
Abstract
To evaluate whether botulinum toxin type A at standard doses spreads to antagonist leg muscles in dynamic equinus foot, we studied 18 ambulatory children with hemiplegic cerebral palsy. The gastrocnemius muscle on the affected side was injected with botulinum toxin type A (Dysport) (mean ± standard deviation, 14.3 ± 0.9 U/kg). Compound muscle action potential areas were assessed in the lateral gastrocnemius and tibialis anterior muscles on the treated and untreated sides before botulinum toxin type A injections and on days 10 and 30 after injections. In all patients, compound muscle action potential areas recorded from both the muscles on the treated side decreased from preinjection values at day 10 (P < .05) and 30 (P < .002). After injection, ankle spasticity had diminished (P < .05), equinus foot excursion increased (P < .05), and functional gait improved (P < .05). This study shows that botulinum toxin type A spreads from foot flexors to antagonist extensors and suggests that spread may be partly responsible for improving gait in children with cerebral palsy.
Case reports and open-label and double-blind trials have amply documented the effectiveness and safety of botulinum neurotoxin type A in children with cerebral palsy.1–6 The toxin relieves the symptoms of spasticity by weakening muscle through a reversible neuromuscular blockade and reducing the hyperactive spinal reflex at the neuromuscular junction.2,7
In children with cerebral palsy, the botulinum neurotoxin type A–induced decrease in muscle spasticity depends on various factors. It is enhanced by higher injection volume. 8 Injecting botulinum neurotoxin type A at multiple sites leaves its effectiveness in decreasing muscle spasticity unchanged. 9 Controversy surrounds the maximal dose to inject in the lower limb in children with equinus foot deformity and the suggested dose to be injected in calf muscles.10,11 Even if the recommended doses of Dysport (Ipsen, Paris, France) are 20 to 25 mg/kg10,12,13 and more recently limited to 15 to 20 mg/kg, 14 accumulating evidence suggests that higher than usual doses of botulinum toxin are both safe and effective in improving the patient’s health state.5,15–18
Alongside the safety and effectiveness of botulinum neurotoxin type A, another feature influencing the efficacy of toxin in equinus foot is regional spreading to neighboring muscles. Locoregional botulinum neurotoxin type A spread depends on several factors including dose, volume concentration, number of injections, and muscular fascia. 19 Botulinum neurotoxin type A spreads to surrounding muscle in experimental studies in rabbits and mice, healthy subjects, and adult patients with occupational cramp and cervical dystonia.20–24 Despite evidence suggesting that botulinum neurotoxin type A spreads also in children, 10 no study has investigated this concern in healthy children or children with cerebral palsy. Despite evidence that the standard recommended doses decrease limb spasticity in children,10,12–14,25,26 more information is also needed on the ratio between the dose and toxin spread.
Our first aim in this study was to investigate whether, and if so to what extent, botulinum neurotoxin type A injected into the gastrocnemius muscle within standard dose ranges spreads to surrounding antagonist muscles in children with cerebral palsy and induces chemodenervation in injected muscles. As the primary neurophysiological outcome measure of botulinum neurotoxin type A induced paresis and spread, we studied changes in compound muscle action potential areas recorded from the lateral gastrocnemius muscle after injecting botulinum neurotoxin type A and from the ipsilateral tibialis anterior muscle in children with spastic hemiplegia. In line with others, we considered a decreased compound muscle action potential area from the lateral gastrocnemius muscle injected with botulinum neurotoxin type A as the neurophysiological index of botulinum neurotoxin type A–induced paresis8,27 and a decreased compound muscle action potential area from the tibialis anterior muscle as the main index of botulinum neurotoxin type A spread to the surrounding anterior leg muscle. Our second aim was to study the short-term clinical effect of botulinum neurotoxin type A injected within standard dose ranges on changes in gait in children with cerebral palsy. As the clinical outcome measures, clinical scales were assessed, and video gait was analyzed before botulinum neurotoxin type A injections (T0) and on days 10 (T10) and 30 (T30) after injections.
