
Abstract
Aim
To examine the experiences, motivations, and perceived inequities of internationally educated nurses (IENs) residing in northern British Columbia and to identify systemic, geographic, and regulatory barriers to workforce integration.
Background
Although IENs are critical to Canada's health workforce, many face prolonged licensure processes and limited access to education and employment, particularly in rural and remote communities.
Design
Guided by Equity Theory and organizational perspectives, this mixed-methods study explored how perceived inequities influence motivation, engagement, and workforce participation.
Methods
Data were collected through three focus groups and interviews (n = 13), an online survey (n = 79), and a key partner workshop with regulators, assessors, educators, a union and health system partners (n = 16).
Results
Four themes emerged: resourcefulness, rural life, mental health and identity, and challenges within the registration process. Participants demonstrated resilience and strong professional commitment but reported delays, financial strain, and limited access to local training and navigational support. Survey findings echoed these barriers. The key partner workshop translated findings into partnership-based strategies to improve educational access, regulatory collaboration, and rural workforce pathways.
Conclusion
Effective IEN integration requires coordinated, equity-oriented partnerships across regulators, educators, and employers. Strengthening these collaborations can improve licensure access, support retention, and enhance healthcare capacity in underserved regions.
Keywords
Background & Purpose
Nurses constitute approximately half the global healthcare workforce (WHO, 2024). Internationally educated nurses (IENs) are an integral part of this workforce, playing a crucial role in addressing healthcare human resource needs across many countries (Ahmed & Bourgeault, 2022). Movement of nurses between countries is not a new phenomenon and is accelerating (Cubelo et al., 2024). The distribution of IENs varies by country with high-income countries relying on IENs for up to 23% of their workforce (WHO, 2025). According to the State of the World's Nursing Report (WHO, 2025), globally approximately 15% of working nurses are internationally educated, indicating ongoing mobility and migration trends.
Migration is driven by diverse factors including improved working conditions and financial incentives (Pressley et al., 2024; WHO, 2025), as well as broader economic, social, educational, and career advancement opportunities (Covell et al., 2017; Roth et al., 2021). However, IENs encounter multiple challenges including insufficient professional recognition, regulatory barriers, prolonged assessment timelines (Chiu, Thiessen, et al., 2025; Cubelo et al., 2024; British Columbia College Nurses and Midwives [BCCNM], 2022), and obstacles to social integration and acculturation (Foo & Goh, 2024; Smythe & Laing, 2026). The transferability of specialty training remains constrained due to the absence of policies or guiding frameworks (Kurup et al., 2024) and consistent assessment practices (Shaffer et al., 2016), while access to affordable supplementary training opportunities is restricted (Flecker, 2025). At the systems level, the migration of IENs from low-income to high-income countries impacts health systems in both source and destination countries, resulting in economic strain. Due to ongoing vacancies and rapid staff turnover, high levels of IEN support are required to facilitate adaptation to new environments and compliance with regulatory standards (Crea-Arsenio et al., 2023).
Globally the nursing workforce faces significant challenges including widespread shortages, maldistribution, and high rates of attrition (WHO, 2025). Despite an annual global growth rate of 2.7%, the nursing shortage is expected to reach 4.1 million by 2030, with Canada predicted to experience a decline in nursing numbers of 2.5% or greater (WHO, 2025). The perception of Canada as a single, unified entity often leads to misunderstandings about how nursing regulation and practice function across the country. Canada's healthcare system is decentralized with nursing regulation governed at the provincial and territorial level, not federally. Each province or territory has its own nursing regulatory body with varying licensure requirements and ongoing reforms. Chiu, Alostaz, et al. (2025) note these changes, which, when implemented quickly, require continued evaluation to assess their impact on healthcare and identify scalable, equitable solutions. While regulators are central to ensuring patient safety, workforce sustainability, and system responsiveness, there is growing scrutiny about their mechanisms for partner collaboration and the degree to which their policies and practices are informed by evidence (Chiu, Thiessen, et al., 2025).
Similar to other high-income countries, IENs play an increasingly critical role in the Canadian healthcare system by helping to address workforce shortages and support long-term sustainability (Baumann et al., 2024; Health Canada, 2024). However, estimates of the size of the IEN workforce vary substantially across data sources and jurisdictions. Using census data, Frank et al. (2023) report that only 34% of employed IENs were working as registered nurses (RNs), whereas Alostaz et al. (2025) found that up to 41% of new nursing registrants in Ontario were internationally educated. These discrepancies suggest that a significant portion of the potential nursing workforce remains underutilized, largely due to barriers related to licensure and limited access to reentry or bridging programs. Accurately determining the number of practicing IENs is further complicated by the fact that new registrant data may not include workforce counts or demographic breakdowns. Many IENs initially obtain licensure in jurisdictions with fewer regulatory barriers and subsequently relocate to other provinces, a phenomenon described as “province-hopping” (Chiu, Alostaz, et al., 2025) or “jurisdiction shopping”, whereby licensure is obtained in a province in which the nurse does not intend to practice. Recent regulatory reports indicate that this pattern of labor mobility can pose risks and, in some cases, result in serious harm (College of Registered Nurses of Manitoba, 2025). In response to these challenges, the independent organization Health Workforce Canada seeks to bring together workforce experts, policymakers, researchers, patients, and caregivers by facilitating data sharing to support the development of innovative, nationally coordinated workforce solutions (Health Workforce Canada, 2025).
Domestic Internationally Educated Nurses
International recruitment is commonly prioritized to address nursing shortages, while domestic IENs, those already residing in Canada, are frequently overlooked (Ahmed & Bourgeault, 2022), particularly in rural and remote regions such as northern British Columbia (BC). Many domestic IENs remain underemployed or excluded from the nursing profession due to the need to travel for assessment, supplementary education or clinical site access, or regulatory barriers (Canadian Federation of Nurses Unions [CFNU], 2025). Furthermore, relationships between regulators, educators, and employers can either constrain or enable these IEN opportunities (WHO, 2025).
