
Abstract
Long-Haul Truck Drivers (LHTDs) have been identified as a high-risk population for chronic conditions. Health promotion programs have largely focused on individual behaviours, with less emphasis placed on the broader environmental factors. However, there is growing evidence that effective strategies must consider both individual and environmental factors. Through a social-ecological lens this mixed-methods study explored how the mobile work environment impacts health and health behaviours amongst LHTDs on the Canadian Prairies. Data were collected through semi-structured interviews with 13 participants, diet and activity logs, and a mobile work environment assessment of the Trans-Canada Highway between Manitoba and Alberta. Individual, occupational and policy level influences on the health and health practices of LHTDs were identified. Leaders in health policy are in a key position to build inter-sectoral, collaborative relationships and advocate for the necessary policy changes to create a healthy work environment for LHTDs.
Introduction
Long-Haul Truck Drivers (LHTDs) are a high-risk population for cardiovascular disease, diabetes, sleep apnea, musculoskeletal injuries, and stress.1-3 Sedentary work, irregular schedules, limited opportunities for Physical Activity (PA), and diet, all contribute to the onset of chronic conditions among LHTDs.2,4,5 Commercial truck driving has been described as an “obesogenic” occupation, with multiple risk factors contributing to poor health outcomes. 6 Driver obesity and associated chronic illnesses have been linked to increased absenteeism, driver turnover, lost time injuries, and higher crash rates.5,7
Research consistently reports poor diet and limited PA behaviours among LHTDs. Studies show that the majority of LHTDs consume fewer than the recommended servings of fruits and vegetables and most include unhealthy foods in their daily diet.1,8,9 Approximately 65.3% of LHTDs are inactive, 1 70% of drivers report they do not exercise regularly 10 and 80% do not meet the national activity guidelines for moderate and vigorous intensity PA. 11
Health Promotion (HP) programs have the potential to improve the health of LHTDs. However, the primary focus of many initiatives has been on individual level interventions with little attention to the organizational, environmental, and policy factors necessary to support health. 12 Houghtaling et al 13 conducted a systematic review examining aspects of the trucking environment that influence food and PA practices of LHTDs. Environmental barriers to healthy eating include less availability of healthy, affordable food options and the wide availability of unhealthy foods and beverages for purchase.14,15 Lack of time, inflexible hours, limited exercise facilities, and showers were identified barriers to PA. 13
LHTDs spend long periods of time away from home and the amenities available to them while on the road comprise an important component of their work environment. Lincoln et al 14 conducted an environmental assessment of truck stops across the U.S. and found that 81% of truck stops lack a safe walking area, 50% lack fresh fruit, and 37% lack fresh vegetables in their restaurant or convenience store. Although a similar environmental assessment of the mobile work environment in Canada has not been conducted, one study examined the truck stop preferences of Canadian LHTDs and identified the availability of healthy and affordable foods, access to exercise facilities, equipment, showers, and washrooms were among the most important amenities needed to support health and wellness. 15
Social-ecological approaches to workplace HP are designed to address the complex interdependencies between individual health practices and aspects within the work environment. An ecological perspective that targets both workers’ behaviours, as well as environmental and structural factors, is recommended as a more effective approach to HP programming amongst LHTDs.
7
LHTDs spend long periods of time on the road, yet only a few studies have explored how the work environment impacts their ability to maintain a healthy diet and PA. This research adopts a social-ecological perspective16,17 to address this gap. The objectives of the study are to: 1. Describe how the mobile work environment supports or hinders the HP practices of LTHDs. 2. Identify the current dietary and PA practices of LHTDs while at work. 3. Explore LHTDs’ perceptions of barriers and facilitators to adopting and maintaining healthy lifestyle practices while at work.
Methods
Ethics Statement
Approval for the research was received from the Brandon University Ethics Committee #22832.
Data Collection
This study used a parallel mixed-methods design. Data were collected from three sources: an environmental assessment of the mobile work environment, semi-structured interviews, and self-reported diet and activity logs.