Methods
In a prospective, randomized, open-label study lasting 30 days, we studied 18 ambulatory children outpatients with hemiplegic cerebral palsy (spasticity largely confined to one side) aged 6.1 ± 0.6 years (mean ± standard error) (Table 1). Patients entered in the study voluntarily, and their parents gave informed consent. Inclusion criteria for the study were spasticity refractory to oral medication; patients able to walk independently or with aid; no contraindications to botulinum neurotoxin type A treatment such as fixed contracture, aminoglycoside therapy, and myasthenia gravis and no other neuromuscular diseases; no previous orthopedic surgery; normal or mildly declined cognition; and previous treatment at least 6 months before the study. Exclusion criteria were all contraindications to botulinum neurotoxin type A treatment. The institutional review board at the Neurological Sciences Department of the University of Verona approved the protocol.
Demographic and Clinical Characteristics of All Enrolled Children With Cerebral Palsy Who Received Botulinum Type A Injections
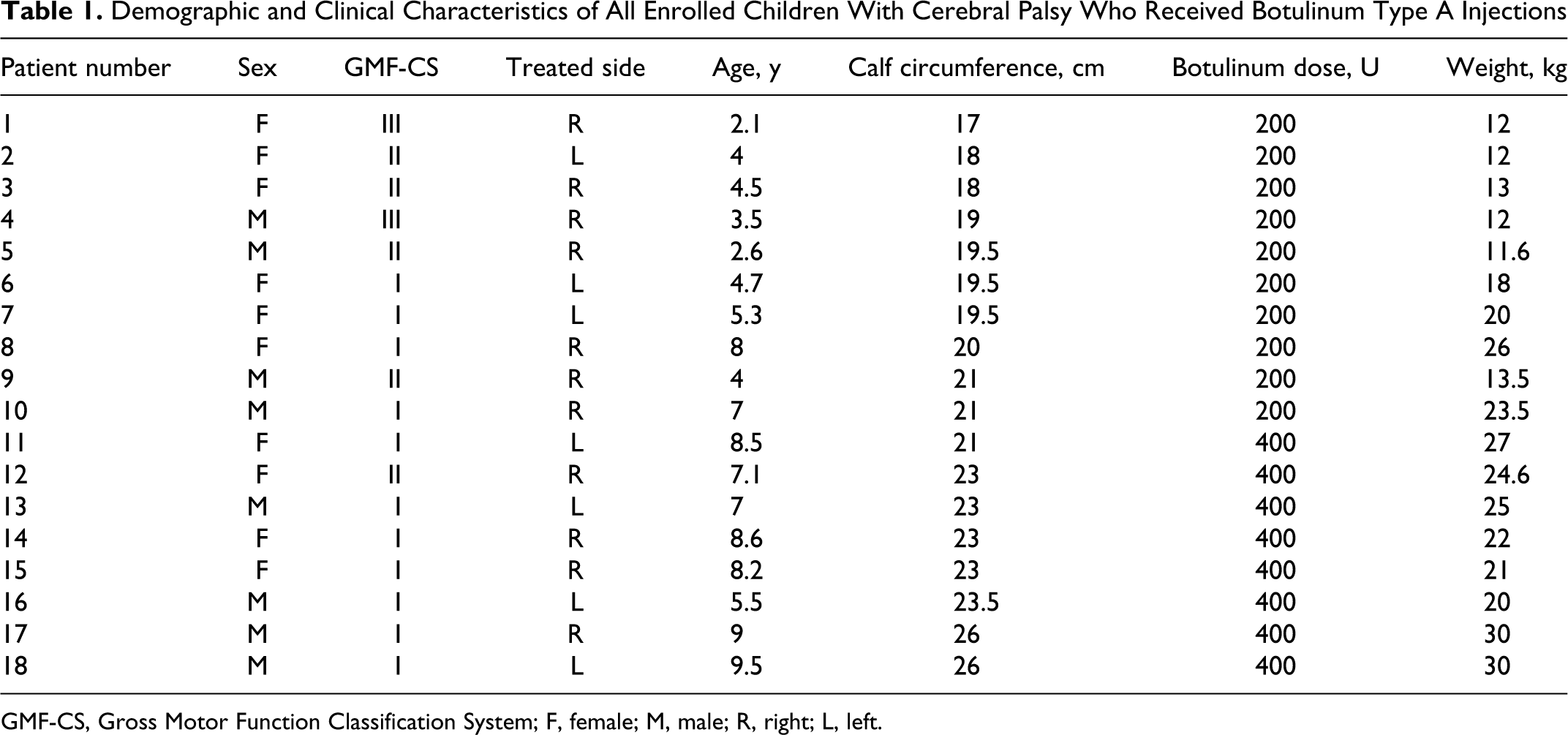
GMF-CS, Gross Motor Function Classification System; F, female; M, male; R, right; L, left.
