
Abstract
Burnout among Canadian Family Physicians (FPs) is a significant concern, as is their lack of capacity and skillset in supporting patients’ mental health conditions in clinics. This article reports evaluation results of an 8-week group-based mental health skills program delivered virtually to 698 physicians in British Columbia with the dual objectives of (1) providing skills physicians can use to support patients experiencing mental health concerns and (2) supporting physician wellness. A mixed methods approach was employed. Professional Fulfilment (PF), Burnout (BO), and resiliency outcomes were assessed at pre-, post- and 1-year follow-up using the Stanford Professional Fulfillment Index and the Brief Resiliency Scale (resiliency). An anonymous survey was administered upon completion of the program, and again at 1-year follow-up to assess learning outcomes and program value. Twelve participants provided additional feedback through focus groups and interviews. Participants were primarily family physicians working in urban settings. Pre- to post-paired t-test results showed improvements for professional fulfilment (P < .001), burnout (P < .001), and resiliency (P < .001), with no loss in gains at 1-year follow-up for professional fulfilment (P = .202) and resiliency (P = .184), and further improvements in burnout (P = .016). Participants agreed that the program energized them in their work and that they would recommend the program to colleagues. Most were actively using the mental health skills in their professional and personal lives at 1-year follow-up. The CBT Skills Mental Health Physician Groups Program is effective at supporting physicians’ personal and professional well-being and mental health upskilling, with participants highly valuing the program.
Introduction
An estimated 80% of people rely on their Family Physician (FP) or other Primary Care Clinician (PCC) for their mental healthcare needs, yet recent research suggests that 41% of people with a mental health disorder feel their mental health needs are completely unmet or only partially met.1,2
A major contributor to this problem is the primary care crisis, making primary care increasingly inaccessible. 3 Up to 25% of Canadians are unattached to a PCC, and many struggle to access timely care.3-6 Burnout further compounds the problem by driving many to leave practice or narrow their scope of practice.7-13
Limited access to mental health support is further exacerbated by insufficient capacity, time, and expertise among family physicians caring for patients with mental health conditions.14-16 Research suggests that physicians who feel ill-equipped to support these patients experience greater distress and a desire for social/clinical distancing, reinforcing stigma.2,17,18 These challenges also contribute to moral injury and occupational stress, further increasing burnout.7-13
While many of these issues require system-level solutions,5,8,10-12,19 individual-level interventions that support physician resilience, well-being, and upskilling are also essential.11,12,14-20 Several evidence-based approaches show promise, such as interventions that teach mindfulness, stress management, and Cognitive Behavioural (CBT) skills,16,19,21-23 as well as group-based peer support interventions.19,20,24,25 The effectiveness of CBT in improving health-related quality of life across various mental and physical health conditions is well established, although it is not often a prominent component in physician wellness interventions.22,23
This article evaluates an 8-week virtual mental health skills group intervention accredited as Continuing Professional Development (CPD) and delivered to 698 physicians in British Columbia (BC) from 2022 to 2025, with the dual objectives of (1) providing skills that physicians can use in their practices to support patients experiencing mental health concerns and (2) supporting physician wellness.
About the Mental Health Skills Physician Groups
Background
Mind Space (Skills for Wellbeing) is a provincial nonprofit that enables physicians to provide group medical visits to patients with mild-to-moderate mental health conditions through BC’s publicly funded health system. Facilitators teach self-management skills derived from CBT, mindfulness, dialectical behaviour therapy, and acceptance and commitment therapy. 26
Mind Space programs have substantially increased access to treatment while maintaining effectiveness. Since 2015, over 18,000 patients have participated and over 440 groups are now offered annually. 26 Patients report comparable reductions in symptoms of depression and anxiety to individual CBT,27,28 and 89% of referring clinicians report the groups improve access to mental healthcare for their patients. 29
Development of the Physician Groups
The CBT Skills Mental Health Physician Groups were developed in response to requests from physicians whose patients had participated in the patient program. 30 These physicians sought greater familiarity with CBT concepts and terminology to strengthen their therapeutic knowledge and better support patients’ ongoing application of skills. As interest grew, content from the patient program was adapted into accredited physician-only groups. Although initially intended for family physicians, participation was expanded provincially to include specialists through a partnership between Mind Space and University of British Columbia’s Division of Continuing Professional Development (UBC CPD). A small group of nurse practitioners also participated in the groups. Sixty-four groups, each accommodating up to 15 physicians, were funded by the Shared Care Committee, a joint collaborative committee of the Doctors of BC and the BC Ministry of Health.
