
Abstract
Introduction:
Medical assistance in dying (MAID) was legalized in Canada in 2016, creating a significant shift in end-of-life care. However, Indigenous populations face unique challenges with MAID due to historical mistreatment, cultural differences, and systemic barriers within the health care system.
Objectives:
By means of this scoping review, we identify the critical gap in understanding Indigenous experiences with MAID. We also seek to identify barriers and facilitators to providing culturally appropriate care and to incorporate Indigenous perspectives into MAID policies and practices.
Results:
We identified key themes, including the need for cultural sensitivity and safety, the importance of community and family involvement, communication barriers, and policy and legislative considerations.
Future Directions:
From our findings, we highlight the necessity of engaging Indigenous communities in developing MAID services to ensure they are culturally appropriate and respectful. Addressing these needs is essential to providing respectful end-of-life care for Indigenous peoples in Canada. We also highlight significant gaps in the literature and the urgent need for further research to ensure that MAID services are culturally appropriate and aligned with Indigenous values and needs.
Definition:
In this article, the term “Indigenous peoples” refers to the original peoples of North America and their descendants. The Canadian Constitution recognizes three distinct groups of Indigenous peoples: First Nations, Inuit, and Métis.
Keywords
Introduction
Medical assistance in dying (MAID) in Canada was first legalized in June 2016 and marked a significant shift in our country’s approach to end-of-life care. Initially, certain groups, such as mature minors and individuals whose sole underlying condition is a mental illness, were excluded from eligibility. However, on March 17, 2021, amendments were made to broaden the eligibility criteria, although individuals with mental illnesses remain temporarily excluded until further revisions, which are scheduled to take place in March 2027. 2 The current federal eligibility requirements include being 18 years or older, having decision-making capacity, being eligible for publicly funded health care services, making a voluntary request, and experiencing intolerable physical or psychological suffering due to a severe and incurable illness, disease, or disability (Government of Canada, 2021; Bill C-7, 2021; Bill C-14, 2016).2,3 See Figure 1 for a timeline of MAID in Canada.
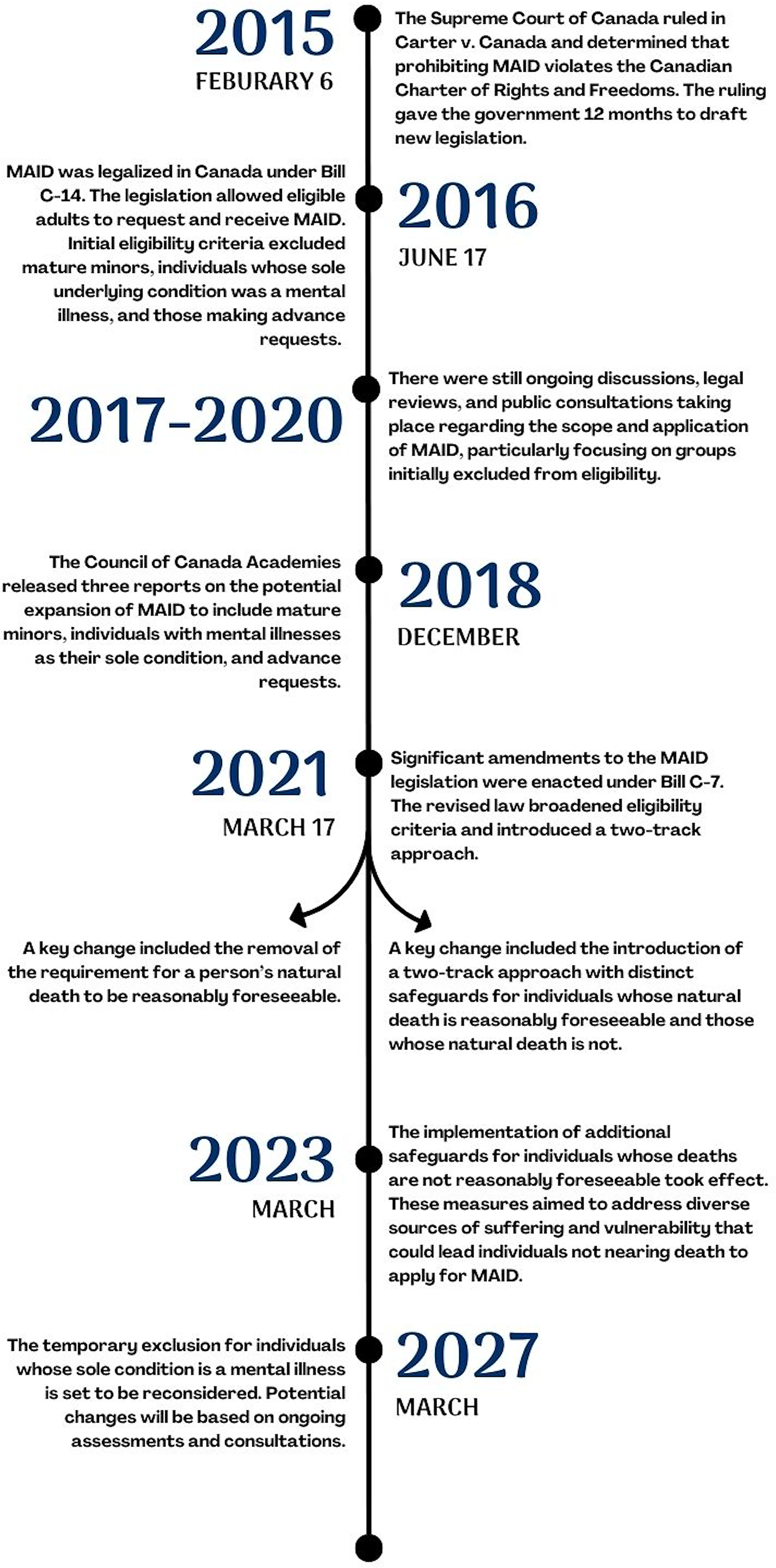
Timeline of medical assistance in dying (MAID) in Canada.
