
Abstract
Diabetes disproportionately affects Indigenous populations in Canada, reflecting the enduring impacts of colonialism, structural inequities, and systemic barriers within healthcare. The “Walking Together in the Same Direction” project developed a community-driven, culturally rooted diabetes prevention framework with ten First Nations communities across South Vancouver Island, British Columbia. Through circle discussions, communities did not simply share experiences—they co-created a 13 Moons framework grounded in Indigenous ways of knowing. This cyclical model reflects a holistic understanding of health across physical, emotional, mental, and spiritual domains, aligned with seasonal teachings and community life. It represents a critical shift from adapting Western models toward centring Indigenous knowledge as the foundation of care, demonstrating community-led design, self-determination beyond consultation, and tangible Indigenous-led outcomes. This work highlights the importance of moving from linear, biomedical approaches toward relational, culturally grounded models that privilege trust, continuity, and holistic wellness.
Introduction
Chronic diseases, particularly type 2 diabetes, represent a significant and growing burden among Indigenous peoples in Canada. Prevalence rates are several times higher than in non-Indigenous populations, with earlier onset and more severe complications. These disparities are rooted not in individual behaviours, but in the social and structural determinants of health, including colonization, intergenerational trauma, and systemic barriers to culturally appropriate care.
Conventional chronic disease management models often fail to meet the needs of Indigenous communities as they are typically designed around biomedical frameworks that do not fully account for wholistic approaches to health, cultural context, relational approaches to care, or community priorities. There is increasing recognition that effective diabetes care must move beyond standardized clinical pathways toward approaches that are culturally safe, community-led, and grounded in Indigenous ways of knowing. This includes incorporating First Nations’ perspectives on health and healing and the root causes of diabetes 1 as well as drawing on the strengths and resilience of First Nations Peoples, including the strengths of families, communities, and cultures to support First Nations people in adopting healthy behaviours. 1
While many chronic disease initiatives seek to incorporate Indigenous perspectives into existing healthcare systems, this project differs in that Indigenous knowledge systems were positioned as foundational to the design of care itself. The resulting 13 Moons framework emerged directly from community-led engagement and reflects a place-based, relational, and cyclical understanding of wellness grounded in Indigenous ways of knowing. This article contributes practice and organizational insights for healthcare systems seeking to move beyond culturally adapted care toward Indigenous-led care design and governance.
Context and Setting
Type 2 Diabetes (T2D) presents a significant and growing health challenge worldwide, with its prevalence continuing to escalate in recent years. The condition arises from various factors, including genetic predisposition, lifestyle influences, and environmental influences.2,3 However, the impact of T2D extends beyond individual health outcomes, particularly within Indigenous communities, where historical and ongoing colonial trauma exacerbates health disparities.3-8
This article draws on a regional initiative in British Columbia aimed at improving diabetes care for Indigenous populations through a model referred to as “Walking Together.” The initiative was developed through partnerships between health leaders, First Nations communities, and primary care providers, with a shared commitment to advancing equity and reconciliation in healthcare delivery.
The population served includes diverse First Nations communities across urban, rural, and remote settings where First Nations access to care is often fragmented, with significant geographic, cultural, and systemic barriers impacting continuity and quality of care.
Methods
This First Nations-led engagement and quality improvement project was supported by a Michael Smith Foundation for Health Research Collaboration and Convening (C2) grant and hosted by Island Health. The project aligned with First Nations Health Authority (FNHA) “7 Directives” and underwent Island Health Quality Improvement Ethics review.
The project team included First Nations and non-Indigenous leads, community health workers, nutritionists, diabetes nurses/dieticians, local First Nations health leadership, FNHA researcher, and most importantly, community advocates. The project aimed to answer four key questions through invitational Indigenous circle discussions: 1. What does diabetes mean to you and how has it impacted you and your loved ones? 2. What do you find most helpful in supporting you or your loved ones’ journey with diabetes? 3. What could be improved upon to better support you or your loved ones’ journey with diabetes? 4. What are some community activities/programs/strategies you would like to see to help prevent diabetes for your children, grandchildren and the future generations?
