
Abstract
Principle 4 of the Pan-Canadian Health Data Charter calls for common standards to enable interoperability, access, and portability of health data. Yet clinically meaningful information, particularly nursing documentation, remains largely unstructured and siloed across care settings. This article argues that nursing data represent a critical but under-leveraged asset for improving patient safety and continuity of care, as it captures early indicators of deterioration, functional decline, and social context often absent from structured datasets. While traditional approaches to standardization have relied on behavioural change, emerging Artificial Intelligence (AI) tools offer a practical alternative by translating narrative documentation into standardized, interoperable formats. Drawing on institutional examples and current evidence, the article examines the possibilities and potential benefits of leveraging AI to fully realize the promise of common standards in practice without creating undue burdens for clinicians.
Introduction: A Preventable Deterioration
At 2:30 a.m., Margaret, a 72-year-old resident of a long-term care facility, arrives at a regional emergency department by ambulance. She is febrile, hypotensive, tachycardic, and confused. She cannot provide a reliable history. The emergency department electronic record shows hypertension and type 2 diabetes. No recent laboratory results. No documented recent infections. No visible trend data.
What is not visible to the emergency team is that over the preceding 48 hours, nurses at her residence documented progressive lethargy, decreased appetite, reduced mobility, and new urinary incontinence. They also recorded subtle confusion and noted that Margaret has previously deteriorated rapidly when urinary tract infections develop. The nursing notes describe these changes in detail.
Each of these observations reflected changes in Margaret’s baseline functional and clinical status—signals that, taken together, could indicate early infection or clinical deterioration. The information exists. It was documented carefully. But it was not captured using common standards. It was not structured for portability. It does not follow her across systems.
Margaret progresses to septic shock within hours. She requires Intensive Care Unit admission and vasopressor support. She survives, but with prolonged hospitalization and significant loss of functional independence.
No clinician failed; however, the system did not meet the expectations embedded in Principle 4 of the Pan-Canadian Health Data Charter: common standards for terminology, health data design, stewardship, interoperability, access, and portability. 1 The failure was not a lack of care. It was a lack of portable, standardized information to support clinical decision-making.
Principle 4: Why Common Standards Matter
The Pan-Canadian Health Data Charter recognizes that without common standards, health systems cannot ensure safe, coordinated, and high-performing care. Common standards enable:
1
• shared terminology across professions and institutions, • consistent health data design, • accountable stewardship, • interoperability across systems, • timely access to clinically relevant information, and • portability of semantic meaning and outcomes measurement across care transitions.
Common standards are therefore not simply technical specifications; they are infrastructure for patient safety and quality. 1
Internationally, HL7’s Fast Healthcare Interoperability Resources (FHIR) 2 has become a foundational framework for interoperable health data exchange. Standardized terminologies such as SNOMED CT 3 and the International Classification for Nursing Practice (ICNP) 4 provide semantic consistency across systems.
These standards are inherently interprofessional. Physicians, nurses, pharmacists, therapists, social workers, and other health professionals all generate clinically meaningful information that must retain semantic meaning as it moves across systems and care settings.
Yet despite broad endorsement of these standards, operational adoption remains uneven—particularly in the domain of nursing documentation. As the largest healthcare profession practicing across all healthcare settings, it is important that nursing documentation is sufficiently standardized to inform the delivery of safe quality care.
While this article highlights nursing documentation as a prime example of an area of clinical practice that would benefit from the application of Principle 4, the concepts and approaches discussed here are equally be applicable to other professional domains. For example, physiotherapists document mobility recovery, pharmacists document medication reconciliation and adherence concerns, and social workers capture social and environmental determinants of health, all of which would benefit from the application of Principle 4 in a similar manner as nursing data. Moreover, Principle 4 extends beyond the sharing of data for clinical care. Common data standards can profoundly improve secondary use of health data, including for research, innovation, population health, and health system management.
Why Standards Struggle in Practice
If common standards are widely endorsed, why do they fail to fully materialize in clinical workflows?
Clinical Work Is Narrative
Many health professionals, especially nurses, rely on free-text documentation to capture evolving clinical situations, contextual observations, and professional judgment that cannot easily be represented through rigid structured fields. These observations are clinically significant but are frequently documented in narrative formats that are not consistently structured or interoperable across systems.
Behavioural Standardization Does Not Scale
Mandating structured documentation assumes uniform adherence under time pressure. A growing body of evidence demonstrates that increasing documentation requirements contributes significantly to clinician burnout and reduced time for patient care, while failing to meaningfully improve the consistency or usability of clinical data.5-7
In short, standards require common behaviour—but common behaviour is difficult to enforce in complex clinical environments.