Mobile Work Environment
The mobile work environment assessment explored the amenities that were available to LHTDs at truck stops along the Trans-Canada Highway (TCH) between Winnipeg and Calgary. The TCH was divided into highway segments of approximately 100 kilometers, and a list of all truck stops within each segment was created. Stratified, random sampling was used to select a sample of 20 truck stops. An adapted version of the National Institute for Occupational Safety and Health observational checklist of truck stop resources 14 was used to assess truck stop amenities. Information on rest stops, safe and accessible parking, and roadside pullouts along the TCH were assessed using an in-transit assessment tool developed specifically for this research.
Semi-Structured Interviews
Semi-structured interviews were conducted with 13 truck drivers who drove a long-haul route between Manitoba and Alberta. Interview questions explored the current health practices of participants and perceived barriers and facilitators to healthy eating and PA while on the road.
Diet and Activity Logs
Nine of the thirteen participants completed diet and PA logs while driving their long-haul route. Drivers manually recorded their food intake in a logbook and were provided with a tablet to take photographs of all food and beverages consumed while on the road. In addition, they recorded the type, intensity and purpose of all PA. A second semi-structured interview was conducted after the trip to review the data.
Participant Recruitment
Convenience sampling was used to recruit participants. Information about the research was provided to eligible drivers through company communications. Recruitment postcards were also distributed to trucking companies and the Manitoba Trucking Association. Informed consent was obtained prior to beginning each interview.
Data Analysis
A parallel approach to data analysis was used. Each source of data was analyzed independently and integrated once the analysis of each component was complete. Qualitative interview data were transcribed verbatim and a framework approach to qualitative analysis was carried out. Framework analysis provided a structured and rigorous process for conducting qualitative data analysis while maintaining the flexibility required to identify and characterize themes that emerge from the data. 18 Consistent with the approach described by Richie and Spencer 19 the framework analysis was carried out in five distinct, yet interconnected stages: familiarization, identifying the thematic framework, indexing, charting, and mapping and interpretation. Frequency distributions and percentages were tabulated for the quantitative data from the environmental assessment tool, interview guide, and the diet and PA logs. Nutrient analysis of the diet log data was carried out using the Diet and Wellness Plus software program 2020-2025 version. This software compares dietary intake with the recommendations of the MyPlate guidelines provided by the United States Department of Agriculture and aligns closely with Canada’s Food Guide. An American nutrient analysis program was utilized because at the time the study was conducted, a credible Canadian tool of this calibre was not available.
Results
Sample Characteristics
A total of 13 LHTDS participated in qualitative interviews and 9 participants completed the diet and PA logs. The average age of participants was 48, all participants identified as male, and years of experience as a truck driver ranged from 5 to 50 years. Six participants drove in teams of two and seven drove alone. Three quarters (77%) of participants had a BMI in the overweight to obese category. On a scale of one to ten, self-reported ratings of their current health ranged from a low of 5 (n = 3) to a high of 8 (n = 1). The majority of participants (n = 7) rated their health as a 7 or 7.5. All drivers, regardless of their self-rating, felt their overall health status could be improved.
Mobile Work Environment
Truck stops had limited availability of key food items (fruits, vegetables, unprocessed meat, wholegrains, healthier restaurant menu options) that contribute to a healthy diet. Less than half (40%) of the locations sampled offered fresh vegetables, only 10% sold unprocessed meats, none of the locations had plant-based meat alternatives and although 50% of truck stops sold fresh fruit, variety was limited. Snacks were readily available; however, healthier options (baked, unsalted, low fat) were not available at all locations.
Indoor or outdoor exercise facilities were not available at any of the truck stops sampled and only 10% of locations had access to a designated walking path. A lack of parking for trucks restricted access to grocery stores, restaurants, and other services outside of truck stop locations. The number of rest stops and roadside turnouts accessible to single trailers and Long Combination Vehicles (LCVs) was extremely limited. As a result, drivers conducted vehicle checks on the shoulder of the highway where they were exposed to highway traffic and associated hazards.
