
Abstract
In Long-Term Care (LTC), many residents live with dementia, a chronic and progressive disease that is often complicated by behavioural and psychological symptoms. A changing context, including the COVID-19 pandemic, health human resource challenges, and increasing medical complexities, has led to greater reliance on medical management of dementia, with risks to residents’ health and quality of life. In response, we have developed a regional LTC program that integrates quality, clinical practice and education, research, and nursing specialist expertise to enhance the ability of care teams to provide evidence-based, person-centred dementia care. This strategy includes dedicated quality improvement supports; innovative non-pharmacological approaches, such as optimizing care-in-place with virtual care; and collaborative research opportunities. We describe these strategies and promising results to date, which include shifting the culture of care to support the holistic physical, social, emotional, and spiritual needs of residents living with dementia.
Introduction
Chronic disease is often associated with well-known health conditions such as diabetes, heart disease, asthma, and some cancers. However, dementia, an umbrella term for various forms of chronic, progressive cognitive decline, is a leading cause of death due to chronic disease for Canadian seniors 1 and often misunderstood due to the complexity of behavioural and psychological symptoms (BPSD) associated with it. In Canada, the current prevalence of people living with dementia is close to 800,000 with a projected increase to 1 million by 2030, many of whom will require Long-Term Care (LTC). 2 Coupled with increasing demand for limited spaces, the LTC sector faces the additional pressures of staffing challenges 3 and growing increases in the medical complexity of residents, including those with more than seven chronic conditions. 4
Within this context, LTC teams strive to provide person-centred quality of care and enhance quality of life for residents. Evidence shows that the ability of care teams to implement person-centred practices and adhere to best practice guidelines is related to and influenced by an interplay of contextual factors. In part, these include the presence or absence of supportive leadership, local champions, formal learning opportunities, interprofessional teamwork, and protected time, at multiple levels of influence from the organization to the unit.5,6
This article reviews our strategy to put this evidence into practice, through a team-based, resident-centred approach that connects continuous quality improvement (QI) with standardized application of clinical practice and education. LTC has been described as a place of “hidden complexity” 7 as each home is its own care setting with its own challenges to evidence-based implementation. We have developed a regional resource team that connects quality resource leaders, clinical nurse educators, research, data analytics, and nursing specialist expertise, with regular and ongoing collaboration with LTC leaders and direct care staff. We support a hybrid system of 60 LTC homes that totals over 5,700 publicly funded beds across a wide geographic area that comprises differences in owner/operator model, size, staff mix, and more. Our diverse team brings a variety of skill sets and cooperation with LTC leaders to build infrastructure and programming for all homes to have consistent access to specialized support, coaching, and education on dementia care. These have helped to reduce potentially inappropriate use of antipsychotics, strengthened palliative approaches to care, and increased access to speciality services allowing care-in-place.
Our approach is grounded in the principles of a learning health system: strengthening facilitators and reducing barriers to LTC teams applying evidence-based best practice; learning from experience; and generating novel evidence. The synergy of these elements provides a promising avenue to improve and sustain positive quality care and quality of life for people who live with dementia in LTC. In this article, we describe these elements in more detail, provide examples of their application in a range of initiatives, and highlight positive impacts for both residents and staff.
Discussion
A Model of Care to Build Capacity on the Potentially Inappropriate Use of Antipsychotics
The medical management of dementia with antipsychotic medications for BPSD has been used for many decades and increased during and after the COVID-19 pandemic.
8
This off-label use is ineffective in most cases and can lead to negative outcomes, such as falls and stroke, or more rapid decline for people who live with dementia.
