
Abstract
The authors previously reported on the initial manifestations in a set of female twins, who presented soon after birth with bath-induced paroxysmal events each time they were immersed in a warm water bath. These episodes progressively ceased by the age of 36 months, replaced by paroxysmal episodes of alternating hemiplegia unrelated to water immersion. By age 4 years, the twins developed the classic features of alternating hemiplegia of childhood. Clinical outcomes at the age of 11 years are now reported. Standard and video-electroencephalograms showed a large, slow background activity followed by lower amplitude waves without focal abnormalities or other abnormal findings. This represents the first report on (a) alternating hemiplegia of childhood started with bath-induced paroxysmal episodes; (b) this condition in monozygotic twins; and (c) an 11-year follow-up study in which the twins continue to experience episodes of alternating hemiplegia in the setting of baseline cognitive impairment without epileptic episodes.
Alternating hemiplegia of childhood is a rare disorder that usually commences before 18 months of age. 1,2 Clinically, the patients present with paroxysmal episodes of motor failure (repeated attacks of hemiplegia involving either side of the body), movement disorders (tonic or dystonic episodes), autonomic phenomena, and ocular manifestations. Developmental delay, psychomotor regression, and/or behavioral disorders may ensue. 3,4
We previously reported on the initial manifestations of a set of monozygotic twins who had paroxysmal events triggered by warm water bathing since their first few days of life. 5,6 The twins are currently aged 11 years and since the age of 4 years have developed the classical syndrome of alternating hemiplegia of childhood. The present observation shows that alternating hemiplegia of childhood may manifest as warm water bath–induced paroxysmal events beginning at a few days of life, and the report provides longer term follow-up of the twins, who at age 11 years continue to experience typical episodes of alternating hemiplegia and have associated cognitive impairment.
Case Summary
These female monozygotic twins were born by caesarean section to unrelated, healthy Italian parents after a full-term pregnancy. The mother denied infectious diseases during the pregnancy and had taken no drugs. The birth weights, lengths, and head circumferences of the twins were in the normal range. As recalled by their mother, since the age of 3 days, the twins had paroxysmal attacks each time they were immersed in the warm water of a bath. These paroxysmal episodes never occurred (since their onset and over the years) during sea immersion or cold-water contact. The attacks consisted of irritability, unprovoked smiles, fixed stares, head deviation, upper limb hemi- and hypertonia, guttural sounds, and noisy breathing. These paroxysmal episodes, which lasted from seconds to a few minutes and ceased with a cry, were initially underestimated by the parents and family doctors and considered to be anomalous but not serious events. 5,6 Repeated standard electroencephalogram recordings were made during several attacks, which showed long phases of discharges of large, slow background activity followed by lower amplitude waves without focal abnormalities or other abnormal findings (Figure 1A-1C); during sleep (Figure 1D, 1E) these phases decreased, giving way to longer phases of normal background activity.