In this study the term IEN refers specifically to “domestic” IENs: internationally educated individuals who already reside in northern BC and seek licensure or employment within the BC workforce. Despite their clear workforce potential, little empirical research has examined how these IENs experience licensure and integration, or how cross-sector partnerships might reduce these barriers. Without coordinated solutions, skilled nurses remain underemployed while communities continue to face persistent shortages.
To examine inequities systematically noted in the IEN literature (Bayuo et al., 2023; Cubelo et al., 2024), we drew on Equity Theory (Adams, 1963). This proposes that individuals evaluate fairness by comparing their inputs (time, skills, effort, financial investment, credentials checking) with outcomes (recognition, employment, and career opportunity). When perceived inequities persist, motivation, engagement, and retention decline. Applied to IEN integration, prolonged licensure processes and underemployment may create perceived inequities that discourage workforce participation. This framework provided a lens for understanding IEN experiences and guided the study's design and partnership-based approach, asking:
What are the lived experiences of IENs as they navigate licensure and workforce integration? How can regulators, educators, and health system partners collaboratively reduce systemic barriers and improve equitable access to nursing careers?
To address these questions, and prior to undertaking this study, we partnered with the local regional health authority to conduct an environmental scan to identify IENs facing barriers to workforce re-entry. The findings from the environmental scan were presented at the 2022 Canadian Association of Nursing Schools conference. This preliminary work informed the development of this mixed-methods study examining IENs’ experiences, motivations, and perceived inequities across the licensure process. Ethical approval for this study was obtained from RISe (REB H23-00845). Participation was voluntary with all participants receiving information about the study, their right to withdraw, consent form, and available additional supports for IENs.
Methods and Procedures
General Design and Frameworks
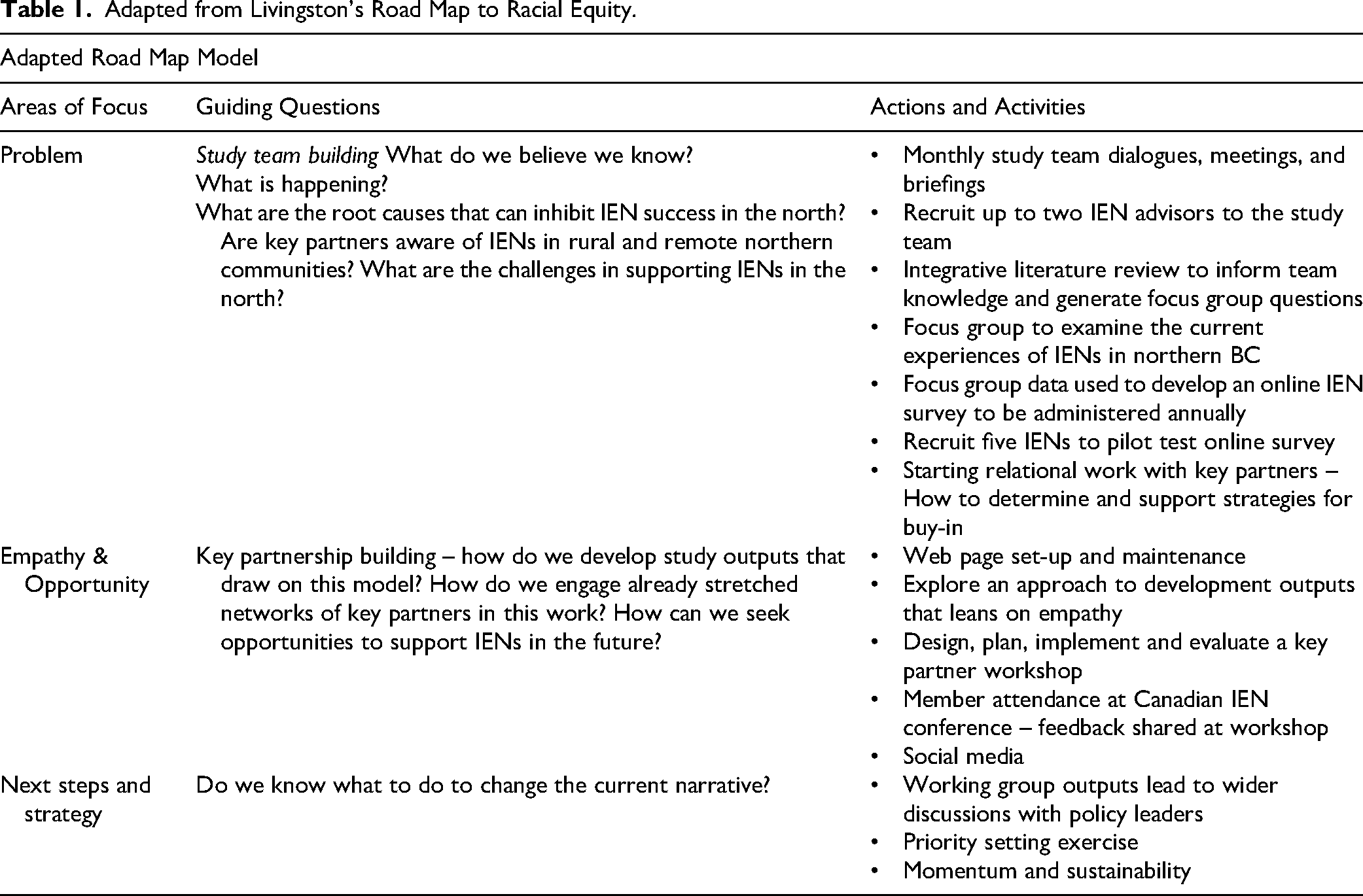
The study applied both the equity theory framework (Adams, 1963; Davlembayeva & Alamanos, 2025) and utilized Lee and Wojtiuk's (2021) commentary and Livingston's (2020) “Road Map for Racial Equity”, to facilitate problem identification, empathy-building, and strategic action to address systemic barriers. Adam's equity theory and Livingston's road map are aligned in their shared concern with fairness and inequity, but they operated at different levels within this study. Equity theory served as the analytical lens for examining how IENs interpreted inequities in their licensure and workforce integration experiences, whereas Livingston's framework informed the methodological approach to key partner engagement by structuring processes of problem identification, empathy-building, and collaborative action. Our methodological approach was three phased with an emphasis on relationship building, equity, and authentic organizational commitment to support inclusion and diversity as it gathered the perspectives of IENs (Table 1).
