
Abstract
The Canadian healthcare landscape’s deep fragmentation of service-centric data silos is causing harm to patients, providers, and the overall healthcare system. This article examines Principle 1 of the Pan-Canadian Health Data Charter: Person-Centric Health Information Design (PCHID). Unlike traditional models, PCHID creates a technical architecture organizing data around individuals to ensure continuity of information across the care continuum. Canada can realize significant gains in health equity, clinical safety, and population health and innovation by moving from an “ego-centric” system of institutional data control to an “eco-centric” model of shared stewardship. This article outlines pathways for health leaders to operationalize PCHID. These include governance and public engagement, harmonized policies and legislation, investment in health data literacy, culture change, and embedding Indigenous data sovereignty. Ultimately, PCHID serves as the foundational blueprint for a trusted, integrated health ecosystem that prioritizes the well-being and agency of all people in Canada.
Introduction
Canadian health leaders and policy-makers are increasingly confronted with a critical governance challenge: ensuring health data infrastructure supports safe, equitable, and coordinated care amid persistent fragmentation.
Imagine a health ecosystem where data are not held within institutional silos but are a dynamic resource empowering people and providers. Person-Centric Health Information Design (PCHID) can help health leaders and policy-makers address systemic risks associated with fragmented data systems and dissolve historical harms of disconnected systems. This can advance a future based on trust, equity, and an integrated, ecosystem-focused health data environment.
The Canadian healthcare landscape is at a point where traditional healthcare and data silos are detrimental to modern society. Quality, accessible health data are essential, supporting clinical decisions, coordinating care teams, ensuring continuity of care across settings, informing population health planning, driving quality improvement, and supporting innovation and research. 1 However, organization, governance, design, and use of health data remain fragmented and mostly service-centric. 2
This article, written for health leaders and policy-makers, presents PCHID as a leadership and policy framework requiring deliberate governance, accountability, and coordinated implementation. It also grounds the analysis from a patient-centred view, reflecting real experiences within fragmented health systems. This dual framing keeps the discussion actionable, relevant, and grounded in real-world experience, enabling informed leadership decision-making.
The Pan-Canadian Health Data Charter, a framework proposed by the Expert Advisory Group (EAG) of the Pan-Canadian Health Data Strategy, aims to guide transformation towards a world-class health data system in Canada. The Charter’s first and most critical principle centres on PCHID, also known as person-centric health data architecture. 3 PCHID is the foundation for information continuity. 4 The Charter requires that PCHID ensure health data follow individuals across care points. It supports individual, clinical, and analytical access and use, while respecting privacy under current legislation. 4
Adopting PCHID requires shifting from a service-centric model, where data are bound to institutions, organizations, or clinicians, to one where data are dynamic, accessible, and a valued asset, empowering patients and strengthening the system. 5 For policy-makers and health leaders, this shift introduces critical governance and implementation considerations. These include redefining data stewardship, aligning incentives across jurisdictions, enabling interoperability, using shared standards, and ensuring that equity, including Indigenous data sovereignty, is embedded in policy and system design.
Applying a person-centric lens to the current state of health data can help identify harms arising from system fragmentation and define steps to establish a trusted, adaptive, and equitable health data ecosystem promoting patient well-being. 1 Addressing these harms requires coordinated leadership action, deliberate policy execution, and sustained governance reform. Positioning PCHID as a leadership and policy framework enables the development of an integrated system-level agenda supporting improved patient outcomes, workforce sustainability, and public trust.
Current State of Health Data in Canada
Canadian health data are fragmented across jurisdictions, sectors, and organizations. There is significant variability in digital maturity and interoperability between providers and systems. 6 This fragmentation stems from service-centric design that assumes care is static and local, leading to unsafe practices and harm to individuals, populations, and health systems. 7
While many Canadians assume their data follow them seamlessly, the reality is a gap between expectations and fragmented infrastructure, causing frustration and mistrust. 8 Patients navigate multiple care settings, each holding unique, fragmented information. They must often manage and share their data but have little control over access or use.