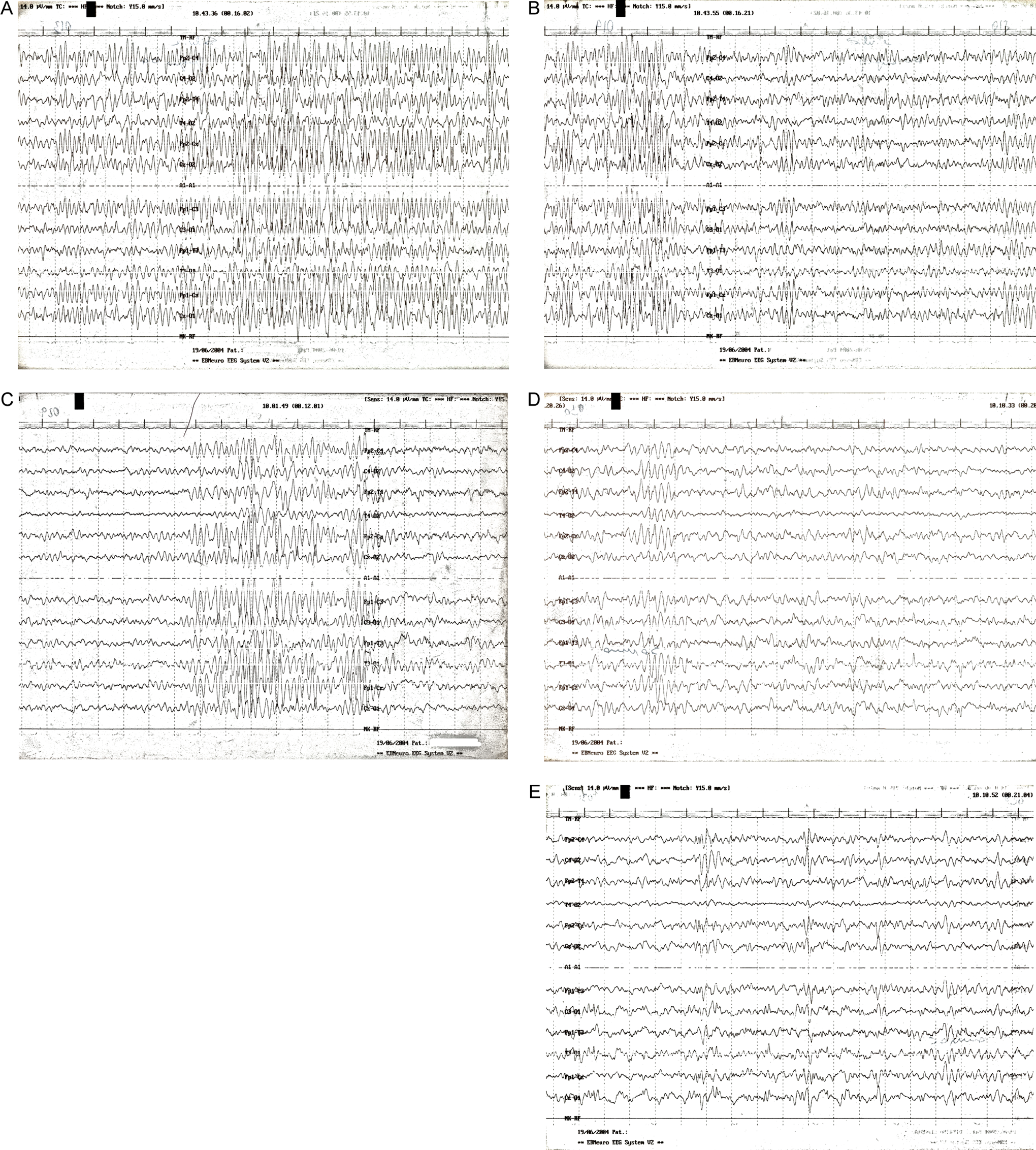
Standard electroencephalograms obtained at age 25 months during an unprovoked episode show (twin 1, A and B; twin 2, C) long phases of discharges of large, slow background activity followed by lower amplitude waves without focal abnormalities or other abnormal findings; during sleep (twin 1, D; twin 2, E) these phases decreased, giving way to longer phases of normal background activity.
The twins first came to our attention in the University Department of Clinical Paediatrics in Catania, Italy, at the age of 25 months. At that time, we personally observed the bath-induced bouts. Standard electroencephalograms recordings in the interictal phase showed the presence of background slowing and generalized slowing (Figure 2A, 2B). Repeated standard electroencephalograms recorded a few days after were normal (Figure 2C, 2D).
