
Abstract
Study Background
Nurses continue to migrate to Canada. Majority are visible minorities. Once employed, internationally educated nurses can struggle to integrate into their workplaces. A comprehensive understanding of factors that support internationally educated nurses’ workplace integration is lacking, limiting our ability to design appropriate policies and practices.
Purpose
The aim is to (1) examine internationally educated nurses’ perceptions of the extent to which they have integrated in their workplaces and the individual and contextual factors that supported their workplace integration, (2) explore whether internationally educated nurses’ perceptions differed by visible minority status, and (3) identify the key factors that predict internationally educated nurses’ workplace integration.
Methods
Cross-sectional survey of 1215 internationally educated nurses. All were immigrants, permanent residents, and employed as regulated nurses. Multiple linear regression was used to examine the influence of individual and contextual factors on perceived degree of workplace integration.
Results
Visible minority status had a large, statistically significant negative association with workplace integration (ß = −0.236, p < .001). Good relationships with coworkers (ß =0.043, p < .005), and continuing to develop nursing knowledge and skills (ß =0.178, p < .003), had statistically significant, positive associations with workplace integration.
Conclusions
Internationally educated nurses’ visible minority status can influence their workplaces. Providing education, managerial support, and mentorship fosters internationally educated nurses’ workplace integration.
Background and purpose
Internationally educated nurses (IENs) migrate to Canada from many countries worldwide (Covell et al., 2017), bringing with them significant amounts of nursing human capital, acquired through their education and previous professional work experience (Covell et al., 2015). However, IENs are a heterogeneous group, in that their level of education and type and amount of professional experience can vary dramatically. Some IENs quickly enter the profession and integrate into their workplaces, while others encounter obstacles and setbacks (Neiterman & Bourgeault, 2015).
As a major receiving country of internationally educated health professionals, Canada has created supports to assist IENs with overcoming the barriers to professional recertification and employment (Covell et al., 2018). Some of these supports, such as bridging programs, have been found to significantly influence IENs’ success on nursing licensing examinations and securing employment as regulated nurses (Covell et al., 2017, 2018); however, once employed IENs can continue to experience challenges (Primeau, 2014).
Upon entering their first jobs many IENs discover how nursing is practiced in Canada and how it differs from what they are accustomed (Murphy, 2008). It is during this time when IENs become aware of the need to continue to advance their nursing knowledge and skills, perfect their language and communication skills, while striving to develop a sense of belonging and comfort at work (Murphy, 2008). This process is referred to as workplace integration—the need to culturally “adapt, or change certain ways of thinking, speaking and acting in the workplace” (Holmes, 2012, p. 6).
Recognizing workplaces and the nursing practice can differ dramatically from what IENs expect, some Canadian stakeholders have put supports in place to assist employers with easing IEN’s integration into the workplace (Baumann et al., 2015; Ontario Hospital Association, 2015). At the organizational level, supports can vary from time-limited employer-sponsored orientation programs (Primeau et al., 2016), or larger system wide initiatives designed to facilitate IENs’ workplace integration, career development, and retention (Hamilton Health Sciences, 2019). However, due to funding constraints, these types of initiatives are sporadic or not readily available across all health-care sectors or Canadian jurisdictions.
Several qualitative studies have explored IENs’ experiences when trying to integrate into their workplaces (Babenko-Mould & Elliott, 2015; Lum et al., 2016). The findings from these studies identified individual factors and contextual barriers to IENs’ workplace integration.
The individual factors identified by IENs primarily focus on the need to improve their communication skills and gain an understanding of how nursing is practiced in the host country, which may differ from their country of origin. In particular, IENs find the nature and tone of interprofessional communication, the scope of nursing practice, and the autonomy afforded to Canadian nurses to be different from what they are used to (Covell et al., 2015; Neiterman & Bourgeault, 2013). IENs who are attached to traditional gender roles have deep-seated respect for older adults (Neiterman & Bourgeault, 2015) or are unprepared to act as patient advocates (Neiterman & Bourgeault, 2015) find they need to acquire additional knowledge to develop the required professional behaviors or practices. Even those who are native English or French speakers report difficulty understanding local expressions and unfamiliarity with the occupational-specific vocabulary used in the workplace (Cheung et al., 2013). Thus, perfecting their communication skills and learning about how nursing is practiced in the host country by continually advancing their nursing knowledge may help IENs integrate more smoothly into their workplace.