The physician program was initially designed to improve clinical skills in supporting patients with mental health conditions. However, feedback from early cohorts revealed a strong interest in addressing personal burnout and mental health symptoms as their primary aim. In response, facilitators shifted the focus towards personal reflection and application of skills in participants’ own lives while maintaining clinical skill development as a secondary benefit.
While this program shares several features with other physician wellness interventions available in Canada and internationally, such as an emphasis on peer support and resilience-building,31-33 this program’s uniqueness is its combination of collegial support with a more structured evidence-based skills building approach to simultaneously support physician well-being as well as capacity to care for patients with mental health concerns, by inviting physicians to learn these skills through personal application, rather than considering them only as a clinical tool.
Methods
The evaluation was undertaken as part of an ongoing Quality Improvement (QI) process,
34
employing a mixed methods approach with three main objectives: 1. assess changes in professional fulfilment, burnout, and resilience; 2. understand participants’ perceptions of program impacts and value; and 3. evaluate participant satisfaction.
Quantitative Wellness Measures
Professional fulfilment and burnout were measured using the 16-item Stanford Professional Fulfillment Index (SPFI).35,36 Items are rated on a 5-point scale from 0 to 4, with higher scores indicating greater professional fulfilment and burnout. Resilience was measured using the six-item Brief Resilience Scale (BRS). 37 Items are rated on a five-point scale (1 to 5), with higher scores indicating greater resilience. The BRS was added in August 2022, after recognizing that anecdotal resilience benefits were not being adequately captured.
Measures were administered at three time points: before taking the program, immediately after completion, and at 1-year follow-up. Surveys were linked across time points using unique identifiers. Paired t-tests with Bonferroni corrections (alpha = .025; 95% confidence level) were used to analyze changes in resilience, professional fulfilment, and burnout at pre- and post-program, and from post-program to 1-year follow-up.
Evaluation Survey
Participants also completed an anonymous evaluation survey immediately after the program, and at 1-year follow-up. Surveys assessed learning outcomes, perceived impacts, and satisfaction using Likert agreement and frequency of use scales.
Qualitative Feedback
To further understand participant experiences, 12 participants provided feedback through 4 focus groups and 2 individual interviews. Members of the evaluation team, who were not connected with the physician facilitators nor UBC CPD, organized and conducted the focus groups and interviews. Sessions were transcribed and coded for main themes.