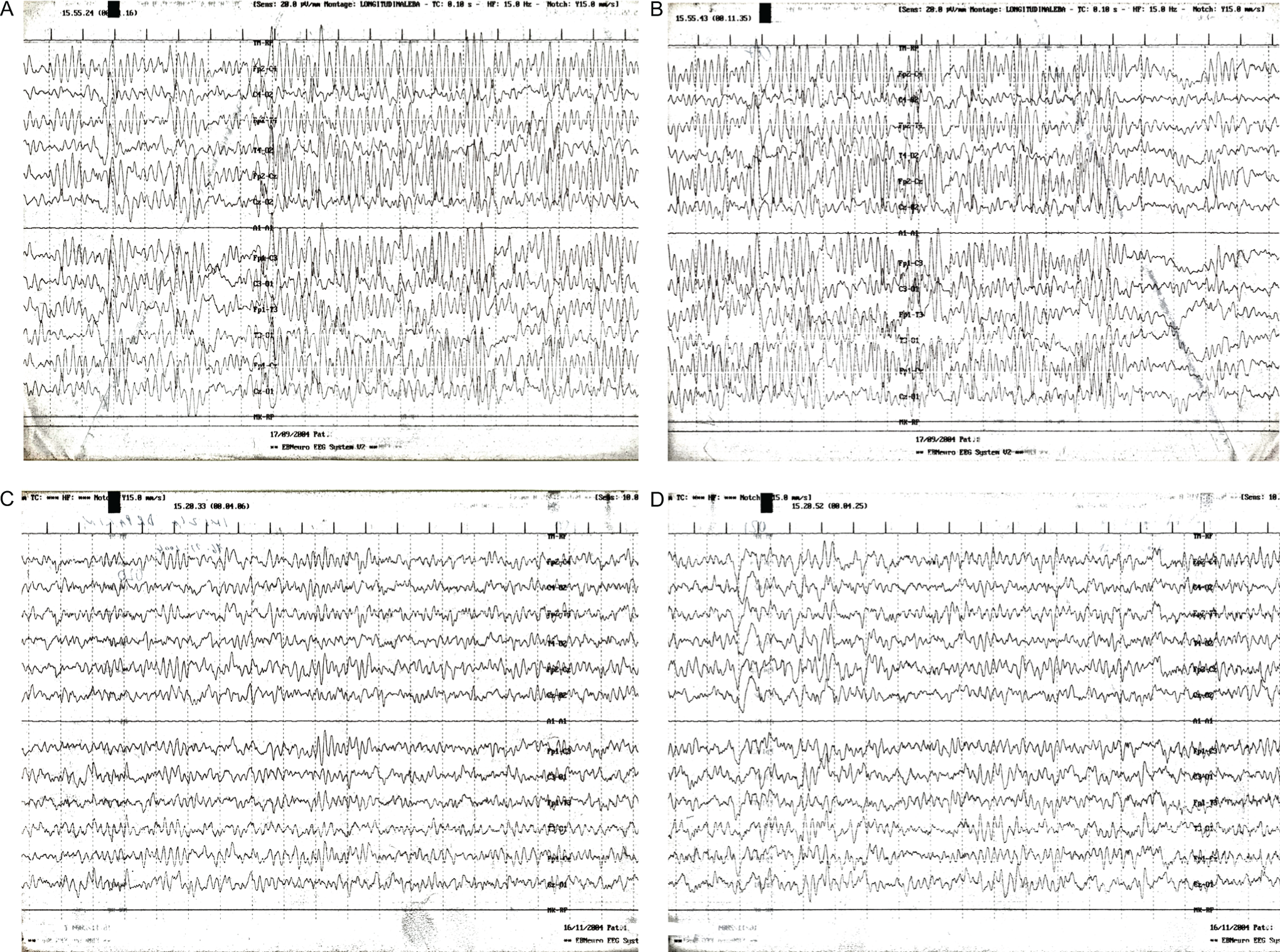
Standard electroencephalograms made during a provoked attack (see text) show long phases of discharges of large, slow background activity followed by lower amplitude waves without focal abnormalities or other abnormal findings (twin 1, A; twin 2, B). Repeated electroencephalograms recorded a few days after are normal (twin 1, C; twin 2, D).