Adapted from Livingston's Road Map to Racial Equity.
Phase 1 – Literature Review and Focus Groups
An integrated review of IEN literature, based on principles outlined by Toronto (2020), was undertaken to inform the research team's knowledge. Using the outcomes from this literature review, combined with Krueger's (2013) structures for guiding interviews, focus group questions were developed (see supplementary information). These questions were then reviewed by the wider study team and pilot-tested by two IEN advisors to the study team.
Using the findings from our earlier environmental scan, IENs who had indicated interest were invited to participate in focus groups: They had to be fluent in English and could be at any stage in their IEN credentialing, assessment, or education process. Potential participants were randomly assigned to five clusters (A-E) of 15 individuals using an online randomization generator. The health authority was not involved in the recruitment process and remained unaware of which IENs participated. To engage IENs not affiliated with the health authority, the health authority communications team contacted 23 communities using an existing social media platform and ran a 20-day advertisement. Twenty IENs expressed interest in the study; 13 participated, with seven reporting scheduling conflicts or later declining. The participating IENs had completed their primary nurse education in the Philippines, India, Africa, the United Kingdom, and the United States. Three focus groups (60–90 min each) were held and six individual videoconferencing or telephone interviews conducted by two team members (CS, TM) between November and December 2023.
Field notes were kept by the two researchers to check accuracy and discuss the focus groups and interviews post-transcription. No participant requested to review the transcripts. Thematic analysis was used to analyze and theme the data (Willig et al., 2017). Consistent with our equity-oriented design, analytic procedures were intentionally structured to center IEN voices. To reduce potential bias, three team members - a Canadian-trained nurse (TM), an international nurse (CS), and an English major (DH) - conducted data interpretation following a structured process of keyword and supportive quotation selection, coding, theming, and interpretation (Naeem et al., 2023). This inductive approach was complemented by a deductive process, which explored themes aligned with equity and motivation.
Phase 2 – Online Survey
Drawing on insights from our environmental scan, literature review, and focus group analysis (Nassar-McMillan & Borders, 2002), an online survey was developed that examined how perceived inequities affected motivation, social comparison, and professional integration among IENs as they undertook the process to transition to RNs. Survey pilot testing was conducted by team members (MF, CC, TM) and five self-selected IENs from the focus groups. Feedback-informed refinements. The final ten-minute survey comprised sixteen demographic questions, followed by self-selection into one of four categories: 1) not started the IEN process, 2) post-credential assessment, 3) currently undertaking required education, or 4) practicing as a registered RN, with specific questions for each category. The survey continues to operate on an open-ended cycle, with data from only the first 12-month period being included in this paper. Descriptive statistics were used to summarize responses to closed-ended questions.
Phase 3 – Key Partner Workshop
Throughout the study, meetings were held with key partners including the BC nurse regulator, IEN competency assessor provider, nurses’ union, senior health authority leadership, northern educational partners, and the university's office for international and continuing studies. These meetings focused on information exchange, supplementing immigration knowledge, access to learning opportunities, and culminated in a key partner northern IEN workshop.
Informed by our underlying positioning of equity and motivation, we developed knowledge translation products e.g., stories, poems, and artwork, to foster empathy, curiosity, and collaboration with our partners during a key partner workshop. IEN stories were created and set against nonproprietary northern images collated by our study team. These stories were narrated by a range of IENs from various countries and then printed into a paperback collection for distribution and use at the workshop. One member of the study team (DH), with a background in poetry, worked with the data to generate a series of poems, whereby each line was a direct quote from a participant. To complement this, a local young Indigenous art student created a pastel drawing to visually represent one of the poems.
Sixteen key partners including the British Columbia College of Nurses and Midwives (BCCNM) (nursing regulator); a BC nurses’ union; partners delivering the Inspire Global Assessment, which is the mandatory competency check that measures nursing competencies on behalf of the regulator; post-secondary education sectors from across the north; and health authority leadership attended the two-day Northern Workshop in May 2024. The workshop was developed using Pip Decks Workshop Tactics (Burdett, 2021) and Liberating Structures resources (Lipmanonwicz & McCandless, 2013) and included a mixture of focused activities and smaller group work with real time feedback captured using Mentimeter (n.d.).
Although regulators, educators, and employers participated in the workshop as knowledge partners, they were not included as primary research participants. This decision was intentional and consistent with our equity-oriented design: The study prioritized centering the voices of IENs whose experiences are often underrepresented in workforce planning and policy discussions.
Data Analysis and Credibility
Throughout the phases of data collection and analysis, the research team met regularly to discuss, challenge, and share emerging findings. Reliability was supported through follow-up sessions with the two study IEN advisors to enhance the credibility of the findings. An embedded audit approach was used; whereby quality assurance practices were incorporated into the analysis to critically review and refine decision-making and thematic representations. This collaborative process extended throughout the study into all knowledge translation activities, including website development, the arts-based outputs, workshop facilitation, and engagement tools.
Results
The results are divided into three sections: focus group analysis, survey results, and key partner workshop.
Focus Groups
Four key themes were identified from the focus groups: resourcefulness, rural life, mental health and wellbeing, and the technical process and workplace transitions. Guided by our equity framework, analysis prioritized how systemic and regulatory inequities shaped participants’ motivation, wellbeing, and decisions to persist in or leave the nursing workforce. Emphasis was placed on centering IEN voices and interpreting challenges as structural rather than individual deficits; accordingly, participant quotations are foregrounded throughout to reflect lived experience and counter the historical underrepresentation of IEN perspectives.