Diet and Physical Activity
All participants brought food from home. One participant consumed only home food, and eight participants consumed a mix of home and purchased food. Based on the MyPlate guidelines, the nutrient analysis showed that only a small percentage of the daily requirements for fruit (11%), vegetables (12%), whole grains (21%), lean protein (15%), and low fat or fat-free dairy (5%) were met by participants.
Work related tasks accounted for 91% of all PA while on the road. PA occurred in short bursts and followed long periods of sedentary driving. A total of 63.5% of activity was rated as low intensity and included vehicle checks, refueling, and walking. Moderate intensity (17.56%) and high intensity (7.66%) activities included load securement, coupling and uncoupling trailers, and cardio workouts. Low intensity walking was the most frequent activity undertaken for leisure or exercise (70%), often carried out in 5 to 15 min intervals during refueling and/or vehicle check stops. No participants reported using exercise facilities while on the road.
Multi-Level Influences
Through a social-ecological lens, the qualitative data analysis revealed interrelated, and multi-level factors impacting the dietary and PA practices of LHTDs. These factors were categorized into three levels: individual and family, occupational/organizational, and policy. (Figure 1). Multi-level influences on health behaviours of long-haul truck drivers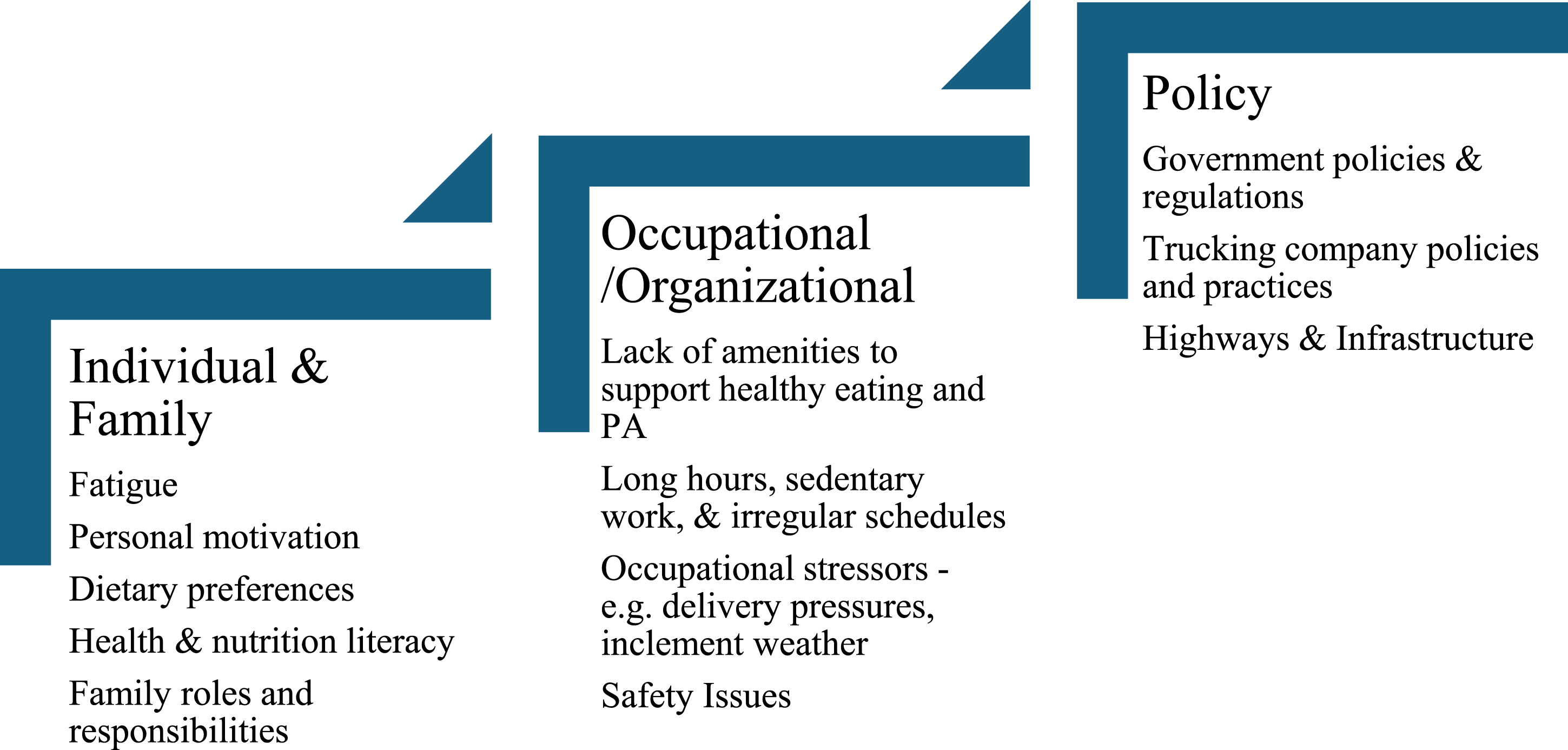
Individual/Family Factors
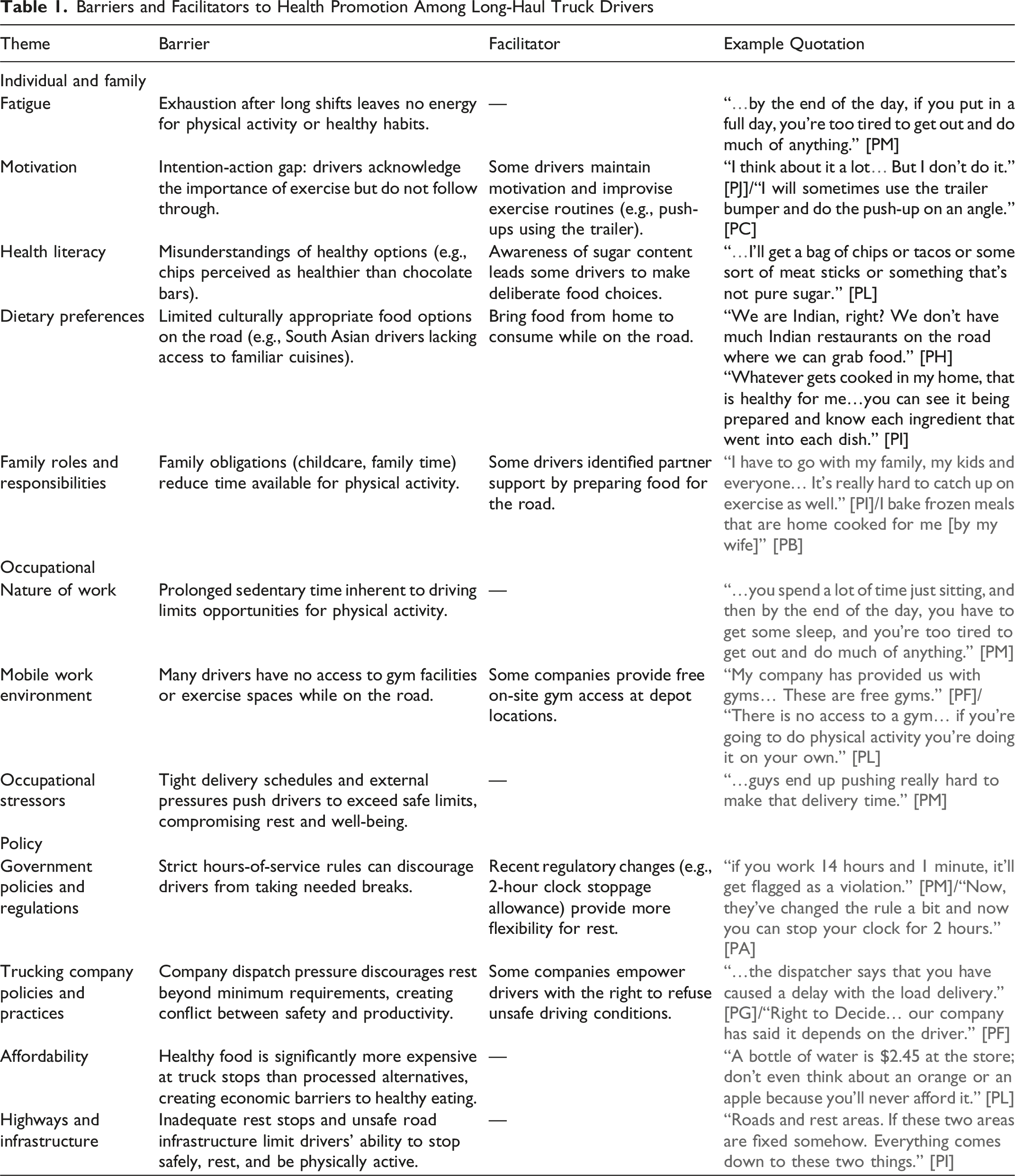
Barriers and Facilitators to Health Promotion Among Long-Haul Truck Drivers
Occupational/Organizational Factors