Ethics Statement
The evaluation adhered to the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2). 38 Risk was assessed as minimal, based on a score of 2 on the A Project Ethics Community Consensus Initiative (ARECCI) Ethics Screening Tool. 39
Results
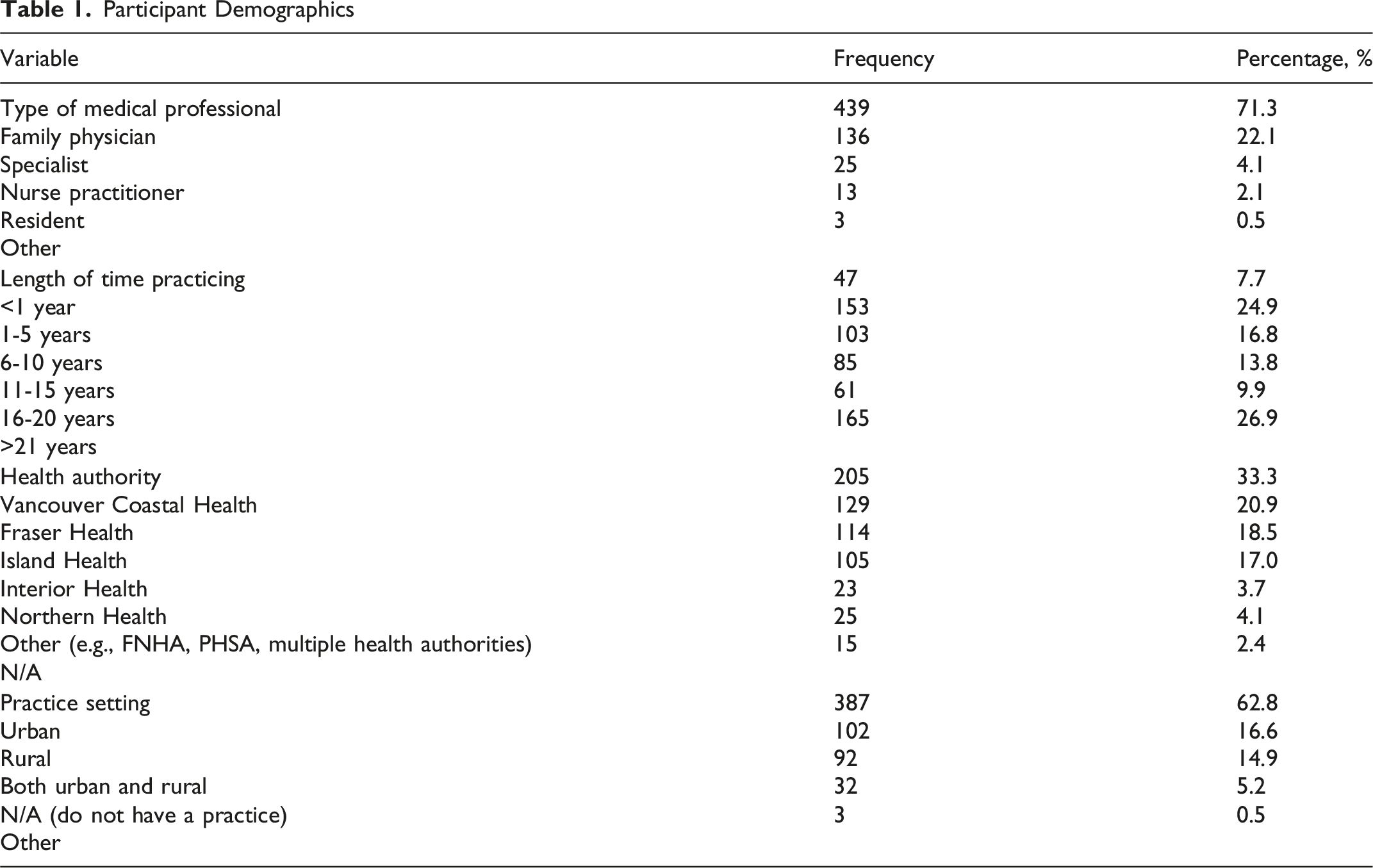
Participant Demographics
Quantitative Results: Wellness Outcomes
For the SPFI and BRS measures, 660 participants completed the pre-survey, 248 completed the post-survey, and 106 completed the 1-year follow-up survey. A total of 199 surveys could be matched for pre- to post-analyses, and 50 could be matched for post- to follow-up analyses. Scores were normally distributed.