Resourcefulness
IENs were motivated to prove themselves as valuable contributors to the Canadian workforce and economy. Once in Canada, IENs had to tap into their adaptability to learn about registration, as well as a new environment, different technology, foreign medical terminology, and an unfamiliar culture. As Participant B shared, this required planning: “[being] fairly fresh out of nursing school. You’re motivated. You’re ready to get into practice. I just dove right in which, partly, was my mistake. I should have kind of figured out and had a game plan prior to, but I wasn’t anticipating it to be this hard.”
When faced with challenges they responded with patience, hard work, and a deep commitment. Many IENs brought humor to their situation, making light of confusing linguistic and cultural differences. Participant K: “somebody asked me to go into the store and get them a pop. And I looked…. I came back out and I’m sorry, like there's no pop in this convenience store. And I got just a strange look of bewilderment. It turns out they were asking for a soda…. it's the funniest thing”.
IENs shared a willingness (and often a desire) to pursue further education to achieve their dream of becoming an RN, as well as for personal and professional advancement. With limited post-secondary re-entry programs in BC, “two or three programs,” long distances to travel and prerequisites that some IENs “couldn’t qualify for” or “long waiting list[s],” the process of pursuing further education was incredibly challenging and burdensome. “[I] couldn’t figure out how I would be able to afford moving …I kind of lost motivation” (Participant B).
Resourcefulness was critical as IENs were in a constant state of communication and outreach – sending emails, making phone calls, and online searching – particularly when information sources were sparse or conflicting. When IENs were successful in gaining licensure, this did not always mean getting hired: “there's nothing, because the competition is very stiff. It's very competitive. But if you want to go up north, we have jobs for you” (Participant J). Sharing how moving north was what helped them stay connected to nursing and build confidence, as people were “really very nice” and they “wanted me to work with them.” For support and connection to their culture and language, IENs relied on their families, friends, and their IEN community. In times of need, friendships and mentorships became vital sources of hope and determination.
Rural Life
Following the immigration process, IENs had to adjust to new geographical, social, and cultural experiences. For some IENs, the north was celebrated for its small-town camaraderie, close-knit atmosphere, and its multiculturalism. Participant B described: “it was actually nice to have [that] kind of the rural small-town living.” Starting clinical work in rural places was also celebrated, “if you start in a rural area, you have more opportunities to learn” (Participant A).
However, small town experiences could also be exclusionary or discriminatory, and attitudes towards immigration could be threatening and harsh. Assimilationist attitudes were, in some cases, subtle but inarguably present. Participant K: “because I speak English and I’m white, I think that it's very easy for me to pass as a Canadian…. So, I think I’m super lucky in that aspect…. [but] I didn’t get any orientation to like the town or anything. I never even laid eyes on it until I signed a lease”.
Rural places also brought a set of new experiences for IENs that were unexpected, such as harsh weather conditions, different social/gendered roles, and new cultural/professional protocols. There was an expressed need for additional supports, given that “with [learning about] the culture it's up to us [to learn] and we need some help” (Participant E). Challenges with English as a second language remained, since their accent was “heavy,” but they could read, speak, and write well (Participant F). Even when working as a licensed practical nurse wanting to return to work as an RN this could be a barrier, despite “managers writing to the regulator that speaking is not a problem; is already working in the hospital” (Participant F).
All IENs expressed a deep interest in learning about Canada's cultural and colonial history, eager to integrate into their new communities. Many were drawn to rural settings for their natural beauty and sense of belonging. Participant C shared, “I really want the strong sense of community in a small rural place… I know there is diversity… but I’m motivated to stay here in [rural town]. I like being connected to the natural environment. It's beautiful here”. This sentiment was echoed in participants’ desire to contribute meaningfully to their communities by alleviating healthcare system pressures. Emotional accounts highlighted the urgency and frustration surrounding delayed registration processes. Participant Y: “It's really painful… we went to the emergency… you have to wait for many, many hours… so many residents in need of care… I want to use my nursing skills, but registration is slow or impossible”.
Mental Health and Self-Identity
Being a nurse was a central part of IENs’ identities, as exemplified by the philosophy “once a nurse, always a nurse” (Participant X). The difficulty of being denied an opportunity to quickly return to the workforce impacted on their self-worth and value. Participant X shared how they felt this disconnect as “a deep pain because being [an] RN is part of my identity, part of why I came to Canada and it's been taken away from me, right before my eyes.”
The process of achieving registration was associated with mental exhaustion, strain and confusion: “I got my licence in two years, but with conditions, which is different than the other province where I could work” (Participant H). This also translated to teaching in post-secondary with stories about friends and colleagues with a nursing background or PhD teaching but “people are saying that because you don’t have your licence, you can’t even do theory courses. But one of my friends who has done a PhD, they don’t have licence, and they are teaching in nursing programs” (Participant H).
The emotional aspect of being stuck was the one unforgivable aspect of the process: financial recovery is possible, but “the confidence and self-esteem, that damage is done” (Participant X).
Technical Process and Transition to the Workplace
The actual, technical process of becoming registered in BC was felt to be misaligned for some, while others were more prepared: “I knew about the process when I was still in [home location]…my friends are telling me lots and some of my friends who came first tell me it will be a long process” (Participant C).
Frustration was expressed at the seemingly randomized success rate to become an RN in BC, suggesting that IENs are “willing to do the hoops, but the hoops have to be standardized” (Participant A). Participants lamented about how long processes can take: “my story is so long…. Maybe I [will be] transitioning to retirement [before] its finished” (Participant J).
There was discrepancy between their formal education and the actual application of this education in the workplace with several IENs sharing that the reality of practice was unlike the competencies taught in their primary education: “whole different scenario in the hospital” (Participant A). Even when IENs were proactive in connecting with local colleges and universities to access education they were told: “there is nothing for me…I wanted more…I wanted a program to integrate me…I learn better on the job in practice” (Participant D). They described having to travel but “unfortunately the [program] didn’t do much to prepare me for like real-life Canadian nursing.” Transition to consolidate learning was helped by the post-program employer team who provided good preceptorship and accessible clinical nurse educators.