Between July 2022 and November 2023, we engaged circle discussions with 10 First Nations communities to explore experiences related to diabetes prevention, treatment, and management. Guided by four key questions, discussions followed First Nations knowledge-sharing practices grounded in storytelling, relationality, and respect. Communities included Xwsepsum (n = 17), Paaʔčiidʔatx̣ (n = 15), W̱JOȽEȽP' (n = 26), SȾÁUTW̱ (n = 25), T’Sou-ke (n = 15), Songhees First Nation (n = 13), Sc’ia’new (n = 8), Tseycum First Nation (n = 6), Malexet (n = 19), and BOḰEĆEN (n = 7). These discussions were possible because of the existing relationships that the diabetes nurse and dietician had with existing communities and were integral to establishing trust, deepening mutual understanding, and enabling community members to share personal and communal insights on diabetes.
Circle discussions were facilitated using relational and trauma informed approaches grounded in Indigenous engagement practices.9-11 Facilitation emphasized respectful listening, voluntary sharing, and flexibility to support community-defined priorities and comfort levels. Community relationships established prior to the project were central to creating culturally safe spaces for dialogue and participation.9-11
Narrative data from each circle discussion remained anonymous and were recorded and securely stored in a REDCap (Research Electronic Data Capture) database, stratified by community. The data were then exported into an Excel spreadsheet, imported into NVivo10 software, and analyzed using inductive thematic analysis. Coding were developed for thematic categories or “domains” and were initially analyzed for each community, with creation of “sub-themes” where appropriate. The domains were then compared across communities and merged to identify common themes. We determined the identified domains and themes were common across all participating First Nations communities and no unique themes emerged for individual communities. However, personal experiences and expressions varied within common themes. Finally, the themes were integrated across the four guiding questions to present a comprehensive understanding of diabetes-related experiences, barriers, strengths, and priorities. Themes were validated through collaborative discussion with participating communities during design of the 13 Moons framework. 12
Key Themes From Community Engagement on Diabetes
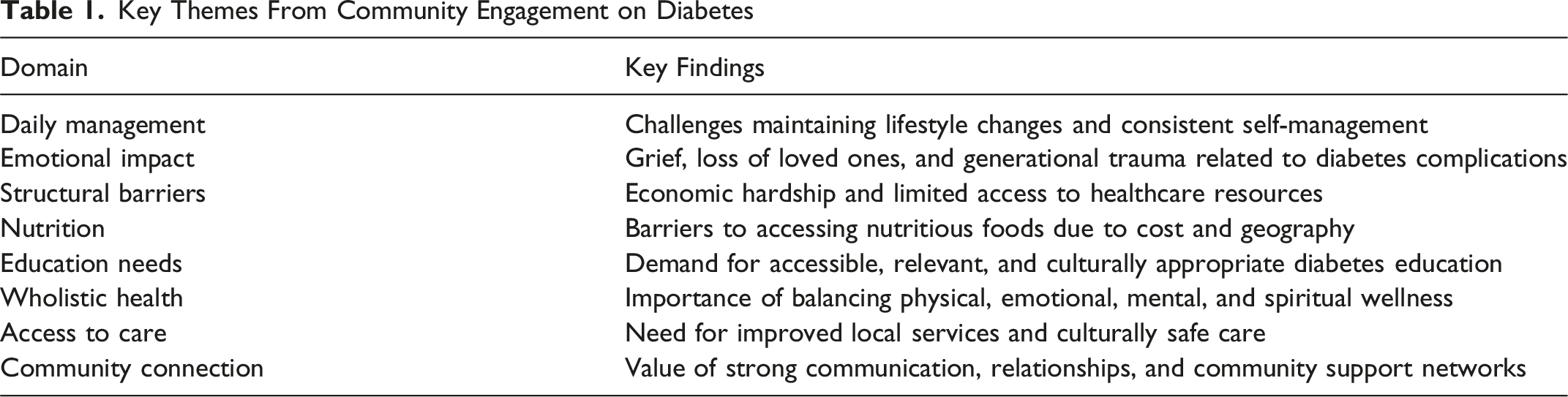
Illustrative examples include: “Its hard knowing I lost uncles to it [diabetes].” (Emotional impact) “Diagnosed in 2020 and today is the most I’ve learned about it [diabetes].” (Educational needs) “Need to make community resources, such as gym spaces or building spaces, accessible and low or no cost.” (Daily management) “Consultation with our families, elders and individuals in our community who have diabetes and support loved ones with diabetes to find out exactly what they need.” (Community connection)
These findings highlight the need for culturally grounded interventions that address not only individual health, but also the broader social, emotional, and family and community contexts of wellness.