Consistent with the findings of the environmental assessment, the lack of amenities available at truck stops to support healthy eating and PA was highlighted by participants. The limited availability of affordable healthy food options and limited access to exercise facilities were considered barriers. Participants also reported the sedentary nature of their work, physical demands of truck driving, long hours away from home, irregular schedules, occupational stressors (e.g., delivery pressures, inclement weather, limited temporary, and overnight parking), and safety concerns were barriers to maintaining a healthy lifestyle while on the road.
Truck and company amenities were identified as key facilitators. The presence of a fridge and microwave in the truck allowed participants to bring food from home. Exercise facilities, provided by several trucking companies for their drivers, were viewed favourably, although time constraints and other occupational pressures limited participant use (Table 1).
Policy Factors
Trucking company policies and dispatch personnel who respected drivers’ decisions and a company culture that supported the health and safety of drivers were identified as important factors to promote driver health and well-being. The lack of infrastructure to support the health and safety of drivers was highlighted by all participants. Poorly maintained highways (e.g., snow clearing in winter and potholes in summer), too few designated rest stops, inadequate access to roadside turnouts, limited walking paths, washroom facilities, and limited temporary and overnight parking spots were all highlighted as barriers to health and safety (Table 1).
Discussion
The trucking industry in Canada employs over 324,000 truck drivers and generates more than 39 billion Canadian dollars in annual revenue. 20 The sustainability of the industry requires a healthy workforce and a mobile work environment that supports the health of LHTDs, yet the findings of this study highlight that significant improvements to the environment across the Canadian Prairies are needed.
Consistent with prior studies, the truck stops included in this research offered a limited variety of healthy/healthier food options,6,7,14,15 and the few items that were available were considered too expensive by many drivers. 15 To accommodate the lack of healthy, affordable food available for purchase, LHTDs brought all or some of their food from home. Home foods ranged from snack items to fully prepared meals that were purchased at grocery stores or prepared at home in advance of their trip. The availability of fridges in the truck cabins was a key facilitator; however, the fridges were small, and the amount of food LHTDs could bring was limited. As a result, drivers have to purchase additional food items at truck stops. 15 To facilitate healthy eating, it is important that truck stops carry commonly used food items, such as eggs, bread, fruits, and vegetables, and that healthy foods are sold at affordable prices. 15
As reported in other studies, the LHTDs in this study did not meet the guidelines for daily servings of fruits, vegetables, lean proteins, and low-fat dairy.1,8 Several of the LHTDs interviewed lacked basic knowledge of nutrition and were uncertain of the healthiness of certain foods and nutrients. Limited food and nutrition literacy acts as a barrier to healthy eating7,13,21-23 and is important to address in HP programming.