As shown in Figure 1, participants demonstrated significant improvements in professional fulfilment (t (198) = −6.83, P < .001), burnout (t (198) = 6.39, P < .001), and resilience (t (144) = −4.13, P < .001) from pre- to post-program. Effect sizes ranged from small (resilience, Cohen’s d = .34) to moderate (professional fulfilment Cohen’s d = .48, burnout Cohen’s d = .45). Matched pre- to post-t-test analysis for professional fulfilment, burnout, and resiliency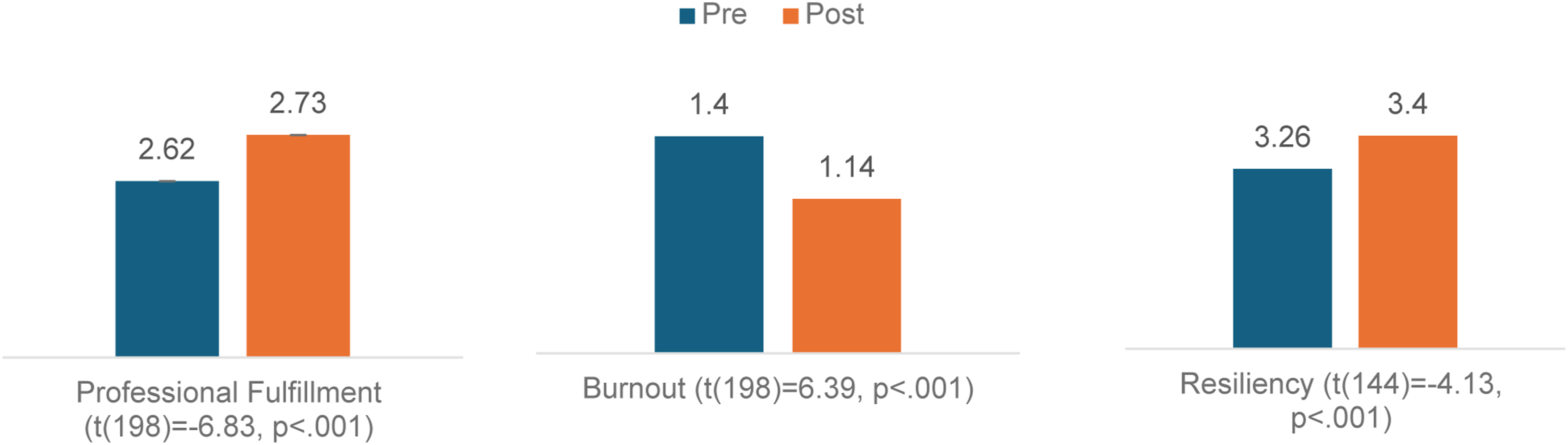
Improvements in professional fulfilment (t (49) = −1.29, P = .202) and resilience (t (30) = −1.36, P = .184) were retained between post-program and 1-year follow-up, while scores for burnout were further improved (t (49) = 2.51, P = .016, Cohen’s d = .35) over the same period.
Evaluation Survey Results
Post-Group Evaluation Survey Findings
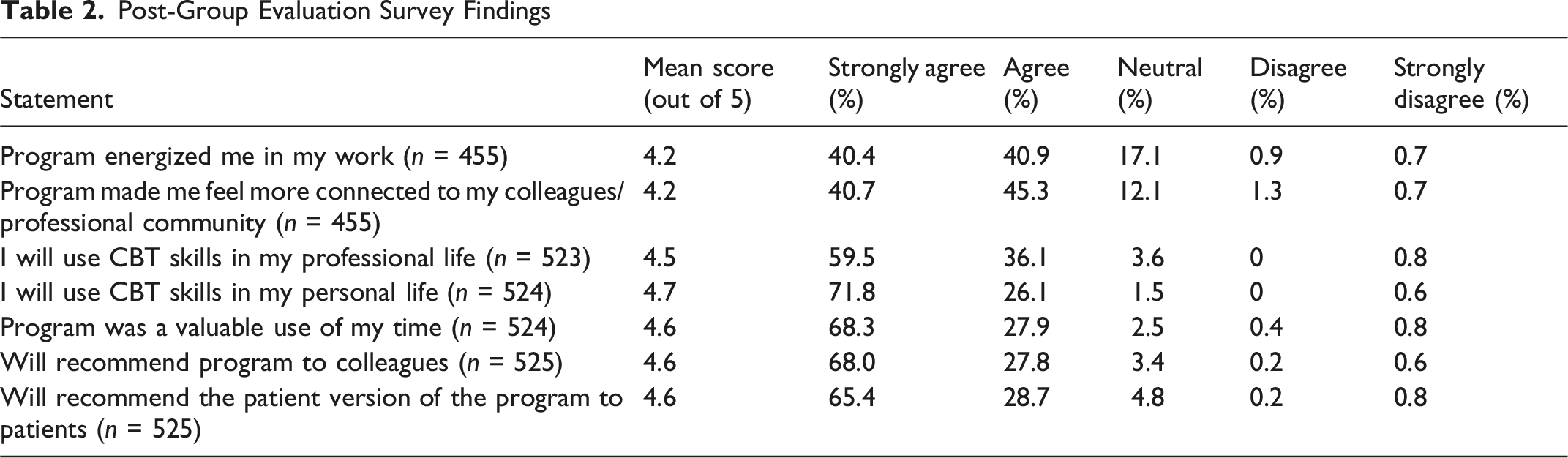
At 1-year follow-up (n = 118), 76.9% continued to feel that the program energized them in their work. Nearly all participants also reported continued use of the skills in both their personal (94.1%) and professional lives (91.5%). Participants who were not using the skills professionally typically indicated that they did not have an active clinical practice or did not have their own patients.
Qualitative Results
Qualitative feedback explored program strengths, impacts of the program, and recommendations for improvement.
In terms of program strengths, respondents consistently emphasized that the program reduced feelings of isolation and strengthened connections with colleagues. Peer support emerged as one of the program’s most valued components. “[The CBT Skills Group] filled a huge gap…I think people genuinely needed this group. Just even for peer support. Just having a safe space to show up and be present with colleagues who understood what they were going through or could empathize with them.”
Other commonly cited strengths included the quality of the content, skilled facilitation, and the accessibility of the online format. “The facilitator set the tone for the meetings, allowed excellent discussion between group members. Breaking up the knowledge content with practical exercises helped absorb and practice the material being taught. The program was delivered in a way that promotes spiral learning and ongoing engagement.”
In terms of program impacts, participants emphasized gaining practical tools to better regulate emotions, shift perspectives, and manage work stressors. “Before I took the course, I was sometimes having thoughts like ‘I don’t know how long I can do this job’. Now…I’m feeling more that I can see myself having a decades long career at my current job.”
