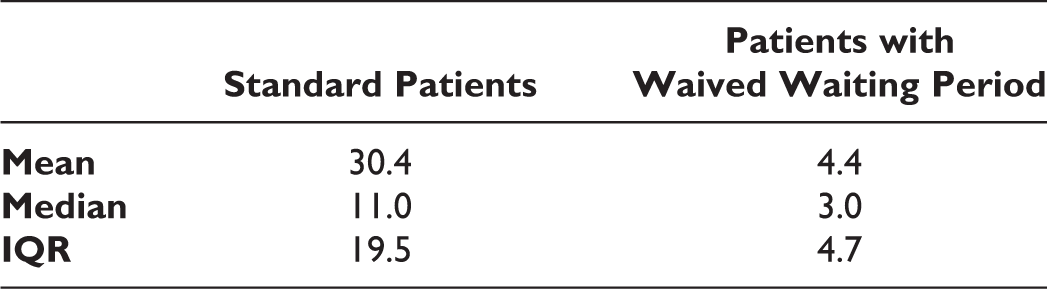
Time (in days) between written request for medical assistance in dying (MAID) and receipt of procedure. IQR denotes interquartile range.
Location of the MAID Assessments and Procedure
Medical assistance in dying assessments are preferably done in hospital at the bedside, or in patients’ private residences or long-term care facilities. However, in some instances, a community assessment was not possible due to the call schedules of provider physicians who had not previously been accustomed to house-calls. This presented challenges regarding where out-patient assessments could be completed in the hospital, how to register these patients while preserving patient and physician confidentiality, and addressing whether to alter usual hospital code blue protocols in the event that a MAID patient deteriorates during their hospital assessment visit. It was decided that in the event of a MAID patient deterioration (while not in the company of a MAID provider), they would be treated in the same manner as any other in-hospital code blue. The code team would be called and would question accompanying family members about patient resuscitation wishes. This would likely lead to the administration of palliative medications and the withholding of any aggressive resuscitative measures.
For the procedure location, we thought that the following criteria were ideal: privacy for both patients/family and providers, quiet, a comfortable environment for family to gather, and seclusion (to protect the confidentiality of care providers). Initially, we sought to bring MAID providers to patients’ ward settings to perform the MAID procedure. However, this approach created privacy/confidentiality challenges that we have been unable to overcome. For example, it was important to engage local leadership about what would be taking place on their floor, but this led to conversations about exactly who needed to know. Several staff, in deducing what had transpired through observation (eg, patient expresses wish to die, then a new team takes over, and the patient is dead a week or 2 later), voiced a perceived right to know because either they were at one time in the circle of care or because they “always knew when a withdrawal was taking place” and could thus be more sensitive to those nearby (both visitors and staff). This was problematic for our providers who wished to have their involvement in MAID procedures unknown within the broader hospital community. Thus, when we encountered other departments who did not feel it appropriate to conduct the procedure on their floor, it was an easy decision to look for a designated location.
Eventually, the IRG secured a designated hospital location that provides the desired attributes to be used as both an assessment and a provision location.
Health-Care Personnel Discomfort With MAID
Despite the mandate from the provincial college that physicians who object to MAID for personal reasons still provide effective referrals, there are 2 challenges we have experienced. The first situation is the physician who deliberately blocks patient requests for MAID, thereby violating the college’s mandate and possibly the standard of care. This includes not making a referral at all, coercing patients to undergo further palliative care prior to making the referral, or waiting until patients have made an unreasonably large number of requests. The second situation that we have encountered is the patient who expresses a desire to stop active treatment in order to pursue palliative care. In 1 case, physicians misinterpreted these requests for palliative care as expressions of interest for MAID. Very brief interviews by members of our committee identified the distinction, and patients’ clinical goals were been adjusted to focus on palliation, rather than cure or MAID.
Opportunity for MAID as a Relief to Patients
In our experience, it has been the rule rather than the exception that once patients recognize MAID as a clinical possibility, their moods improve significantly. The ability to control the timing and the manner in which they die (down to the clothing they will wear) is very cathartic. Even for those patients who never actively pursue MAID, the knowledge that it exists as a possibility should their quality of life deteriorate is empowering.
Conclusion
Medical assistance in dying is now a legal option for many Canadian patients. The health-care community as a whole is now challenged with addressing this novel patient request in a compassionate, timely, and professional manner. Sensitivity to local communities is essential to create and adapt systems that meet the needs of our patients, while respecting the individual views of providers.
Finally, in an effort to ensure quality, we have found data collection to be critical to our efforts. Although we were unsure at the outset which data points ought to be collected, we believe we now collect the right information to inform quality improvement initiatives. We are concerned that neither existing legislation nor pending provincial legislation will address the reporting and collection of such data. In particular, we note that completed cases (as captured through the current reporting process to the coroner’s office), represent only a fraction of the ongoing work in this field. Higher quality data and sharing of these data between provider groups could improve patient care.
Key Lessons
Establish a multidisciplinary committee for managing patient requests for MAID,
Establish a core team (and regional network) of physicians, nurses, and pharmacists—and community providers
Clarification and management of expectations with patient/family should be on-going
Review every case for improvement opportunities
While currently a legal option, MAiD remains fairly uncommon. Expect resistance but continue to put patients first.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.