IENs acknowledged there was much to learn particularly associated to nuances in language with medications or values: “blood sugars. Oh my God. Like 3 to 8, you’re doing great, but like in the States it's 90 to 120…this guy comes to ED and he's like my blood sugar is 21 and I was like… he could die. It turns out it was totally the opposite” (Participant K).
Despite funding options, financial stress remained due to fees and the inability to fully work, causing a burden to IENs and their families. These concerns prevented some experienced nurses from pursuing registration. “I haven’t started…I’m reconsidering due to my age—I’m 50, should I still try?” (Participant E). Many IENs acknowledged financial stress, lengthy registration processes, and limited local assessment or education options, making it challenging to almost impossible to return to nursing.
Survey
Seventy-nine IENs completed the survey. Half were aged 30–39 years (50%) and the majority identified as female (86%). Participants most commonly identified as Asian (45%) or Latino/Hispanic (24%). Over one quarter resided in northern British Columbia (26%), while most lived elsewhere in the province (58%). Most respondents held a bachelor's degree or higher (82%) (Table 2).
Demographic Characteristics of Survey Participants (N = 79).
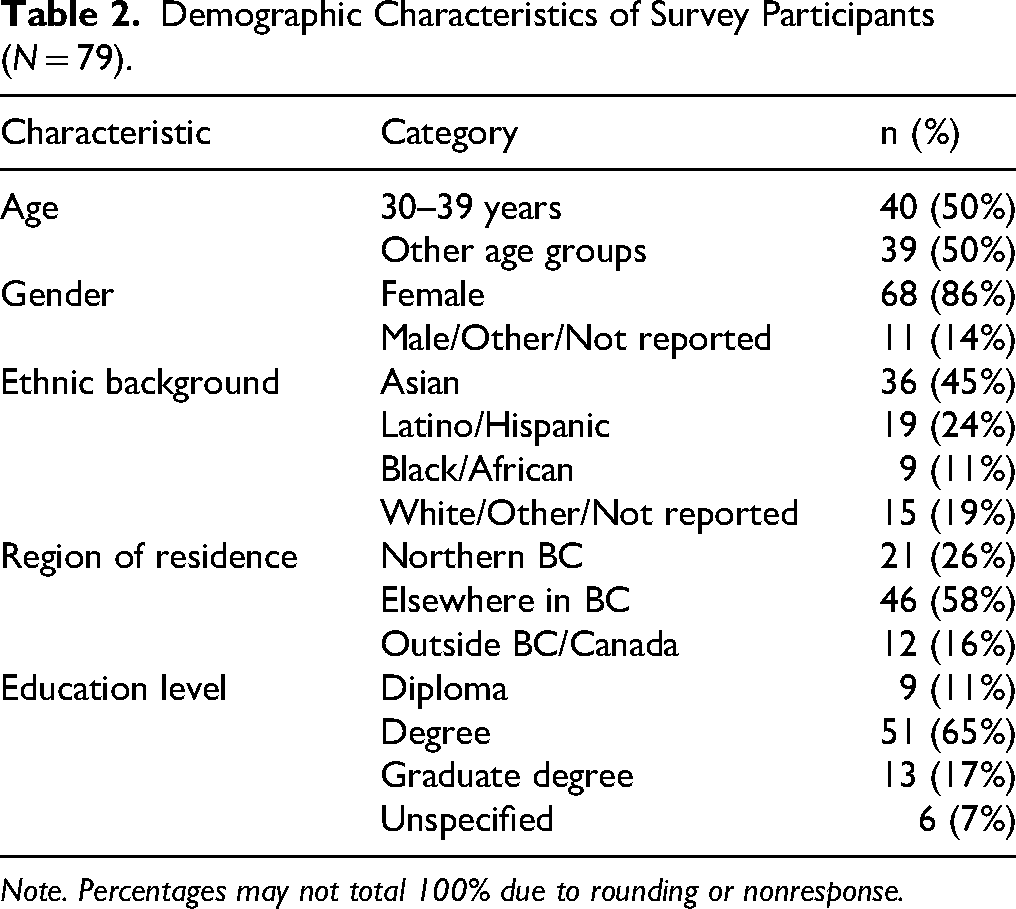
Note. Percentages may not total 100% due to rounding or nonresponse.
The survey data supported, confirmed, and reinforced the findings from the focus groups with 68% of survey participants identifying credentialing delays as the most common barrier to licensure, and 62% expressing concerns about the financial costs associated with assessment, educational programs and licensure. Limited availability of and access to rural education or bridging programs was a barrier for 58% of respondents. Difficulties in navigating the assessment and licensure system were an obstacle for 55% of respondents, with less than half of respondents (39%) reporting language and accent concerns. Overall, the quantitative data corroborates the qualitative themes. For example, highlighting the financial stress, unclear signposting and information about the process, and the hidden costs associated with travel, barriers to educational access, and credentialing delays reported in the qualitative phase. See Figure 1 for key barriers to IEN workforce integration, and the full survey data is publicly available on the study team's website (https://csanders.opened.ca/outputs-from-the-2024-ien-survey/).
