
Abstract
Many clinicians are using their personal digital devices (such as smartphones) while at work for personal and professional purposes. The purpose of this research was to understand how Ontario nurses used their own digital devices within the workplace. Reported here are the findings from the on-line questionnaire of a mixed methods design. Participants (N = 169) had a mean age of 41 years, were mostly female, and with an average of 15.2 years of nursing experience. Most (73%) used their own device within the workplace for pragmatic reasons (telling time), patient care (accessing information, drug management, and administration), and communication among the healthcare team. This research offers emerging insight into how personally owned devices are being integrated into healthcare practices and highlighted tensions among workplace efficiency and enhanced team communication. This research supports the development of guidelines for personal device use within healthcare settings.
Introduction
The use of Electronic Medical Records (EMRs) and Electronic Health Records (EHRs), (collectively referred to as electronic documentation systems) is becoming widespread in Canada. 1 Electronic documentation systems have been integrated within healthcare organizations to provide a centralized and accessible source of clinical information for healthcare providers and administrators. 2 Yet, despite the increase in technological infrastructures within many healthcare organizations, many clinicians are using their personal digital devices (smartphones, smartwatches, and apps) while at work for personal and professional purposes.3,4
Background
There has been an increase in the use of digital technologies and particularly smartphones by healthcare providers in the last several years, including an increase in the use of healthcare apps. 5 Quality of care is directly influenced by healthcare providers’ ability to access timely, comprehensive, and accurate health information. 6 However, despite the increase in technological infrastructures (e.g. patient documentation systems) among many healthcare organizations to support healthcare provider practices and patient care, many Registered Nurses (RNs) and Registered Practical Nurses (RPNs) are using their own personal digital devices (smartphones and apps) while at work for personal and professional purposes. 5
Personal digital device use within healthcare settings has taken on even greater importance within the global pandemic crisis. There are anecdotal reports of healthcare providers using their own personal devices for patient and family care; instances related to life-saving decision-making using video chat with family members who were restricted from the healthcare setting about critical health decisions (acute care intubation) or to give a patient’s family member the ability to “be with” them at their time of death (long-term and end-of-life care). Despite the proliferation of digital device use in the healthcare setting, RNs’ and RPNs’ use of personal digital technologies within workplace settings is relatively unexplored within the research literature. In addition, there is limited research available that focuses on nurses’ use of health-related apps in the workplace. 7
The expectation of evidence-informed patient care practices highlights the importance of access to pertinent health-related resources among nurses and other healthcare providers. An evidence-informed framework necessitates nurses to critically evaluate all forms of health-related evidence in the provision of quality patient care. The evidence-informed practice model requires nurses to engage in a process where they make decisions based on their clinical expertise, the patient’s needs, and research evidence. Given the convenience of personal device use and associated ease of access to on-line information (healthcare resources), we are interested in understanding how RNs and RPNs across a variety of healthcare settings (acute care, long-term care, home care, and public health) are leveraging their own digital devices for personal and patient care-related purposes.
The research questions guiding this study are as follows: 1) How are Ontario-based RNs and RPNs using their personal digital technologies (e.g. personal smartphone) in their workplace and in support of their healthcare practice during pre-pandemic and current (pandemic) contexts? 2) What are the perceived effects of personal digital technology use on healthcare practice among RNs and RPNs within diverse healthcare settings?
Methods
Design
This study utilized a mixed methods approach following a sequential explanatory design.8,9 The sequential explanatory design is characterized by a two-phase structure in which quantitative data collection and analyses is conducted first and is then followed by qualitative data collection and analyses.9,10 Reported in this paper are the findings from the first phase of the study which used an on-line questionnaire to collect data.
The research was introduced to participants as a project aimed at describing RNs’ and RPNs’ use of their personal technology in support of their nursing role within diverse healthcare settings. Participants were invited to complete an on-line questionnaire hosted by Qualtrics XM 11 inquiring about the type and nature of personal digital device use within diverse healthcare settings. The time to complete the questionnaire required approximately 20 minutes. This study was reviewed and approved by the university research ethics board.
Participant recruitment was conducted using a multi-strategy approach. A convenience sample of RNs and RPNs was generated using multiple participant recruitment strategies. A list of mailing addresses was provided from the College of Nurses of Ontario (CNO) of RNs/RPNs who were working in Ontario and that had consented to be contacted for research purposes. Restricted to traditional mail services, a study package including a letter of information with a link to the on-line questionnaire was mailed to 1,900 randomly selected potential participants. As well, recruitment flyers were shared on popular social media channels to reach RNs and RPNs, working in a broad range of settings across Ontario, with the expectation that the information would be re-shared to others’ networks.
Participants were eligible to participate if they met the following inclusion criteria: (a) currently registered with the College of Nurses of Ontario; (b) currently employed full-time or part-time; and (c) practice class of RN or RPN or extended class NP. As a token of appreciation for those that participated in the questionnaire, 12 individuals were offered a chance to enter their name into a draw for a chance to win one of four $50 gift cards.
Data collection
Data were collected during the early stages of the COVID-19 pandemic, over several months that straddled 2020-2021. The on-line questionnaire inquired about participants’ basic demographic details, their workplace setting, the frequency and nature of personal device use, and perceived effects of their personal device use at work. We created a series of questions to understand how and how often participants used their personal devices to support their patient care role, to access and share information, and communicate with the healthcare team. Participants were asked to recall and report on their personal device use (excluding scheduled breaks and mealtimes) prior to the COVID-19 pandemic and also report on current use (during COVID-19 pandemic). The questionnaire included researcher-generated questions based on findings of a scoping review of the literature 5 and peer consultation with practicing nurses and nurse practitioners across healthcare settings. We also included the validated survey by McBride et al. 13 on use of personal communication devices by hospital RNs, modified for our study purpose.
Analysis
A descriptive statistical approach was used to address our research questions. The statistical analysis described the demographic information of participants, their reported healthcare setting and employment status, the type and frequency of technology use to support their nursing role, and the perceived effect of personal device use on workplace performance among self and colleagues. Wilcoxon signed-rank tests were conducted to determine differences in participants’ type and frequency of current self-reported personal device use and recall of their pre-COVID use. Mann-Whitney U tests were also conducted to determine differences in participants’ use of personal devices across settings, that is, acute care compared to community-based nursing practices. Community-based nursing practice included participants who reported working in long-term care, primary care, public health, home care, and college/university settings.