Since 36 months of age, both girls experienced long-lasting (eg, nearly all day) but also brief (from a few minutes to 1 or 2 hours) paroxysmal bouts of hemiplegia unrelated to water immersion. Confusion, autonomic disturbances (eg, salivation and hot flashes), speech arrest, ataxia, intermittent oculomotor paroxysms, and attacks of dystonia of the hands were recorded. All of these current bouts occurred mainly within one type of episode, were aborted by sleep, and typically reappeared 10 to 20 minutes after awakening. Repeated strandard electroencephalograms recordings in the interictal phase showed the presence of generalized, slow background activity with a phase of high voltage without focal anomalies (Figure 3A-3C).
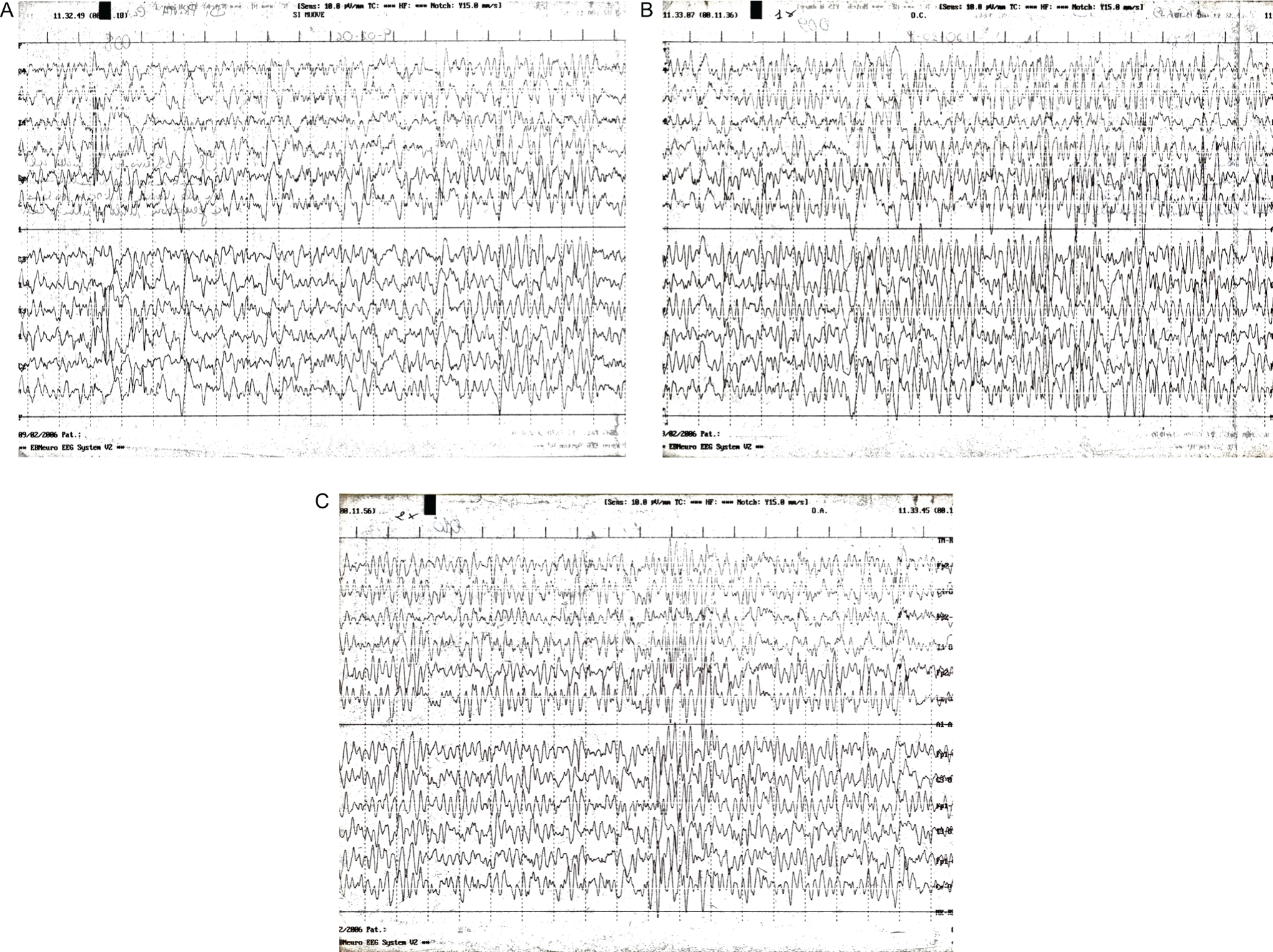
Repeated standard electroencephalograms obtained at age 36 months (twin 1, A and B; twin 2, C), when the twins started to have paroxysmal bouts of hemiplegia unrelated to water immersion, in the interictal phase show the presence of generalized, slow background activity with a phase of high voltage without focal anomalies.
