
Abstract
Purpose:
To evaluate the prognostic value of carotid plaque features derived from high-spatial-resolution vessel-wall MRI (HR-MRI) for long-term major adverse cardiovascular events (MACE) after carotid revascularization.
Methods:
Consecutive patients undergoing carotid revascularization between April 2017 and April 2024 with preoperative carotid HR-MRI were included. Ipsilateral intraplaque hemorrhage (IPH) was identified as a hyperintense plaque component on SNAP images and manually segmented on each relevant slice using Vessel Explorer 2.0 software. IPH volume was calculated as the sum of the segmented IPH areas multiplied by slice thickness. MACE comprised cardiovascular death, nonfatal myocardial infarction, coronary revascularization, and stroke. Associations were assessed using Cox regression and Kaplan–Meier analysis. Prediction models were evaluated using the concordance index (C-index), calibration, and decision curve analysis (DCA).
Results:
Among 296 patients (mean age [65.04 ± 9.47] years; 244 [82.4%] men), 154 underwent carotid endarterectomy (CEA) and 142 underwent carotid artery stenting (CAS). During a median follow-up of 4.5 years, ipsilateral IPH volume was an independent predictor of MACE in the overall cohort (hazard ratio [HR], 1.49; 95% confidence interval [CI], 1.34-1.66; P < .001), as well as in the CEA subgroup (HR, 1.31; 95% CI, 1.11-1.55; P = .001) and CAS subgroup (HR, 1.21; 95% CI, 1.05-1.40; P = .007). Contralateral IPH was also independently associated with higher event risk in the overall cohort (HR, 2.37; 95% CI, 1.34-4.19; P = .003) and in both procedural subgroups (CEA: HR, 2.79; 95% CI, 1.16-6.67; P = .022; CAS: HR, 2.47; 95% CI, 1.22-5.00; P = .012). Kaplan–Meier analysis showed significantly lower event-free survival in patients with ipsilateral or contralateral IPH. Prediction models demonstrated acceptable discrimination (C-index: overall, 0.725; CEA, 0.755; CAS, 0.711), good calibration, and consistent clinical net benefit.
Conclusions:
Among HR-MRI–derived carotid plaque features, ipsilateral IPH volume and the presence of contralateral IPH were independently associated with long-term cardiovascular events after carotid revascularization. These findings support carotid IPH as an imaging marker of systemic atherosclerotic vulnerability and may improve individualized risk stratification after revascularization.
Introduction
Cardiovascular disease remains a leading cause of mortality worldwide, with atherosclerosis as its fundamental pathological substrate. 1 Carotid atherosclerotic disease contributes to ischemic cerebrovascular events and reflects systemic atherosclerotic burden and overall cardiovascular risk. 1 In current clinical practice, conventional vascular imaging – including duplex ultrasound, CT angiography, MR angiography, and digital subtraction angiography – primarily evaluates luminal stenosis and vascular anatomy. Although these parameters provide essential structural information, they may not fully capture plaque composition and biological vulnerability related to rupture, thromboembolism, and systemic atherosclerotic risk.
Carotid high-spatial-resolution vessel-wall magnetic resonance imaging (HR-MRI) enables in vivo characterization of carotid plaque morphology and composition, including plaque burden, intraplaque hemorrhage (IPH), lipid-rich necrotic core (LRNC), and fibrous cap disruption. 2 These features have been consistently associated with future ischemic events independent of stenosis severity,3-5 with meta-analytic evidence demonstrating their additive prognostic value beyond structural measurements. 6 In asymptomatic and population-based cohorts, MRI-derived markers of plaque vulnerability, particularly LRNC, further predict cardiovascular events independent of traditional risk factors and plaque burden. 7
However, most evidence linking plaque imaging features to clinical outcomes derives from non-interventional populations. Patients undergoing carotid revascularization represent a clinically distinct group with advanced carotid disease, high systemic vascular risk, and altered local hemodynamics after treatment. Although carotid endarterectomy (CEA) and carotid artery stenting (CAS) reduce the risk of ipsilateral cerebrovascular events related to the treated lesion, these patients remain vulnerable to long-term systemic cardiovascular events. Existing imaging studies in revascularization cohorts have mainly focused on periprocedural or short-term outcomes, 8 whereas the prognostic relevance of preoperative carotid plaque phenotype for long-term cardiovascular risk remains insufficiently defined.
Therefore, this study aimed to evaluate the prognostic value of carotid plaque features derived from HR-MRI for long-term major adverse cardiovascular events (MACE) in patients undergoing carotid revascularization. We further sought to identify informative imaging markers and to assess their potential utility for individualized post-revascularization risk stratification.
Methods
The study protocol was reviewed and approved by the Institutional Review Board (Approval No. 2025265x) and conducted in accordance with the Declaration of Helsinki. 9 Owing to the retrospective study design, written informed consent was not required.
Study Population
This retrospective study included patients who underwent carotid revascularization, including carotid endarterectomy (CEA) or carotid artery stenting (CAS), at our institution between April 2017 and April 2024. Patients were eligible if they had complete preoperative HR-MRI at our institution within 90 days prior to the index procedure. The exclusion criteria were: (1) non-atherosclerotic carotid disease (eg, dissection, aneurysm, Takayasu arteritis); (2) any prior carotid revascularization (CEA/CAS); (3) HR-MRI performed >90 days before revascularization; (4) incomplete MRI sequences or insufficient image quality for reliable plaque characterization; or (5) missing key clinical variables or unavailable follow-up. The patient selection process is summarized in Figure 1. No previous publication has been based on this study population or an overlapping subset of patients.