Results
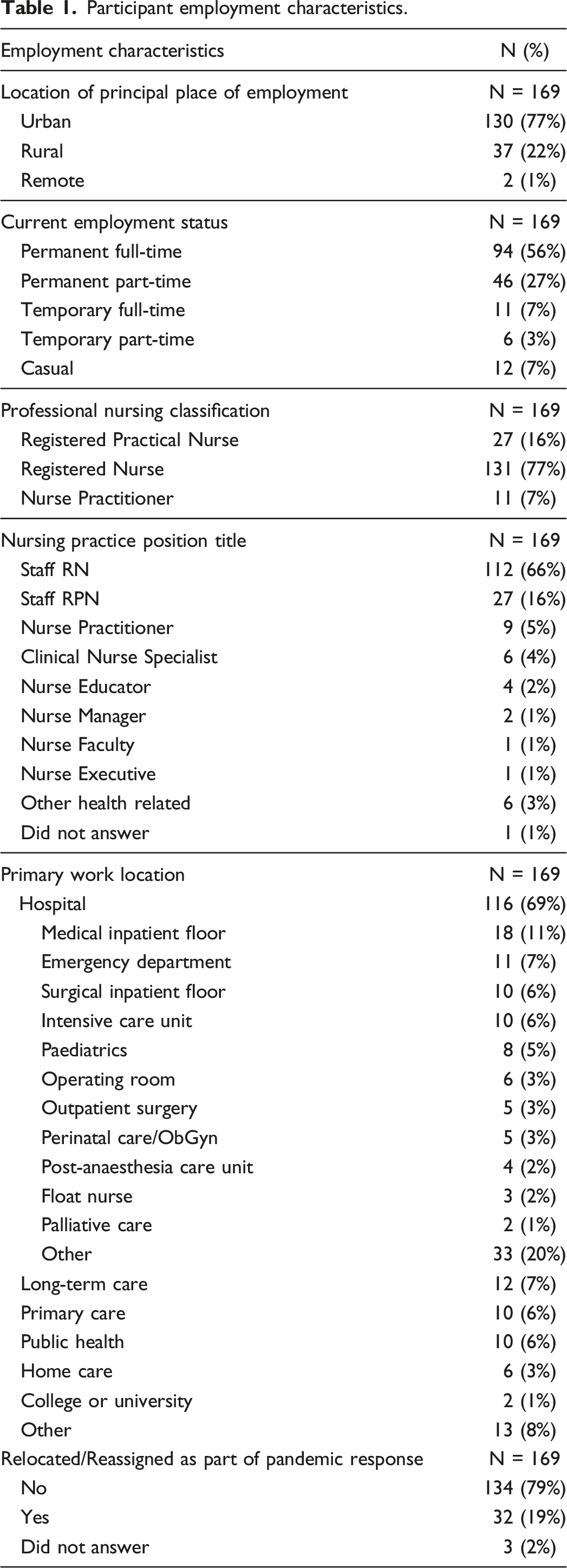
Participant employment characteristics.
Type and frequency of personal device use
The majority of participants reported owning a smartphone (N = 150, 89%) and 73% (N = 123) of participants indicated that they used their smartphone at work. When asked if their smartphone use at work had changed because of the COVID-19 context, about 14% (N = 24) responded affirmatively to pandemic-driven change in use. Participants (N = 62, 37%) also reported using personal digital devices other than a smartphone within their place of employment. The use of tablets (N = 13, 7.7%), laptops (N = 22, 13%), smartwatches (N = 27, 16%), and activity tracker (N = 20, 11.8%) were reported in addition to smartphone use.
When asked about their knowledge of organizational policy regarding the use of their personal smartphones within the workplace setting, over half of participants (N = 88, 56.8%) reported that their workplace permitted nurses’ use of personal smartphones, 23.9% (N = 37) reported their organizations did not permit personal smartphone use, and about 20% (N = 30, 19.4%) were unaware of their organization’s position on the use of personal smartphone devices within the workplace. When asked, participants reported physicians were permitted to use their personal smartphone devices within the workplace (N = 104, 61.5%), but almost 30% of participants (N = 48, 28.4%) did not know if personal smartphone use among physicians was permitted.
Type and frequency of personal device use at work
Participants used their personal devices in very pragmatic ways, as a flashlight (41.9%), and as a way to monitor time (64.4%) (see Figure 1). Current frequency of personal pragmatic work-related device use, all participants (N = 169).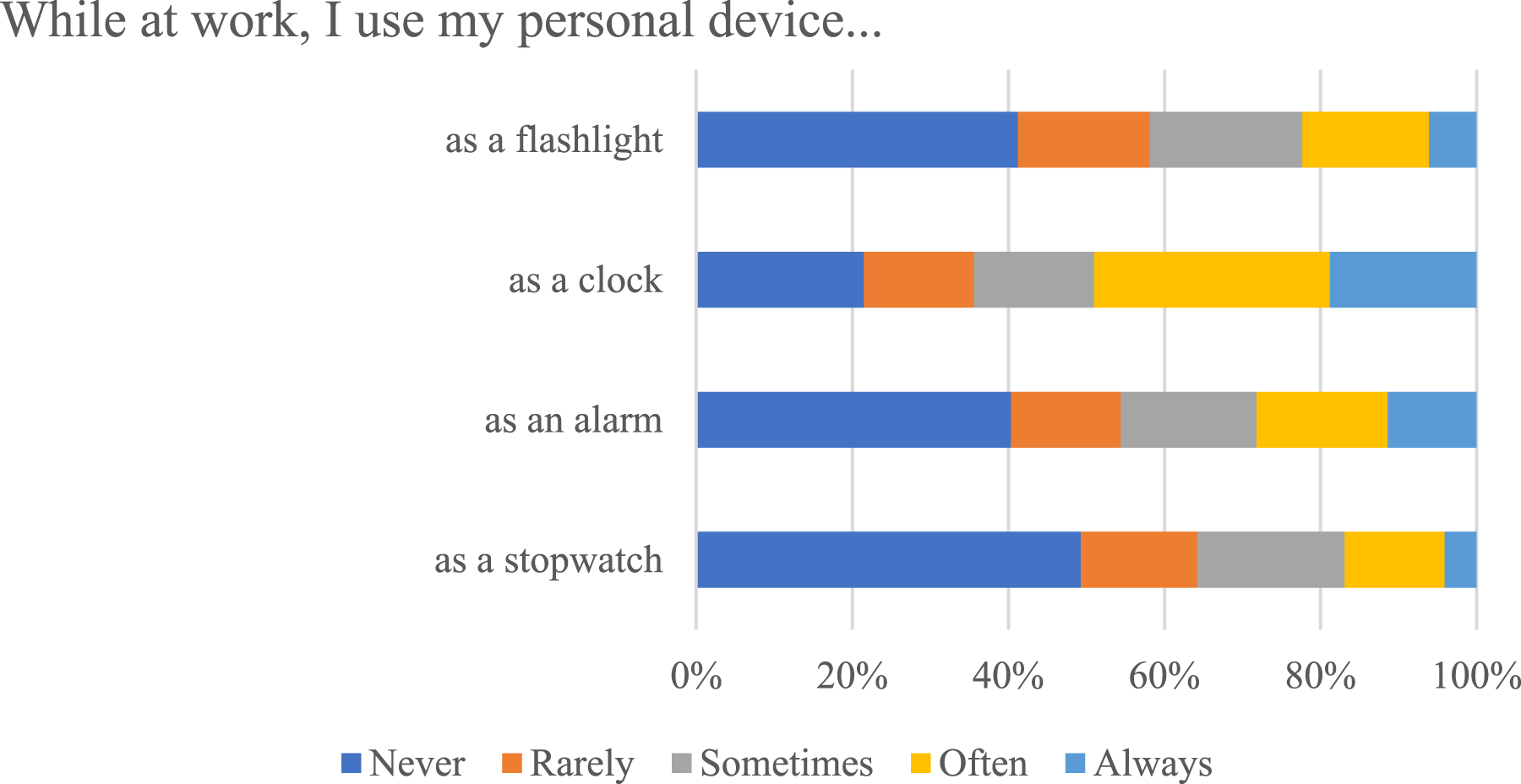
There was also a variety of ways that personal device use was leveraged for patient care purposes; participants indicated that they used their smartphones with some degree of regularity (sometimes/often/always responses) to look up patient symptoms (56.5%), treatments (48.7%), lab results (26.6%), and information about procedures (43.6%). In addition, approximately 25% of participants reported accessing patient-related on-line apps to assist them in providing patient care (see Figure 2). Current frequency of personal work-related device use for patient care, all participants (N = 169).