9
To address this priority quality and safety issue, we implemented several initiatives that introduced standardized training, work processes, and new tools to implement non-pharmacological interventions and influence practice change. The wrap-around resources of a regional quality, education, and research team have allowed the roll-out of multiple supports at individual and system levels and decreased the potentially inappropriate use of antipsychotics in our program by 4.3% over 2.5 years (Figure 1). Quarterly rates of potentially inappropriate use of antipsychotics (adjusted) across all homes, over a 2.5-year period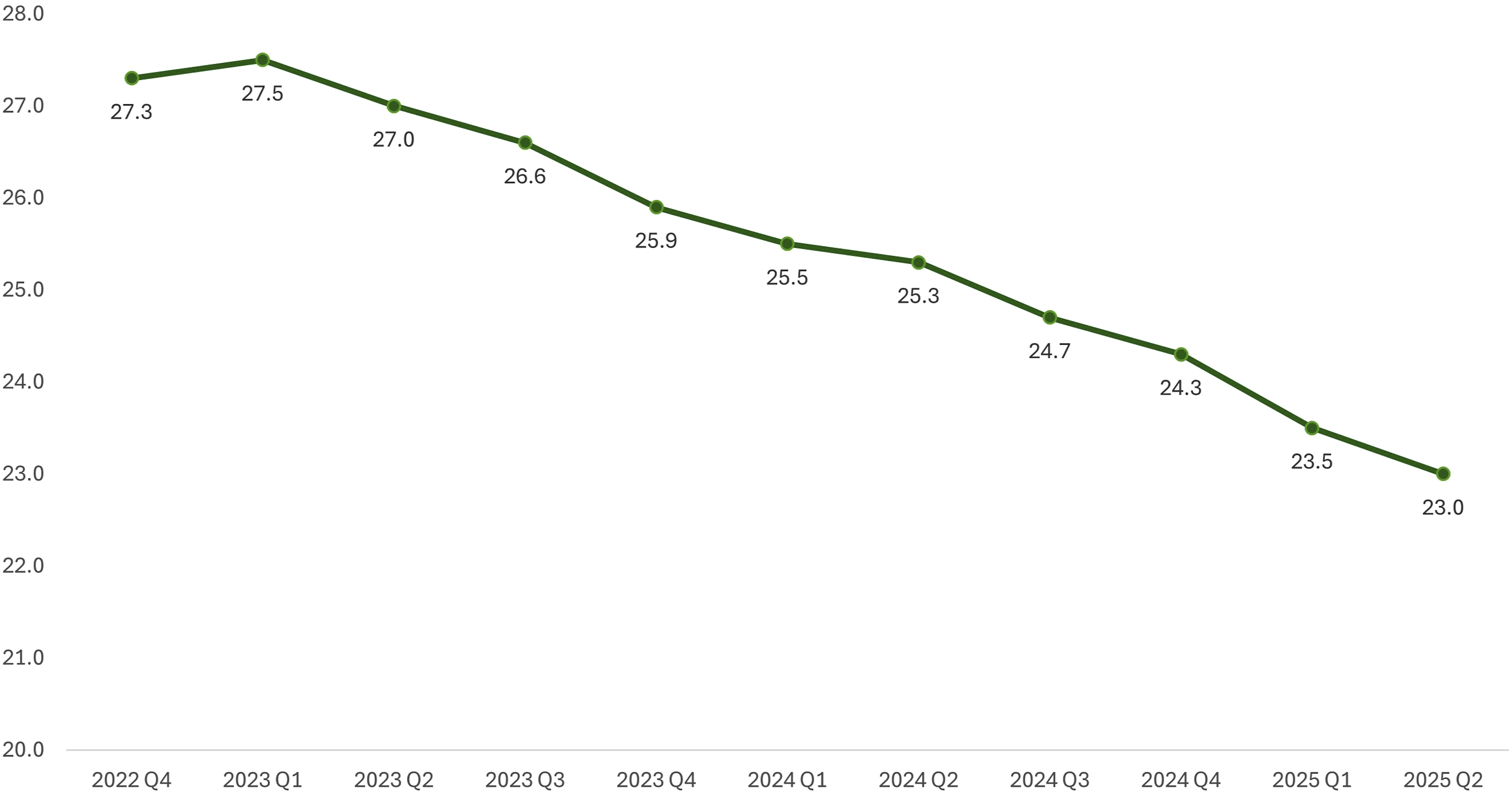
Core among these supports is an innovative model of care called the HCA PIECES Care Coach Program, 10 a peer mentor program for healthcare aides (HCAs) to learn practical application of the PIECESTM approach through U-First training. 11 The Care Coach Program targeted known barriers that make it difficult for HCAs to use best practice in their daily work, such as a lack of formal learning opportunities, perceived low social capital, and interdisciplinary collaboration. 6 The regional clinical nurse educators delivered the curriculum, while quality resource leaders provided at-the-elbow support as care teams put learning into practice. The administrative burden of securing funding, metric tracking, and program evaluation was relieved by the regional team. Care Coaches received 15 hours of training in BPSD, person-centred care, essential communication skills, and peer coaching. This included encouraging conversations about residents’ life stories to ensure care approaches match preferences and needs. As unit champions, they collaborated with PIECES practitioners (nurses who complete education in the PIECES program) to identify underlying causes of changes in resident behaviour, gather information from families, huddle with the interprofessional care team, and lead non-pharmacological care strategies. After one year, we found positive results for clinical outcomes, quality of life, and care team satisfaction. 10 To complement reduced reliance on antipsychotics, we have also explored innovations in non-pharmacological approaches, including trials of virtual reality technology and an evening activities program to enhance therapeutic recreation. An internal evaluation shows that the evening activities program reduced residents’ typical as-needed antipsychotic use by 50.9% on average.