Many also described improved confidence in recognizing and supporting mental health concerns among their patients. “I'm much more cognizant of seeing people and realizing, ‘Wait a second, this is more than, say, a depression. It’s more anxiety…’ I actually have more accuracy in diagnosis.”
Participants’ recommendation for improvement focused on the following: increasing awareness of the program, including clearer communication regarding its purpose and intended audience; offering greater flexibility in length, scheduling, and delivery format, including in-person options; and offering additional opportunities for applied learning and practice in translating skills to patient care.
Discussion
The CBT Skills Mental Health Physician Groups were initially developed as a professional development opportunity to strengthen physicians’ therapeutic skills and improve support for patients with mental health challenges. These benefits are demonstrated by the finding that most participants used the skills in their clinical work at 1 year follow-up. The program pivoted early on, to more directly address physicians’ own wellness, and the efficacy of this is reflected in the pre- to post-gains in resilience, burnout, and professional fulfilment, the further improvement for burnout scores at 1-year follow-up, and the retention of gains for professional fulfilment and resilience. Although the observed effect sizes were small to moderate, they are meaningful given the complexity and persistence of physician burnout and well-being challenges. Such interventions often produce modest effects, and even small improvements may be systemically important when achieved across many individuals and sustained over time.
In addition to direct benefits of participating in the physician groups, improvements in burnout from post-program to follow-up may have been influenced by broader changes in the practice environment. During the evaluation period, access to Mind Space patient programs expanded substantially, such that clinicians could refer patients to a publicly funded resource in which they could register in an average of 5 days, an accessibility not previously available in BC. More than 94% of physician wellness participants said they would recommend the patient version of the program to patients, suggesting they were likely to benefit from this resource. This also represents an innovation in team-based care, since patient groups are delivered by specially trained family physicians who are not embedded in the local care team but function as extensions of their colleagues’ therapeutic capacity. As such, these findings may support the premise that physician well-being is strengthened not only through individual skill development but also through improved access to collaborative mental health resources that reduce the burden of managing complex patient needs in isolation.