Despite these advancements, members of some marginalized groups may have unique cultural needs impacting their experiences with MAID, which have not yet been thoroughly examined. Specifically, Indigenous peoples in Canada carry a history of colonial trauma and systemic inequities that continue to shape health care encounters and levels of trust today. Implementing MAID within Indigenous communities presents unique challenges. Historically, Indigenous peoples in Canada have faced significant disparities in health care access and outcomes. This disruption, coupled with past colonial policies, poor living conditions, and systemic racism, has led to a persistent mistrust in health care systems.4,5 Notable examples include the coercive sterilization of an estimated 1200 Indigenous women between 1970 and 1975 (whose consent was often uninformed) and the operation of racially segregated “Indian hospitals” from the 1930s to the 1980s that delivered substandard, non-consensual care.6,7 These legacies, which are compounded by epidemics introduced by European settlers, the criminalization of traditional healing practices, and ongoing social determinants, continue to drive health inequities and inform attitudes toward MAID.8–11
One significant event contributing to this mistrust is the history of forced sterilizations of Indigenous women in Canada. Between 1970 and 1975, approximately 1200 Indigenous women in Canada were sterilized, often without their informed consent. Many of these women were misled to believe that the procedures were reversible forms of birth control, when, in fact, they were permanent. This practice, rooted in eugenic policies, has had lasting impacts on Indigenous communities and their trust in the health care system. 6
Additionally, the establishment of racially segregated “Indian hospitals” further deepened mistrust. Operating from the 1930s to the 1980s, these institutions were initially created to address tuberculosis but later functioned as general hospitals exclusively for Indigenous people in Canada. Indigenous patients often experienced substandard care, isolation from their communities, and were subjected to medical procedures without proper consent. By 1960, the government owned 22 such hospitals with more than 2200 beds, primarily in Ontario and western provinces. 7
Beyond these systemic injustices, the arrival of Europeans in North America brought diseases that decimated Indigenous populations and severely strained their traditional healing systems. 8 Colonial policies, including amendments to the Indian Act (1876) that criminalized Indigenous healing practices, also further marginalized Indigenous health. 8 These policies and social, economic, and political changes have reinforced power imbalances that continue to shape Indigenous health care experiences and contribute to enduring health disparities. 9
For instance, Indigenous populations in Canada face a significantly higher prevalence of type II diabetes, which is directly linked to historical trauma and land dispossession. 10 Moreover, housing conditions on reserves are often inadequate and contribute to higher rates of respiratory illness and mental health issues. 11 From these factors, we see the impact of settler colonialism and systemic racism on Indigenous health.
Although there is evidence of the continuous impact of systemic racism on the well-being of Indigenous populations, there is a lack of studies that focus on MAID. Therefore, by means of this scoping review, we explore the current state of the literature on the topic of Indigenous peoples in Canada and MAID services. By examining existing policies and legal frameworks, we seek to understand how they consider—or fail to consider—Indigenous peoples’ unique needs and rights. Despite the growing body of research on MAID in Canada, there is a noticeable gap in the literature regarding Indigenous perspectives. Many existing studies and policies have been developed without adequately addressing the unique cultural and spiritual considerations of Indigenous populations. Through this scoping review, we highlight these gaps, ensuring that future health care policies and practices are aligned with Indigenous values and needs. See Table 1 for key takeaways from this article.
Key Takeaways
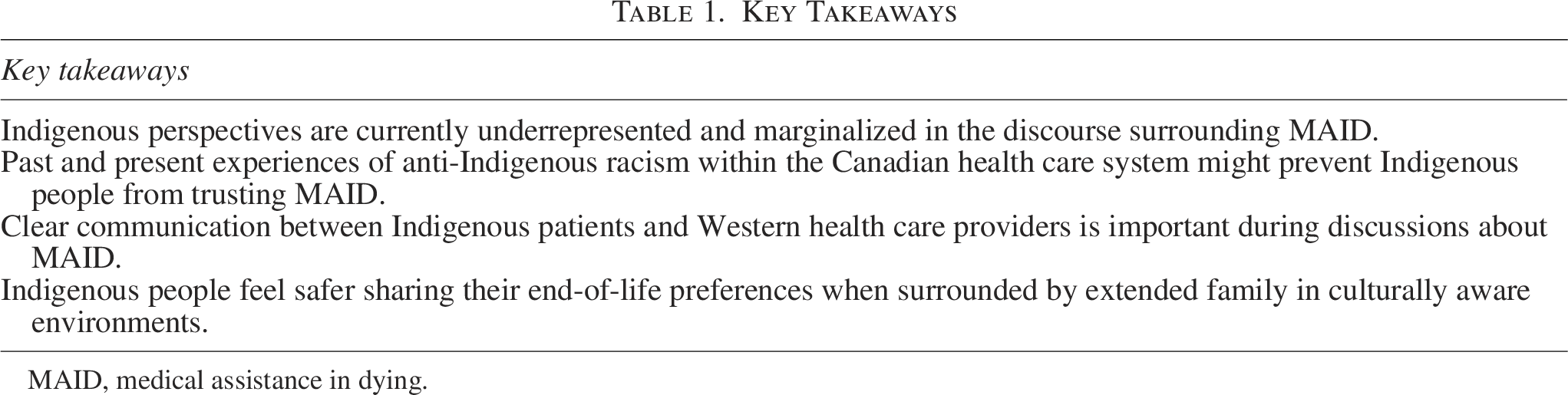
MAID, medical assistance in dying.