Noteworthy is that a majority of participants reported using their personal devices with some regularity (sometimes/often/always responses) for almost every aspect of medication management and administration. Nearly two-thirds of participants (61%) reported using their personal devices as a calculator for nursing/medical formulae and nearly half (52%) used it as a drug calculator. Additionally, participants used their personal devices to access work-related medication/drug references (54%) and to look up drug names (54%), drug contraindications (41%), drug calculations (41%), and drug interactions (see Figure 3). Approximately 12% (N=18) of participants indicated that they personally paid for apps or web site subscriptions used. Current frequency of personal work-related device use for medication management and administration, all participants (N = 169).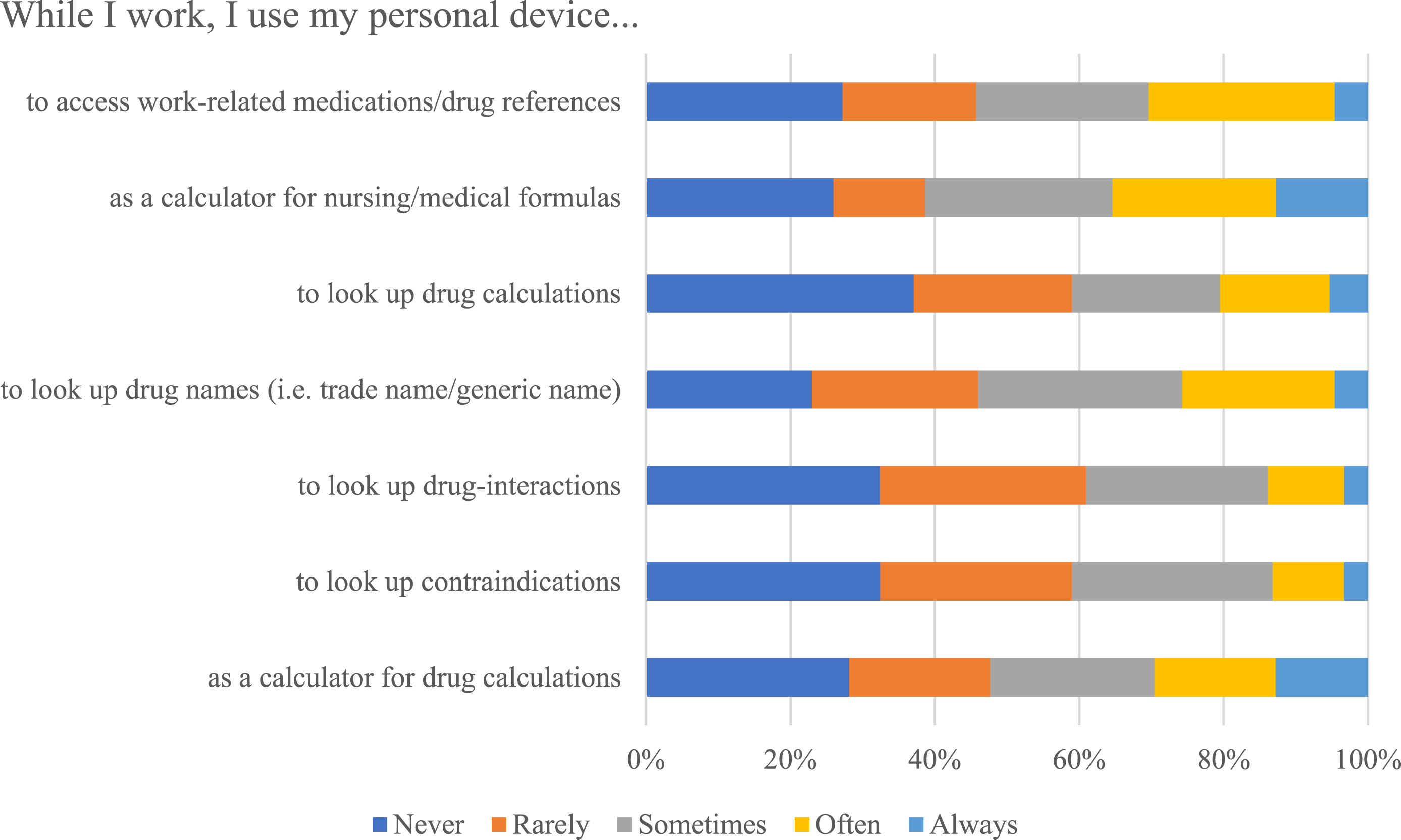
Personal device use was also utilized to support communication among the healthcare team. Almost 40% of participants sometimes/often/always used their personal devices to send and receive e-mails or texts, related to patient care, and approximately 10% of participants reported sending or viewing patient-related images or photos (see Figure 4). Open-ended responses within the survey indicated that participants communicated about staffing and work scheduling with other team members and about patient or family requests for status updates, to remind co-workers about new orders and/or patient appointments, to convey to other RNs physicians' verbal orders, to ask for assistance from someone on another floor or room, to locate colleagues on the unit, to take pictures of supplies needed for restocking or to be ordered, and to inquire about basic patient updates (“but no patient names”). When asked about unanticipated personal device use for COVID-19-related communication, participants reported use of translation functions on their personal devices among families with English as a second language and with patients who “don’t have the means to pay for their own phone.” Participants also reported the use of video communication (FaceTime) to connect patients with family. Participants also used their device as a speakerphone for family phone meetings “because of a lack of teleconferencing in meeting rooms,” to provide virtual care from home (with blocked number). One participant reported use of their personal device “as a hotspot” to gain on-line access. Participants also reported the use of popular messaging apps as a way to communicate with colleagues that were inclusive of Facebook Messenger (N = 13, 9%), iMessage (N = 37, 25.7%), WhatsApp (N = 30, 20.8%), and Instagram (N = 6, 4.2%). Participants did not indicate any workplace use of the following on-line apps: Twitter, TikTok, Line, or Viper. Current frequency of personal work-related device use for team communication, all participants (N = 169).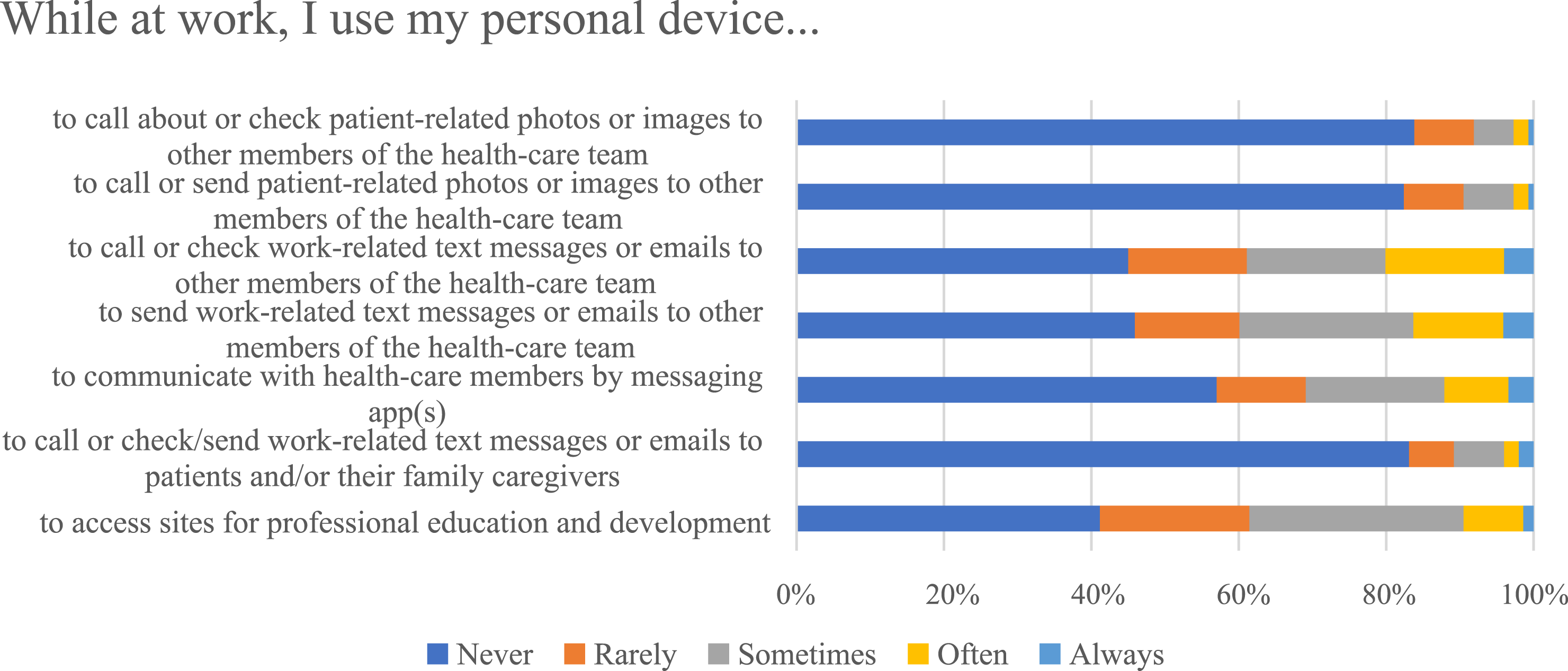
In the open-ended responses, participants reported taking photos of a patient’s rash, ulcer, ECG output, and wound, of lab work “if it seems off and I can't write it out” and to respond to physician requests for photos (dermatology consult photos). One participant reported taking pictures of a ventilator setting before and after making changes “to have a record and easily revert to old settings if the patient’s condition changed or deteriorated” and another participant conveyed that they did not send a photo but would take a photo to show the physician and then delete it.