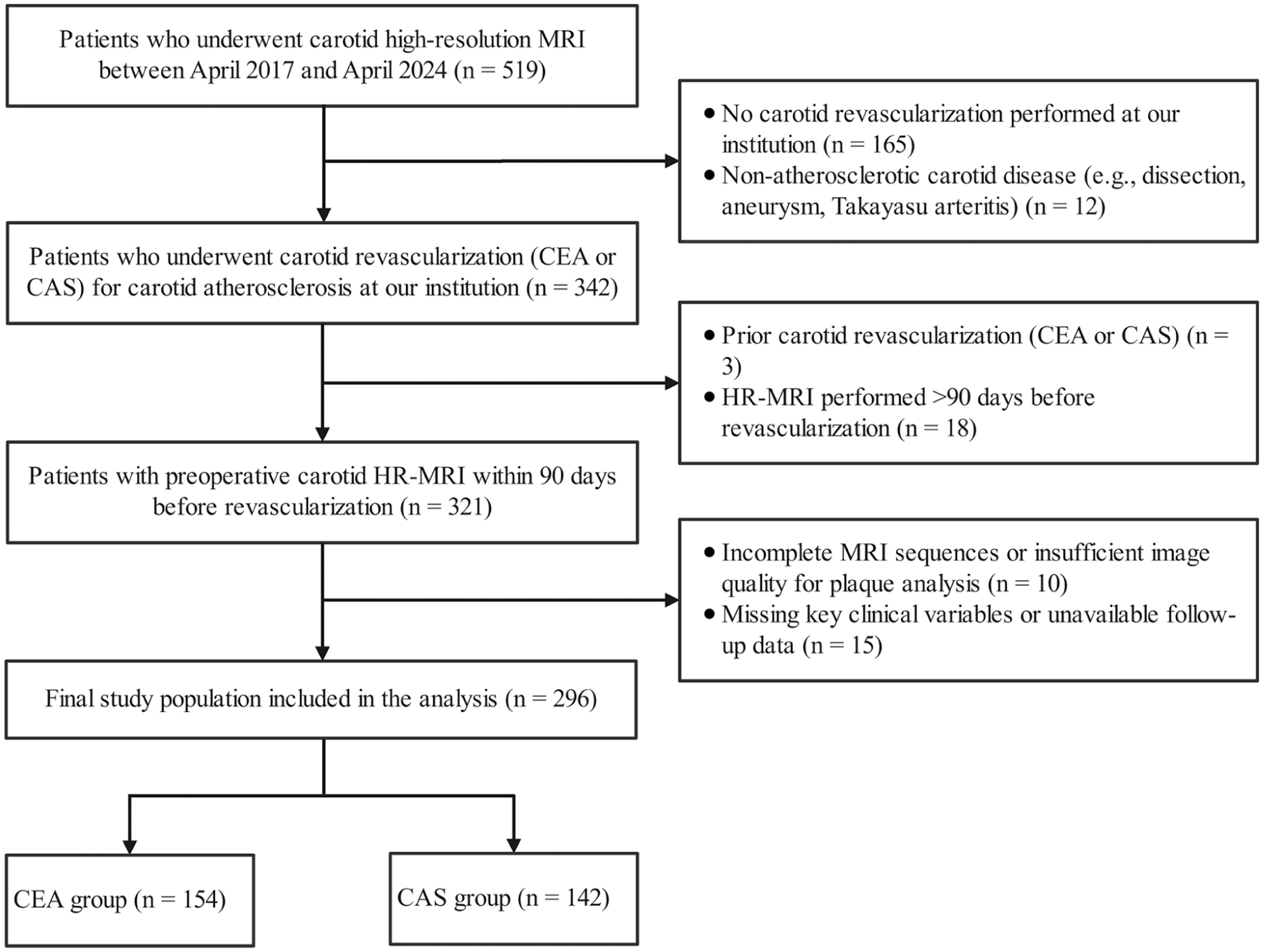
Flowchart of patient selection and study population.
HR-MRI Acquisition and Analysis
Carotid HR-MRI was performed using a 3.0-T scanner (Ingenia CX, Philips Healthcare, the Netherlands) with a 32-channel head coil combined with an 8-channel dedicated neck coil. Imaging was centered at the level of the maximum plaque burden and extended to cover both carotid bifurcations. A standardized multicontrast vessel-wall protocol was applied, including 3D time-of-flight (TOF) MR angiography, black-blood T1- and T2-weighted imaging, simultaneous non-contrast angiography and intraplaque hemorrhage (SNAP), and contrast-enhanced T1-weighted imaging. Detailed sequence-specific acquisition parameters, including repetition time, echo time, field of view, in-plane resolution, slice thickness, and number of slices, are provided in Table S1. Image quality was independently assessed by 2 radiologists with 5 and 3 years of experience in cardiovascular imaging, respectively, using a previously described 4-point scale. 10 Images rated as poor were excluded from further analysis. Disagreements were resolved by consensus, with adjudication by a senior cardiovascular radiologist with 10 years of experience when necessary.
Image analysis was performed using dedicated vessel-wall software (Vessel Explorer 2.0, TSImaging Healthcare). The 2 radiologists who assessed image quality, with 5 and 3 years of experience in cardiovascular imaging, respectively, also performed manual delineation of the lumen and outer wall boundaries on pre-contrast T1- and T2-weighted images. Both readers were blinded to clinical data and outcomes. Plaque components were characterized using multi-contrast MRI information. IPH was defined as hyperintensity on SNAP relative to the sternocleidomastoid muscle. 11 LRNC was defined as non- or minimally enhancing region on post-contrast T1-weighted images. Calcification was defined as signal hypointensity on all sequences; Plaque ulceration was defined as a focal luminal indentation (>1.0 mm in width or >2.0 mm in depth) and was required to be confirmed on both TOF and post-contrast imaging. Representative images are shown in Figure 2. Volumes of plaque components were computed by the software based on manually traced contours and slice thickness.