First Nations, Inuit, and Métis peoples face health systems that worsen existing inequities. This limits their ability to exercise their right to self-determination, especially regarding health data. 1
There is unintentional fragmentation of health data by privacy legislation, cementing interoperability gaps and short-term priorities contributing to the complexity and intractability of the Canadian health data system.3,5
Care providers report increasing burnout and moral injury due to fragmented health data and poor interoperability, reducing their ability to deliver safe, timely, and efficient care.1,9,10 Current data arrangements are inadequate for supporting transparent, person-centred secondary uses. These include quality improvement, research, innovation, and population health surveillance, and data resources remain difficult to access or reuse in practice.11-13
Despite federal investment in health data, barriers remain. Limited interoperability of electronic medical records and political or legal obstacles discourage data sharing, worsening the challenge.6,14 Estimates say Canada could benefit over $9.4 billion annually by maximizing health data use. 15 Benefits include financial gains, better research, innovation, improved health outcomes, and quality of life.11,15
Health Data-Related Harm (Figure 1), defined as the “harm suffered by individuals, populations, and/or the health system arising from poor data access, quality, or use,” is affecting individuals, populations, and the health system as a whole.7,16 This understanding of health data-related harm expands the focus beyond traditional privacy-focused harms and highlights the importance of PCHID.
17
Health Data-Related Harm Framework. Adapted with permission from Deonarine A et al. Validation of a Novel Framework for Assessing Health Data-Related Harm Arising from Artificial Intelligence and Information Systems Use in Healthcare: A Pilot Survey and Mixed Methods Study. Unpublished manuscript, 2026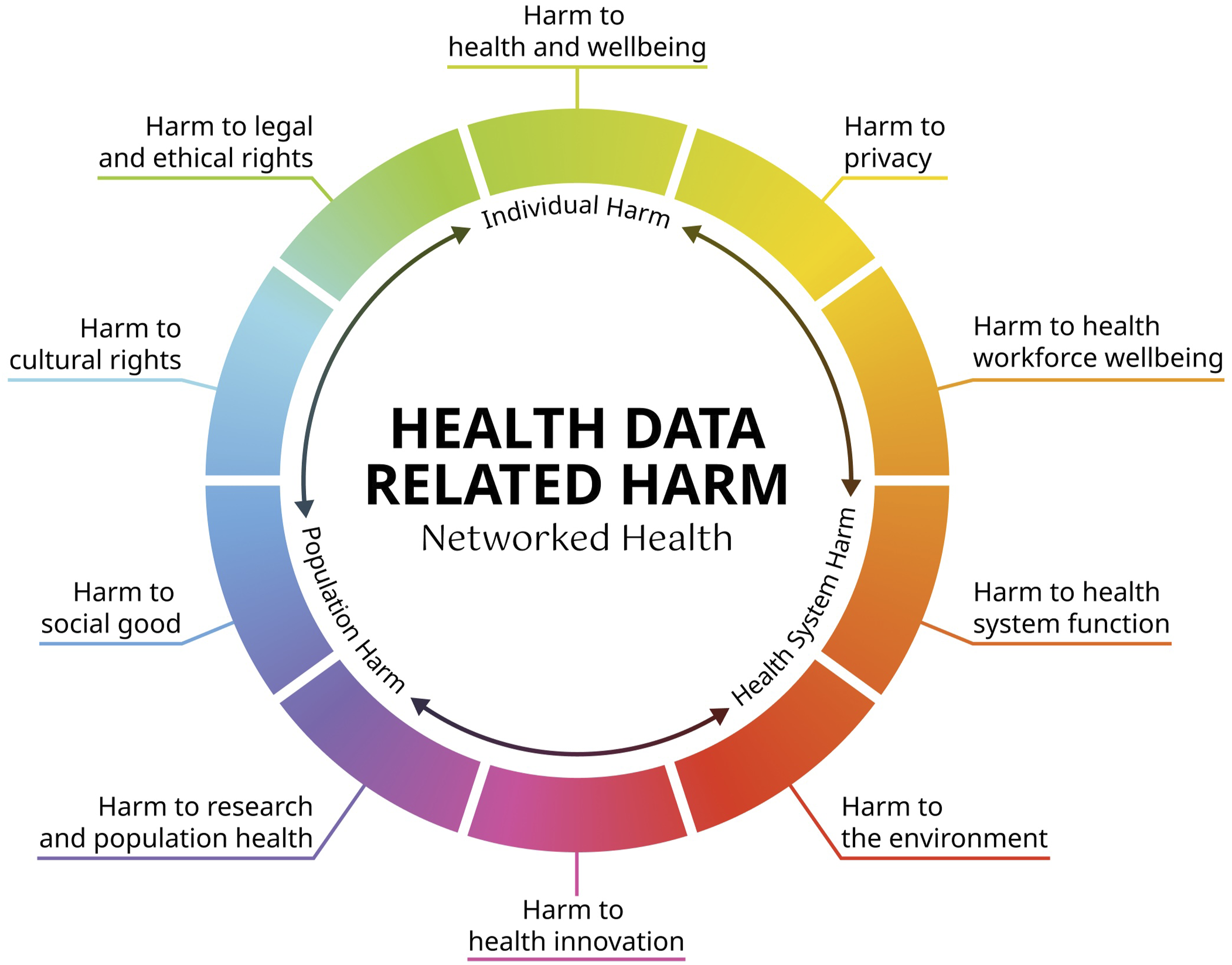
Importance of a PCHID Approach
It is important to distinguish person-centred care from PCHID. The terms are similar but function at different levels. For leaders and policy-makers, making this distinction is key for governance, investment, and implementation decisions.