When enrolled, all the children were able to walk, independently or with a manual walking aid, and were evaluated with the Gross Motor Function Classification System for cerebral palsy and assigned to levels I to III (Table 1). 28 Patients with normal mild global cognitive level or performance as evaluated with the Griffith Scale 29 and Progressive Raven’s Matrices 30 were included in the study.
Each patient underwent calf circumference measurement before botulinum neurotoxin type A injections (Table 1). Because calf circumference in our patients varied from 17 to 26 cm, we identified (based on the median) 2 subgroups: to minimize the risk of muscle size influencing spread, children with calf circumference from 17 to 21 cm received 200 U botulinum neurotoxin type A, and those with circumference from 22 to 26 cm received 400 U.
At the first nerve conduction study, to ensure that none of the children had peripheral neuropathy, bilateral sural nerve action potential amplitude and distal latency were evaluated, and tibial and peroneal nerve M-wave amplitude, distal latency, and conduction velocity were recorded. A Reporter Esaote Biomedica electromyograph (Esaote Biomedica, Florence, Italy) was used to generate the stimuli and record all responses (filter settings, 20 Hz to 5 kHz). All muscle responses were recorded through disposable surface electrodes 11 mm in diameter. Compound muscle action potential areas from the lateral gastrocnemius and tibialis anterior muscles were obtained during supramaximal stimulation of the tibial nerve at the popliteal fossa and common peroneal nerve below the head of the fibula bilaterally. Stimulus duration ranged from 0.1 to 1 millisecond depending on the different skin impedance, and voltage intensity (mV) was set to obtain the maximal compound muscle action potential area. The recording electrode was placed over the belly and the reference electrode over the tendon of the lateral gastrocnemius and tibialis anterior muscles. Distances from the popliteal fossa and corresponding recording electrode and from the head of the fibula and recording electrode were measured to ensure that electrodes were correctly placed for each study. All traces were rectified. We ensured that the surface skin temperature of the foot was above 32°C. The same examiner, blinded to treatment group, did all the neurophysiological studies.
Botulinum neurotoxin type A (Dysport, Ipsen) was injected at a similar dose into the medial and lateral gastrocnemius muscles unilaterally on the affected spastic hemiplegic side (Table 1). The botulinum neurotoxin type A dose injected in each patient ranged from 200 to 400 U (mean ± standard error, 277.8 ± 24.3 U) according to calf diameter. The mean dose per kilogram injected was 14.3 ± 0.9 U/kg (range, 7.4-20 U/kg) diluted in 2.5 mL saline. We used this dose because it is within the standard dose suggested by the 2006 and 2009 European Consensus Conference14,15 as appropriate to avoid adverse events. Botulinum neurotoxin type A was injected with a 27-gauge needle intramuscularly immediately below the site of maximal M-wave area in the lateral gastrocnemius muscle and into the nearby medial gastrocnemius muscle.