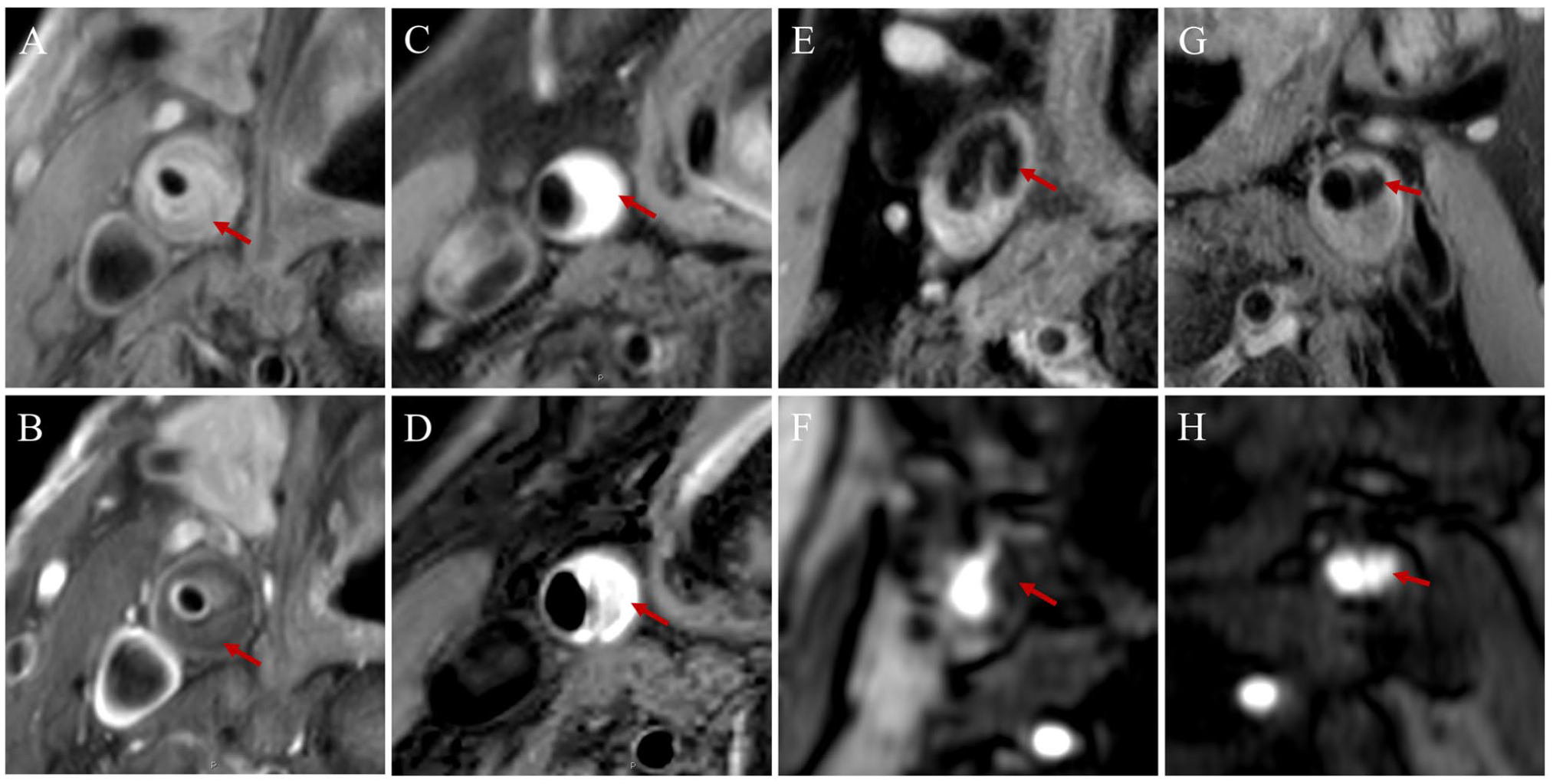
Representative HR-MRI images of carotid plaque components. (A, B) Pre-contrast T1WI and post-contrast T1WI demonstrating LRNC. (C, D) T1WI and SNAP showing IPH as hyperintensity on SNAP. (E, F) T1WI and TOF illustrating calcification (signal hypointensity). (G, H) T1WI and TOF demonstrating plaque ulceration (focal luminal indentation).
Plaque characteristics on the ipsilateral artery were assessed quantitatively, including volumetric measurements of plaque components, because the ipsilateral artery represented the treated culprit side and was the primary target for detailed plaque-component analysis. In contrast, contralateral plaque characteristics were evaluated by visual review and recorded as binary variables (presence/absence) for IPH, LRNC, calcification, and ulceration. This approach was used because the contralateral artery was included mainly to capture bilateral or systemic plaque vulnerability, and contralateral plaques were often smaller, less advanced, or more diffuse, making component-specific volumetric segmentation less reproducible. Contralateral stenosis was categorized as <50% versus ≥50%, and contralateral Plaque-RADS grade was dichotomized as <3 versus ≥3 points. 12
Interobserver reproducibility was assessed in a random subset of 30 cases using intraclass correlation coefficients for quantitative measurements and κ statistics for qualitative plaque features.
Clinical Outcomes and Follow-Up
The study endpoint was MACE, including cardiovascular death, nonfatal myocardial infarction, coronary revascularization (percutaneous coronary intervention or coronary artery bypass grafting), and stroke (ischemic or hemorrhagic). For time-to-event analyses, only the first occurrence of an endpoint event was considered. Patients were followed from the date of the index revascularization procedure until December 31, 2025, the occurrence of the study endpoint, or the last available follow-up, whichever came first.
Clinical Data Collection
Baseline clinical characteristics were obtained from electronic medical records, including age, sex, smoking, drinking, hypertension, diabetes mellitus, and a history of cardiovascular disease. Smoking history and alcohol use history were defined as any documented history of cigarette smoking and alcohol use in the electronic medical record. Hypertension was defined as systolic/diastolic blood pressure of ≥140/90 mmHg on repeated measurements or current use of antihypertensive medication. Diabetes mellitus was defined as fasting plasma glucose ≥7.0 mmol/L and/or treatment with glucose-lowering agents. Serum lipid profiles and high-sensitivity C-reactive protein (hsCRP) were measured using standardized laboratory assays. Body mass index was calculated as weight divided by height squared (kg/m2).
Statistical Analysis
Continuous variables are summarized as mean ± standard deviation or median (interquartile range), as appropriate, and categorical variables as counts and percentages. Between-group comparisons were performed using the Student’s t test or Mann–Whitney U test for continuous variables, and the χ2 test or Fisher’s exact test for categorical variables.
Because this was a retrospective cohort study including all consecutive eligible patients during the specified study period, no a priori sample size calculation was performed. To reduce the risk of overfitting, the number of covariates included in the multivariable Cox regression model was restricted according to the number of observed MACE events. Covariates were selected based on clinical relevance and univariable associations with outcome to maintain an adequate events-per-variable ratio.
The main analyses focused on clinically relevant MRI-derived carotid plaque vulnerability features, particularly IPH-related variables. Because these variables were selected based on biological plausibility and clinical relevance rather than data-driven screening alone, no additional multiple-comparison correction was applied to the main Cox regression analyses. Baseline comparisons, secondary plaque-feature analyses, and subgroup analyses were considered exploratory and interpreted cautiously.