A key outcome of the engagement process was the co-creation of a 13 Moons framework, developed directly from community knowledge shared through engagement. Participants did not only describe barriers and supports—they articulated a cyclical, seasonally grounded understanding of health that reflects Indigenous ways of knowing. This framework aligns wellness across physical, emotional, mental, and spiritual domains with seasonal teachings, cultural practices, and community life. Unlike linear, biomedical approaches to chronic disease management, this framework emphasizes balance, continuity, and relational engagement over time. The framework represents a tangible, community-led output that reflects self-determination in action and moves beyond consultation toward Indigenous-led knowledge creation.
Operationally, the framework informed discussions regarding seasonal activities, food practices, movement, community gatherings, land-based wellness, and relational approaches to chronic disease management. Rather than organizing care solely around biomedical indicators or episodic appointments, the framework supported ongoing engagement grounded in culturally continuity, community rhythms, and wholistic wellness practices identified by participating Nations. The framework also provided a shared structure for conversations between communities, healthcare providers, and leadership regarding priorities for culturally grounded diabetes prevention and care.
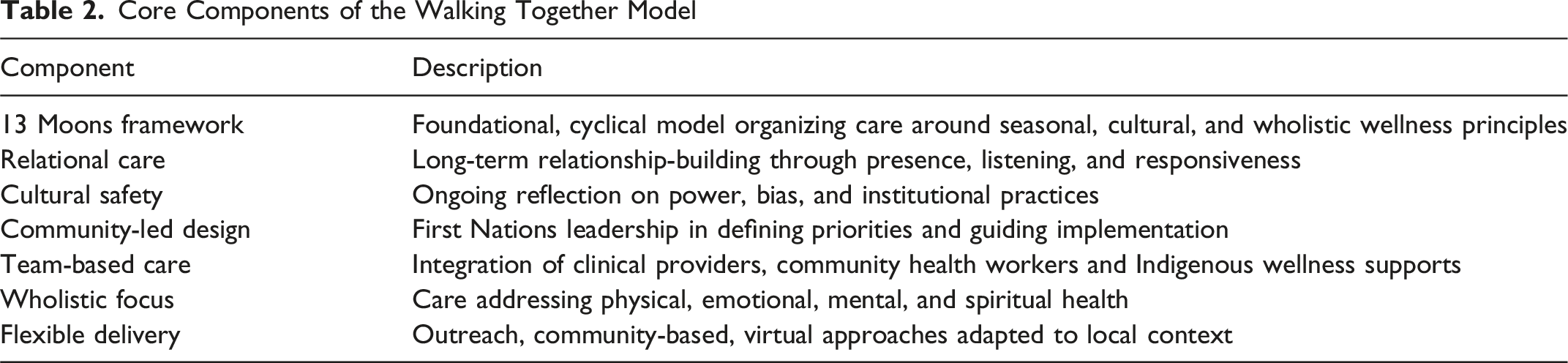
Model Description: A Walking Together Approach
The Walking Together model is grounded in principles of relationality, respect, reciprocity, and self-determination. Rather than imposing externally designed interventions, the model emphasizes co-development with communities and flexibility to adapt to local context.
Core Components of the Walking Together Model
Implementation and Enablers
Implementation emphasized flexibility and sustained relationship-building. Trust between healthcare providers and First Nations communities was foundational.
Key enablers included strong partnerships between communities and health authorities, leadership support, and embedding Indigenous specific anti-racism and cultural safety within organizational priorities. Flexible funding mechanisms enabled teams to adapt services to community needs, rather than adhering to rigid program structures.