The neurophysiological outcome measures included changes in the compound muscle action potential area from lateral gastrocnemius and tibialis anterior muscles evaluated before botulinum neurotoxin type A injection (day 0) and after injections. After botulinum neurotoxin type A injection, patients underwent nerve conduction studies twice (days 10 and 30). The compound muscle action potential area decrease was evaluated in both lateral gastrocnemius and tibialis anterior muscles before botulinum neurotoxin type A injection (day 0) and at 2 time points thereafter (days 10 and 30). The compound muscle action potential area before treatment/compound muscle action potential area after treatment times 100 (compound muscle action potential percentage) was evaluated. The compound muscle action potential percentage decrement on the injected side and on the uninjected side was compared on each day (10 and 30).
The clinical outcome measures included evaluations before treatment (at baseline, T0) and changes after botulinum neurotoxin type A treatment at T10 and T30 in the Modified Ashworth Scale at the ankle 31 : 2 levels of passive range of motion referring to R1 and R2 angles. R1 referred to the point in the passive range of motion where a “catch” was felt during a quick stretch of the ankle plantarflexor, whereas R2 referred to total passive range of motion into ankle dorsiflexion with extended knees. The ankle passive range of motion angle in the modified Tardieu scale was measured by manual goniometry with the “neutral-null” method (dorsiflexion angle over the neutral position was counted in positive degrees and under the neutral in negative degrees). 32 R2 minus R1 yielded the dynamic component of spasticity. 33 A dynamic response greater than 15° is considered associated with a better response to botulinum neurotoxin type A treatment. 34 Passive range of motion was evaluated also for the contralateral side and knees. To evaluate gait, we used the Edinburgh Visual Gait Score containing 17 variables of observation during gait at 6 anatomic levels (foot, ankle, knee, hip, pelvis, and trunk), including sagittal and frontal observations. 35 Recorded variables were assessed using a 3-point ordinal scale: 0 (normal), 1 (moderate deviation), and 2 (marked deviation). Both sides of the patients were scored separately. The observer was recommended to use slow-motion facilities, to stop or repeat the video if necessary, and to take his or her time. The physician was instructed not to measure degrees directly from the video screen but to give his or her best visual estimate. For all patients, both sides were scored. All outcome measures were assessed by the same physician, who was unaware of the type of intervention that the child had received. All patients took part in a rehabilitation program.
Statistical Analysis
Because the number of patients was small and values had a non-Gaussian distribution, we used nonparametric tests. We used a nonparametric 2-way analysis of variance test to compare the compound muscle action potential percentage area changes on treated and untreated muscles, Modified Ashworth Scale, passive range of motion, and Edinburgh Visual Gait Score at the 3 time points before (T0) and after (T10 and T30) botulinum neurotoxin type A injection. A nonparametric test for paired data (Wilcoxon test) was used to compare the calf circumference on both sides and the compound muscle action potential area on the treated side with the compound muscle action potential area on the untreated side before (T0) and after (T10 and T30) botulinum neurotoxin type A treatment. Spearman correlation test was used to compare calf circumference, total botulinum neurotoxin type A dose, lateral gastrocnemius and tibialis anterior compound muscle action potential areas, and clinical evaluation scores. P values ≤.05 were considered to indicate statistical significance.
Results
In all 18 patients with cerebral palsy studied, recordings at baseline (T0) showed similar compound muscle action potential areas in treated and untreated calf muscles (lateral gastrocnemius, 30.3 ± 18.5 mVms; tibialis anterior, 16.45 ± 8.3 vs 16.2 ± 8). In all patients, the compound muscle action potential percentage areas of the injected lateral gastrocnemius and tibialis anterior muscles were significantly lower than the compound muscle action potential percentage areas of the uninjected lateral gastrocnemius and tibialis anterior muscles at T10 (both muscles, P ≤ .0001) and T30 (both muscles, P ≤ .0001). In all patients, the injected lateral gastrocnemius compound muscle action potential percentage area decreased significantly after botulinum neurotoxin type A injection and remained low on days 10 (P = .019) and 30 (P = .001), whereas the uninjected lateral gastrocnemius M-wave area remained unchanged from day 0 to day 30. Similarly, the injected tibialis anterior compound muscle action potential percentage area decreased significantly after botulinum neurotoxin type A injection and remained low on days 10 (P = .005) and 30 (P = .002), whereas the uninjected side tibialis anterior compound muscle action potential area remained unchanged from day 0 to day 30 (Figure 1A). Traces collected on the treated side showed a clear decrease in the tibialis anterior and lateral gastrocnemius compound muscle action potential areas; on the untreated side, although the tibialis anterior and lateral gastrocnemius compound muscle potential areas were unchanged after botulinum neurotoxin type A injections, we showed waveform changes due to a small difference in electrode location and orientation during the 3 recording sessions (Figure 1B). Calf circumference was similar on both sides in all patients (treated side, 21.2 ± 0.6 cm [mean ± standard error]; untreated side, 22.5 ± 0.9 cm).