The contextual factors that act as barriers to workplace integration center around behaviors and practices IENs perceive as discriminatory or racist. These include IENs having limited opportunities to participate in professional development, being socially excluded or marginalized by their colleagues (Babenko-Mould & Elliott, 2015; Walani, 2015), and being subjected to racist behaviors or comments from patients and families (Baptiste, 2015). Despite having professionally recertified as regulated nurses, IENs often report feeling devalued in the workplace, in that they believe their previously acquired professional knowledge and skills go unacknowledged (Samali et al., 2017). IENs also believe racial discrimination plays a role in their inability to secure leadership positions (Ramji & Etowa, 2018) or advance their careers (Baptiste, 2015). When asked about their preferences for achieving career goals, the majority of IENs indicate that they have already met their goals of mentoring other nurses and being given more responsibility; however, they had yet to attain higher level positions (St-Pierre, Covell, Primeau, Ndengeyingoma, et al., 2015). Having good relationships with their coworkers support from their managers (Salma et al., 2012) and mentorship from other nurses have been identified as factors that can ease IENs’ workplace integration.
The reasons for IENs’ encountering racism and discrimination in the workplace are not fully understood. It is surmised that changes in demographic profile of IENs in Canada, in that higher proportion of IENs are migrating from low-income countries, have created an IEN population diverse in educational preparation, professional experience, language and communication skills, and race and cultural backgrounds (Covell et al., 2017). This diversity suggests that IENs are a heterogeneous group in that some IENs are job-ready upon hiring, while others require more time and support to adjust to how nursing is practiced in the host country. Consequently, many organizations across the country do not fully understand the unique needs of newcomers, especially those who are visible minorities, or how to help them integrate smoothly into their workplaces (Holmes, 2012). Understanding the type and amount of support required by IENs is integral for ensuring all IENs, regardless of their race, ethnicity and professional background have the opportunity to become valued members of their workgroups and are retained within the organization and the host country’s health-care system.
The Conceptual Framework of Support for IENs’ Workplace Integration was developed for this study (Figure 1). We conceptually defined workplace integration as IENs becoming members of a workgroup within a nursing organization where they can use their nursing knowledge and expertise (Covell et al., 2014, 2016) to fulfill their patient care responsibilities in collaboration with other health-care providers. The framework identifies key individual and contextual factors as supportive of IENs’ workplace integration. IENs’ workplace integration was conceptualized as being supported by the individual factors of communication competency and nursing knowledge and contextual factors of education, support, and mentorship in the workplace and positive work relations.
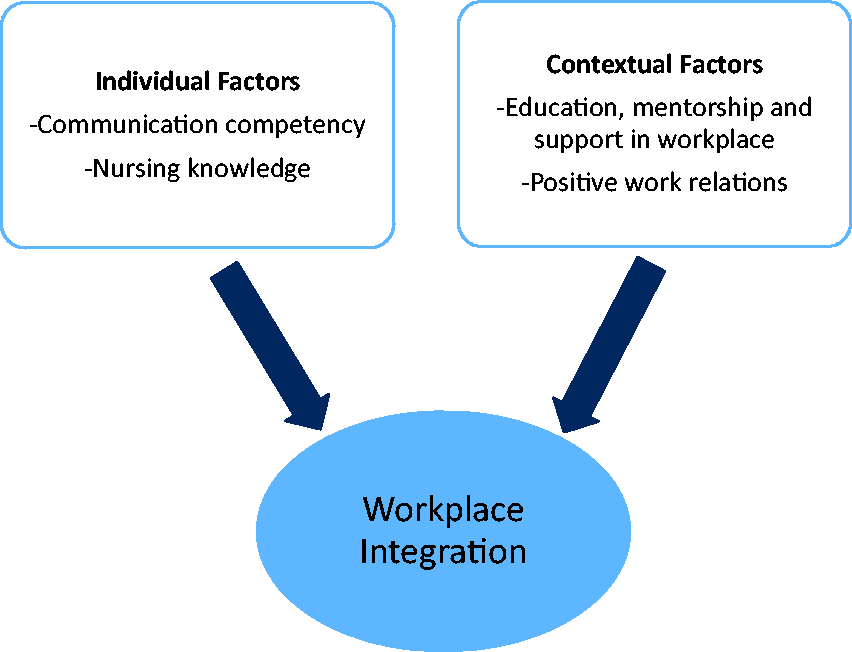
Conceptual framework of support for IEN workplace integration.