Person-centred care is the philosophy that guides care delivery. PCHID is an architectural concept for designing health data around the individual as the owner and basic unit of care, ensuring data follow a person over time and place during care. 3 PCHID is a technical architecture allowing person-centred care at scale, but success depends on leader choices about standards, stewardship, and interoperability.
A person-centric health data system means health information belongs to the individual and is organized around them. This approach puts personal needs above institutional boundaries or legacy IT systems.
18
It marks a shift in mindset from service-centric to person-centric systems. Operationalizing it requires clear policy direction and sustained leadership (Figures 2 and 3). In a service-centric model, health information is organized around institutions, programs, and providers, not individuals. Fragmented access can compromise coordination, safety, and system performance Person-centric health information design organizes data around the individual. This supports continuity, safer care, and effective coordination across the health system. It benefits the individual, their care teams, and the entire system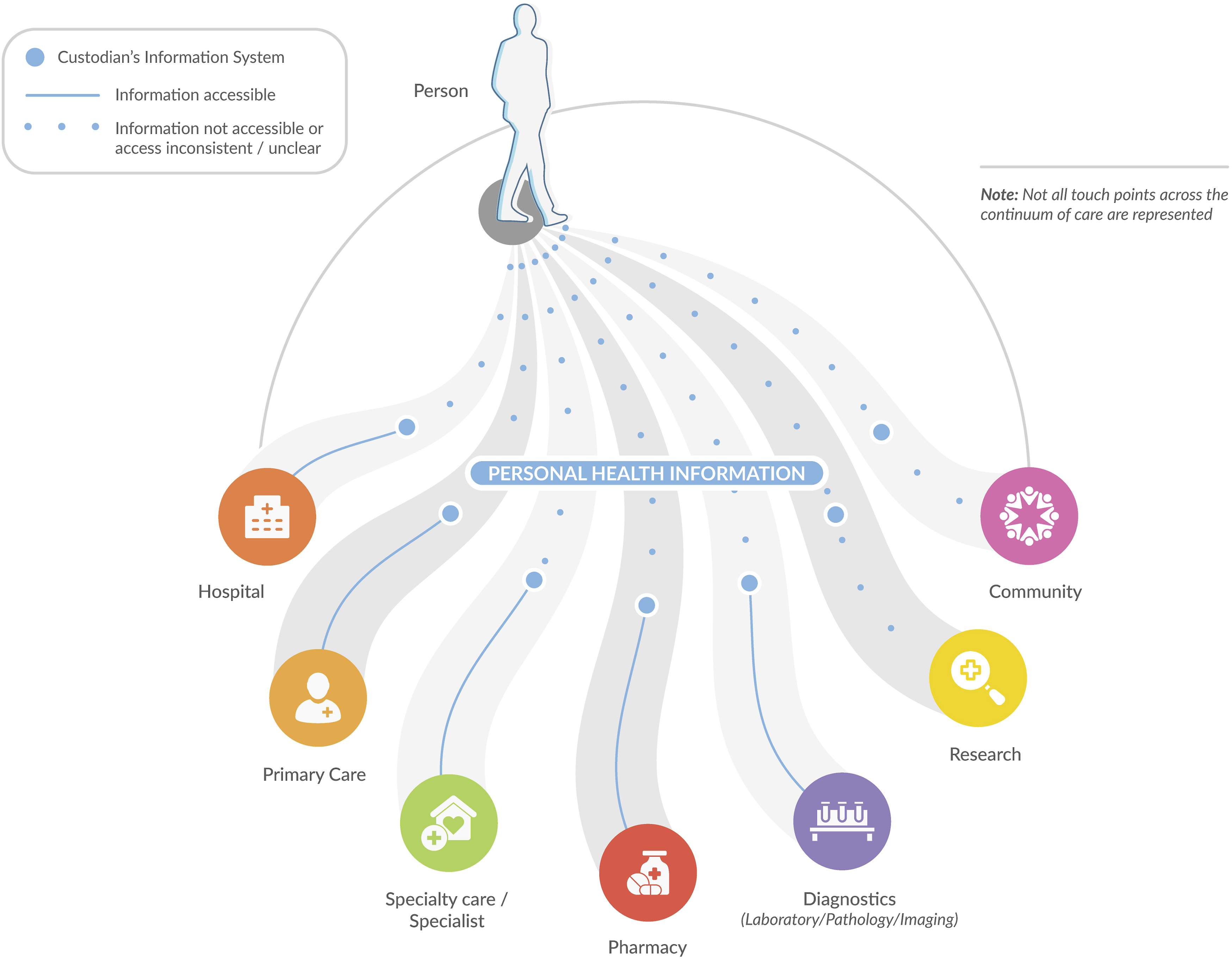
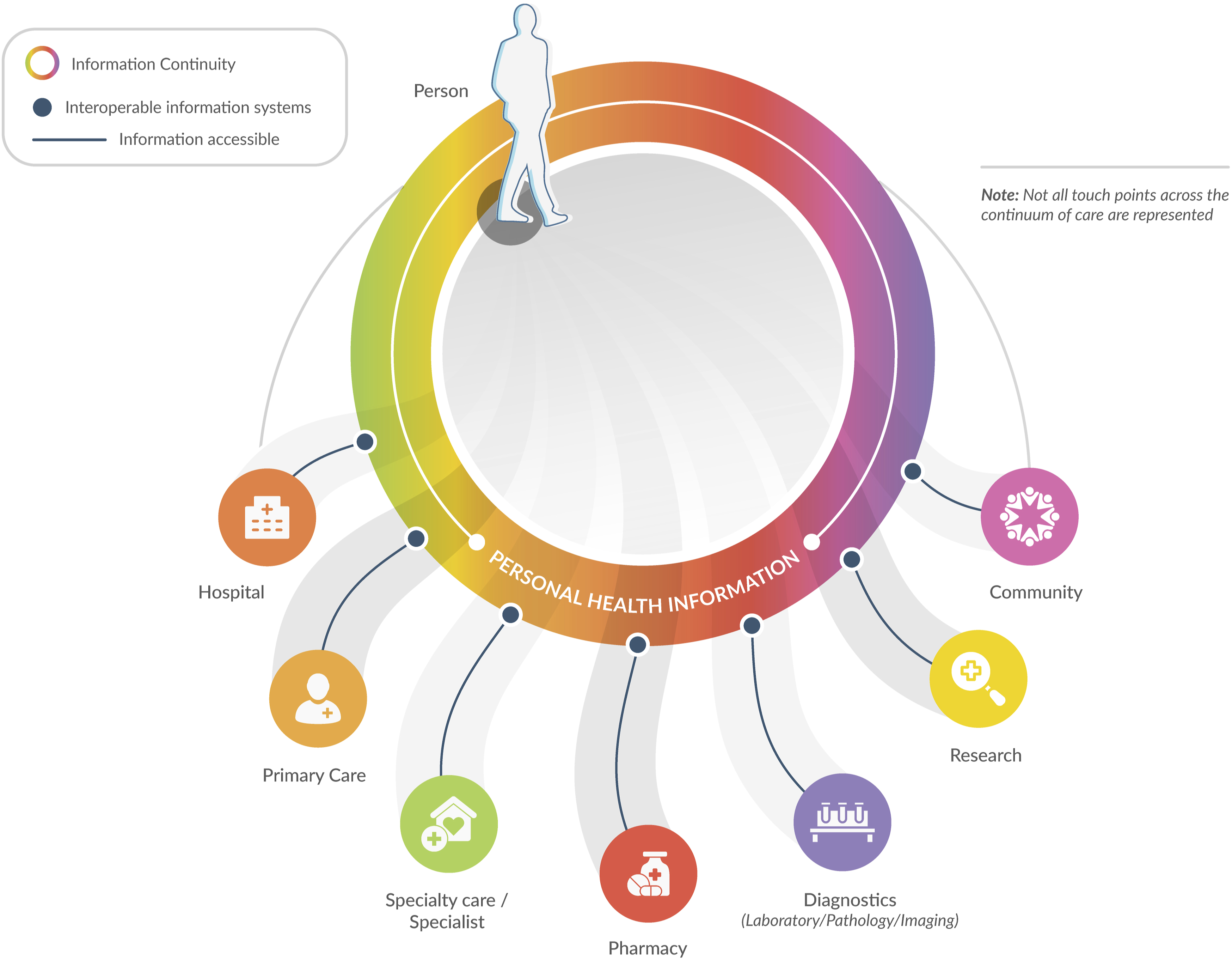
Practically, PCHID allows an individual’s health information from primary care, hospitals, laboratories, pharmacies, mental health, community health, public health, and social services, and other settings, to follow them across the system.