Participants also reported use of their devices for personal entertainment and communication while at work. On-line activity included gaming and shopping (24.8% sometimes/often/always responses) and time spent on social media sites (27.5% sometimes/often/always responses) and to communicate with family members or friends (43.5% sometimes/often/always responses) (see Figure 5). Current frequency of device use for entertainment and personal communication, all participants (N = 169).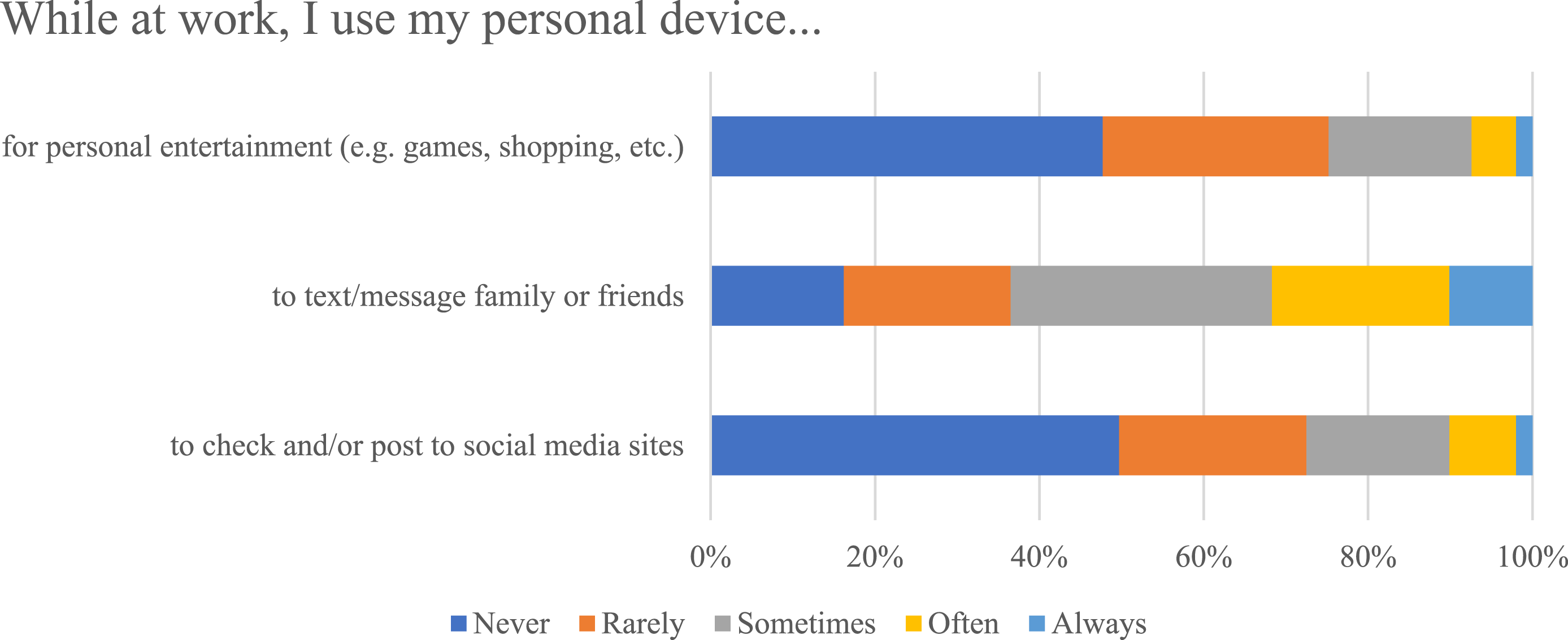
Participants also reported the use of their personal digital devices to monitor family member activity and/or safety (8% sometimes, often, always responses) and as a personal safety strategy (20.8% sometimes, often, always responses) (see Figure 6). Current frequency of device use for personal/family safety, all participants (N = 169).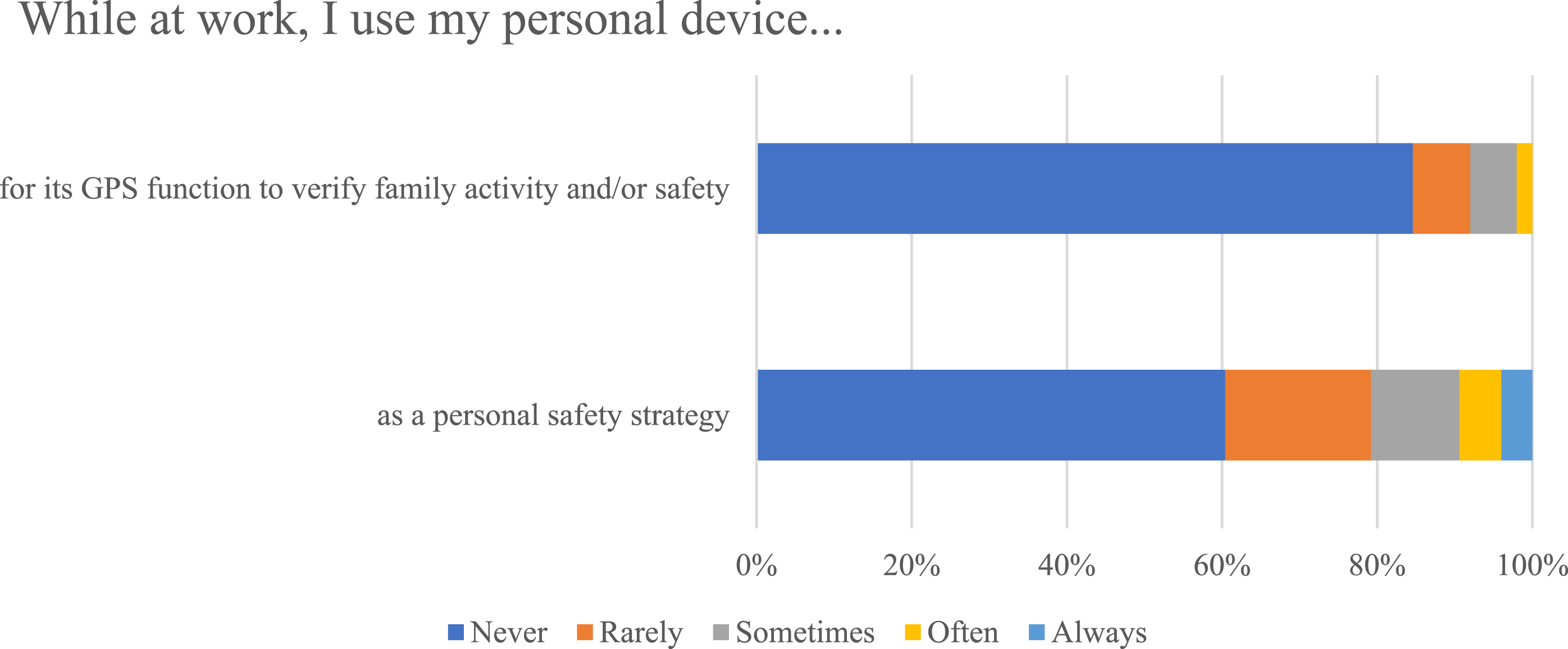
Current use vs. pre-pandemic use of personal technology
Frequency of personal device use at work for work-related activities before the pandemic and current behaviours, all participants (N = 169).