Time-to-event outcomes were analyzed using Kaplan–Meier methods, and differences between groups were compared using the log-rank test. Associations between candidate variables and MACE were first evaluated using univariable Cox proportional hazards regression. Variables associated with MACE in univariable analyses, together with clinically relevant covariates, were considered for multivariable Cox regression models to identify independent predictors. Hazard ratios (HRs) and 95% confidence intervals (CIs) were reported.
Model performance was assessed in terms of discrimination, calibration, and clinical utility. Discrimination was evaluated using Harrell’s concordance index (C-index) with 95% CIs. Calibration was assessed by comparing predicted and observed 3-year MACE-free survival probabilities using bootstrap resampling (B = 200). Clinical utility was evaluated using decision curve analysis (DCA) by quantifying net benefit across a range of clinically relevant threshold probabilities.
Statistical analysis followed the TRIPOD (Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis) guidelines for model development, validation, and reporting. 13 All statistical analyses were performed using R software (version 26.0, IBM Corp., Chicago, IL, USA). A two-sided P value <.05 was considered statistically significant. In the presence of sparse events or separation, Firth’s penalized likelihood Cox regression was applied as appropriate.
Results
Baseline Characteristics
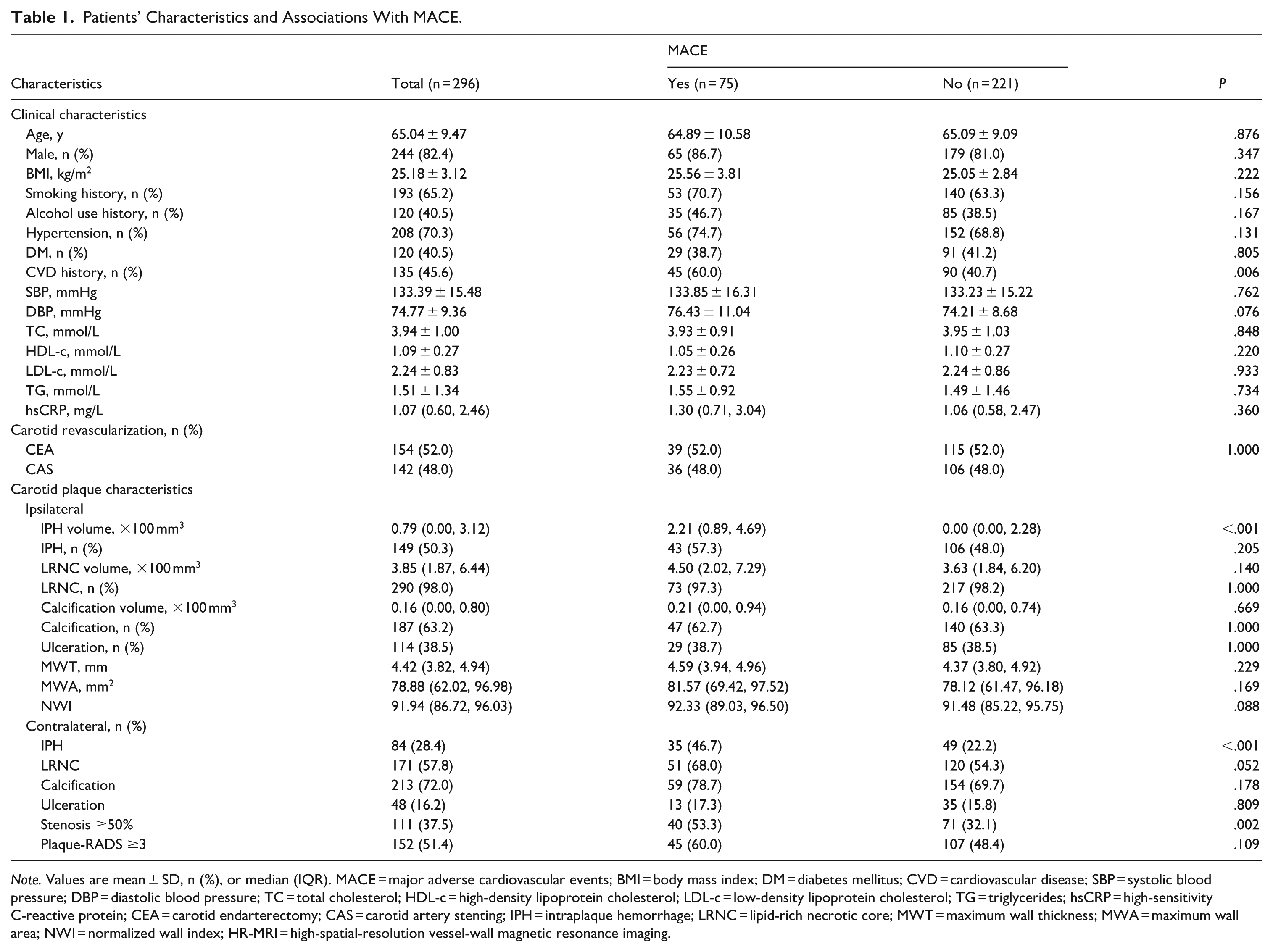
A total of 296 patients were included, of whom 154 underwent CEA and 142 underwent CAS. During a median follow-up of 4.5 years (interquartile range [2.7-6.8] years; full range [1.1-8.7] years), 75 patients (25.3%) experienced MACE (Table 1). The mean age was 65.04 ± 9.47 years, and 82.4% were male. Most baseline clinical characteristics were comparable between patients with and without MACE (all P > .05), except for a higher prevalence of CVD history in the MACE group (60.0% vs 40.7%, P = .006).
Patients’ Characteristics and Associations With MACE.
Note. Values are mean ± SD, n (%), or median (IQR). MACE = major adverse cardiovascular events; BMI = body mass index; DM = diabetes mellitus; CVD = cardiovascular disease; SBP = systolic blood pressure; DBP = diastolic blood pressure; TC = total cholesterol; HDL-c = high-density lipoprotein cholesterol; LDL-c = low-density lipoprotein cholesterol; TG = triglycerides; hsCRP = high-sensitivity C-reactive protein; CEA = carotid endarterectomy; CAS = carotid artery stenting; IPH = intraplaque hemorrhage; LRNC = lipid-rich necrotic core; MWT = maximum wall thickness; MWA = maximum wall area; NWI = normalized wall index; HR-MRI = high-spatial-resolution vessel-wall magnetic resonance imaging.