Materials and Methods
We used the methodological framework for scoping studies developed by Arksey and O’Malley to guide our research process. 12 A Senior Indigenous Research Member, P.F., was involved throughout this process to uphold Indigenous research methodological principles in the research process. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews Checklist was used to report the methods of this scoping review. 13
Framework stage 1: Identifying the research question
Defining goals of research at the study’s outset guided the search strategy for the scoping review. Our goal was to examine the current state of the literature on the topic of Indigenous peoples in Canada and MAID services. The term “Indigenous” was defined to include people who self-identified as Indigenous and lived on or off reserve. In Canada, there are three groups of Indigenous peoples: First Nations, Inuit, and Métis.1,14 First Nations peoples were the first inhabitants of Canada. The Métis are of mixed European and Indigenous descent, and the Inuit live in Canada’s northern regions.15,16 The Indian Act (1876) identifies two subcategories of First Nations peoples: Status Indians and Non-Status Indians. Status Indians are First Nations registered with the federal government, while Non-Status Indians are not. 17
Framework stage 2: Identifying relevant studies
This process involved defining eligibility criteria and searching electronic databases for research evidence. The eligibility criteria were defined at the outset of this scoping review and related to the type of study, type of intervention, MAID recipient group, and MAID administrator group.
Eligibility criteria
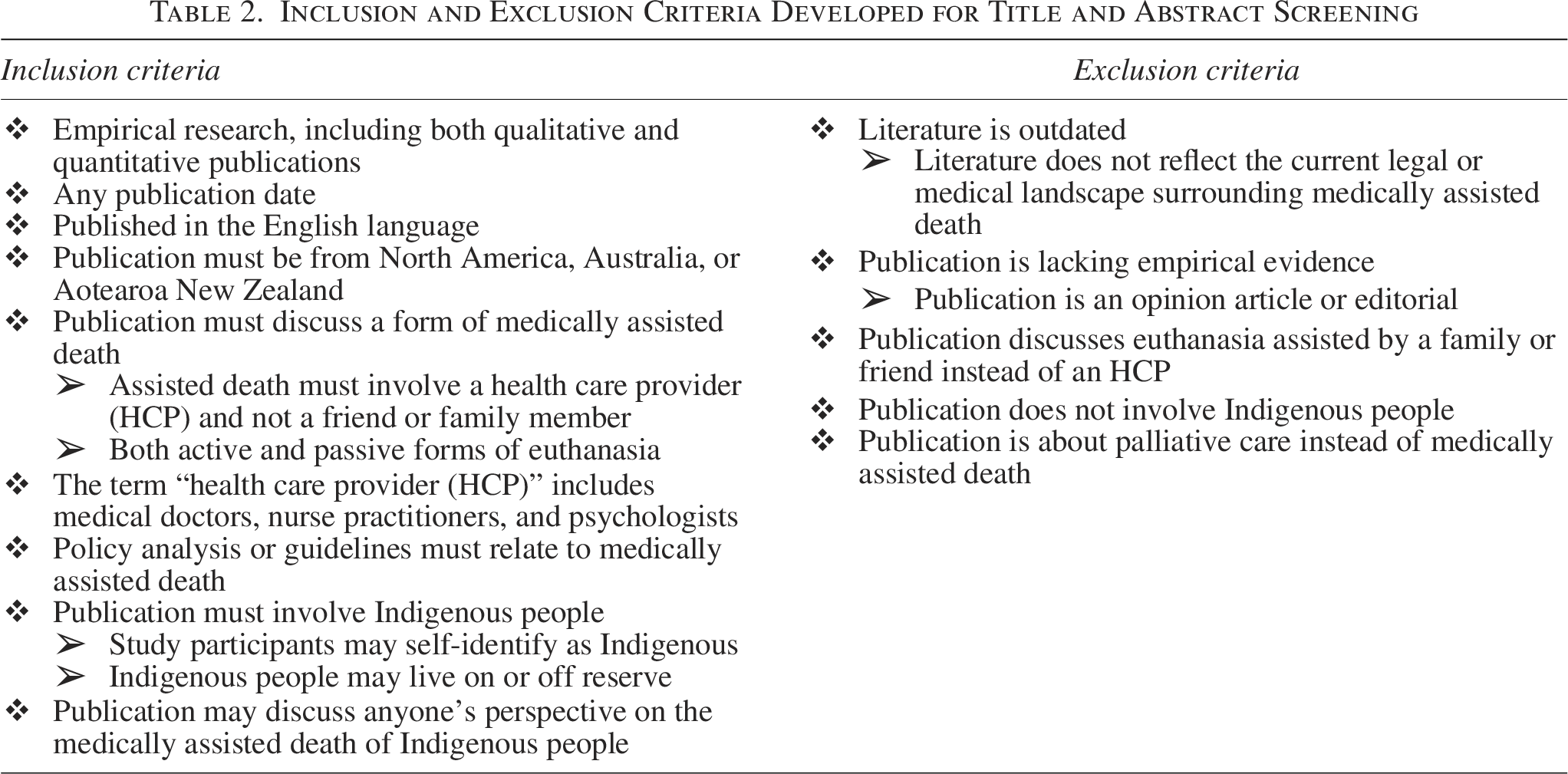
To be eligible for inclusion in the review, all papers needed to be (1) empirical research; (2) of any publication date; (3) published in the English language; (4) published from North America, Australia, or Aotearoa New Zealand; (5) discussing either passive or active euthanasia involving a health care provider (HCP) instead of a friend or family member; (6) using term “healthcare provider (HCP)” to refer to only medical doctors, nurse practitioners, and psychologists, since medical doctors and nurse practitioners are the only two HCPs who are eligible to administer MAID in Canada and psychologists provide patients with information about MAID and determine the individual requesting MAID’s capacity to provide fully informed consent,18,19 (7) analyzing only policy and/or guidelines related to medically assisted death, (8) involving Indigenous people who may self-identify as Indigenous and live on or off reserve to maintain comprehensiveness since this population is already underrepresented in literature, (9) discussing anyone’s perspective on the medically assisted death of Indigenous people, also to maintain comprehensiveness. Publications that did not meet this eligibility criterion were excluded. Papers were also excluded if they were outdated and did not reflect the current legal or medical landscape surrounding medically assisted death. Lastly, articles about palliative care instead of medically assisted death were excluded. See Table 2 for a complete list of the eligibility criteria.