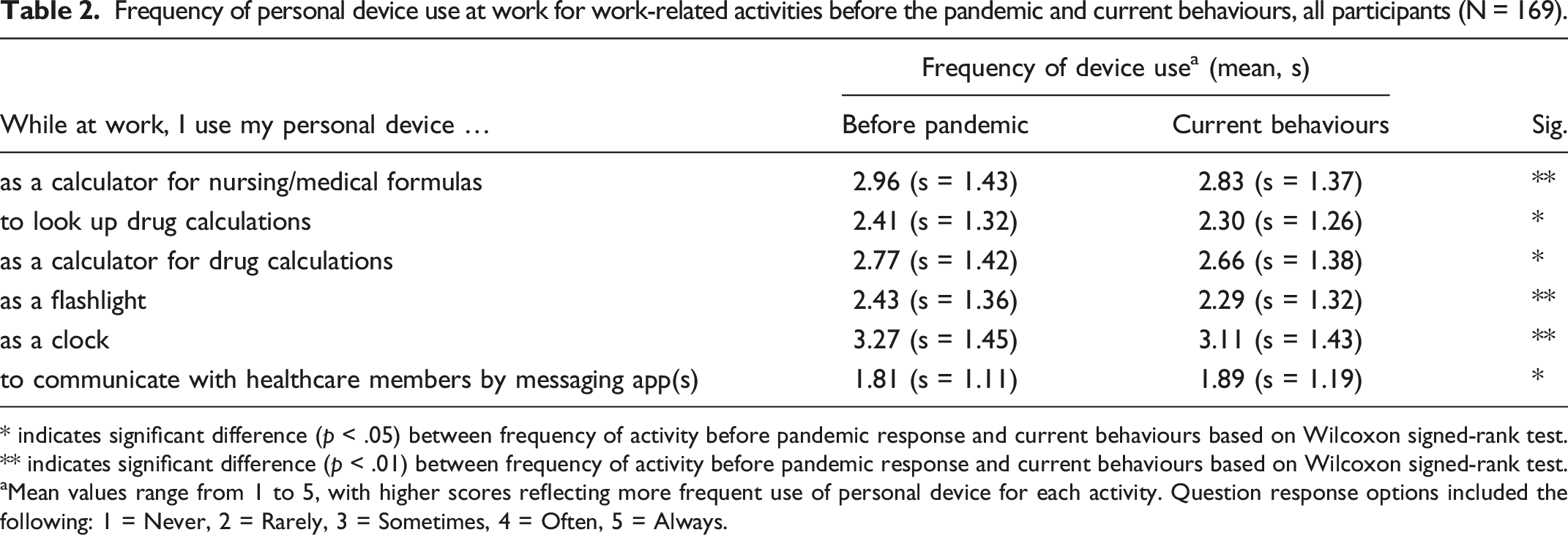
* indicates significant difference (p < .05) between frequency of activity before pandemic response and current behaviours based on Wilcoxon signed-rank test.
** indicates significant difference (p < .01) between frequency of activity before pandemic response and current behaviours based on Wilcoxon signed-rank test.
aMean values range from 1 to 5, with higher scores reflecting more frequent use of personal device for each activity. Question response options included the following: 1 = Never, 2 = Rarely, 3 = Sometimes, 4 = Often, 5 = Always.
Hospital vs. community-based personal device use for work-related activities
Current frequency of personal device use at work for work-related activities and hospital settings compared with community settings.
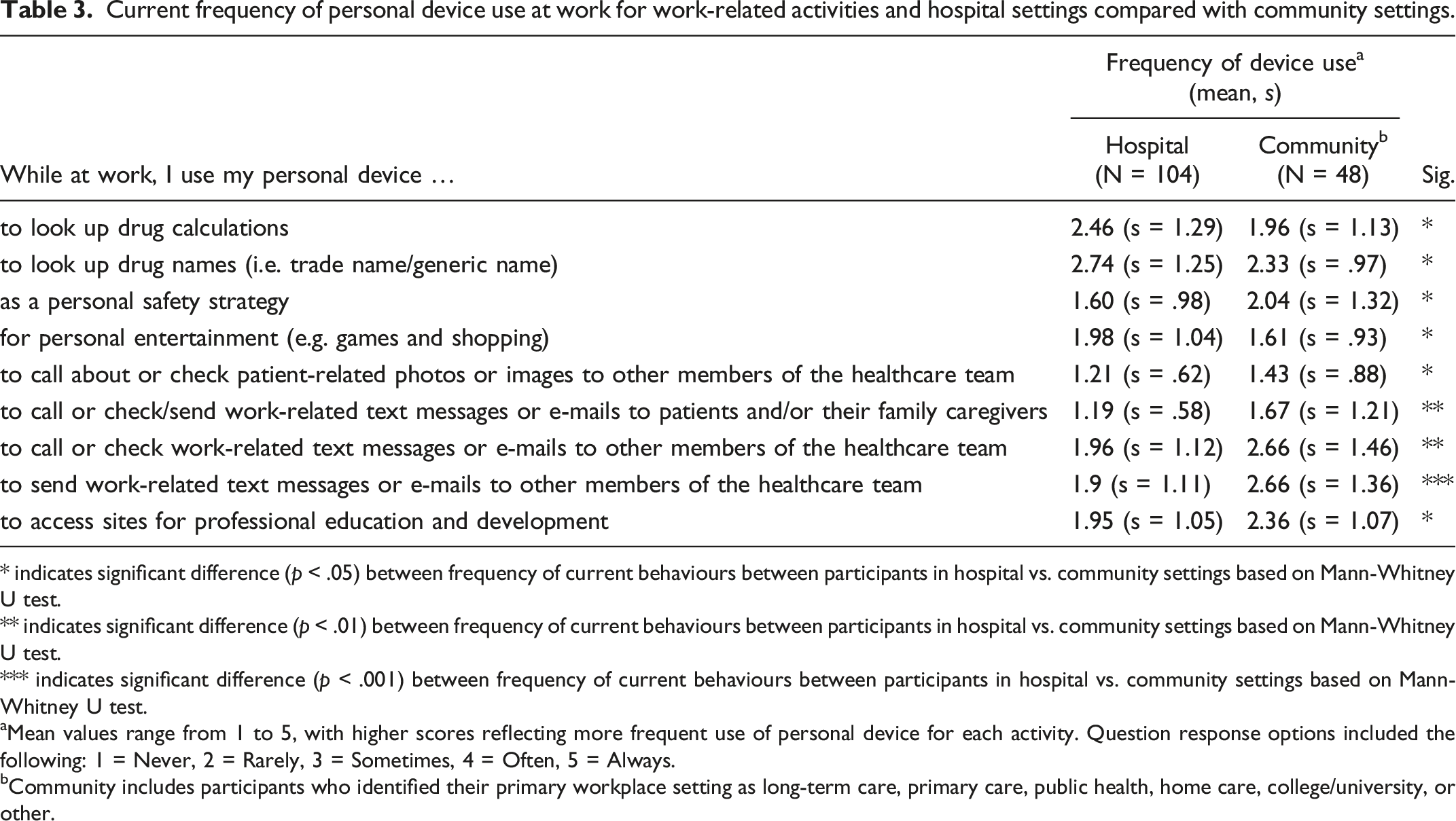
* indicates significant difference (p < .05) between frequency of current behaviours between participants in hospital vs. community settings based on Mann-Whitney U test.