For this study, we operationalized the individual factors of workplace integration as communication competency, that is, perfecting communication skills and nursing knowledge as continuing to develop nursing knowledge and skills. The contextual factors were operationalized as factors that occur in the IENs’ workplace. They include (1) continuing professional education operationalized as participating in employer-sponsored orientation programs, (2) receiving mentorship from colleagues, (3) receiving support from managers and the staff union, and (4) positive work relationships with coworkers.
Our study aimed to (1) examine IENs’ perception of the extent to which they have integrated in their workplaces and the individual and contextual factors that supported their workplace integration, (2) explore whether IENs’ perceptions of workplace integration differed by visible minority status, and (3) identify key individual and contextual factors that predict IENs’ workplace integration.
Methods and procedures
The population targeted for this study was IENs and drawn from the large pan-Canadian cross-sectional study (St-Pierre, Covell, Primeau, Kilpatrick, et al., 2015). The survey was conducted between February and October 2014, following the procedures outlined in Dillman et al. (2014).
Nurses were eligible to participate whether they were permanent residents of Canada, received their basic nursing education abroad, held permanent licenses as a regulated nurse (registered nurse (RN), licensed practical nurse (LPN) or registered psychiatric nurse (RPN)), and were employed as nurses in Canada at the time of the study. IENs were identified through the nursing regulatory bodies within the provincial and territorial jurisdictions of Canada. Nineteen of the 24 approached regulatory bodies agreed to help identify IENs. A total of 2693 IENs responded to an anonymized online or mail survey with complete and usable data (St-Pierre, Covell, Primeau, Kilpatrick, et al., 2015). A subsample of all participants who immigrated in 2002 or after was targeted for this study. These respondents were chosen to create a sample of relatively recent arrivals to Canada and to reflect the implementation of the Canadian Immigration and Refugee Protection Act 2001 (Government of Canada, 2001) which provides additional supports to internationally educated health professionals.
A total of 1215 participants met the eligibility criteria for this study. The sample size was adequate to compare two groups of IENs defined by visible minority status (no or yes) and examine the influence of seven individual and contextual factors, measured by the Support for Workplace Integration questionnaire, on perceived degree of workplace integration (Cohen, 1992).
Variables under investigation were demographic characteristics, individual and contextual factors supportive of workplace integration, and IENs’ perceptions of integration into their workplaces. Demographic characteristics included age, gender, visible minority status, source country, year of immigration, language proficiency, regulated profession, level of nursing education at time of immigration, jurisdiction of employment, and years of professional experience in Canada. Age was reported in years. Gender was assessed as a dichotomy (1 = male, 2 = female). For visible minority, the participants were asked to identify whether they were members of a visible minority group using the categories included in the Canadian Census (Government of Canada, 2011). The visible minority category included participants who identified as Arab, Black, Chinese, Filipino, Japanese, Korean, Latin American, Mixed Race, South Asian, Southeast Asian, and West Asian. Nonvisible minorities included participants who identified as White.
Source country was assessed with an open-ended question where the participants identified the country where they completed their basic nursing education. Participants were asked to indicate the year they immigrated to Canada. Proficiency with an official language of Canada was measured with a Likert-type scale that asked respondents to indicate the level of experience with English or French language. The scale was anchored in 1 = no experience at all and ranged to 6 = first language and language of education. Level of nursing education at time of immigration was categorized as diploma, nonuniversity, or baccalaureate or higher. Regulated profession was represented with three categories: RN, LPN, and RPN, and participants indicated which permanent nursing license they held in Canada at the time of the survey. Categories for jurisdiction of employment reflected the 10 provinces and 3 territories of Canada. Participants were asked to indicate the number of years of professional experience prior to immigrating to Canada. Their responses were categorized into less than three years, three to five years, and greater than five years.