New Services to Optimize Care-in-Place
Shifting away from a medical management model toward non-pharmacological alternatives is underpinned by a person-centred philosophy. This means partnership and shared decision-making between staff, providers, residents, and their families to ensure we uphold each person’s goals of care, preferences, independence, and quality of life. As we care for people in their final stages of life, we especially prioritize meeting needs on-site to avoid unnecessary transfers to acute care, which can be stressful and confusing experiences. Incorporating a palliative approach to care is an important enabler of person-centred care-in-place. More than a specific “type” of care provided to those who are actively dying, palliative approaches encompass holistic care planning and provision that include social, emotional, and spiritual needs throughout the changing course of dementia. 12 Common challenges to implementing it in LTC include increased resident acuity and complex behaviours, limited staff training, and inconsistent policy guidance. 12
To support better adoption in our program, clinical nurse specialists have standardized guidelines and education for a palliative, non-operative approach to hip fractures. Hip fractures can often signal decline and be a potential terminal event for a resident in LTC, and standard practice is to transfer to acute care for surgery. While surgery can happen in the context of palliative care, this is contrary to some residents’ expressed goals and wishes. Care of a resident with a palliative non-operative hip fracture means that a resident who lives with dementia can remain in place, to be cared for by a team who knows them well and avoid a potentially harmful transfer in their last days or weeks of life. This decision should take place in the context of a good understanding of what the resident’s goals of care are and in the context of previous conversations regarding the event of a hip fracture. It must also take place with good guidance on appropriate residents for this care, depending on their health history, dementia progression, quality of life, and possibility of poor outcome with surgical intervention.
As residents’ acuity and complexity has increased in recent years, 4 individual care homes are increasingly challenged by the resources and expertise that these situations require. Our regional strategy for our large, geographically distributed program includes offering an interprofessional Person-Centred Support Team staffed by a clinical nurse educator, clinical nurse specialists, and quality resource leaders. This team helps to address long-standing gaps in support for behaviours associated with acquired brain injury, mental health conditions such as personality disorders, substance use disorders, and/or major neurocognitive disease, and/or cognitive impairment. Their services include delivering education and learning materials to enable and empower care staff to respond to these complex care needs in a person-centred, culturally competent, and trauma-informed manner. Importantly, this service is provided to all publicly funded homes, ensuring equity between health authority-owned-and operated and contracted operators. A referral form is completed requesting a virtual consult for complex behaviour care planning and includes a process to access physician specialists. The support team also meets directly with residents and families to identify goals of care, develop coping skills, and enhance understanding of how dementia and other major neurocognitive disorders can affect behaviour. In addition, virtual learning sessions with a geriatric psychiatrist are held monthly on BPSD; these are well attended by HCAs and nurses from across the region.