Early impacts include increased patient engagement, improved continuity of care, and strengthened provider confidence in delivering culturally safe care. Patient engagement has increased, with more consistent participation in diabetes care and follow-up. Providers report improved understanding of culturally safe practices and greater confidence in working collaboratively with First Nations communities. Continuity of care has improved through stronger relationships and more coordinated service delivery. Importantly, success was defined not only by clinical indicators but by relational outcomes such as trust, connection, and alignment with community priorities. This emphasizes the need to have learning and systematic evaluation embedded not only within practice, but within healthcare systems themselves. This is required for sustainable commitment to organizational goals addressing Indigenous health and for consideration of system-level impacts on the Indigenous communities they serve. Ongoing challenges include workforce capacity, jurisdictional complexity, and the need for sustained investment, highlighting the importance of system-level change (Figure 1). 13 Moons framework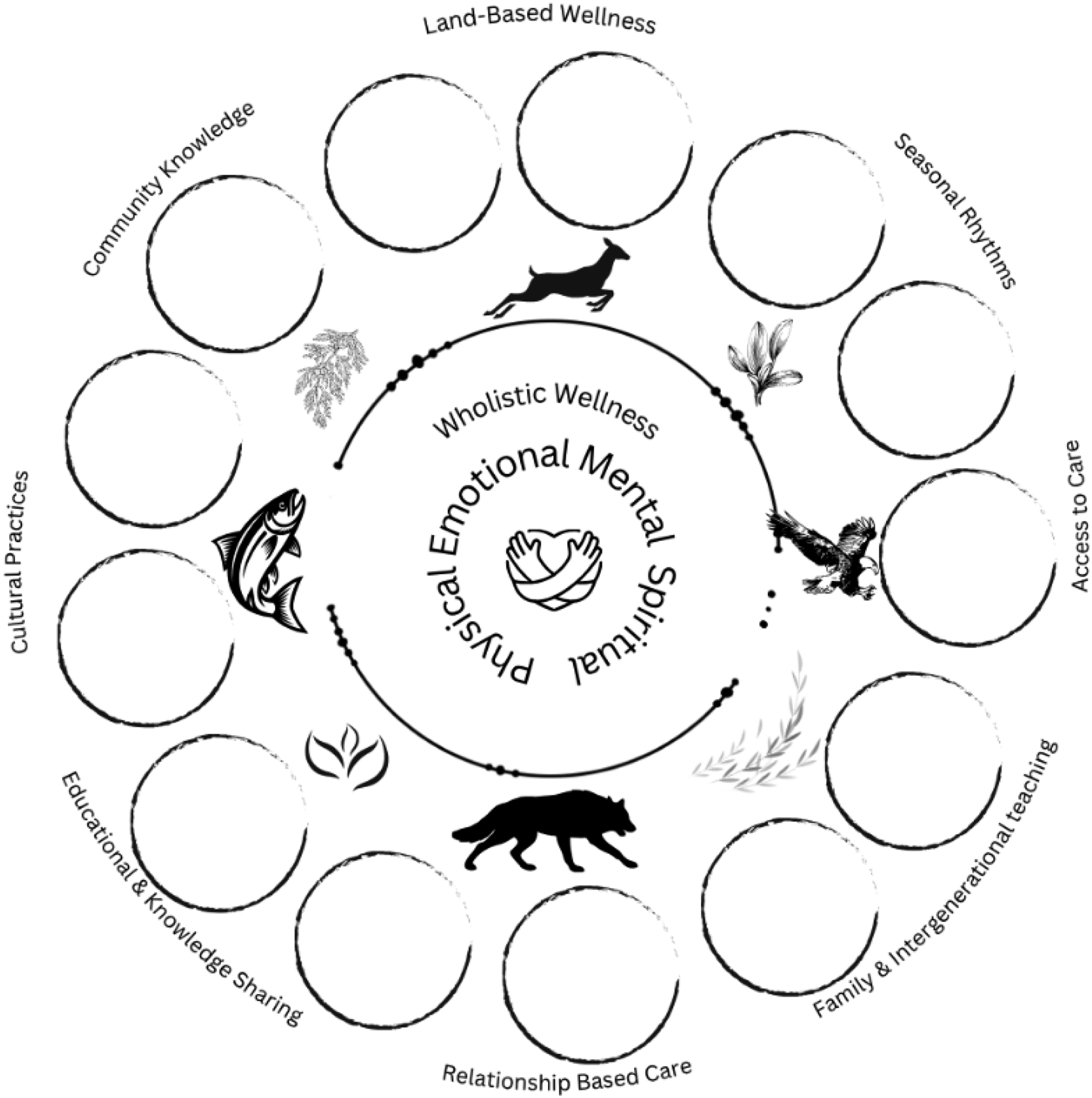
Discussion
The Walking Together model illustrates a definitive shift from disease-focused, transactional models to wholistic, relational models of care for chronic disease management for Indigenous populations. Central to this shift is the 13 Moons framework, which moves beyond integrating Indigenous perspectives into existing systems and instead uniquely positions Indigenous knowledge as the foundation for care design. This requires that leaders, governance and care delivery models organize health services delivery around cyclical, seasonal, and relational principles. The 13 Moons framework challenges dominant linear approaches to chronic disease management and supports more continuous and contextually relevant engagement with health from a wholistic, rather than disease-focused perspective.
For health leaders, this shift requires more than program adaptation—it requires structural and organizational change grounded in local relationships and accountability. This initiative uniquely demonstrates that Indigenous health frameworks cannot be standardized, generalized or made to conform to fragmented business or tech-enabled models of care delivery. Care delivery must be rooted in local knowledge systems and developed in direct partnership with the specific Nations in whose territories care is being delivered. Embedding Indigenous partnerships within governance and decision-making is essential to ensuring that care models reflect community priorities, cultural teachings, and expressions of self-determination. For this to succeed, leaders must consider how their governance models, business models and care-delivery models either align or conflict with the Indigenous 13 Moon framework and adjust both structures and processes as necessary to prioritize and respect Indigenous care designs.