Regarding carotid plaque characteristics, patients who developed MACE had significantly greater ipsilateral IPH volume (median [IQR], 2.21 [0.89-4.69] vs 0.00 [0.00-2.28]; P < .001), while other ipsilateral plaque features were not significantly different between groups (all P > .05). In addition, contralateral IPH and ≥50% stenosis was more common in the MACE group (46.7% vs 22.2%, P < .001; and 53.3% vs 32.1%, P = .002, respectively).
The incidence of MACE was similar between CEA and CAS groups (25.3% vs 25.4%). Among patients who developed MACE, cardiac events slightly predominated over cerebrovascular events in both the CEA (59.0% vs 41.0%) and CAS groups (55.6% vs 44.4%; Figure S1).
Interobserver Reproducibility
Interobserver reproducibility was high for quantitative plaque measurements, with ICCs ranging from .80 to .92. Agreement for qualitative plaque features was also excellent, with κ values of approximately 0.90.
Cox Regression Analysis
In univariable Cox analysis, several clinical and plaque-related variables were associated with MACE in the overall cohort and in procedure-specific subgroups (Table 2). In the overall cohort, CVD history, ipsilateral IPH volume, presence of contralateral IPH, and contralateral stenosis ≥50% were associated with MACE in univariable analysis. After multivariable adjustment, CVD history (HR, 1.71; 95% CI, 1.07-2.75; P = .026), ipsilateral IPH volume (HR, 1.49; 95% CI, 1.34-1.66; P < .001), and presence of contralateral IPH (HR, 2.37; 95% CI, 1.34-4.19; P = .003) remained independently associated with increased risk of MACE.
Cox Regression Analysis of Predictors of MACE in the Overall Cohort and Procedure-Specific Subgroups.
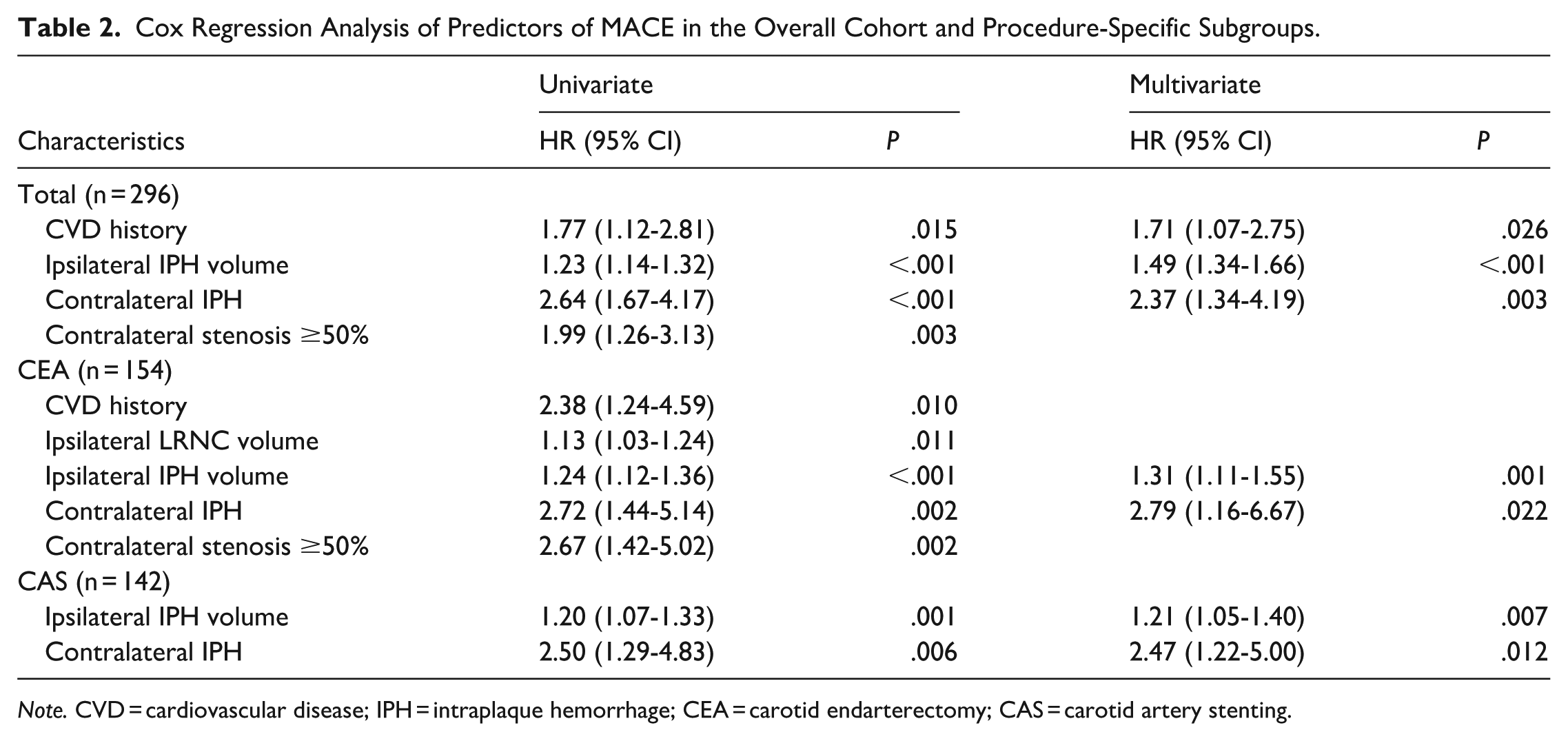
Note. CVD = cardiovascular disease; IPH = intraplaque hemorrhage; CEA = carotid endarterectomy; CAS = carotid artery stenting.
In the CEA subgroup, CVD history, ipsilateral LRNC volume, ipsilateral IPH volume, presence of contralateral IPH, and contralateral stenosis ≥50% were significant in univariable analysis. In the multivariable model, ipsilateral IPH volume (HR, 1.31; 95% CI, 1.11-1.55; P = .001) and presence of contralateral IPH (HR, 2.79; 95% CI, 1.16-6.67; P = .022) remained independently associated with MACE.