Recent innovations in virtual care offer other new opportunities to expand specialty services access and turn-around time in LTC, upholding the principles of health equity, accessibility, and appropriate care across the complexities of dementia. 13 Only two Nurses Specialized in Wound, Ostomy and Continence (NSWOCs) serve our large program, yet their work is essential to maintaining skin integrity; virtual care has greatly improved access to NSWOCs, especially for rural homes. Meeting residents’ spiritual care needs and end of life support for families was the latest addition to virtual care services in LTC with access to spiritual health practitioners. Other technological improvements are being trialed to support physician clinician decision-making and further enhance care delivery on-site, such as mobile, wireless point-of-care ultrasound, which has been shown to enhance triage and transfer decisions in other care settings. 14
Standardizing Our Approach to Continuous Quality Improvement
Sustaining practice improvements in dementia care, such as reducing the potentially inappropriate use of antipsychotics, requires the combination of education with public reporting and policy change as part of well-designed strategies supported and reinforced by the organization.5,15 The backbone of our approach to supporting evidence-based dementia care in LTC is a quality framework, which sets an organizational benchmark for quality care. Based on the dimensions of quality established by the province, 13 it formalizes a vision of quality that centres resident- and family-centred care and prioritizes quality of life. Accountability and responsibility parameters are inherent in the continuous QI process with annual site visits and quarterly check-ins. The framework includes the regional team infrastructure and a scorecard based on four global indicators: resident and family; clinical performance; care team; and care home. Aspects of the scorecard include integration of Canadian Institute for Health Information quality indicators 16 generated from the resident assessment instrument tool. Scorecard results inform QI planning for each LTC home with an expectation to demonstrate evidence of improvement.
The framework and scorecard also capture the responsibility of LTC teams for meaningful, bi-directional engagement with residents’ families. Actively addressing gaps and opportunities identified by families can help both to directly shape person-centred care planning and inspire QI change ideas. Our regional team facilitates a jurisdictional forum across resident and family councils and recently partnered together to co-create new resources and amplify their voices in system improvements.