To provide an understanding of their workplace in Canada, respondents were asked to indicate the sector of employment (public or private), primary work setting (acute care hospital, nursing home/long-term care, public/community health, academia, clinic/physician office, private agency/duty, government/professional association, occupational health, or other), and primary area of responsibility (direct patient care, leadership, teaching, research, other). The Support for IENs’ Workplace Integration Questionnaire was used to assess IENs’ perceptions of the individual and contextual factors that supported their workplace integration. The questionnaire was developed, translated, and validated prior to its use in the pan-Canadian survey (St-Pierre, Covell, Primeau, Kilpatrick, et al., 2015). The questionnaire asked IENs to rate the extent to which workplace integration had been supported by the following individual factors: (1) continuing to develop nursing knowledge and skills and (2) perfecting communication skills and contextual factors: (3) participating in employer-sponsored orientation program for IENs, (4) receiving mentorship from colleagues, (5) receiving support from manager, (6) having good relationships with coworkers, and (7) receiving support from their union. The rating scale ranged from 0 = no support at all and ranged to 4 = very high amount of support.
The dependent variable was IENs’ perceived workplace integration. Participants were asked to indicate on a 10-point Likert-type scale anchored in 0, the degree they were integrated into their workplace.
Ethics approval to conduct the larger study was granted from l’universite du Quebec a Montreal (CER 167), University of Ottawa (J08-12-16B) and l’universite du Quebec en Outaouais (13–119-CERES-R). Return of a questionnaire implied consent.
Data were analyzed using SPSS version 25 (IBM SPSS Statistics for Windows, Armonk, NY, USA). Descriptive statistics were computed to describe the IENs’ demographic characteristics, degree of workplace integration, as well as IENs’ perception of the individual and contextual factors that supported their workplace integration (Aim 1). Since visible minority status could influence the type and amount of support IENs require to integrate into their workplaces, an independent sample t test was used to compare IENs’ responses to the individual and contextual factors reflected in the Support for IEN Workplace Integration Questionnaire for the two groups of IENs, those who were (1) not visible minorities and (2) visible minorities (Aim 2).
Linear multiple regression analysis was applied to examine the influence of the individual and contextual factors on the perceived degree of workplace integration (Aim 3). The Support for IEN Workplace Questionnaire asked participants to indicate whether they participated in an employer-sponsored orientation program. Only those who answered yes, were permitted to rate how supportive the contextual factor was for their workplace integration. We found that more than one-half of the participants did not participate in an employer-sponsored orientation program and could not rate the factor. To account for the influence of IEN’s visible minority status on their workplace integration, we dummy coded visible minority status (0 = no, 1= yes) and entered it first, followed by the individual and contextual factors reflected in the Support for IEN Workplace Integration Questionnaire. This sequence of entry was used to determine the best prediction of workplace integration above and beyond visible minority status. Multicolllinearity statistics were reviewed and showed no interrelations among the independent variables.
Results
Demographic characteristics of study sample
Table 1 summarizes the demographic characteristics of the study sample (N = 1215). The respondents’ ages ranged from 24 to 75 years (M= 41.05, standard deviation (SD) = 8.65), 80% (n = 967) were females and 60% (n = 803) were visible minorities. The median year of immigration was 2007. Majority originated from a developing country (65.5%) and had moderate-to-high proficiency in the English or French Language. Most respondents were RNs (84%, n = 1020). Alberta, Quebec, and Ontario were the primary jurisdictions of employment. On average, the respondents had greater than five years professional work experience. Majority worked in public sector (80.4%, n = 977) and in acute care hospitals or nursing homes (82.5%, n = 1002) providing direct patient care (88.6%, n = 1076). On average, the participants reported being well integrated into their workplaces (M = 8.28, SD = 1.93).
Study variables for sample (N = 1215).