At the age of 4 years, the diagnosis of alternating hemiplegia of childhood was made. At that age, the twins were hyperactive during their daily activities and manifested oppositive and emotionally unstable behavior with their family members and with their peers. As these episodic attacks persisted, the twins were enrolled in the Italian Registry of alternating hemiplegia of childhood and were started on treatment with topiramate (75 mg/day) and later with flunarizine (5 mg/day), 7,8 which were discontinued because of the appearance of side effects (including fatigue, confusion, and somnolence) and of incomplete control of symptoms.
At clinical follow-up at the age of 7 years, the twins exhibited moderate mental delay with a full-scale IQ measured at 53 and 55, respectively (verbal IQ scored at 64 and 67, performance IQ scored at 50 and 51, respectively; the ▵ verbal IQ/performance IQ ratio was 15). At different times, routine laboratory investigations and metabolic screening were performed for blood lactate and pyruvate, glucose, plasma amino acids, acylcarnitine, thyroid hormones, urine organic acids, neurotransmitters, and protein metabolites in the cerebrospinal fluid. Magnetic resonance imaging (MRI) and magnetic resonance angiography were normal. In both twins, analyses for mutations in the alternating hemiplegia of childhood ATP1A2 (α-2 isoform of sodium-potassium-adenosine triphosphatase) gene were negative.
Currently older than 11 years, the twins meet the clinical diagnostic criteria for alternating hemiplegia of childhood. No convulsive episodes were recorded during the entire follow-up period. The follow-up standard electroencephalograms were similar in both twins and showed a large, slow background activity followed by lower amplitude waves without focal abnormalities or other abnormal findings (Figure 4). Both twins are currently under no treatment with a spontaneous reduction in frequency and intensity of bouts with 1 to 2 attacks every 3 to 4 months.