We also lead QI initiatives coordinated centrally across the region. In partnership with LTC NSWOCs, occupational therapists and LPN skin wellness associate nurses, we recently co-developed an evidence-based Skin Wellness Initiative to intervene on pressure injuries for high-risk residents. Pressure injuries affect many LTC residents, especially those who live with dementia, and can be difficult to heal. This initiative enhanced interdisciplinary care through a combination of nurse-HCA peer mentorship and 12 weeks of targeted in-service education, focused skin assessments, early identification, and escalation pathways. In the first cohort, we reduced the number of residents with pressure injuries by 35.3% and increased healthy skin on the heels and coccyx/sacrum by 37.9% and 35.2%, respectively (Figure 2). Of the difference that this program has made, one HCA said, “This project has given new staff and HCA students on practicum needed education, and for staff that are burnt out or have picked up bad habits, it has reset them.” This example of empowering care teams to lead in their practice demonstrates the collaboration of our integrated approach in healthcare leadership. Changes in percent of residents with heel and coccyx/sacrum pressure injuries before and after the Skin Wellness Initiative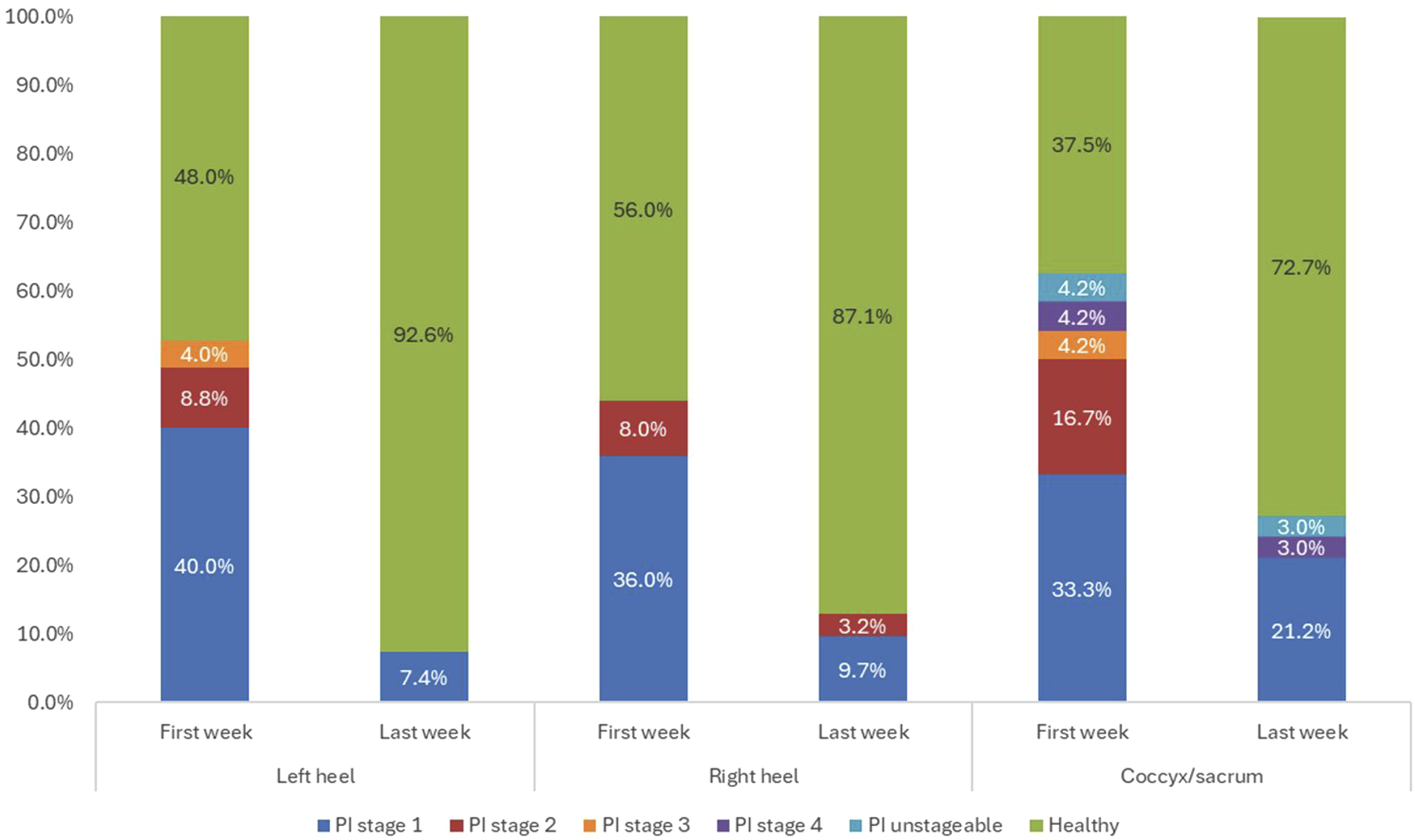
Where continuous QI harnesses smaller-scale, short-term tests of change, research is another opportunity to generate and evaluate information that may be used in future operational decisions and practice guidelines. Partnering with local and national academic researchers has allowed our program to contribute to emerging knowledge on topics that matter to people living with dementia, from the determinants of quality of life in LTC to reducing stigma and fostering dementia-friendly communities. In addition, evidence shows that the process of participating in research is in itself beneficial to people living with dementia, both as a source of learning and growth, and as an avenue to elicit meaningful social engagement, creativity, expertise, and competence from those who are often passive recipients of care. 17 A growing literature advocates for participatory approaches that directly engage LTC residents and caregivers on research teams. This means going beyond consulting or informing, to empowering the people who have the experience of living with dementia and living in LTC to shape the questions that research addresses and the goals it may achieve. 18 We explored this with a health equity study that included four current residents on the research team, grounding the work in resident-identified priorities and needs.