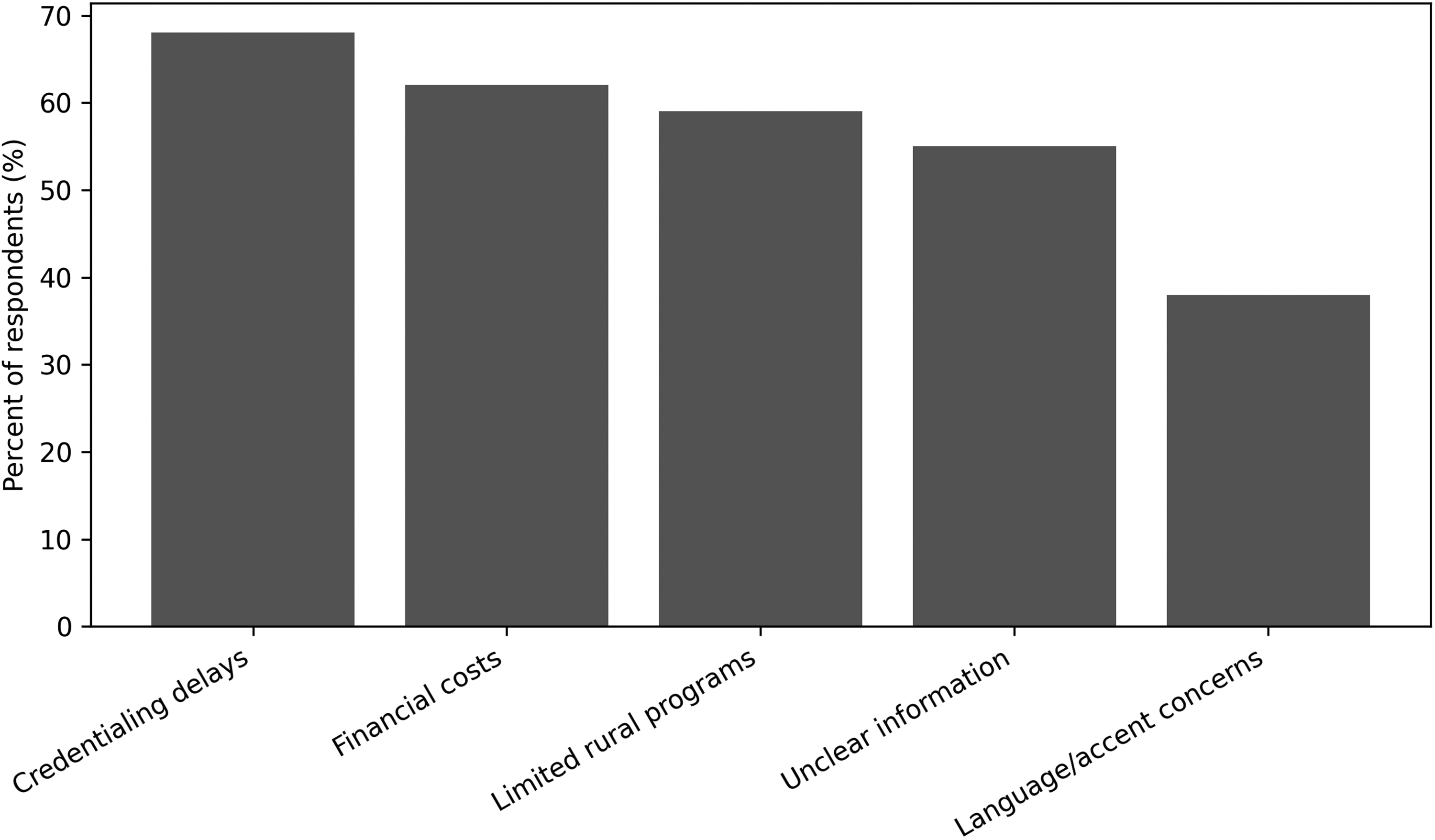
Key barriers to IEN workforce integration. Note. Bars represent the percentage of respondents endorsing each barrier.
Workshop
All partners in the workshop recognized the challenges IENs faced, and each party offered a commitment to explore new opportunities and support ongoing work with the study team. These new opportunities and support have led to post-secondary educational institutions and health partners working together with the BC Ministry of Post-Secondary Education and Future Skills (PSFS) to secure new financial investments that have led to the opportunity to develop and pilot test new rural IEN entry to practice programming around the province.
Discussion
The findings from this study underscore the urgent need to address systemic, geographic, and regulatory barriers that hinder IENs from re-entering the workforce in northern BC and across Canada. While the findings from Bayuo et al. (2023) and Cubelo et al. (2024) demonstrate that the demand for IENs remains high, their integration into healthcare systems is complex and fraught with challenges, often leading to deskilling, emotional distress, and unmet expectations.
Our findings align with the prevailing literature, which has employed a range of diverse methodologies and methods, i.e., meta-synthesis (Bayuo et al., 2023), scoping review (Njie-Mokonya et al., 2024), systematic review (Pressley et al., 2022), narrative systematic review (Rajpoot et al., 2024) and workshop approaches (CFNU, 2025) to investigate this problem over several decades, with the COVID-19 pandemic having further increased workforce recruitment challenges (Alostaz et al., 2025; Higginbottom, 2011; Tilley, 2021).
Focus group findings highlighted what can be described as independent equity sensitivity (Huseman et al., 1987); although individual perceptions varied, the group of IENs presented consistent examples of inequity, often described as frustration. At an individual level, IENs evaluated the unfairness of the process of becoming an RN in BC by comparing their efforts or input (contributions) to the outcome (reward) (Davlembayeva & Alamanos, 2025). They had high hopes, invested time and finance, trusting they could achieve registration, but often experienced delays and hurdles. Alostaz et al. (2025) reported similar results in Ontario with 12 IENs who experienced challenges with pre-registration despite wider policy changes to streamline processes.
The IENs in this study frequently described a mismatch between their expected and actual integration experiences, reflecting the inequities associated with prolonged licensure processes and limited access to employment. As noted by Cubelo et al. (2024), such discrepancies can diminish motivation and discourage continued pursuit of nursing careers in Canada. However, consistent with the CFNU IEN Report (2025), our findings indicate that many IENs, particularly those in rural communities, remained optimistic about re-entering the workforce. Participants drew strength from family, peer networks, and their local communities, valuing the opportunities that smaller settings offered and expressing a strong commitment to contributing their skills to meet local healthcare needs.