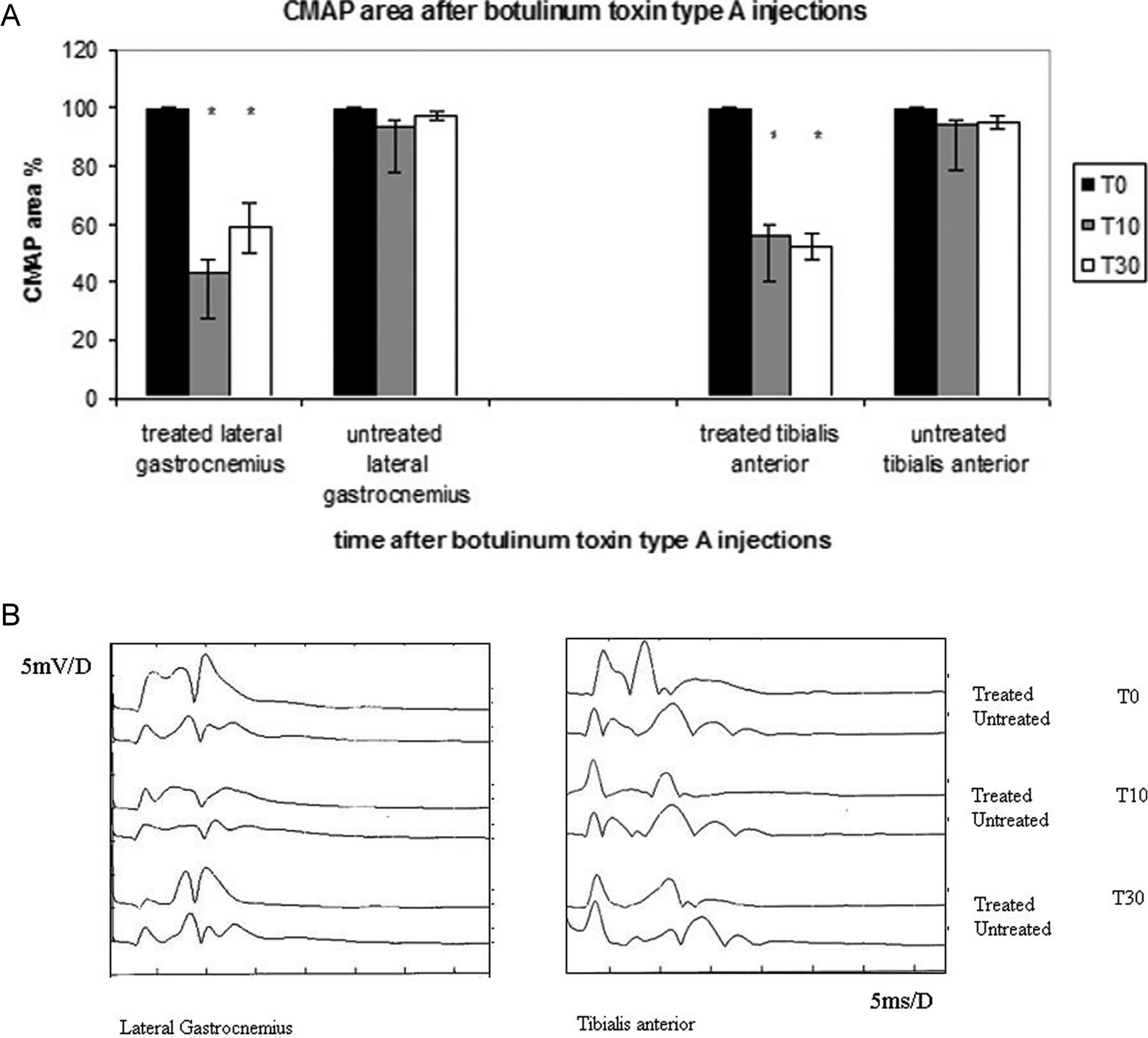
(A) Histogram representing the compound muscle action potential (CMAP) area of lateral gastrocnemius and tibialis anterior muscles before and after treatment with botulinum toxin type A on the treated and untreated sides. (B) Traces showing the compound muscle action potential area from the lateral gastrocnemius and tibialis anterior muscles before and after botulinum toxin injected in the gastrocnemius muscle at T0, T10, and T30 in a patient.