Conclusion
Dementia care is a unique chronic disease to manage because of its physical and psychosocial complexities. How care is delivered in LTC is greatly dependent on context and culture, including interprofessional communication, leadership support, and formal learning opportunities.
6
In hybrid systems spanning vast geographies, there can be great variability in context, and individual homes may not be able to provide all the resources that are required for the increasingly complex nature of dementia care. While structural variables cannot be modified, we established regional infrastructure to bridge these gaps, reduce barriers, and strengthen enablers of evidence-based practice. Feedback from care teams speaks to the impact that this type of support can bring (Figure 3). Selection of feedback from LTC staff about regionally supported initiatives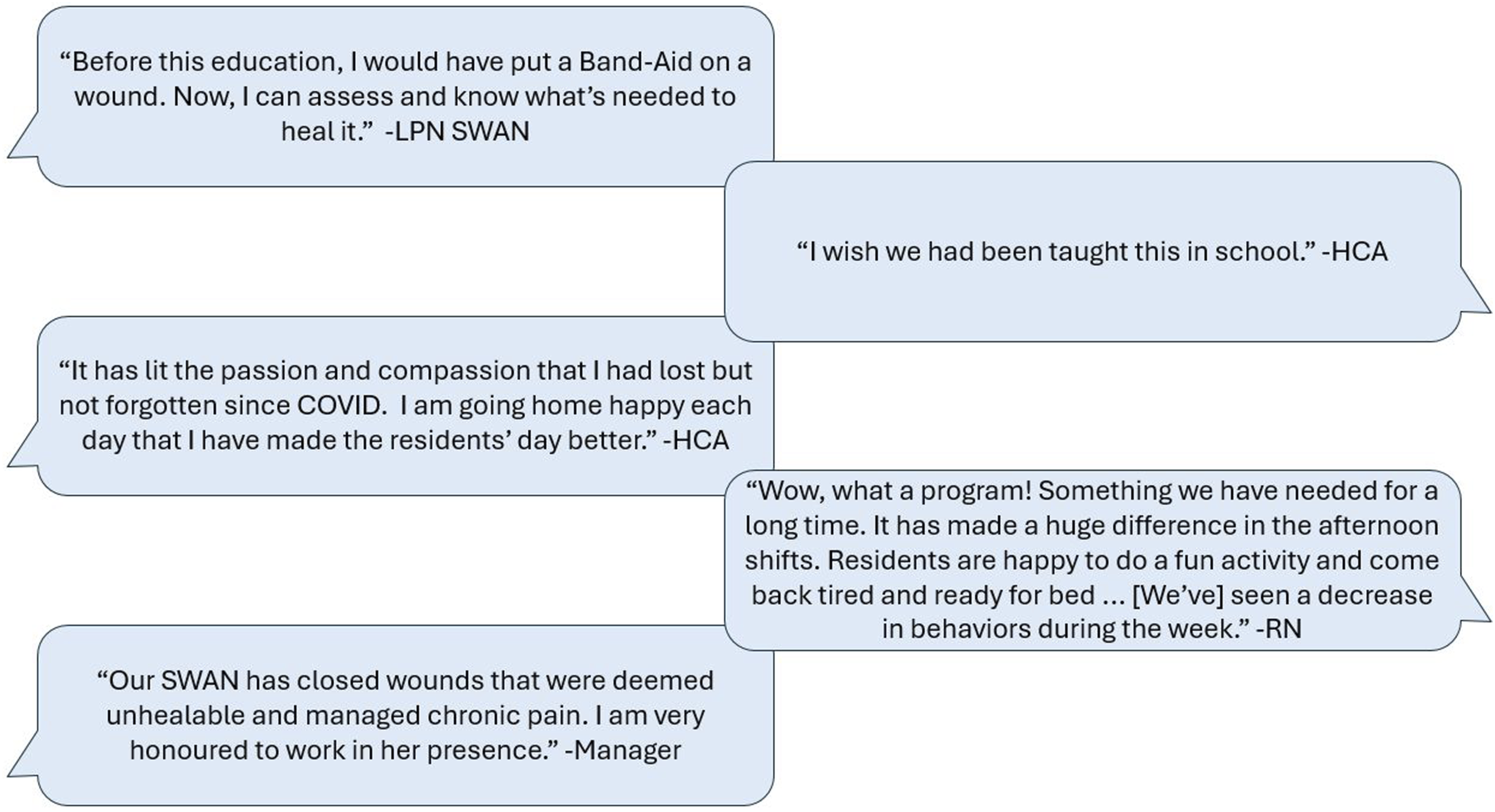
We encourage other LTC leaders to explore opportunities to incorporate some of the strategies that we have been able to provide across a diverse program. Senior leader support is key to resourcing, sustaining, and spreading such a model, 5 and we have experienced enthusiastic buy-in. Our integrated approach with the symbiosis between continuous QI, supporting clinical education and applying evidence-based practice through research has been recognized by senior leaders at our health authority clinical governance tables and provincial government levels. 19 Similar models to integrate quality, education and research are in existence today in other health authorities to support healthcare leaders in promoting person-centred care in their work.
The ethical dilemma of balancing self-determination and safety of a person who lives with dementia was an essential consideration when building and framing policy, programming, and education. 20 Through mutual understanding of the dementia journey and the associated progression of behaviours and symptoms, was the impetus to constructively integrate and lead QI processes, clinical practice, and education and research. Autonomy of the person balanced with safety can be managed with dignity and respect through the co-creation of resources, programming, and education to support the teams caring for residents who live with dementia and their families.
Footnotes
Acknowledgements
We would like to thank the long-term care residents, families, staff, and care teams that we have the pleasure and privilege to work with, for your trust and your efforts to advance person-centred dementia care.
Ethical Approval
There are no human participants in this article, and informed consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.