Our findings reinforce existing evidence that partnership-based approaches are critical to support IEN integration and address systemic barriers such as discrimination, language challenges, and fragmented supports (CFNU, 2025; Chiu, Alostaz, et al., 2025; WHO, 2025). However, this study extends prior work by demonstrating how these challenges persist for domestic IENs in rural and northern contexts, where access to licensure pathways, local education, and navigational supports remains limited.
Despite ongoing regulatory reforms and provincial investments to streamline assessment and the licensure processes, participants continued to experience prolonged delays, unclear pathways, and restricted local opportunities. These findings suggest that policy changes alone are insufficient without coordinated, place-based partnerships that translate reforms into accessible, on-the-ground support for IENs.
The northern workshop served as an effective knowledge translation strategy, a critical mechanism for creating change by bringing decision-makers into direct contact with IENs’ lived experiences through stories, quotations, and arts-based knowledge translation products. Grounding policy discussions in personal narratives fostered empathy, clarified system barriers, and created a shared sense of responsibility to act.
BCCNM as a Key Partner: Why This Mattered
The workshop was instrumental in bridging the gap between regulatory frameworks and the lived experiences of IENs. The engagement of key partners, especially BCCNM, was central to shifting awareness. Rather than positioning the regulator solely as a gatekeeper, the workshop reframed its role as a collaborator in reducing inequities. This relational approach helped bridge the gap between regulatory processes and everyday realities faced by IENs, enabling partners to see how well-intentioned policies were experienced as barriers in rural settings.
BCCNM's openness to supporting northern IENs is particularly important given the decentralized nature of healthcare regulation in Canada. Each province operates independently, and BC's rural geography presents unique challenges that require tailored solutions. As a result, discussions moved beyond problem identification toward concrete commitments, including improved pathway signposting, strengthened coordination with northern educational institutions and the health authority, including the securing of new government financial investments. Further, the work in the north enabled post-secondary institutions and health partners to work with the BC Ministry of PSFS to secure new financial investments to develop and pilot test rural IEN programming. BCCNM's participation lent credibility and momentum to these efforts, encouraging alignment among unions, assessors, and post-secondary partners. Together, these actions signal a transition from isolated reforms to coordinated, place-based solutions aimed at improving licensure access and workforce participation for rural IENs.
Building a Sustainable Future
Securing investment and building partnerships reflects a growing recognition that IEN integration is not just a regulatory issue; it is a workforce, equity, and community development issue. Northern BC, like many rural regions, faces persistent healthcare staffing shortages. Unlike internationally recruited nurses who must navigate immigration and relocation processes, many domestic IENs are already embedded in these communities, with established social networks and a strong commitment to local practice. While the narratives shared by IENs in this study highlight the emotional toll of exclusion, they also highlight the profound commitment to contributing meaningfully to Canadian society. Their stories of perseverance, cultural humility, and professional dedication challenge deficit-based views and call for a strengths-based approach to policy and practice. BCCNM's role in this transformation cannot be overstated. As a regulator, their support signals a shift toward inclusive excellence, where standards are upheld, but pathways are made accessible.
Recommendations
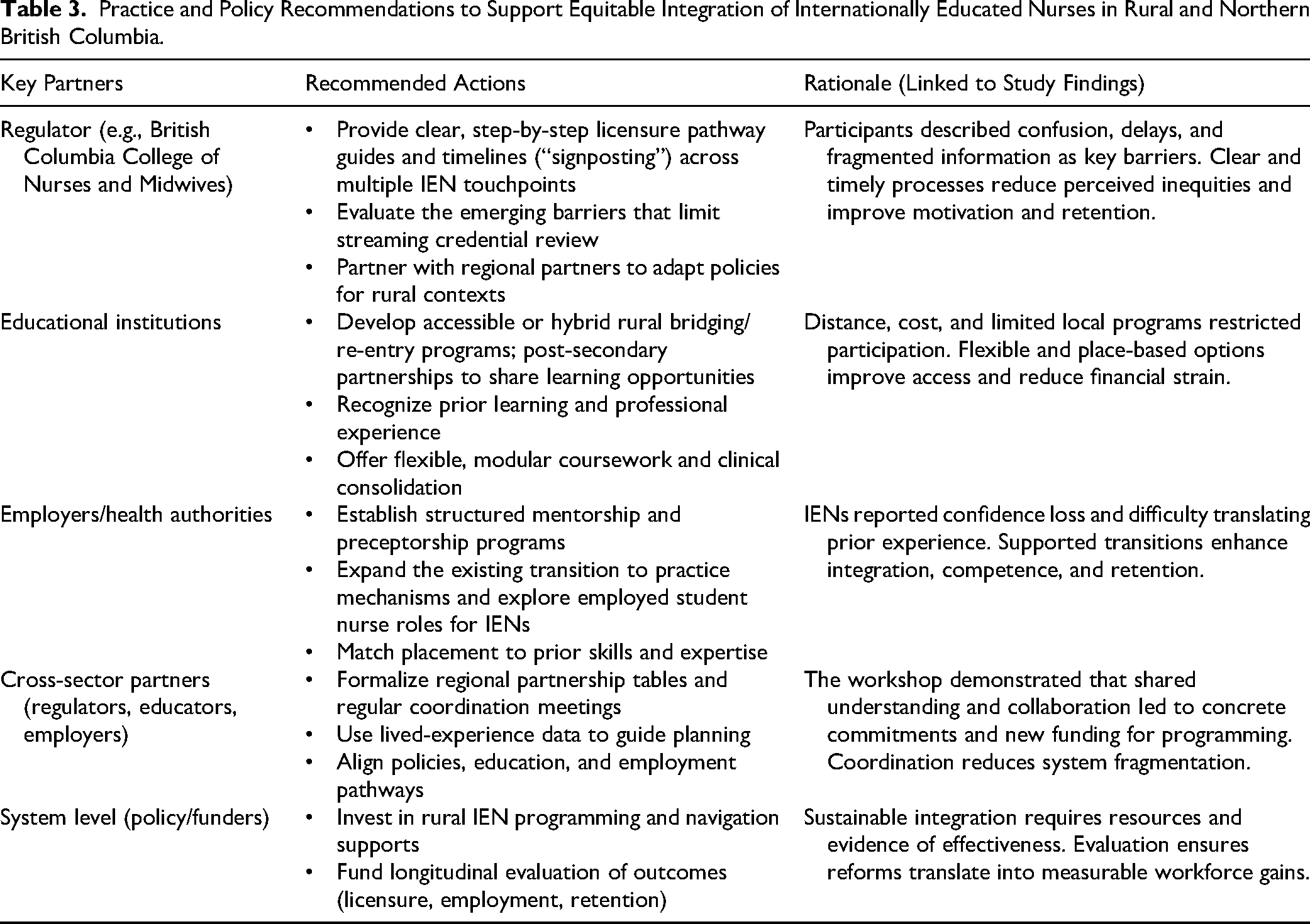
Findings from this study highlight the need for coordinated equity-oriented strategies that move beyond policy reform toward practical, place-based implementation. Based on IEN experiences and the outcomes of the northern workshop, we propose the following actions for regulators, educators, and health system partners, see Table 3. Collectively, these strategies support a shift from gatekeeping toward partnership, strengthening equitable access to nursing careers while addressing workforce shortages in rural and northern communities.