Inclusion and Exclusion Criteria Developed for Title and Abstract Screening
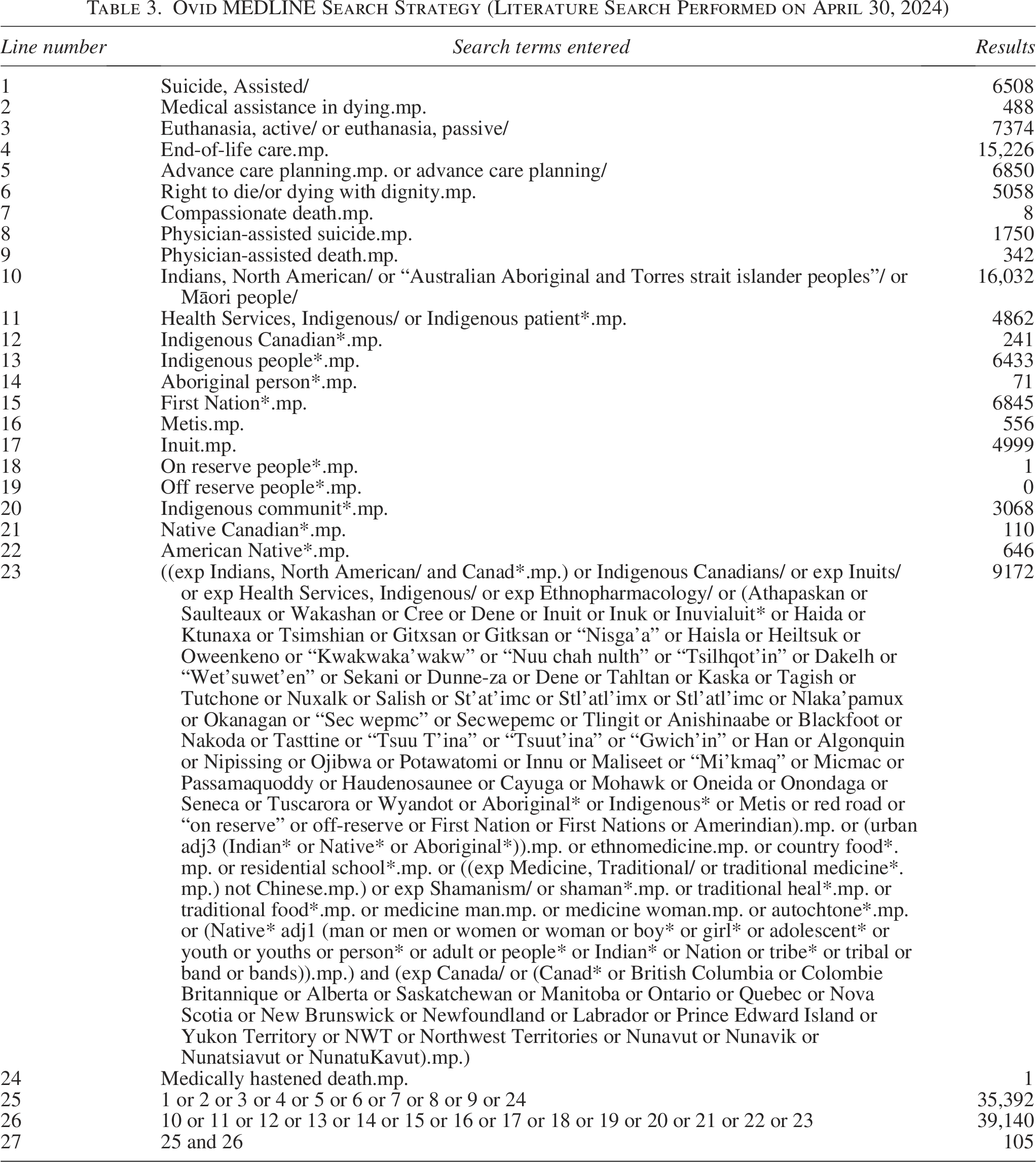
The following bibliographic databases were searched for relevant publications: Ovid MEDLINE, CINAHL, Web of Science, Embase, Emcare, PsychINFO, the Informit Indigenous Collection, and I-Portal: Indigenous Studies Portal. A senior librarian and Health Sciences Library assistants at McMaster University refined the terms of the database search. The search dates included articles published from database inception until April 30, 2024. The number of results from each database is written in Figure 2. See Table 3 for the final Ovid MEDLINE search strategy. All final search results were exported into Covidence on the same date (April 30, 2024).