** indicates significant difference (p < .01) between frequency of current behaviours between participants in hospital vs. community settings based on Mann-Whitney U test.
*** indicates significant difference (p < .001) between frequency of current behaviours between participants in hospital vs. community settings based on Mann-Whitney U test.
aMean values range from 1 to 5, with higher scores reflecting more frequent use of personal device for each activity. Question response options included the following: 1 = Never, 2 = Rarely, 3 = Sometimes, 4 = Often, 5 = Always.
bCommunity includes participants who identified their primary workplace setting as long-term care, primary care, public health, home care, college/university, or other.
Perceived effects of technology use
A majority (74%) of participants agreed or strongly agreed that having access to their personal smartphone while at work was useful. About 1/3 of participants (31.5%) agreed or strongly agreed that it would be harder to provide good patient care without the use of their personal smartphone within the workplace and 44.8% of participants agreed or strongly agreed that the use of their personal smartphone supported and offered a beneficial impact to patients. Participants agreed or strongly agreed that personal smartphone use positively affected workplace efficiency (40.9%), reduced work-related stress (46.9%), improved patient safety (26.8%), and improved healthcare team cohesion and teamwork (33.6%), including coordination of patient care (30.4%). Over 80% of participants strongly disagreed or disagreed (83.8%) with the statement that their personal smartphone use negatively affected their workplace performance. Interestingly, 53.8 % participants agreed or strongly agreed that other nurses’ use of their personal smartphone device at work as negatively affecting their workplace performance (see Figure 7). Perceived effects of personal device use at work for work-related activities, all participants (N = 169).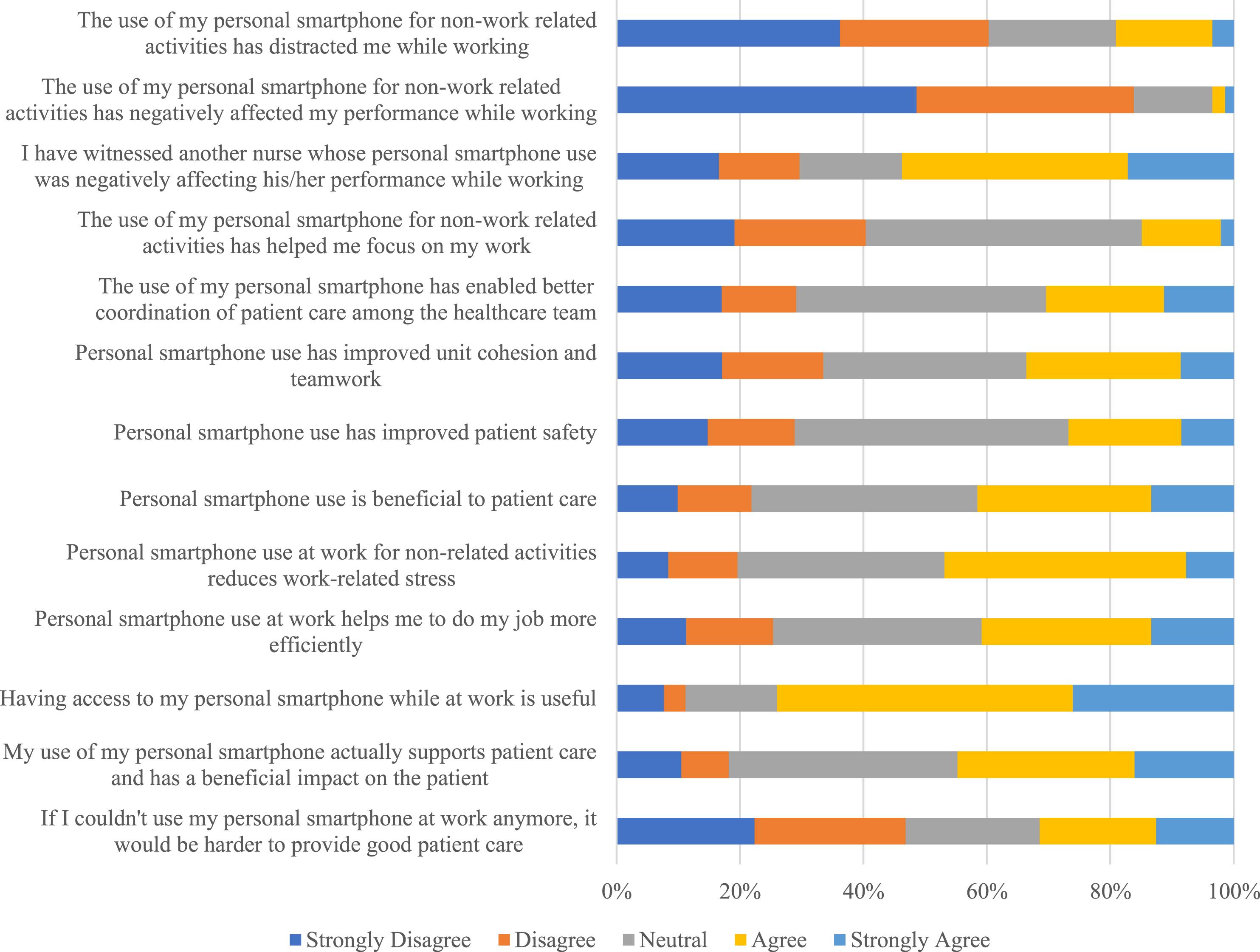
Perceived effects of personal device use at work for work-related activities and hospital settings compared with community settings.