Walking was the most frequent form of PA by LHTDs in this study. Drivers tried to get in “a few extra steps” when refueling or conducting safety checks or by taking short walks before or after their shift. Two HP programs that aimed to increase the daily step counts of LHTDs have shown positive short-term results24,25; however, the efficacy of HP programs can be enhanced through organizational policies that address workplace pressures, management support, and a company culture that emphasizes the health of drivers.26-28 Investments in highway infrastructure are also needed. The LHTDs in this study identified a sparsity of roadside turnouts, walking paths and rest areas accessible to single trailers and LCVs. As a result, drivers were forced to walk along the highway adjacent to traffic. This represents a serious safety hazard and highlights the need for improved infrastructure to support driver health and safety.
The infrastructure to support PA while on the road is extremely limited. None of the truck stops included in this study provided exercise facilities or equipment, and only 10% had access to a walking path. Company gyms were available to a small number of participants, and while perceived as valuable, they were rarely used. Access to exercise facilities while on the road is important to promote PA 15 ; however, these findings highlight that building gyms is not enough. Like other studies, LHTDs identified long working hours, irregular schedules, delivery pressures, lack of managerial support, and compensation by the mile are significant barriers to PA for LHTDs.15,26-31 To be effective, HP initiatives need to also address these broader organizational and policy factors.
A Multi-Level Approach to Health Promotion: Recommended Actions
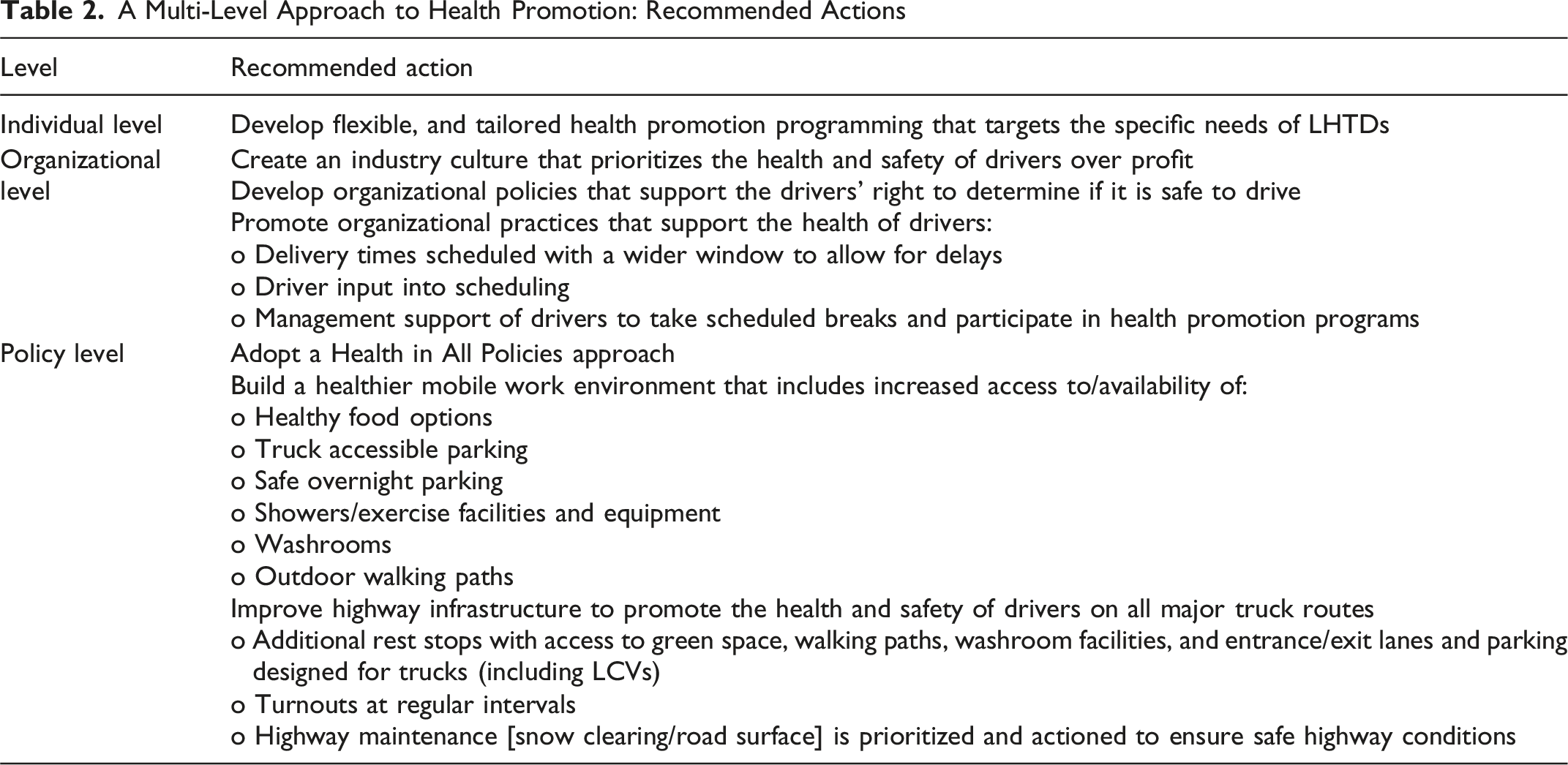
Health in All Policies is an approach that highlights the importance of considering the potential health effects of every decision and policy. It recognizes that the health of a population extends beyond the health sector to include multi-levels of government and sectors. 34 This approach is key to promoting the health of LHTDs in Canada. Responsibility for the policies, laws, regulations, roads and infrastructure that impact the trucking industry, and the health of drivers, span multiple sectors within local, provincial, territorial, and federal governments. Increased coordination between trucking companies, truck stop businesses, and multi-levels of government are needed to address these key occupational and population health challenges. Health policy leaders are uniquely positioned to advocate for Health in All Policies and build inter-sectoral, collaborative partnerships between the trucking industry and all levels of government to create a healthy work environment for LHTDs.