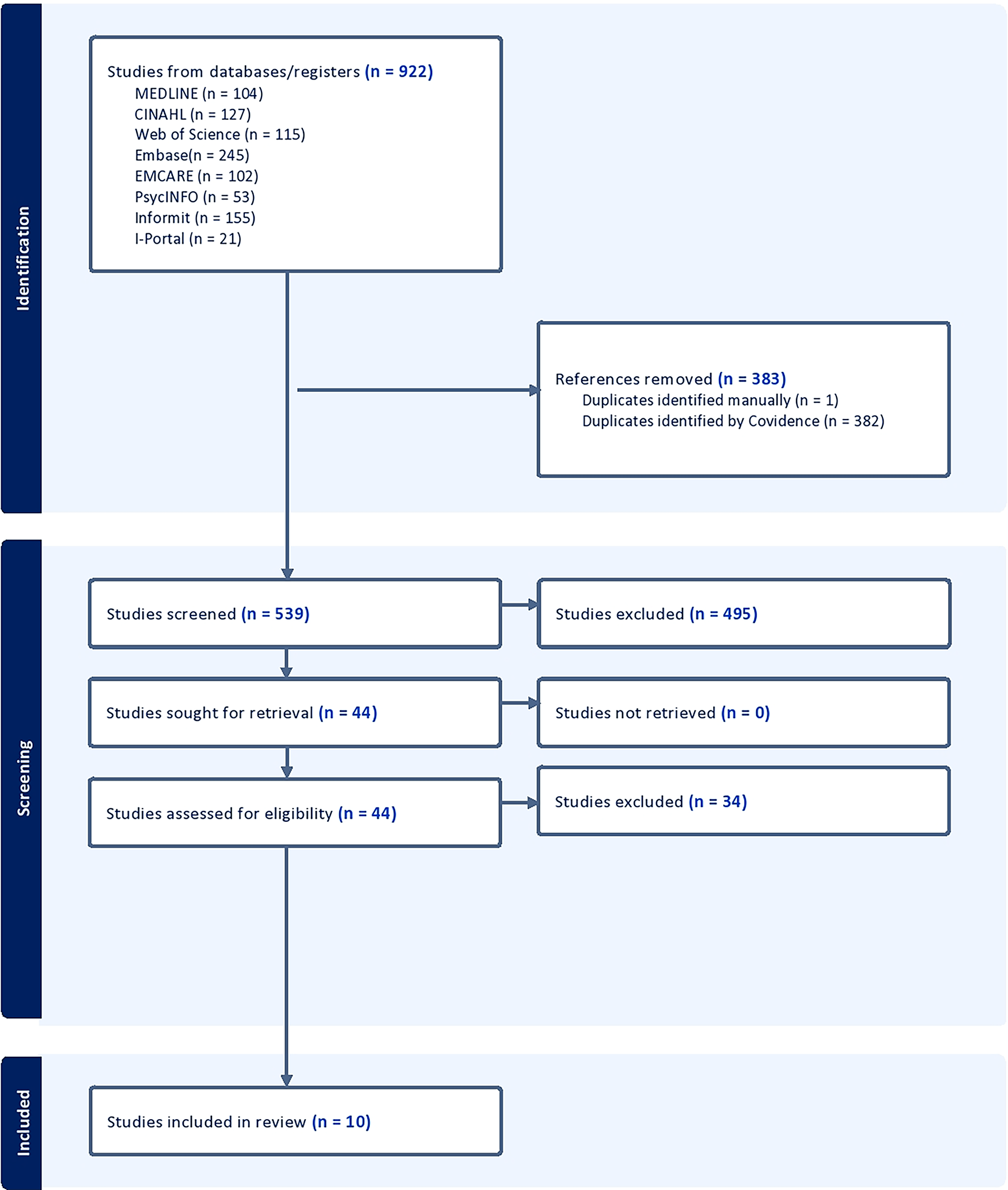
PRISMA flow diagram for the scoping review of the barriers and facilitators Indigenous populations face with MAID in Canada. PRISMA, The Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Ovid MEDLINE Search Strategy (Literature Search Performed on April 30, 2024)
Framework stage 3: Study selection
A total of 539 publications were identified from the electronic databases as potentially relevant. Two reviewers, N.P.R. and G.B., screened the titles and abstracts of each of these publications to maximize consistency. P.F. dealt with any disagreements and made a final decision on the studies that would be included in the full-text screening. A total of 383 duplicates were identified and removed through Covidence, 44 publications were sent for full-text screening, and 10 met the eligibility criteria and were marked for inclusion (Fig. 2).
Framework stage 4: Charting the data
Two reviewers, N.P.R. and G.B., collaborated to develop a data-charting spreadsheet to determine which variables to extract. Key study characteristics and detailed descriptions of themes relevant to the aims of this scoping review were captured using this tool. The two reviewers screened relevant articles for suitability of inclusion in the review. Abstracted data included article characteristics (publication author, publication title, type of publication, year of publication, study location, study populations, study aims, methods, outcome measures, and essential results), study themes that were relevant to the objectives of this scoping review along with supporting evidence for these themes, labels marking the studies for inclusion or exclusion and the Covidence number and reference ID of each study.
Framework stage 5: Collating, summarizing, and reporting the results
To ensure a systematic approach, all relevant findings were extracted and organized into an inductive coding framework. N.P.R. and G.B. conducted an initial categorization based on recurring themes identified in the studies. These preliminary categories were then discussed, refined, and consolidated into four overarching themes. The final selection of themes was based on their recurrence across multiple studies and their relevance to MAID in Indigenous populations. This process ensured that the themes reflected the most significant barriers and facilitators in the literature.
The ten articles included were analyzed using qualitative thematic analysis. The articles’ key findings were categorized into four themes: Cultural Sensitivity and Safety, Community and Family Involvement, Communication Barriers, and Policy and Legislative Considerations.
Results
This section presents the findings from ten key articles exploring Indigenous populations’ experiences and perspectives on MAID and end-of-life care. The ten articles included in this review vary in geographic focus and methodological approach. Across these studies, eight used qualitative design (e.g., semi-structured interviews, focus groups, ethnography, or critical discourse analysis), one adopted a mixed-methods framework combining surveys with qualitative interviews, and one was a qualitative policy analysis. Stating these designs at the outset helps contextualize the thematic analysis that follows. Six studies were conducted in Canada and examined First Nations, Métis, and Inuit perspectives on end-of-life care and cultural safety. These studies highlight the role of community involvement, systemic health care barriers, and culturally safe practices within Indigenous health care settings in Canada. The remaining four studies originate from New Zealand and Australia as they focus on Māori and Indigenous Australian perspectives on assisted dying. Although these non-Canadian studies offer valuable comparative insight, Indigenous nations are not homogeneous. Māori, Indigenous Australian, and First Nations, Métis, and Inuit peoples each possess distinct historical, spiritual, and sociopolitical contexts that shape end-of-life values. Findings should therefore be interpreted with this cultural heterogeneity in mind.
The objectives of the studies included in this review also vary. Some studies focus specifically on MAID-related issues, while others explore broader themes of Indigenous health care, such as cultural safety, family involvement, and communication barriers. Given the limited availability of literature on this topic, including studies from comparable Indigenous communities worldwide, provides a more holistic understanding of potential challenges and considerations. We categorized these findings into four themes and highlighted Indigenous peoples’ cultural, spiritual, and systemic challenges when accessing health care services, including MAID.