The Modified Ashworth Scale score at the ankle joint on the treated side was significantly reduced after treatment (T10, P = .001; T30, P = .002). R1 angle in the modified Tardieu scale assessed at the ankle joint, with the knee extended, on the treated side improved significantly after treatment (T10, P = .03; T30, P = .02). R2 angle did not significantly change after treatment. The dynamic component of spasticity (R2-R1) was 19.1° ± 2.6° at baseline and was significantly reduced after treatment (T10, 14.2 ± 2.1, P = .03; T30, 14.1 ± 2.0, P = .02). No differences were found in ankle spasticity and passive range of motion on the untreated side before and after botulinum neurotoxin type A injections. At baseline, Edinburgh Visual Gait Scores were significantly higher on the treated side and decreased significantly after treatment (T10, P = .04; T30, P = .02), whereas scores for the untreated side remained statistically unchanged (Figure 2).
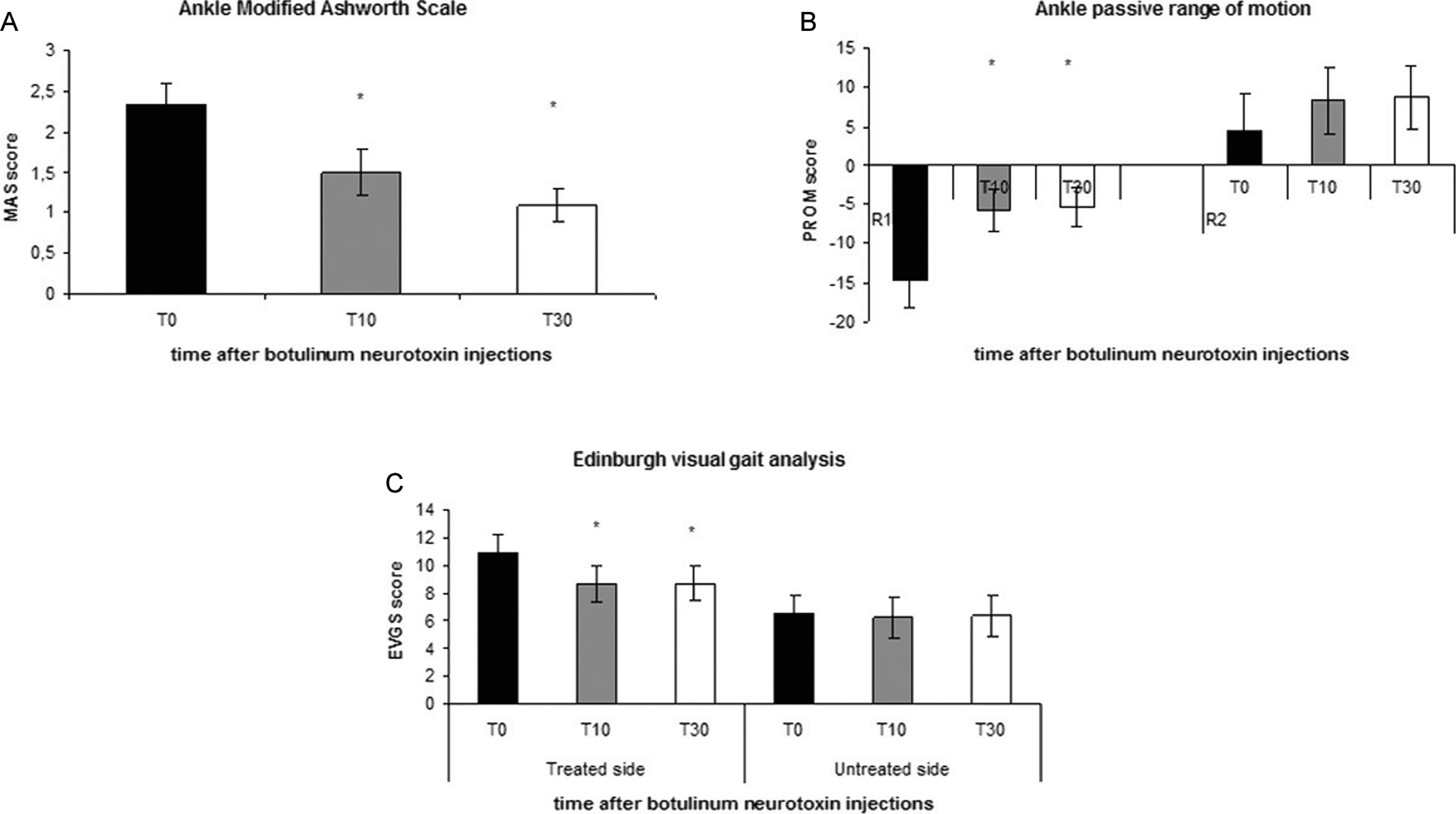
(A) Modified Ashworth Scale, (B) passive range of motion for R1 and R2 for the treated side, and (C) Edinburgh Visual Gait Score at T0, T10, and T30.
No significant correlation was found between the total toxin dose, calf circumference, compound muscle action potential area and changes in passive range of motion, Edinburgh Visual Gait Score, and Modified Ashworth Scale score. Spearman test also showed a nonsignificant correlation between the toxin dose and the decrease in tibialis anterior compound muscle action potential area (R = .19) or calf circumference and the decrease in tibialis anterior compound muscle action potential area (R = .17). None of the treated children or their parents reported adverse effects at the injection sites or generalized weakness after botulinum neurotoxin type A injections.
Discussion
In this study, after we injected botulinum neurotoxin type A into the posterior calf muscles in children with dynamic equinus foot, the toxin spread to surrounding antagonist muscles and induced chemodenervation in injected muscles. The standard, recommended botulinum neurotoxin type A doses we injected in this study induced this dual effect in all the 18 children with cerebral palsy we treated. Despite, or possibly thanks to local toxin spread, after receiving botulinum neurotoxin type A injections, all the children found their gait had improved.
Besides confirming the effectiveness of botulinum neurotoxin type A injections for children with cerebral palsy, our study therefore provides new neurophysiological evidence showing that even when injected at doses similar to or lower than the standard or recommended dose of 15 to 20 U/kg, Dysport (Ipsen) 14 botulinum neurotoxin type A spreads from the treated spastic gastrocnemius to the antagonist tibialis anterior muscle. Neurophysiological proof of chemodenervation due to botulinum neurotoxin type A spread to the surrounding anterior leg muscle came from the decreased compound muscle action potential area from the tibialis anterior muscle. The toxin spread even when we minimized the effect of muscle size by subdividing the total dose for each leg according to the calf diameter.