To enable information continuity, leaders and policy-makers must make the deliberate choice to cooperate around harmonized interoperability, shared standards, and governance across jurisdictions. 19 This is especially important in rural, remote, and marginalized communities, where it can improve health equity and outcomes. 20
Information continuity, enabled by PCHID, helps leaders support three critical domains of use, each with distinct benefits: 1. 2. 3.
A PCHID approach can support a learning health system, improving patient experience, enhancing population health, reducing costs, promoting clinician well-being, advancing health equity, and aligning with the Quintuple Aim.14,22 A PCHID approach does not mean compromising on privacy for access. Instead, it incorporates privacy protections into both technology and legislation from the outset, ensuring secure use of personal health data across the healthcare system.
The Future State of Health Data in Canada
The outlook for healthcare in Canada provides a significant leadership and governance challenge: transitioning from a fragmented, service-centric model to a unified, person-centric data ecosystem, redefining data control, ownership, and agency from institutions to better empower individuals. Several pan-Canadian initiatives have signalled a transition towards a more person-centric data environment through health data stewardship initiatives.24-26
Building a person-centric health data system requires moving away from an “ego-centric system,” where individual and institutional custodians treat data as their exclusive asset, towards an “eco-centric system” where information is seen as a shared resource to be stewarded for the benefit of patients, providers, researchers, innovators, and populations. 27
At the core of the Pan-Canadian Health Data Charter is a commitment to person-centric design. The Charter provides leaders with a blueprint for moving from a fragmented system to a truly integrated one. 3 A system built to ensure health data follow the individual across points of care, supporting individual, clinical, and analytical access and use while respecting privacy, will help avoid harm to individuals, populations, and the healthcare system.
Public Trust
Public trust must be a foundation of any future health system. Trust is earned through trustworthy practices such as transparency, meaningful public engagement, public benefit, and improved health data literacy, so people can participate in discussions and decisions about how health data and related systems are used.21,24,28
An example is the OpenNotes® initiative, which promotes a future in which patients routinely access their health data to prepare for visits and coordinate care with support networks, fostering a sense of control. 29 When patients have greater access to and ability to share their health data, their trust in healthcare professionals and relationships is higher. 30
Recent progress allows patients to change notes, correct inaccuracies, and contribute personal insights. 31 Evidence indicates that access to health data substantially increases disease knowledge, engagement, and medication adherence, particularly among those managing chronic conditions.32,33
Pathways to Achieve a Person-Centric Health Data System
Although the Pan-Canadian Health Data Charter was endorsed by all provinces and territories in October 2023 (except Quebec), 3 this has not translated into significant adoption of a person-centric model of health data system design by any jurisdiction in Canada. The following steps describe key leadership and policy pathways to achieve coherent PCHID across Canada.