In the CAS subgroup, ipsilateral IPH volume and contralateral IPH were associated with MACE in univariable analysis and both remained significant after multivariable adjustment (ipsilateral IPH volume: HR, 1.21; 95% CI, 1.05-1.40; P = .007. Presence of contralateral IPH: HR, 2.47; 95% CI, 1.22-5.00; P = .012).
Kaplan–Meier Survival Analysis
Kaplan–Meier analysis demonstrated significant differences in event-free survival according to CVD history, ipsilateral IPH, and contralateral IPH (Figure 3). CVD history was associated with lower event-free survival in the overall cohort (log-rank P = .011) and in the CEA subgroup (P = .031), but not in the CAS subgroup (P = .277). Ipsilateral IPH showed marked separation of survival curves in the overall cohort as well as in both revascularization subgroups (all P < .001). Similarly, contralateral IPH was associated with poorer event-free survival in the overall cohort and remained significant in both the CEA and CAS subgroups (all P ≤ .005).
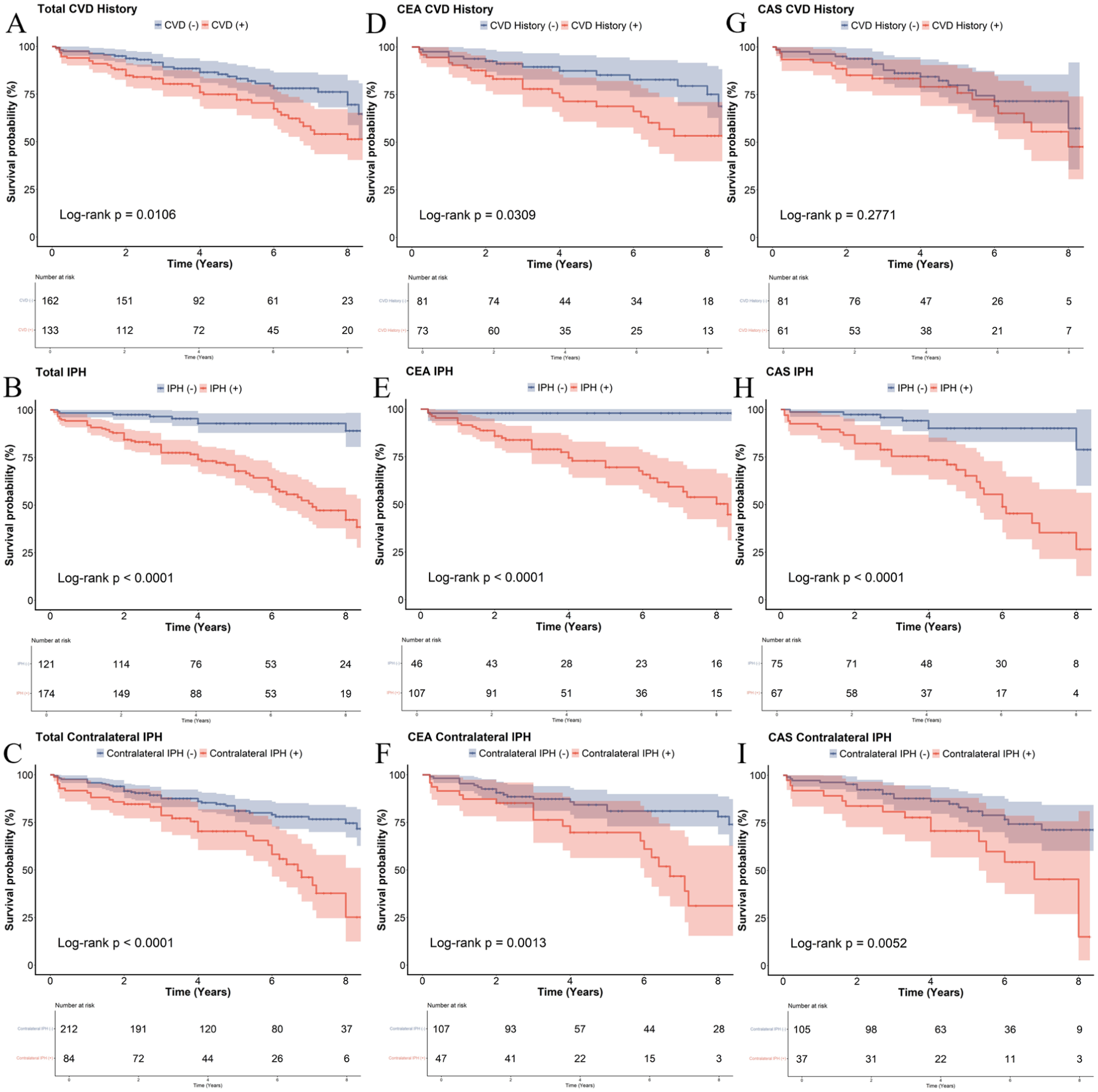
Kaplan–Meier curves of event-free survival stratified by CVD history (A, D, G), ipsilateral IPH (B, E, H), and contralateral IPH (C, F, I) in the overall cohort and by revascularization strategy (CEA and CAS). Shaded areas denote 95% CI; numbers at risk are shown below.
Prediction Model Performance
Prediction models derived from multivariable Cox regression were used to estimate 3-year MACE-free survival. The models demonstrated acceptable discriminative ability in the overall cohort (C-index, 0.725; 95% CI, 0.718-0.732), with the highest performance observed in the CEA subgroup (C-index, 0.755; 95% CI, 0.743-0.767), while maintaining satisfactory performance in the CAS subgroup (C-index, 0.711; 95% CI, 0.697-0.725).
Model calibration for 3-year MACE-free survival showed generally good agreement between predicted and observed outcomes across the overall cohort and both procedure-specific subgroups (Figure 4). The calibration curves were broadly close to the 45° reference line, indicating acceptable agreement between predicted and observed survival probabilities.