Practical Implications and Potential for Scale
Findings have implications for clinicians, healthcare teams, and organizations. For clinicians, the program demonstrates that mental health skills training, especially when personal and experiential, can simultaneously support personal well-being and strengthen confidence in caring for patients. The high rate of ongoing skill use at 1 year suggests they can be readily integrated into routine clinical practice while also supporting personal well-being.
For health teams, the findings highlight the value of creating structured opportunities to learn evidence-based mental health skills while building meaningful connections with colleagues, fostering a shared language around mental health, and strengthening team capacity to support patients. The group-based format is a particularly relevant ingredient in this context, as is the reduction in stigma by promoting mental health skills use for all. The psychological safety created by the program would be an important resource for teams experiencing ongoing demand and adversity.
At the organizational level, the findings suggest that physician wellness initiatives and workforce development efforts need not be pursued separately. Delivered virtually and accredited, the program reached nearly 700 physicians across British Columbia, demonstrating feasibility for broader implementation. The program easily could be incorporated into continuing professional development offerings—offered at cost or funded—onboarding initiatives for early-career clinicians, and/or physician wellness and retention strategies and programs, including by leveraging the existing Mind Space infrastructure and/or approach for scale and spread.27-30
Future research should examine implementation requirements, participation barriers, costs, and impacts on physician retention to better understand the program’s potential contribution to workforce sustainability and healthcare system performance. Future research should also examine how physicians are integrating the skills into their professional and personal lives and ways to further support ongoing skill use, such as refresher sessions or peer networks.
The intervention may be especially valuable when linked to existing mental health resources. In this evaluation, physician training occurred alongside expansion of the Mind Space patient group network, creating complementary pathways that enhanced physician capacity while improving access to mental health supports where they could refer patients. This model suggests healthcare organizations may achieve greater impact by integrating clinician skill development with accessible community-based mental health services.
Strengths and Limitations
This evaluation has several strengths, including a large provincial sample, the use of validated measures, a mixed methods design, and the inclusion of 1-year follow-up data. However, several limitations should be considered. The study lacked a control group, limiting the ability to attribute observed improvements solely to the intervention. Participation and survey completion were voluntary, introducing the potential for selection and response bias. In addition, substantial attrition at follow-up reduced the sample available for longitudinal analyses and may have affected the representativeness of the findings. Finally, outcomes were based on self-report measures and did not assess objective changes in clinical practice or patient outcomes.
Despite these limitations, the findings provide promising evidence that a structured, skills-based group intervention can simultaneously enhance physicians’ mental health knowledge, support clinical practice, and improve personal and professional well-being. The results suggest that clinician wellness and mental health capacity-building need not be separate objectives but may be mutually reinforcing. Programs that combine peer connection with practical mental health skills training may therefore represent a valuable addition to broader efforts to strengthen both the healthcare workforce and access to mental healthcare.
Conclusion
The CBT Skills Mental Health Physician Group program is effective at supporting physicians’ personal and professional well-being and mental health upskilling. Findings reinforce the principle that clinicians are better positioned to support healing in others when they are equipped with the knowledge, skills, and supports need to take care of their own well-being, and that training for this can be closely aligned with existing mental health skills programming and is best delivered in groups.
Footnotes
Acknowledgements
We would like to acknowledge UBC CPD and Lisa Demers for their dedicated efforts in support of this project. We would also like to acknowledge Kailee Hibbert and Corinne Henderson for helpful administrative assistance in preparing the manuscript.
Ethical Approval
Institutional review board approval was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this evaluation was provided by the Shared Care Committee, a joint collaboration of Doctors of BC and the Ministry of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.