Governance, Public Engagement, and Trust
Trust comes from trustworthy practices, not from public persuasion alone. For health leaders, establishing trustworthy data practices includes ongoing inclusive public engagement; reconciliation and recognition of Indigenous data sovereignty; well-defined policies and support for data sharing, access, and use; alignment of data use with public benefit; and the creation and use of technology standards to ensure data safety and seamless sharing.21,28
For health leaders, this requires moving beyond episodic consultation towards formalized co-design with patients, Indigenous communities, racialized and marginalized groups, researchers, educators, innovators, and the workforce. By embedding these groups into governance, leaders can move beyond simple feedback to create accountable frameworks that define public benefit and safeguard person-centric policy. 2
Harmonizing Policies and Legislation
Advancing a unified health data system requires a serious rethink of our existing legal structures. For policy-makers, this requires tackling legislative and provincial silos arising from current custodial models of data oversight, and moving towards a person-centric health data stewardship model. 5 This includes sustained federal and provincial collaboration to align legislation and interoperability requirements.
Prioritizing information continuity, specifically enabling data to follow the individual across the continuum, must be a leadership priority. Health leaders should support and champion policies and legislation that enable health data to follow individuals across the continuum of care. Bill S-5, the Connected Care for Canadians Act, is a first step in this process. 34 Existing custodian or service-centric health data design models, a byproduct of custodial legislation, should be sunsetted to support moving to a person-centric framework.
Investing in Data Literacy
Building a person-centric data system requires a greater understanding of the importance and function of health data by decision makers, healthcare providers, and the public. This requires a common lexicon for health data across Canada. Coordination and responsibility around health data literacy across Canada are essential to support a person-centric health data system.
Leaders should align education, regulatory, and practice environments to embed informatics and digital competencies into undergraduate and continuing health education for health professionals. Treating data stewardship as a professional standard, equivalent to clinical care, ensures professionals understand the value of high-quality data. Data literacy for regulated health information professions should become a standard, professionalizing data stewardship. 5 Simultaneously, public education should focus on health data literacy, clarifying how data are protected and the tangible benefits of sharing.2,8
Culture Change
Achieving PCHID requires a culture shift among health leaders, clinicians, data custodians, and vendors. Organizations must recognize person-centric data stewardship as core to quality care, not simply as an external compliance requirement. 35 Training programs for clinicians and administrators should include data literacy, ethics, and person-centric data frameworks. This ensures staff understand the value of health data and the risks of non-sharing. It also prepares the workforce to steward, interpret, and apply health data responsibly to support high-quality clinical decision-making, learning health systems, and use data in ways that respect privacy, equity, and public trust.24,35 Leaders must model and reinforce these expectations through policy, performance measurement, and organizational culture.
Embedding Indigenous Data Sovereignty
A PCHID approach must incorporate Indigenous data sovereignty principles. For policy-makers and health leaders, this requires a commitment to nation-to-nation engagement and to recognizing Indigenous data governance authority. Creating an environment that does not perpetuate and exacerbate existing structural social inequities, impeding the ability to exercise Indigenous Peoples’ right to self-determination, particularly with respect to health data, is critical. 36
A distinction-based approach, including OCAP (Ownership, Control, Access, and Possession) for First Nations, and similar frameworks for Métis and Inuit communities, is required. 2 This means First Nations, Inuit, and Métis communities determine how and what Indigenous data are collected and maintain governance over its use. 24 Indigenous-led governance frameworks should be part of the broader pan-Canadian data strategy to ensure that the benefits of digital health are realized equitably across all communities. 3
Conclusion
By prioritizing PCHID as a means to achieve information continuity, the unification of Canada’s disconnected health systems can begin. 2 For health leaders and policy-makers, this represents a strategic imperative with direct implications for system performance, equity, and public trust. Bringing the Charter’s first principle to life requires more than technical attention. It is a shift in perspective and centres the system on the individual. This is not only a change in the organizing principles of health data but a profound cultural shift requiring a coordinated push across several fronts: building public trust, aligning health data, legal, and policy frameworks, and investing in the infrastructure and standards needed for data to flow.
Importantly, this work must be rooted in a culture of transparency and co-design, supporting health data literacy and commitment to Indigenous data sovereignty and equity. Without leadership, policy alignment, and accountability, fragmentation, avoidable harm, and inefficiencies will persist across the health system.
With PCHID, Canada can move towards a future where individuals receive safer, effective care, population health is strengthened, and health data can support innovation for the benefit of all people in Canada.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the many dedicated people, organizations, and institutions who are initiating and advancing person-centred health information design across Canada.
Ethical Approval
Institutional Review Board approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.