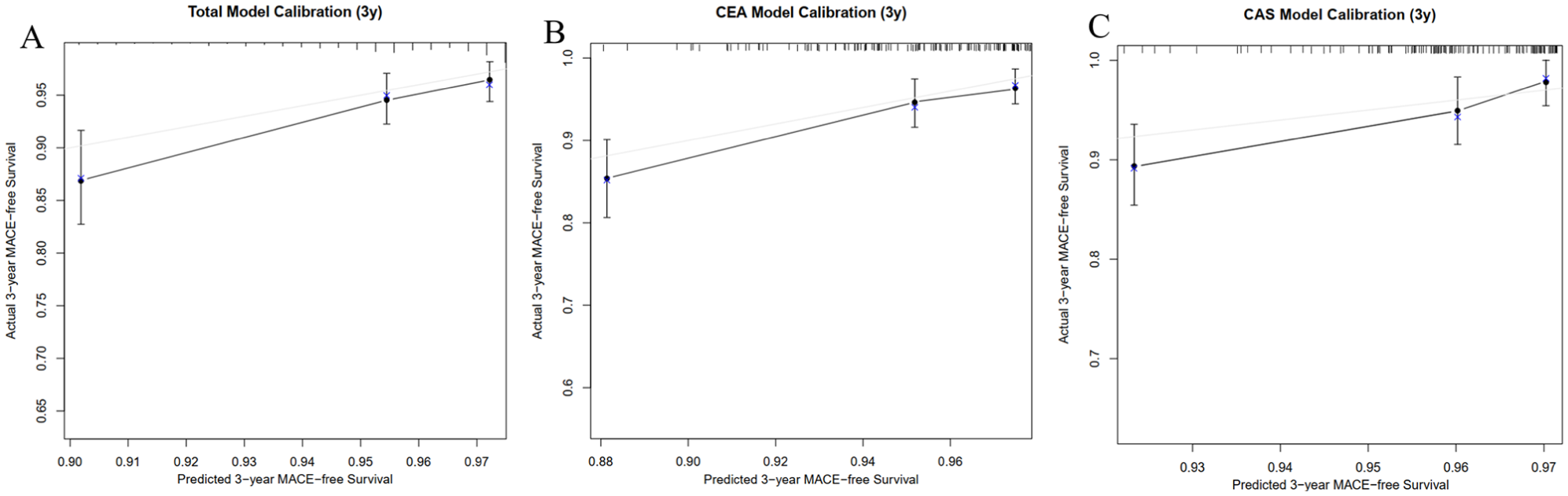
Calibration curves for 3-year MACE-free survival in the overall cohort (A) and in the CEA (B) and CAS (C) subgroups. The diagonal line indicates ideal calibration; bootstrap resampling (B = 200) was used for optimism correction.
Clinical utility was further evaluated using decision curve analysis (DCA) for 3-year MACE-free survival (Figure 5). Across the overall cohort and both procedure-specific subgroups, the models demonstrated higher net benefit than the default strategies (“treat-all” and “treat-none”) over a clinically relevant range of threshold probabilities.
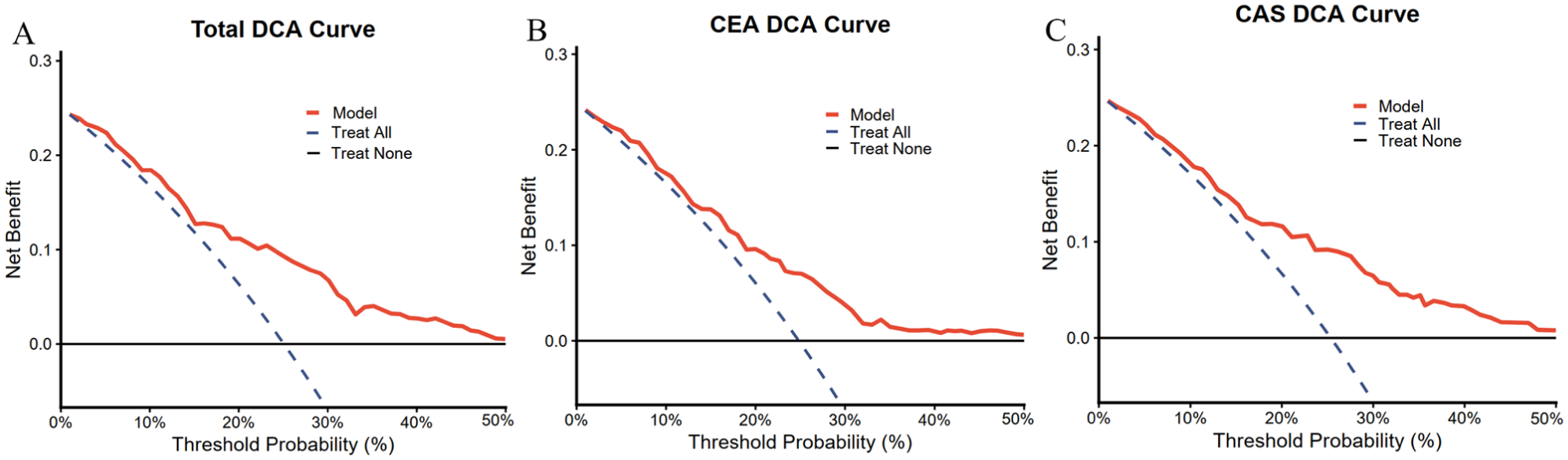
Decision curve analysis (DCA) of the prediction models for MACE in the overall cohort (A), CEA (B), and CAS (C) subgroups. The full model is shown in red, with “treat-all” (blue dashed) and “treat-none” (black) as reference strategies.