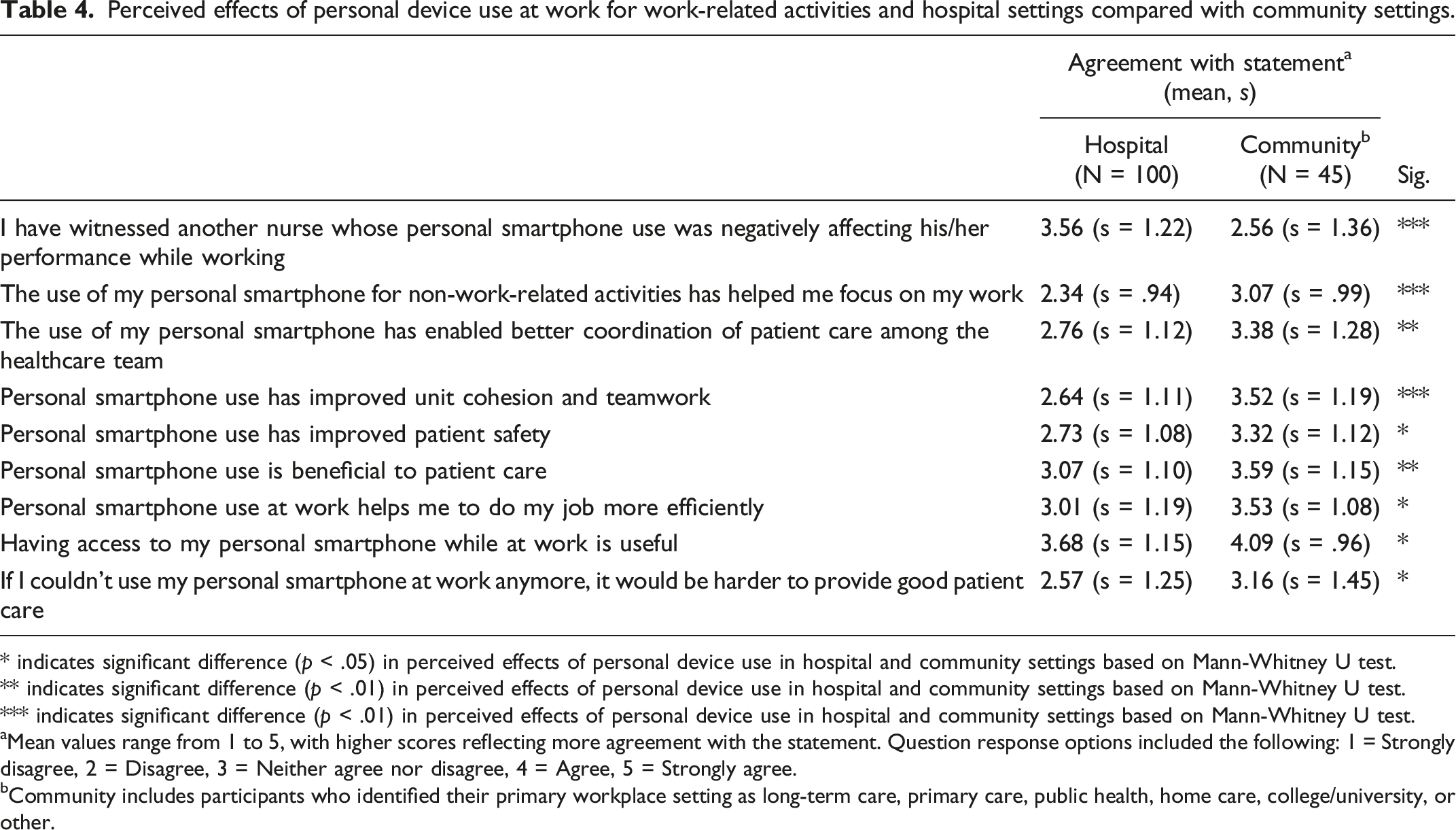
* indicates significant difference (p < .05) in perceived effects of personal device use in hospital and community settings based on Mann-Whitney U test.
** indicates significant difference (p < .01) in perceived effects of personal device use in hospital and community settings based on Mann-Whitney U test.
*** indicates significant difference (p < .01) in perceived effects of personal device use in hospital and community settings based on Mann-Whitney U test.
aMean values range from 1 to 5, with higher scores reflecting more agreement with the statement. Question response options included the following: 1 = Strongly disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Strongly agree.
bCommunity includes participants who identified their primary workplace setting as long-term care, primary care, public health, home care, college/university, or other.
Perceived effects of personal device use at work for work-related activities before the pandemic and current, all participants (N = 169).
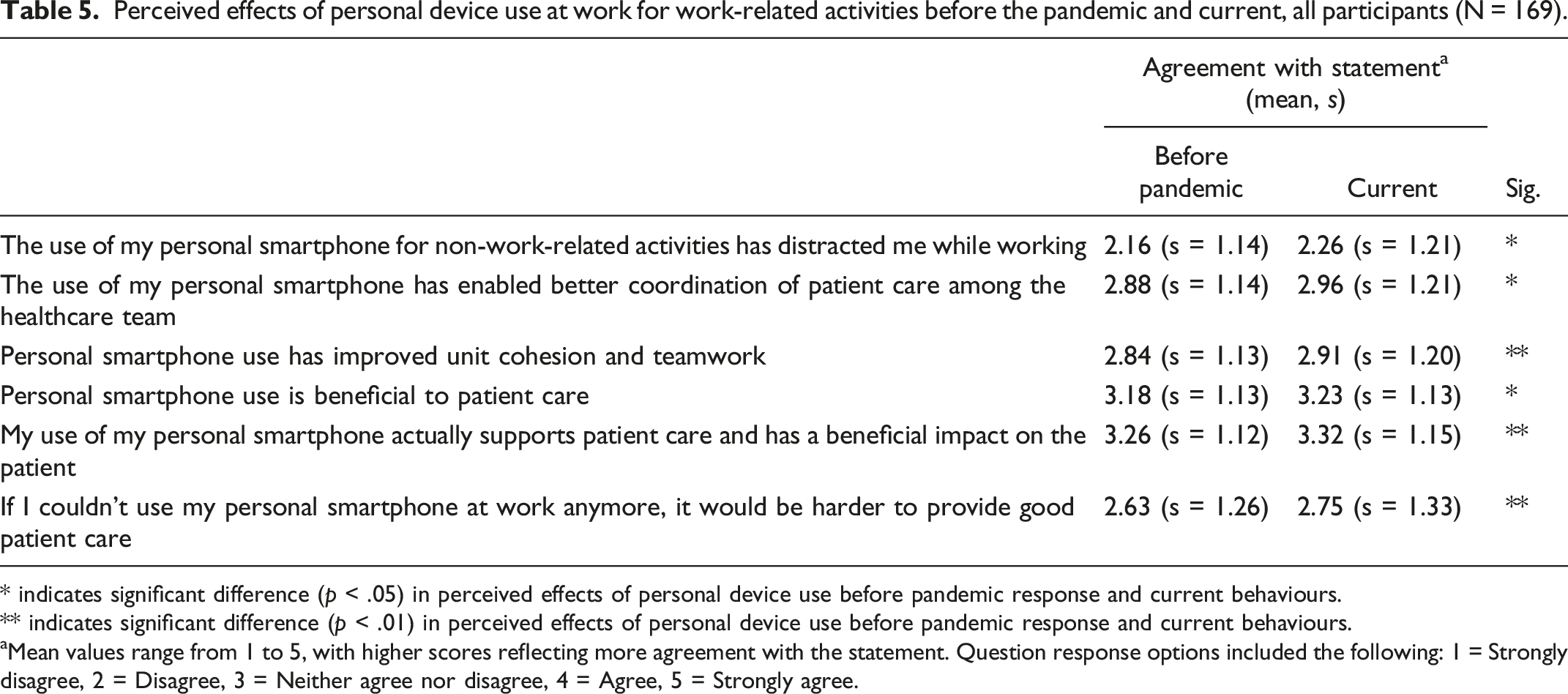
* indicates significant difference (p < .05) in perceived effects of personal device use before pandemic response and current behaviours.
** indicates significant difference (p < .01) in perceived effects of personal device use before pandemic response and current behaviours.
aMean values range from 1 to 5, with higher scores reflecting more agreement with the statement. Question response options included the following: 1 = Strongly disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Strongly agree.