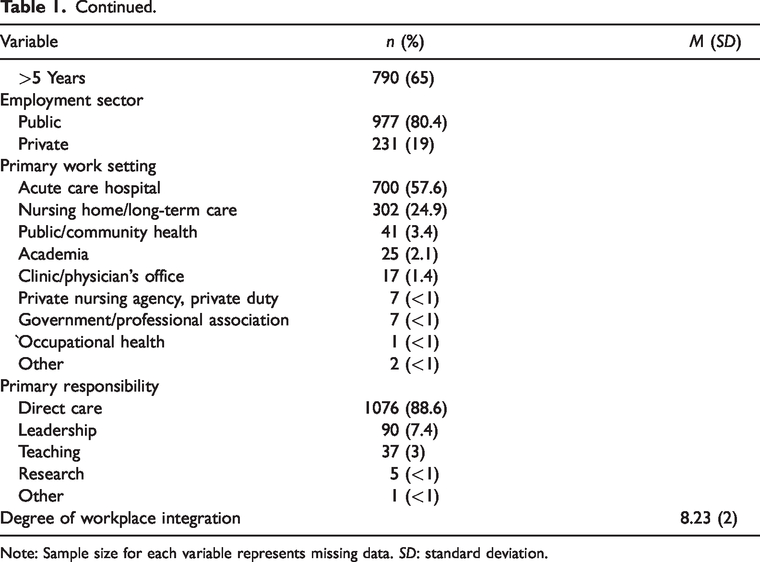
Note: Sample size for each variable represents missing data. SD: standard deviation.
Support for workplace integration
Table 2 summarizes the participants’ responses to the individual and contextual factors as reflected in the Support for IEN Workplace Integration Questionnaire. Overall, the participants rated most factors as moderately to highly supportive. The two factors IENs identified as most supportive for their workplace integration were as follows: continuing to develop their nursing knowledge and skills and having good relationships with their coworkers. They viewed receiving support from their union as the least supportive factor for facilitating their workplace integration.
Support for workplace integration questionnaire.
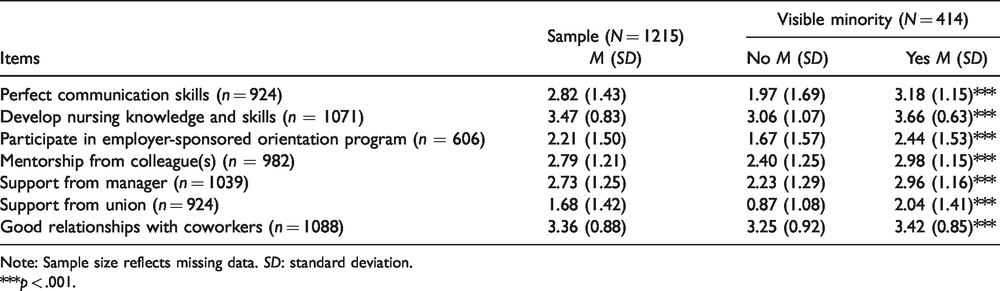
Note: Sample size reflects missing data. SD: standard deviation.
***p < .001.
Differences in the participants’ responses to the individual and contextual factors were noted between nonvisible minority and visible minority IENs. IENs who were visible minorities reported significantly higher ratings for all factors as opposed to IENs who were not visible minorities. Perceived degree of workplace integration also differed significantly between the two groups. Visible minority IENs indicated that they felt significantly less integrated into their workplaces when compared to nonvisible minority IENs (t = 4.49, p = <.001).
Predictors of workplace integration
Multiple regression analysis was used to determine the most significant predictors of workplace integration (Table 3). The overall regression model that includes IENs’ visible minority status and the individual and contextual factors was statistically significant. The adjusted R2 value indicates the model explained 11.2% of the variance of degree of workplace integration. Visible minority status, having good relationships with coworkers, and continuing to develop knowledge and skills predicted the extent to which IENs integrate into their workplaces. Visible minority had a large, negative association with integration (ß = −0.236, p < .001). Good relationships with coworkers (ß =0.043, p < .005), and continuing to develop nursing knowledge and skills (ß = 0.178, p < .003), had statistically significant, positive associations with integration.
Summary table for regression analysis for variables predicting degree of workplace integration (N = 412).