Our observation that botulinum neurotoxin type A spread to surrounding anterior leg muscles, and at the same time our patients’ gait improved, needs careful interpretation considering current knowledge. Spread to antagonist muscles is generally considered a limitation to the effectiveness of botulinum neurotoxin, and spread to the antagonist tibialis anterior muscle could limit gait improvement in children with equinus foot. 10 Some investigators using the toxin at very high doses nevertheless reported its safety and effectiveness in treating children with spasticity and found, as we did, that gait improved.5,15,16,18 Some found a dose-response (Botox [Allergan, Irvine, CA] 200 vs 100 U per leg and 40 vs 20 U per leg muscle belly ) 5 relationship without a plateau, whereas others found no dose-response relationship (Botox [Allergan] 15-25 U/kg vs 5-15 U/kg) 16 or did not report on a dose-response (Botox [Allergan] 15-40 U/kg 15 or Botox ≥800 U18) effect. Hence, current knowledge from many studies suggests that high doses of botulinum toxin seem safe and efficacious in improving spasticity and gait.
A possible concern is that the toxin has a plateau effect in children. In a study describing children with cerebral palsy treated with Dysport (Ipsen) doses ranging from 8 to 24 U/kg body weight, Polak and coworkers 10 found that in all children, gastrocnemius muscle length improved. As we did, they found a nonlinear correlation between dose and clinical response and suggested that motor end plates saturated in the target muscle. 10 The number of end plates is constant from birth and does not vary with body weight. 10 Our findings that the toxin invariably spread to neighboring muscles suggest that motor end plates saturate and the toxin spreads at standard doses. Another finding underlining the difficult balance between the beneficial effects induced by botulinum neurotoxin type A and toxin spread comes from a study in adult patients showing that high botulinum neurotoxin type A doses can lead to overweakening in some individuals and no improvement in most gait measures. 36
Given that in all the children with dynamic equinus foot we treated, the toxin invariably spread to antagonist leg muscles, the mechanism underlying the gait improvement in children with dynamic equinus foot remains unclear. We conjecture, in line with others, 10 that botulinum neurotoxin type A injected into the gastrocnemius muscle brought about a functional improvement in our patients’ spasticity and gait despite drug spreading. A reason that might explain why botulinum neurotoxin type A injections improved our children’s spasticity and gait problems is that the toxin, by altering reflex activity and the force of contraction, influences the development of central circuitry remodeling indirectly. In theory, therapy for spasticity, especially early therapy, could break the cycle muscle hyperactivity, pain, fibrosis, and contracture, thus influencing remodeling in central circuits 37 and leading to a relearning of gait balance.
Although an increasing number of reports describe botulinum toxin used at high doses,5,10,15–18 until the role of botulinum neurotoxin type A spread in children with spasticity is clarified, we suggest that very high doses should be used with care, given botulinum neurotoxin type A’s local physiological effect, the risk of regional and general spread, the need for a progressive treatment strategy, the variability in effects, and the cost of treatment, as Rousseaux et al suggest. 11 Follow-up assessment after botulinum neurotoxin type A injections should include monitoring the compound muscle action potential area in posterior and anterior leg muscles and investigating possible regional botulinum neurotoxin type A spread to other antagonist muscles.
Our study has limitations. First, it is a short-term neurophysiological study, which did not investigate the possible long-term clinical features of gait changes in children. Second, a larger patient sample might yield a correlation between calf circumference and decrease in tibialis anterior compound muscle action potential area after toxin injection, thus allowing the rate of spread to be more accurately calculated.
Future research should be designed to compare very high doses versus low doses of botulinum toxin and undertake neurophysiological assessment to monitor spread and evaluate whether spread limits or interferes with the toxin’s effectiveness or is inherent to successful treatment with botulinum toxin in children with dynamic equinus foot.
Footnotes
All authors had full access to all the data and the accuracy of the data analysis. Study concept and design: EF, ED, and LB. First authors who contributed equally to the work: EF, ED, and LB. Acquisition of data: EF, ED, FB, and PT. Analysis and interpretation of data: EF, FB, PT, and GD. Drafting of the article: EF and PT. Critical revision of the article for important intellectual content: EF, LB, GD, DP, and AF. Statistical analysis: MB. Administrative, technical, or material support: FB, PT, and SV. Study supervision: LB.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The local ethical committee and the institutional review board of the University of Verona approved the study.
The authors received no financial support for the research, authorship, and/or publication of this article.