Nursing Data: A Strategic Blind Spot
Nurses are often the first to detect subtle deterioration. Research on “failure-to-rescue” events consistently shows that adverse outcomes are frequently preceded by early warning signs documented in nursing assessments rather than sudden clinical collapse. The issue is rarely a failure to observe—it is often a failure to make those observations visible across care settings.8-10 As Nagle and White (2025) argue, without standardized clinical data, the impact of nursing practice risks becoming invisible in the digital health ecosystem. 11
Nursing documentation routinely captures predictive indicators of risk, including: • gradual functional decline, • mobility and fall risk, • cognitive fluctuation, • early infection signals, • unmanaged symptoms, • social determinants and caregiver capacity, • patient response to interventions, and • readiness for discharge.
These elements are not peripheral. They are central to safe care.
Functional Decline
Nurses frequently document increasing assistance needs, fatigue, or reduced endurance: “Requires two-person assist to stand; decreased tolerance for activity.”
Functional decline is strongly associated with hospitalization, prolonged length of stay, and institutionalization. Yet functional status is inconsistently structured and rarely portable across systems. Laboratory results may travel; mobility trends often do not.
Mobility and Fall Risk
Fall risk assessments—gait instability, recent falls, and supervision needs—are routinely documented but often captured using local scoring tools that lack semantic alignment across institutions. A “high fall risk” designation in one setting may not be interoperable in another.
As a result, critical safety signals may be lost during transitions of care.
Cognitive Fluctuation
Nurses commonly document early signs of delirium or confusion: “More disoriented than baseline; restless overnight.”
These narrative observations often precede formal diagnosis, yet without standardized representation they remain invisible outside the originating system.
Early Infection Signals
In long-term and home care settings, nurses frequently identify early infection patterns—reduced intake, lethargy, and new incontinence—before laboratory confirmation. In Margaret’s case, these signals were documented, but not portable.
Common standards could support structured representation of such observations, but narrative documentation is rarely mapped consistently.
Unmanaged Symptoms
Nurses monitor and manage symptoms such as dyspnea, pain, nausea, and fatigue. Typically assessed by nurses at varying intervals, using a variety of subjective and objective measures, effective symptom management has been demonstrated to influence outcomes such as length of stay and readmission rates.
Social Context and Caregiver Capacity
Nursing notes often capture caregiver strain, housing instability, or limited support: “Daughter overwhelmed managing medications; patient alone evenings.” These contextual factors significantly influence readmission risk and care outcomes, yet they are inconsistently structured and exchanged.
Response to Interventions
Nurses document dynamic response to care—pain relief after medication, wound healing progression, and mobility improvement. This information reflects care effectiveness but is rarely standardized or shared beyond the local setting.
Readiness for Discharge
Assessing patient’s readiness for discharge is another important metric which is inconsistently documented, if at all, in a majority of acute care settings. Individual’s and families’ capacity to manage continuing care post discharge from acute care requires a more consistent, measured approach.
Why This Matters for Interoperability
These nursing-documented elements are predictive of: 8,9,12 • clinical deterioration, • falls and injury, • delirium, • sepsis, and • readmission.
Yet many interoperability efforts focus primarily on laboratory data, medications, and diagnoses—datasets shaped by billing and reporting requirements.
Common standards for nursing-relevant concepts do exist. SNOMED CT includes nursing terminology, ICNP was developed specifically for nursing language, and FHIR supports structured observations and care plans.
The gap is not the absence of standards. It is the lack of systematic alignment between narrative nursing practice and standardized, portable data design. Without deliberate leadership and professional advocacy, the nursing perspective may continue to be under-represented in standards development and implementation. 11
AI as an Enabler of Common Standards
Artificial Intelligence (AI), particularly Natural Language Processing (NLP), provides a pragmatic bridge between narrative practice and structured standards.
Clinical NLP has demonstrated increasing capability to extract structured concepts from unstructured electronic health record text. Systematic reviews show reliable extraction of symptoms, functional indicators, and care activities from clinical notes.13,14
Importantly, nursing-specific studies have demonstrated that AI models can successfully identify fall risk indicators, mobility changes, and symptom documentation from narrative nursing notes.12,15
AI enables a shift in responsibility. Rather than requiring nurses to encode data into standardized terminologies manually, systems can interpret narrative language and map it to standardized representations aligned with SNOMED CT, ICNP, and FHIR structures.
AI does not replace common standards—it operationalizes them. Moreover, if nursing data can be more easily standardized, emerging AI tools, which depend on structured, interoperable inputs for their quality and effectiveness, can benefit fully from the clinical value offered by nursing data. 11 Without these structured inputs the resultant algorithms may be incomplete and/or inadequate to appropriately inform care decisions.
Enterprise implementations, such as the CogStack platform at University College London Hospitals, demonstrate that large-scale processing of unstructured clinical text is operationally feasible.16,17
From Theory to Implementation: A Practical Model
A realistic strategy aligned with Principle 4 would involve incremental implementation rather than disruptive overhaul.