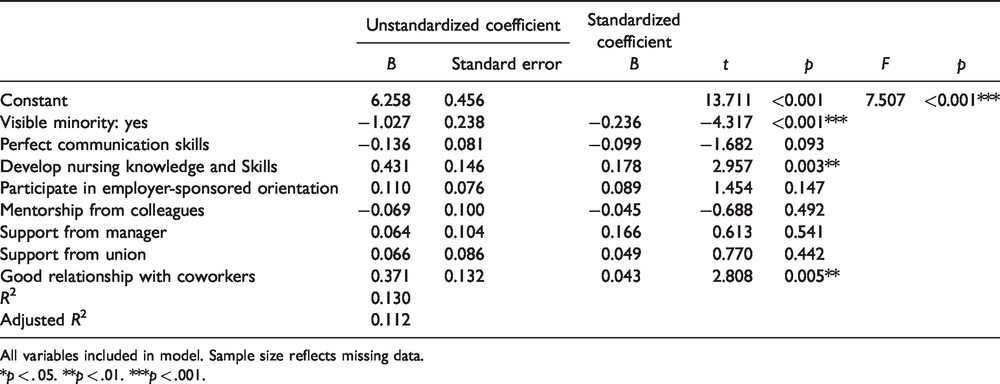
All variables included in model. Sample size reflects missing data.
*p < . 05. **p < .01. ***p < .001.
Discussion
Using data from a large pan-Canadian survey, this study examined IENs’ perceptions of the extent to which they have integrated in their workplaces and the individual and contextual factors that facilitated their workplace integration and whether IENs’ perceptions differed by visible minority status. Predictors of workplace integration were identified.
Our participants rated individual factors of perfecting communication skills and continuing to develop nursing knowledge and skills as moderately and highly supportive respectively, of their workplace integration. Recent evidence supports these findings, as strong communication skills are essential for establishing relationships with coworkers and patients, benefiting from managerial and continuing professional development opportunities (Alexis, 2013; Ramji & Etowa, 2018). To assist IENs with integrating into their workplaces, efforts should be made to help them improve their communication skills through employer-sponsored onsite individualized education and coaching. Special attention should be given by employers to ensuring IENs have the opportunity to advance their nursing knowledge and skills by having access to continuing professional development opportunities (Adeniran et al., 2015).
The contextual factor IENs identified as being most supportive of their workplace integration was having good relationships with coworkers. The other contextual factors, receiving mentorship from colleagues, and support from managers, were perceived as moderately supportive of IENs’ workplace integration. These findings are similar to those of Njie-Mokonya (2016) who found work environments where IENs feel a part of the nursing and patient care team, their contributions to patient care are valued, and they receive support from managers ease IENs’ workplace integration (Covell et al., 2015; Ramji & Etowa, 2018; Samali et al., 2017). For example, when colleagues and managers acknowledge IENs as having the necessary competencies to provide quality patient care, IENs feel a sense of belonging and acceptance. When IENs are able to use their full set of nursing competencies and have the opportunity to work in areas consistent with their previous work experience they are more likely to have positive relationships with their coworkers (St-Pierre, Covell, Primeau, Kilpatrick, et al., 2015).
Participants rated involvement in employer-sponsored orientation programs as moderately supportive. Offering extended employer-sponsored orientation programs for IENs, similar to those designed for new graduates, provides IENs with the necessary time to acquire the organizational specific knowledge and vocabulary used in the workplace as well as gain competencies and confidence needed to become productive members of their work groups within the destination country. However, despite employer-sponsored orientation programs being recommended (Chun Tie et al., 2019; Primeau, 2014; Squires, 2017), more than half of the IENs did not participate in one. This may be because these types of orientation programs are not widely offered in Canada (Covell et al., 2016). Instead, many IENs are required to participate in bridging programs as part of the professional recertification process. However, bridging programs are not designed to help IENs transition to their workplaces but rather to become familiar with the health-care system and update their competencies to meet local standards (Covell et al., 2018; Cruz et al., 2017). Consequently, an IEN’s first job as a regulated nurse can be their initial exposure to the Canadian work environment. As a result, most IENs require additional time and coaching in the workplace to become accepted and productive team members (Ramji & Etowa, 2018). Employers should be made aware that providing additional support to IENs beyond the initial orientation phase may help them integrate more smoothly, increase their job satisfaction and likelihood to stay (Sutton & Griffin, 2004).