Discussion
In this long-term cohort of patients undergoing carotid revascularization, we found that IPH-related plaque features derived from HR-MRI were independently associated with long-term MACE. Specifically, ipsilateral IPH volume and the presence of contralateral IPH were associated with higher event risk in the overall cohort and in both CEA and CAS subgroups. These findings suggest that carotid IPH may reflect not only local plaque vulnerability but also a systemic predisposition to atherosclerotic instability. 14
Our results extend previous carotid plaque imaging studies by focusing on patients undergoing carotid revascularization, a population with advanced carotid disease and substantial residual cardiovascular risk. Previous studies have shown that MRI-derived plaque characteristics, particularly IPH and LRNC, improve risk prediction in asymptomatic or subclinical carotid atherosclerosis,15,16 and that IPH predicts recurrent ipsilateral ischemic events in stroke-focused populations.17,18 In the present revascularized cohort, quantitative ipsilateral IPH volume remained independently associated with long-term outcomes when the endpoint was broadened to systemic cardiovascular events, while the association of contralateral IPH with MACE further supports the concept that plaque vulnerability may represent generalized atherosclerotic instability across vascular territories.19,20
The biological plausibility of these findings is supported by the established role of IPH in plaque progression and destabilization. IPH may promote erythrocyte-derived lipids deposition, oxidative stress, inflammation, necrotic core expansion, and fibrous cap weakening,14,21 thereby increasing the likelihood of plaque disruption and thrombosis. Because contralateral IPH is unlikely to affect outcomes solely through local mechanical effects, its prognostic value in our cohort supports its role as an imaging marker of diffuse atherosclerotic instability and increased systemic cardiovascular risk.22,23
The prognostic relevance of IPH was consistent across CEA and CAS subgroups. Although CEA removes the culprit plaque24,25 whereas CAS restores luminal patency while leaving plaque tissue in situ, 26 the associations of both ipsilateral IPH volume and contralateral IPH with MACE were observed in both procedural groups. This consistency suggests that IPH-related risk may reflect systemic vascular vulnerability rather than procedure-specific effects alone.
From a clinical perspective, patients undergoing carotid revascularization remain at considerable risk of long-term systemic cardiovascular events. In our cohort, MACE incidence was similar between the CEA and CAS groups, and cardiac events accounted for a considerable proportion of outcomes, consistent with previous studies showing that long-term outcomes after carotid intervention are frequently driven by myocardial infarction and cardiac death rather than recurrent ipsilateral stroke alone.25,27-30 These findings highlight the diffuse nature of atherosclerosis,31,32 and support the use of carotid plaque vulnerability, particularly ipsilateral IPH volume and contralateral IPH, as clinically relevant imaging markers for long-term cardiovascular risk after revascularization.
To support clinical translation, prediction models incorporating clinical variables and HR-MRI–derived plaque vulnerability markers showed acceptable discrimination and generally good calibration, although calibration was less precise at the highest-risk end, likely because of limited data density in extreme-risk strata. 33 Decision curve analysis also suggested clinical net benefit across relevant threshold probabilities. 34 These findings indicate that incorporating IPH-related plaque vulnerability markers into routine carotid HR-MRI assessment may help identify patients who require closer follow-up and more intensive secondary prevention after revascularization.
Several limitations should be acknowledged. First, this was a retrospective single-center study, which may limit generalizability and introduce potential selection bias. External validation in independent cohorts is therefore required. Second, contralateral plaque features were assessed using categorical rather than volumetric measures. This approach was chosen because the contralateral artery was included primarily as a marker of bilateral or systemic plaque vulnerability rather than as the treated culprit lesion, and contralateral plaques were often smaller, less advanced, or more diffuse. Although this strategy improved robustness and clinical interpretability in this retrospective cohort, it may have reduced sensitivity for detecting more subtle associations. Future studies using standardized bilateral volumetric plaque segmentation are warranted. In addition, secondary and subgroup analyses were exploratory and were interpreted without formal adjustment for multiple comparisons; therefore, these findings should be interpreted cautiously and require validation in independent cohorts. Third, although model discrimination was acceptable, calibration was less precise at the highest-risk end, highlighting the need for further model refinement and validation. Finally, residual confounding inherent to the observational study design cannot be excluded.
Conclusions
Among carotid plaque features derived from HR-MRI, quantitative ipsilateral IPH volume and the presence of contralateral IPH on preoperative carotid HR-MRI were independently associated with long-term MACE after carotid revascularization. These findings suggest that IPH may serve as a key imaging marker of systemic atherosclerotic vulnerability rather than merely reflecting focal carotid plaque instability. Incorporating IPH–based metrics into clinical assessment may improve individualized risk stratification and support more tailored long-term follow-up and secondary prevention strategies in this high-risk population.
Supplemental Material
sj-docx-1-caj-10.1177_08465371261464591 – Supplemental material for High-Resolution MRI-Derived Carotid Plaque Feature for Long-Term Cardiovascular Risk Stratification After Carotid Revascularization: The Role of Intraplaque Hemorrhage
Supplemental material, sj-docx-1-caj-10.1177_08465371261464591 for High-Resolution MRI-Derived Carotid Plaque Feature for Long-Term Cardiovascular Risk Stratification After Carotid Revascularization: The Role of Intraplaque Hemorrhage by Sunan Xu, Yunhao Lei, Lu Li, Xinyu Wu, Zhenjia Wang and Wei Yu in Canadian Association of Radiologists Journal
Supplemental Material
sj-tif-1-caj-10.1177_08465371261464591 – Supplemental material for High-Resolution MRI-Derived Carotid Plaque Feature for Long-Term Cardiovascular Risk Stratification After Carotid Revascularization: The Role of Intraplaque Hemorrhage
Supplemental material, sj-tif-1-caj-10.1177_08465371261464591 for High-Resolution MRI-Derived Carotid Plaque Feature for Long-Term Cardiovascular Risk Stratification After Carotid Revascularization: The Role of Intraplaque Hemorrhage by Sunan Xu, Yunhao Lei, Lu Li, Xinyu Wu, Zhenjia Wang and Wei Yu in Canadian Association of Radiologists Journal
Footnotes
Acknowledgements
The authors thank all staff and patients involved in this study for their contributions.
Ethical Considerations
This retrospective study was approved by the Institutional Review Board of Beijing Anzhen Hospital, Capital Medical University (Approval No.: 2025265x). The study was conducted in accordance with the Declaration of Helsinki.
Consent to Participate
The requirement for informed consent to participate was waived by the Institutional Review Board of Beijing Anzhen Hospital, Capital Medical University because of the retrospective nature of the study.
Author Contributions
Sunan Xu: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft. Yunhao Lei: Data curation; Investigation; Validation; Writing – review & editing. Lu Li: Data curation; Investigation; Resources. Xinyu Wu: Formal analysis; Software; Visualization. Zhenjia Wang: Methodology; Supervision; Writing – review & editing. Wei Yu: Conceptualization; Funding acquisition; Project administration; Supervision; Writing – review & editing. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of Beijing Municipality (Grant No. 7222047) and the China International Medical Foundation (Grant No. Z-2014-07-2101).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to institutional regulations and patient privacy restrictions, but may be available from the corresponding author upon reasonable request and with appropriate institutional approval.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.