Light Structural Alignment
Light structural alignment does not mean rigid templates or forcing nurses to code in standardized terminology. It means introducing predictable, clinically intuitive headings that reflect how nurses already think and assess patients.5,18,19
This modest design change improves: • semantic clarity, • AI interpretability, • cross-setting comparability, and • portability of meaning.
From Unstructured Narrative to Light Structural Alignment
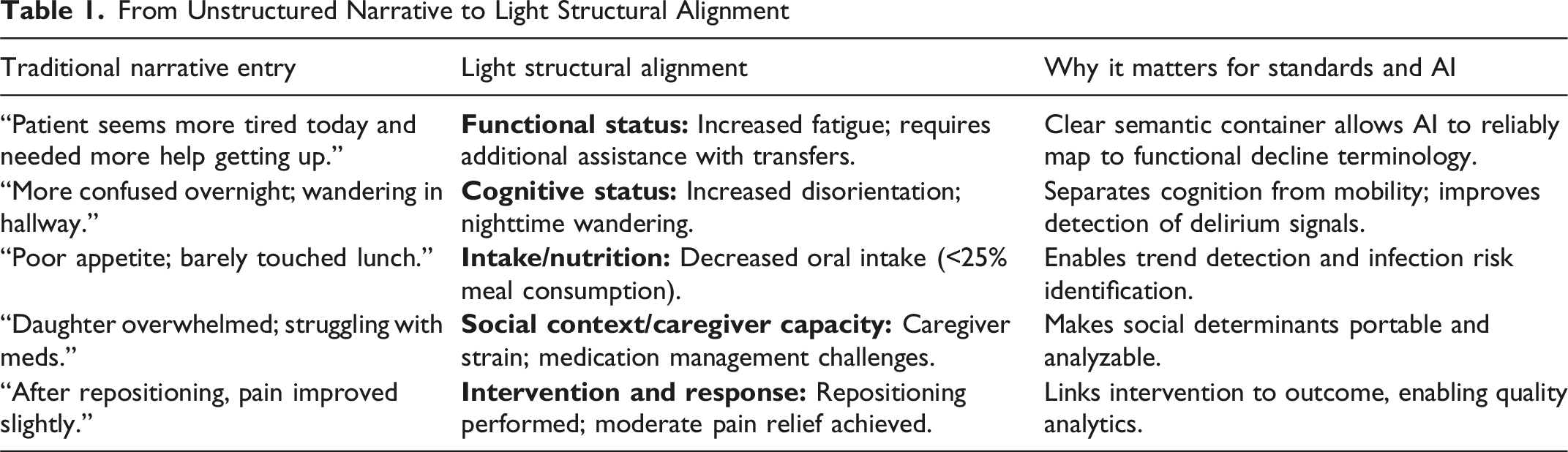
This approach preserves professional judgment while introducing predictable semantic zones.
AI systems perform substantially better when narrative text is bounded within clear contextual categories rather than mixed in a single free-text field.5,18,19
AI-Based Terminology Mapping
Turning Narrative into Portable, Standardized Meaning
Light structural alignment improves clarity. AI-based terminology mapping operationalizes common standards.
The objective is not to replace clinical judgment. It is to ensure that clinically meaningful narrative can be: • interpreted consistently, • mapped to common terminology, • structured for interoperability, and • exchanged in portable formats.
AI tools, either embedded within electronic health records or deployed as middleware, can perform three core functions: 1. Extract key clinical concepts from narrative text; 2. Map those concepts to standardized terminologies; and 3. Output structured representations aligned with FHIR resources.
This is how narrative practice becomes interoperable.
What AI-Based Terminology Mapping Actually Does
When a nurse documents: “Patient more confused than baseline; required two-person assist to transfer; poor oral intake today.”
An AI terminology mapping system performs multiple steps: 1. Identifies clinically meaningful concepts: • increased confusion, • two-person assist for transfer, • reduced oral intake. 2. Determines clinical context: • new change vs. baseline, • functional vs. cognitive vs. nutritional domain. 3. Maps concepts to standardized terminology: • confusion → SNOMED CT cognitive impairment concept, • two-person assist → functional mobility limitation, • reduced oral intake → decreased nutrition intake. 4. Structures output in interoperable format: • FHIR Observation resources, • linked to CarePlan or Condition resources.