The results of our study further reveal visible minority status predicts the extent to which IENs perceive they have integrated in to their workplaces and the amount and types of support required. While the prevalence of discrimination of IENs remains largely underexplored, reports of its occurrence are not unique to Canadian IENs. International evidence from Australia, United Kingdom, United States, and Spain suggests IENs who are visible minorities experience discrimination at work (Baptiste, 2015). For example, in an Australian study, Black, African IENs perceived repeated questioning about their knowledge and skills, and constant surveillance while caring for patients, as lack of acceptance by their colleagues and patients. These participants noted IENs who were Caucasian or from other visible minority groups, for example, Filipinos, were not subjected to the same degree of oversight (Mapedzahama et al., 2012). IENs employed in other destination countries report their race, accents or nationality contributes to discrimination in the form of unequal work assignments, limited opportunities for ongoing education or promotions, and being stigmatized, stereotyped, harassed by patients or bullied by their colleagues (Walani, 2015). IENs who are recipients of racism or discrimination experience more mental and physical abuse and report feeling unwelcomed and unappreciated (Walani, 2015).
Addressing perceived racism and discrimination is essential for ensuring IENs integrate smoothly into their workplaces. However, addressing perceived racism and discrimination may be challenging as they are often subtle and rarely overt (Baptiste, 2015). Thus, creating policies to address such behaviors may be insufficient without the commitment and active participation of the organizations’ leadership (Rosenkoetter et al., 2017). Leadership can help mitigate racism and discrimination by ensuring all health-care staff receive education about racism and discrimination including its effects on the recipients, patients, and the organization (Baptiste, 2015). Additionally, providing ongoing support through regular check-ins with IENs to address challenges and concerns and offering assistance with conflict resolution and stress management are strategies the organizations’ leadership may find useful (Lin, 2014).
Another strategy to support IENs’ workplace integration and prevent perceived racism and discrimination is for employers and coworkers to value IENs’ multicultural and linguistic backgrounds. While communication competency and proficiency in the language used in the workplace are essential for ensuring safety and quality of care, IENs’ fluency in other languages and understanding of cultures can be valuable when providing care to multicultural patient populations. For example, when IENs communicate effectively with patients and families with similar linguistic and ethnic backgrounds, they can improve patients’ care experiences (Njie-Mokonya, 2016). In addition, when IENs work with colleagues of similar ethnic and linguistic backgrounds, they report feeling accepted, understood, and supported in their workplaces (Ramji & Etowa, 2018). Thus, a key strategy for facilitating IENs’ workplace integration is for employers to promote racial and ethnic diversity of the nursing staff and the organization’s leadership. This can be accomplished by leadership encouraging the hiring, mentoring, and promoting of IENs, especially those who are visible minorities (Jefferies et al., 2018).
Strengths and limitations
Strengths include the large scope of the study and the use of a newly developed questionnaire that identifies key elements known to facilitate IENs’ workplace integration. Limitations include a possible sample selection bias since we approached only IENs who agreed to be contacted for research purposes, which may have influenced their responses the survey. In addition, all of the study participants were permanent residents at the time of the study, thus limiting our ability to assess the perceptions of IENs who were in Canada on temporary work visas.
Conclusions
Workplace integration is a reciprocal relationship between the IEN and their employer, with each having specific obligations to fulfill. A collegial work environment characterized by openness and fairness engenders feelings of acceptance and belonging; which can be accomplished by valuing IENs’ unique contributions to patient care. IENs who are visible minorities may need more time and assistance during the integration period, and therefore, organizations and managers must commit to providing IENs with the necessary support through extended orientation and mentorship programs, and equal or greater access to continuing education and career advancement opportunities. Facilitating the integration of IENs not only benefits IENs but also patients and their families, the organization, and wider community.
Footnotes
Acknowledgments
The authors acknowledge the contributions of the research team who collected the primary data used in this study, Isabelle St-Pierre, PhD, RN, Christine L. Covell PhD, RN, Kelley Kilpatrick, PhD, RN, Marie-Douce Primeau, PhD, Assumpta Ndengeyingoma, PhD, RN, and Eric Tchaouaket, PhD.
Authors’ Contributions
Both authors made substantial contributions to the conception and design, analysis, and interpretation of data. Both authors provided critically important intellectual content and gave approval for the version under review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Internationally Educated Health Professionals Initiative at Health Canada. The funding agency had no role in the study design, data collection, analysis, or interpretation of results, or writing the manuscript.