Discussion
This study is the first in Canada to investigate Ontario-based RN and RPN use of personal digital devices to support their clinical role. Literature to date has predominately focused on nurses’ personal device use within acute care settings, 5 and we are reporting on RNs and RPNs working across diverse healthcare settings. Consistent with others’ research, a majority of RNs and RPNs in this study leveraged their own digital devices in support of their clinical role.3,4,14,15 Health leaders and administrators ought to assume that RNs and RPNs will use their personal digital devices within the workplace and for patient care. It is noteworthy that over half of the respondents reported organizational support for the use of personal technology in the workplace. This is a relatively new shift in organizational behaviour. Longstanding healthcare organizational policy often limited or prohibited nurses from bringing their personal devices into work. 15 Future research is needed to explore organizational governance and policy development for RN and RPN use of organizationally owned as well as personally owned digital devices. Nurses’ use of their personal technology may reflect a technological “workaround” and demonstrate nurses’ ingenuity and insight into the limitations of existing organizational information systems.16,17
Organizational policies that limit or prohibit nurses’ use of personal devices such as smartphone use may be short-sighted. Instead, a focused attention to the development of suitable guidelines for professional practice using personal devices is needed. 18 The findings from this study present an opportunity for organizational leadership to reframe nurses’ use of personal digital devices in a positive light and to view their technology “workaround” as a response to longstanding recommendations that nurses need to be part of the design and development of health information technology systems, components, and apps. 19 These findings also offer an opportunity to healthcare leadership and technology developers to reframe nurses’ innovation in developing workplace workarounds as untapped wisdom in the development of effective and responsive technology-enabled solutions.
RNs and RPNs in this study reported the use of their personal devices, mainly their smartphone, for very practical purposes: to tell time, to monitor time (stopwatch), and to enhance visibility (flashlight). This may, in part, have affected RNs’ and RPNs’ perception of their personal devices as contributing to workplace efficiency. These findings are consistent with Korean nurses’ reported use of their personal digital devices within acute care. 20 Researchers reported that personal smartphone use among acute care Korean nurses was common and frequently used for pragmatic reasons similarly reported in this study. Korean nurses also used their smartphones to capture photos of patient data and to seek on-line information. Convenience and efficiency in patient care practice was similarly cited as reasons for smartphone use among acute care Korean nurses. 20
The expectation of evidence-informed patient care practices highlights the importance of access to pertinent health-related resources among RNs and RPNs. Findings from this study are consistent with the use of smartphones among acute care nurses who also highlighted the use of their personal smartphones for professional development and education, to access drug references, as a drug calculator and to communicate with other members of the healthcare team.4,5,20 The prevalence of personal device use to support clinical practices (looking up tests, symptoms, procedures, and medication administration) highlights RNs’ and RPNs’ appreciation of portable, readily accessible, digital technologies in support of patient care that they are already comfortable and familiar with.
That most RNs and RPNs reported safe use of their personal digital devices was an interesting juxtaposition to their perception of their colleagues personal digital device use. Participants perceived that device use among other RNs and RPNs negatively affected their practice. This is consistent with others’ findings that nurses’ use of digital devices within the workplace was perceived as unprofessional and a distraction from patient and family care.5,21 Digital health educators encourage healthcare providers to explain to patients and families why and how they are using their devices in support of care provision, but to date, this has not applied to the healthcare team. This is an important area for further exploration, to fully understand what assumptions were made by RNs and RPNs about others’ device use and what criteria were used to determine RNs’ and RPNs’ use of personal devices as negatively affecting patient care.
Nurses play an integral role in risk mitigation within the medication management process; improper dosing and mode of administration are common contributors to adverse events. 22 The complex processes of prescribing, verifying, preparing/dispensing, administering, and monitoring medications tend to be error prone with the most frequently documented errors being medication administered at the wrong time or omission of administration of prescribed doses, or administration of the incorrect dose.23,24 RNs’ and RPNs’ use of their personal digital devices as a drug calculator and to look up drug calculations and interactions may represent their personal accountability to “best practice” for medication administration within the digital context. Nurses’ use of personal devices for medication administration may serve as an accessible and convenient strategy to ensure accurate medication administration. While computerized medication ordering/administration systems have been touted as a way to enhance accuracy of medication delivery, emerging evidence suggests that reliance on electronic health information systems and specifically medication order entry and decision-making tools as a way to mitigate adverse drug events is not fully warranted. 25
Key findings from this investigation of RNs’ and RPNs’ use of their personal digital devices—especially smartphone—within their workplace include enhanced communication and team cohesion, workplace efficiency, and positive impact on patient care and safety. The convenience of an integrated multi-functional “smart” device (Internet “at hand” with immediate access to information, real-time communication with colleagues, along with photography, flashlight, clock/timekeeping functions) may reflect both a familiarity and an efficiency of use; the “wearable” nature of digital devices (phones or watches) would be particularly appealing to already burdened nurses who are juggling multiple tasks and activities. While not substantial, 16% of RNs and RPNs in this study reported the use of smartwatches which serve as an extension of the smartphone, enhancing convenience of access to information and communication with others. 26 The nursing profession is a target of smartwatch marketing who advertise information accessibility, ease of communication, and voice-activated data collection as proposed benefits of smartwatch use within clinical settings (https://fitfornursing.com/best-smartwatches-for-nurses/).
The use of personal devices as a communication tool was highlighted among the RN/RPN participants. Our findings are consistent with others’ research reporting on acute care RNs’ and RPNs’ appreciation of their personal devices to share information, patient data, and, at times, photos or images among the healthcare team.3,14,15,27 This research also adds to our understanding of personal device use among community-based RNs and RPNs. Relative to those in acute care settings, RNs and RPNs working within community-based settings such as home care and public health reported greater relevance of their personal devices to communicate among the healthcare team.
Effective communication among the healthcare team is essential for quality patient care and effective teamwork. 28 In fact, common reasons for errors resulting in patient harm often result from communication failures. 29 RNs and RPNs in this study reported the use of popular on-line messaging apps to communicate with their colleagues. Enhanced and efficient communication among the healthcare team has the potential to contribute to improved patient care and safety yet at the same time may challenge patient information safety in terms of breaches to information privacy and confidentially.20,29 Opportunities for future research exist to investigate RN and RPN use of personal devices for communication among the broader healthcare team and to understand how patient information safety is being addressed.
RNs and RPNs in the current study reported using healthcare-related apps downloaded on their smartphones. While helpful for patient care, Korean nurses’ use of a mobile EMR app appeared to extend their time on shift, and researchers noted they would access patient care information before or after their shifts to prepare hand-offs and review nursing notes and laboratory results. 20 This finding presents additional opportunities to understand how the use of personal devices and healthcare-related apps affect the work-life balance of already burdened nurses.
Limitations
As with all research, we acknowledge the limitations of this investigation. Only English-speaking RNs and RPNs were invited to participate in the study. Individuals who are more comfortable communicating in languages other than English may not be represented in these findings. We recognize the limitation of convenience sampling and caution that the findings may not be reflective of all practicing RNs and RPNs. Similarly, an on-line survey was one of our primary data collection strategies which may have created a barrier to potential participants with limited digital literacy skills and/or lack of experience with digital technologies.
Conclusion
This research provides insight into the use of personal digital devices for RN and RPN practice across diverse clinical settings and offers emerging insight into how personally owned and operated devices are being integrated into healthcare practices. This research also highlighted important tensions with RN and RPN use of personal devices within the workplace, calling attention to workplace efficiency and enhanced team communication. This research supports the development of guidelines for personal device use within healthcare settings that are informed by a multi-disciplinary group of experts inclusive of RNs and RPNs.
Footnotes
Acknowledgements
We thank the RNs and RPNs who contributed to this research and we value their insight into digitally informed patient and family care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was required and obtained.