Narrative → Standardized Output Example
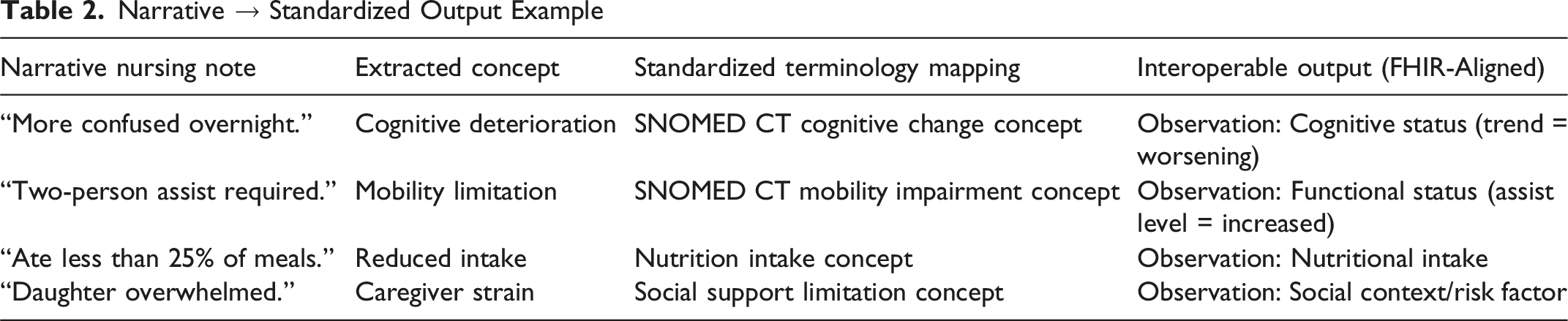
This transformation enables portability without requiring manual coding at the point of care.
Implementation Considerations
Implementation of AI-enabled approaches to interoperability will require more than technology alone. Health systems must still address broader gaps related to governance, procurement, workforce capability, funding, privacy, trust, and organizational change management. Many institutions also continue to face competing operational pressures, legacy infrastructure constraints, and limited interoperability incentives. The availability of AI-enabled terminology mapping and structured data extraction will not, by itself, create interoperable health systems. However, these approaches materially reduce one of the most significant historical barriers to action: the assumption that achieving common standards requires frontline clinicians to fundamentally change how they document care or manually encode large volumes of data into rigid standardized formats.
Importantly, the broader policy and regulatory environment is also evolving. Legislative initiatives such as the proposed Connected Care for Canadians Act (Bill S-5) are expected to accelerate momentum toward interoperable health systems by reinforcing expectations around data portability, accessibility, and interoperable digital infrastructure. As health information technology vendors and institutions increasingly face pressure to support interoperable exchange, AI-enabled approaches offer a practical mechanism to help operationalize common standards in a scalable and workflow-sensitive manner. In this sense, AI-enabled interoperability strategies should not be viewed as an alternative to legislative and policy reform, but rather as a complementary implementation tool that supports and advances those broader objectives. Collectively, these developments reduce many of the longstanding practical “excuses” for inaction and make it increasingly difficult to justify maintaining fragmented, non-portable approaches to the management and communication of clinically meaningful health data.
Ethical and AI Governance Considerations
While AI-enabled interoperability offers significant potential benefits, its implementation raises important ethical, legal, and operational considerations, including privacy, data governance, algorithmic bias, transparency, accountability, and the risk of overreliance on AI-generated outputs. Ensuring appropriate stewardship, human oversight, clinical validation, and equitable model performance across diverse populations will be essential to maintaining trust and patient safety. These considerations warrant careful attention; however, a comprehensive analysis of AI governance and risk management frameworks is beyond the scope of this article.
Re-Imagining Margaret’s Outcome
If Margaret’s nursing documentation had been mapped to standardized terminologies and structured for portability, her early deterioration would have been visible at the point of acute care. The emergency team could have recognized her trajectory sooner. Antibiotics might have been initiated earlier. ICU admission may have been avoided.
Principle 4 is fundamentally about ensuring that information retains its meaning as it moves across systems. AI-enabled terminology mapping and structured extraction make that goal achievable without fundamentally redesigning clinical practice.
Conclusion: Making Standards Matter
Common standards exist. The Health Data Charter articulates them clearly. International frameworks support them. The remaining challenge is operational. Nursing documentation captures the patient’s evolving story. But until that story is standardized and portable, interoperability will remain incomplete.
Artificial intelligence now provides a credible pathway to bridge narrative clinical practice and structured, interoperable data. The opportunity for Canadian health leaders is to move from endorsing common standards to designing systems that make those standards function at the bedside. Because when information follows the patient—and retains its meaning—harm can be averted and outcomes improved.
Footnotes
Acknowledgements
Acknowledgments of AI Use: Artificial intelligence tools were used to support aspects of literature synthesis, drafting, and editing in the preparation of this manuscript. All content was reviewed, validated, and substantively refined by the authors, who retains full responsibility for the accuracy, interpretation, and conclusions presented.
Ethical Approval
Institutional review board approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.