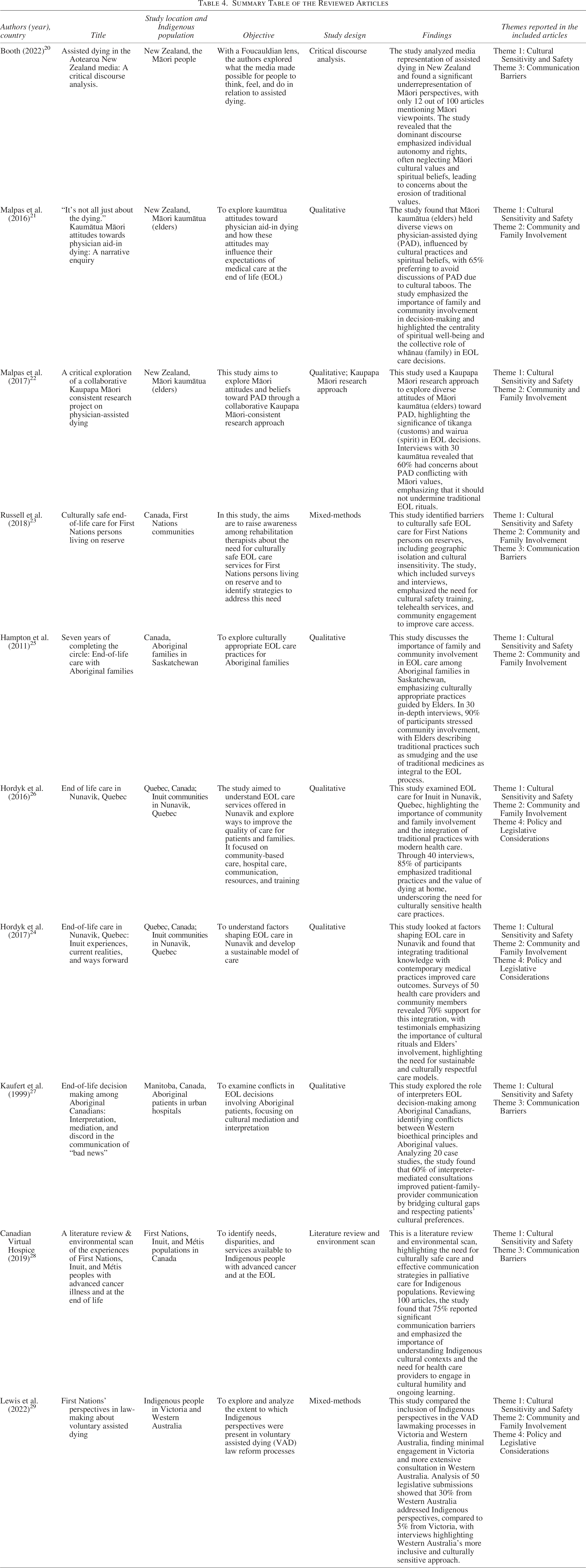
See Table 4 for a summary of the reviewed articles.
Summary Table of the Reviewed Articles
Cultural sensitivity and safety
Cultural sensitivity and safety are crucial in health care, especially when dealing with end-of-life care and MAID. Health care practices must respect and incorporate values for Indigenous populations whose cultural and spiritual beliefs are important in health and well-being. Processes must be in place to actively consider the perspectives of Indigenous people when identifying and creating resources and services for MAID. Without this consideration, the voices and needs of this population are not heard, and this can result in an unsafe health care environment.
A key finding across multiple studies, including Booth and Malpas et al., is the underrepresentation and marginalization of Indigenous perspectives in the discourse surrounding MAID.20,22 Booth and Malpas et al. reveal that Indigenous cultural practices, such as the Māori concepts of tikanga (customs) and wairua (spirit), are often overlooked in favor of Western notions of individual autonomy. This neglect can lead to mistrust in the health care system. Malpas et al. noted that 65% of Māori kaumātua (elders) preferred to avoid physician-assisted death (PAD) discussions due to cultural taboos. 22
The authors of these studies also emphasize the importance of HCPs receiving cultural safety training to understand and respect Indigenous values better. Russell et al. found that 78% of HCPs surveyed lacked training in cultural safety, which contributed to feelings of mistrust and experiences of discrimination among Indigenous community members. 23 Furthermore, Hordyk et al. highlight the successful integration of traditional knowledge with contemporary medical practices in Nunavik, with 70% of HCPs and community members supporting this approach. 24 This integration not only improved care outcomes but also respected and preserved Inuit cultural practices.
Community and family involvement
For many Indigenous communities, health and well-being are not just individual concerns but are deeply rooted in family and community connections. Indigenous people often emphasize collective decision-making, with family members and community leaders playing a key role in guiding care practices.
Hampton et al. found that 90% of Indigenous families in Saskatchewan stressed the importance of family and community involvement in end-of-life decisions. 25 Indigenous elders play a crucial role in guiding culturally appropriate care practices. This approach contrasts with non-Indigenous cultures, where end-of-life decisions are often more individualistic. Elders described traditional practices, such as smudging and using traditional medicines, as integral to the end-of-life process. Similarly, Hordyk et al. and Hordyk et al. emphasized the community and family’s critical role in end-of-life care for Inuit in Nunavik, Quebec. In their studies, 85% of Inuit community members highlighted the significance of traditional practices. Moreover, those interviewed in 40 interviews revealed that balancing traditional Inuit customs with medical interventions was necessary.24,26 The value of dying at home and being surrounded by family and community was a recurring theme by which the authors demonstrated the importance of culturally sensitive health care practices that respect and incorporate Inuit cultural values.