Practice and Policy Recommendations to Support Equitable Integration of Internationally Educated Nurses in Rural and Northern British Columbia.
Limitations
While this study offers valuable insights into the experiences of IENs in northern BC, several limitations must be acknowledged. First, the sample size for focus groups and interviews was small and regionally specific, reflecting the rural northern context. While this limits generalizability, the study prioritized depth of understanding and contextual insight over breadth, consistent with qualitative and equity-oriented approaches that center lived experience. Although the survey reached a broader audience, the self-selection process may have introduced bias, as participants who were more motivated or had stronger opinions may have been more likely to respond.
Second, although regulators, assessors, a union, educators, and employers participated in the workshop as knowledge partners, they were not included as primary research participants. This decision was intentional. Guided by our equity framework, the study first centered the voices of IENs, whose perspectives are often underrepresented in workforce planning discussions. Including institutional partners as equal participants at earlier stages risked reproducing existing power imbalances and shifting focus away from IEN experiences. However, this approach limited our ability to directly examine organizational and operational decision-making and implementation constraints. Future research could incorporate these partners as co-participants to evaluate feasibility and system-level changes over time.
Finally, survey participation was voluntary and may reflect the perspectives of IENs who were more motivated or engaged. While the study aimed to explore equity and motivation, it did not include a formal intersectional analysis of race, gender, or socioeconomic status, which may have further illuminated disparities in access and outcomes, even though this is reported in the online survey. Longitudinal and larger-scale studies are needed to assess how partnership-based initiatives influence licensure outcomes, employment, and retention across jurisdictions.
Conclusion
This study demonstrates that IENs in rural and northern BC experience persistent systemic, geographic, and regulatory inequities that delay licensure, undermine motivation, and contribute to workforce underutilization. Yet participants also described strong resilience, professional commitment, and a clear desire to contribute to their communities, underscoring the significant untapped potential of domestic IENs.
By centering lived experience and engaging regulators, educators, assessors, a union, and employers through a partnership workshop, this study translated evidence into coordinated action, including clearer pathways and new investments in rural programming. These findings highlight that equitable IEN integration requires more than policy reform; there is a need for a sustained, place-based collaboration to strengthen workforce capacity. This issue is particularly salient in rural and northern communities, where chronic workforce shortages, recruitment challenges, and high turnover create persistent gaps in care. Supporting IENs licensure and integration represents a timely and cost-effective workforce strategy, enabling health systems to mobilize existing talent. In this context, addressing systemic barriers for domestic IENs is not only an equity imperative but also a pragmatic solution to strengthening rural healthcare capacity.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621261454191 - Supplemental material for From Gatekeeping to Collaboration: Supporting Internationally Educated Nurses in Rural and Northern British Columbia
Supplemental material, sj-docx-1-cjn-10.1177_08445621261454191 for From Gatekeeping to Collaboration: Supporting Internationally Educated Nurses in Rural and Northern British Columbia by Caroline Sanders, Danielle Haggarty, Madison Friesen, Terri McKellar, Carolee Clyne, Catharine Schiller, Ibolya Agoston and Alison Roots in Canadian Journal of Nursing Research
Supplemental Material
sj-docx-2-cjn-10.1177_08445621261454191 - Supplemental material for From Gatekeeping to Collaboration: Supporting Internationally Educated Nurses in Rural and Northern British Columbia
Supplemental material, sj-docx-2-cjn-10.1177_08445621261454191 for From Gatekeeping to Collaboration: Supporting Internationally Educated Nurses in Rural and Northern British Columbia by Caroline Sanders, Danielle Haggarty, Madison Friesen, Terri McKellar, Carolee Clyne, Catharine Schiller, Ibolya Agoston and Alison Roots in Canadian Journal of Nursing Research
Footnotes
Acknowledgments
The authors would like to thank the IEN Advisory Group members; Joanne Cozac, Northern Health; Sara Telfer, BCCNM; Hazel Piano, BCNU; and Roger Autio, Providence Health
ORCID iDs
Ethical Approval
This research was approved by RISe (Research Information Systems (RISe), used by the University of British Columbia (UBC) and affiliated instituitons) Approval # REB H23-00845
Author Contributions
Conceptualization: CS, IA. Methodology: CS, TM. Analysis: CS, TM, DH, MF. Workshop development and implementation: CS, DH, CC, MF, CSh. Writing – original draft: CS, DH, AR. Writing – review & editing: CS, DH, MF, TM, CC, AR, IA.
Funding
This research was funded by the following grants: Health Research Institute seed grant, Michael Smith Foundation Health Research C2 convening grant
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.