Leadership must also support a transition from episodic service delivery toward relationship-based models of care, recognizing that trust, continuity, and connection are core components of effective chronic disease management and care sustainability. Operationally, this includes aligning funding and accountability structures with long-term, community-driven goals, rather than short-term, efficiency-based metrics. Workforce development must extend beyond training to include ongoing, cultural safety, humility, and reflexive practice grounded in local context. Changes in leadership positions and structures must consider impacts on Indigenous relationships, with transitions and introductions to new leaders conducted with intention, respect and awareness of impact on Indigenous community relations and trust. In parallel, evaluation approaches must expand to reflect not only clinical outcomes but also relational and community-defined indicators of wellness specific to each Nation.
Importantly, implementation challenges were not solely clinical, but structural. Existing healthcare systems are often organized around standardized service delivery, fragmented funding structures, efficiency metrics, and short-term outcomes that may conflict with relational, community-paced, and Nation-specific approaches to care. Sustainable implementation therefore requires healthcare organizations to critically examine how institutional policies, leadership structures, accountability mechanisms, and operational priorities may unintentionally undermine Indigenous-led models of care.
The co-creation of the 13 Moons framework demonstrates that Indigenous-led, place-based knowledge generation is essential to meaningful healthcare transformation. Positioning Indigenous frameworks as foundational—and ensuring they are developed with and accountable to local Nations—provides a pathway for leaders to reorient systems toward more equitable, responsive, and sustainable models of care.
Conclusion
The co-creation of the 13 Moons framework illustrates how Indigenous-led knowledge systems can fundamentally reshape chronic disease care when positioned as the foundation, rather than an adaptation, of healthcare design. Addressing diabetes disparities among Indigenous populations requires more than incremental improvements to existing models of care. It calls for a fundamental shift toward approaches grounded in respect, relationship, and self-determination. The Walking Together model offers a promising example of how healthcare systems can partner with Indigenous communities to co-create more equitable and effective chronic disease management strategies.
Footnotes
Ethical Approval
Institutional Review Board approval was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Michael Smith Health Research BC (C2-2021-2399).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: grant for program evaluation.