Limitations
The use of self-reported data, collected in the diet/PA logs, may have resulted in an over/underestimation of diet/PA behaviours. In addition, the small sample size and the recruitment of all-male participants, limit the generalizability of the study findings.
The initial goal of the study was to recruit 20 LHTDs. However, after 18 months only 13 participants were successfully recruited. Almost 97% of truck drivers in Canada are male. 20 Prior studies have reported similar challenges recruiting men to participate in health research. Identified barriers include health privacy concerns, time commitment, and a lack of interest in the research.35,36 Stigma is another potential barrier to participation for LHTDs. Health stigma places the blame for chronic conditions and poor health on individual behaviours and is associated with reduced participation in health promotion programming.37,38 Although, not explored in this study, health stigma may have had a negative impact on participant recruitment and is an important factor to explore in future HP research with LHTDs.
Conclusion
This study adds to mounting evidence that health promotion for long-haul truck drivers demands a coordinated, multi-level response. As a population carrying disproportionate chronic disease burden, long-haul truck drivers cannot be adequately served by single-sector or individually focused interventions. Health leaders are uniquely positioned to broker the cross-sector partnerships and drive the systemic changes necessary to make healthy work environments not just possible, but standard.
Footnotes
Acknowledgements
A sincere thank you to the Manitoba Trucking Association, members of the Research Advisory Committee, and the research assistants Jasmin Bhasin, Tara Lynn Frykas, and Jesse Windsor for their contributions to this research project.
ORCID iDs
Ethical Approval
This research was approved by the Brandon University Ethics Committee #22832.
Consent to Participate
Informed, verbal consent was obtained prior to beginning each interview. Verbal consent was captured on the interview transcripts and documented by the interviewer.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Research and Workplace Innovation Program of The Workers Compensation Board of Manitoba.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are not available for use by other researchers as open access to data was not included in the approved ethics submission.