Moreover, Hordyk et al. identified systemic barriers to end-of-life care in Nunavik, such as geographical isolation and limited health care infrastructure. 26 The authors of this study emphasized the need for policy changes to address these barriers and improve access to care. The authors of this study conducted surveys with 60 Inuit community members and HCPs, with 80% reporting significant challenges related to geographic isolation. The interviewees revealed that many Inuit felt the health care system did not adequately address their needs due to a lack of infrastructure and culturally insensitive practices. From these findings, the authors illustrate how broader health care access issues and policy development challenges intersect and amplify concerns about the ability of community to be involved in an Indigenous person’s end-of-life care.
Barriers to communication and autonomy
Effective communication is a cornerstone of quality health care—particularly in sensitive areas such as end-of-life care and MAID. For Indigenous populations, communication barriers often arise due to differences in language, cultural expressions, and health care expectations. These barriers can lead to misunderstandings, mistrust, and a lack of engagement with health care services.
The authors of the studies reviewed demonstrate such challenges. Kaufert et al. explored the role of interpreters and cultural mediators in end-of-life decision-making among Indigenous people in Canada. The authors of this study found that 60% of interpreter-mediated consultations improved patient-family-provider communication by bridging cultural gaps. Kaufert et al. illustrate the importance of culturally competent communication strategies that respect communal decision-making and maintain hope. These are central to many Indigenous cultures. 27 Moreover, Canadian Virtual Hospice emphasizes this need for cultural safety and effective communication as well. From their review of 100 articles and reports, Canadian Virtual Hospice found significant communication barriers, such as language differences, mistrust of HCPs, and a lack of culturally appropriate communication methods. Canadian Virtual Hospice highlights the necessity for HCPs to engage in cultural humility and continuous learning about Indigenous cultures to overcome these barriers and ensure that Indigenous patients receive the information and support they need to make informed decisions. 28
Policy and legislative considerations
Policies and legislation surrounding MAID are critical in shaping how these services are accessed and delivered. For Indigenous populations, it is important that these policies respect cultural and spiritual beliefs. The federal MAID policies were primarily developed through legislative processes, including the introduction and passage of Bill C-14 (2016) and Bill C-7 (2021). These bills involved consultations with medical experts, ethicists, and public consultations.2,3 However, limited documentation is available on consultations with Indigenous communities during the development of these policies. While some regions, such as Western Australia, have taken steps to include Indigenous voices in voluntary assisted dying legislation, similar efforts in Canada remain minimal.
The legal landscape of MAID is evolving as there are ongoing discussions about expanding eligibility criteria, particularly regarding individuals with mental illnesses and mature minors. As these progressions occur, policymakers must actively consult Indigenous governance structures, elders, and health care leaders. Without such consultation, MAID risks becoming another health care service that Indigenous people feel distrust toward.
Lewis et al. compared the inclusion of Indigenous perspectives in the voluntary assisted dying (VAD) lawmaking process in Victoria and Western Australia. 29 The authors of this study found that the lawmaking process in Victoria involved minimal engagement with Indigenous communities, whereas the process in Western Australia involved more extensive consultation and consideration of Indigenous views. The study analyzed 50 submissions to VAD legislative processes, with 30% from Western Australia explicitly addressing Indigenous perspectives compared to 5% from Victoria.
In Australia, the Rights of the Terminally Ill Act 1995 (NT) was passed in May 1995, and this was the first law in the world to legalize assisted dying. 30 The studies above indicate that Australia has taken some initiative to consider Indigenous peoples’ perspectives during the development of its assisted dying policy. The MAID policy in Canada was introduced only recently, in June 2016, but there is still no evidence that the perspectives of Indigenous people in Canada are being considered during its evolution. 31 While the studies from Australia offer insights into Indigenous perspectives on MAID, their direct applicability to Canada is limited due to differences in legal frameworks and governments. Some jurisdictions in Australia have more structured Indigenous representation in policy discussions, whereas Canada has yet to fully integrate Indigenous leadership into MAID policymaking. Despite these differences, key themes from the studies are consistently relevant.
To conclude this section, the findings from the ten articles we included underscore the importance of culturally sensitive approaches to end-of-life care for Indigenous populations. Integrating traditional practices, ensuring effective communication, involving Indigenous perspectives in policymaking, and addressing systemic barriers are essential to providing respectful care at the end of an Indigenous person’s life.
Discussion
Our results indicate a limited number of studies focusing specifically on Indigenous experiences with medically assisted death, since only ten publications met the eligibility criteria. The intersection of Indigenous peoples in Canada and MAID has never been examined before, which could explain our small number of results. However, this small number also supports why a scoping review like this is necessary. Also important to note is that among the ten publications that were included, none discussed both Indigenous peoples in Canada and MAID, further highlighting the gap in the literature. In this section, we summarize our findings from the four overarching themes and list considerations for future research on the topic of MAID and Indigenous peoples in Canada.
Cultural sensitivity and safety
In summary, the commonality across the studies in this category is the recognition that culturally sensitive approaches that actively engage Indigenous communities are essential when delivering end-of-life care to Indigenous populations. The need for cultural safety training, the inclusion of Indigenous perspectives in policymaking, and the integration of traditional practices are essential steps toward ensuring that end-of-life care is delivered in a culturally safe and respectful manner. Although Indigenous perspectives pertaining to medically assisted death are diverse, more than half of the Māori elders interviewed by Malpas et al. preferred to avoid discussions pertaining to death due to cultural taboos. The Ministry of Health of New Zealand has reported a few reasons why some Māori elders avoid such discussions in the Review of the End of Life Choice Act 2019. In this review, the authors report that some Māori people believe the body should perish naturally since the wairua (spirit) belongs to God, while others are opposed to assisted dying since they prefer using their whanau (family) support system at the end of life or believe that assisted death would distress their family. 32 Further research is needed to examine Indigenous perspectives and cultural safety pertaining to MAID in Canada.
Community and family involvement
The authors of the studies in this category reveal that effective end-of-life care for Indigenous populations must respect the role of family and community. Incorporating such values ensures that care decisions are made in a culturally congruent and supportive environment, essential for providing respectful and effective care at the end of an Indigenous person’s life. From the current literature, it is understood that Indigenous people prefer having their family and community around when discussing end-of-life options with their HCPs. Dawe et al. write about the importance of family involvement during end-of-life care of Innu people in Canada, sharing that when an Innu person is dying or sick, there are always people at the house providing support for this person by cooking, talking, and praying. This is one of many examples highlighting the necessity of incorporating community into end-of-life care services. 33 To better understand how this pertains to conversations surrounding MAID, opinions are needed from Indigenous communities in Canada. These opinions could be gathered from surveys and/or focus group interviews. This data is currently absent from the literature.
Barriers to communication and autonomy
From the findings in this category, we see that addressing communication barriers is essential for enabling Indigenous patients to fully engage in their health care decisions when receiving palliative care. Ensuring that communication strategies are culturally sensitive and inclusive is vital to respecting the autonomy and preferences of Indigenous patients in end-of-life care. For instance, Johnston et al. report that Mi’kmaq people in Canada avoid using the term “end-of-life” since the Mi’kmaq people view death as a continuation into the next life. Therefore, different terminology should be used when discussing death with the Mi’kmaq community. 34 To better understand the effect of communication barriers in relation to Indigenous people and MAID, more input from Indigenous communities in Canada is needed. For example, interviews could be held, and findings from these conversations could be added to the literature.
Policy and legislative considerations
The common thread between the studies in this category is the critical need for policy and legislative frameworks to be developed in consultation with Indigenous communities. The legal landscape of MAID is evolving as there are ongoing discussions about expanding eligibility criteria, particularly regarding individuals with mental illnesses and mature minors. As these progressions occur, policymakers must actively consult Indigenous governance structures, elders, and health care leaders. Such engagement is essential to assess whether MAID practices are culturally appropriate, supportive of Indigenous rights and autonomy, and responsive to the unique challenges faced by Indigenous populations in accessing end-of-life care. Without such consultation, MAID risks becoming another health care service that Indigenous people feel distrust toward. Future research should explore how international approaches can be adapted to increase Indigenous consultation during MAID policy decision making in Canada while respecting the distinct cultural traditions of First Nations, Métis, and Inuit communities.
Limitations
One of the primary limitations of our scoping review is the limited availability of research specifically addressing Indigenous perspectives on MAID. From the scarcity of published studies on this topic, we can highlight a significant gap in the literature, which restricts the comprehensiveness of our findings. This lack of research is particularly concerning given the unique cultural, spiritual, and systemic challenges Indigenous peoples face in accessing health care services, including MAID. The absence of extensive data makes it difficult to draw robust conclusions. It suggests that the needs and perspectives of Indigenous communities have been largely overlooked in existing MAID discourse and policymaking.
However, this limitation underscores the necessity and urgency of our research. By identifying and addressing these gaps, we are contributing to an insufficiently explored critical area of inquiry by means of this scoping review. We emphasize the importance of incorporating Indigenous voices into the conversation around MAID, ensuring that future policies and health care practices are culturally sensitive.
Conclusion
This is the first scoping review examining the intersection of Indigenous peoples in Canada and MAID services. Since our results indicate a lack of literature on this topic, we call for more research looking at Indigenous peoples’ perspectives and experiences with MAID in Canada. We also highlight the critical need for a more culturally sensitive approach to MAID and end-of-life care that fully considers the unique perspectives and needs of Indigenous peoples. From our findings, we extract critical areas for improvement, including enhancing cultural sensitivity, ensuring meaningful community and family involvement, overcoming communication barriers, and integrating Indigenous perspectives into policy and legislative processes. Addressing these issues is essential for providing respectful end-of-life care and honoring Indigenous values and rights.
Moving forward, future research and policy development must prioritize including Indigenous voices to ensure that end-of-life care and MAID services are culturally appropriate and aligned with Indigenous populations’ diverse beliefs and needs. By doing so, we can work toward a more equitable Canadian health care system that truly respects and incorporates Indigenous cultural and spiritual values in end-of-life care.
Authors’ Contributions
N.P.R.: Searched databases for relevant publications; screened publications; did qualitative thematic analysis of research evidence; wrote the Methods section, Discussion section, statements and declarations, Title Page, and Cover Letter; created Table 1, Table 2, Table 3, and Figure 2; formatted images, text, and references. G.B.: Searched databases for relevant publications; screened abstracts; screened publications; did qualitative thematic analysis of research evidence; wrote Introduction section, Results section, Limitations section, Conclusions section; created Figure 1 and Table 4; formatted images, text, and references. P.F.: Provided support and guided research process according to Ownership, Control, Access, and Possession (OCAP) (R) principles and principles of Indigenous Research Methodology; edited several versions of the article. L.B.: Provided support and guidance regarding scoping review methodologies; selecting and searching databases, and reviewed iterations of the article.
Footnotes
Acknowledgments
We would like to acknowledge the invaluable guidance and support of Dr. Patricia Farrugia, an Indigenous scholar and health care professional whose insights have been instrumental in shaping this review. Dr. Farrugia’s expertise and lived experience have helped us navigate the complexities of Indigenous perspectives on MAID, ensuring that our research is conducted with the utmost cultural awareness and integrity. We are grateful for her mentorship and the opportunity to collaborate on this important work. Finally, we would like to acknowledge Laura Banfield, a librarian at the McMaster Health Sciences Library, for her guidance in generating and refining search terms, selecting databases, and providing instruction on database usage. She has also generously edited this article.
Author Disclosure Statement
N.P.R. and G.B., the primary researchers conducting this scoping review, are not Indigenous and acknowledge our positions as settlers on this land. We recognize the importance of this context in our work and have taken careful measures to approach this research with cultural sensitivity and respect. We are deeply committed to ensuring that the voices and perspectives of Indigenous peoples are accurately represented and honored in our findings.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Data are available upon request.
Ethical Considerations
Since there are no human or animal participants in this article, informed consent is not required.