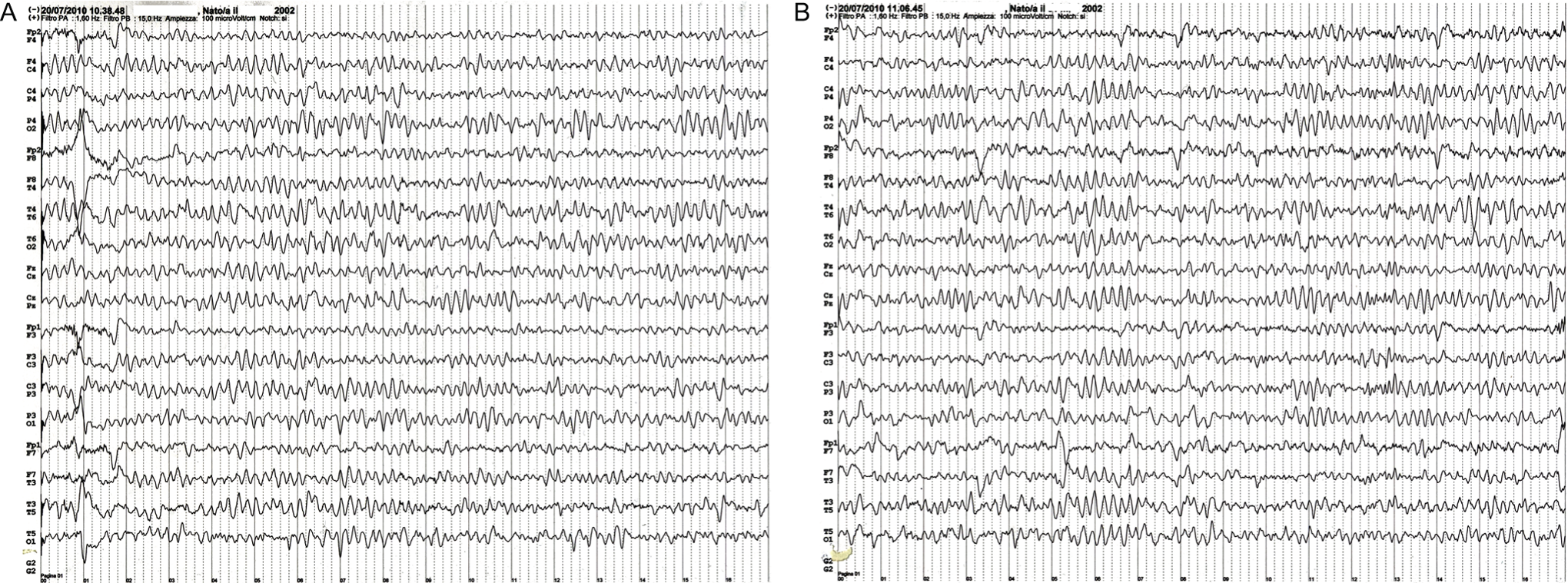
Follow-up standard electroencephalograms recorded at the current age of older than 11 years were similar in both twins (twin 1, A; twin 2, B) and showed no focal abnormalities with a normal background activity.
Discussion
These monozygotic twins have had episodic attacks of (warm water) bath–induced paroxysmal disorders since the neonatal period.
Recently, Sweney et al 2 reported a collaborative study on 103 patients affected by alternating hemiplegia of childhood and found that paroxysmal ocular movements are the earliest and most suggestive signs of alternating hemiplegia of childhood since these abnormal ocular movements are present in 83% of patients in the first 3 months of life, followed by hemiplegic episodes, which appear by 6 months of age in 56% of those affected. In the cases reported by Sweney et al, 2 distinct convulsive episodes were frequently reported together with ataxia and cognitive impairment in almost all of the cases. However, no case was reported that had early onset of seizures or bathing-induced episodes similar to the cases herein reported. 1 –4,7,8
In the twins reported here, the clinical course was unusual but identical in each twin. The episodes began when the twins were immersed in the warm water of a bath beginning in the first few days of life; notably, since their onset and over the years, the paroxysmal episodes have never occurred during sea immersion or cold-water contact. 9 -15 These were the main symptoms until 3 years of age, when the episodes began to manifest with different features. The attacks were unrelated to water immersion and were of different durations but always associated with alterations in consciousness, oculomotor paroxysms, and dystonia localized in the hands with no overt convulsive episodes in either twin. The cognitive delay and behavioral impairment were recorded at about 7 years of life and were of a less severe intensity than usually recorded in the cases of alternating hemiplegia of childhood that we followed within the Italian registry of alternating hemiplegia of childhood. Repeated video-electroencephalograms showed generalized slow background activity with a phase of high voltage without focal anomalies. The brain MRI studies in our twins, as usually reported in the cases in the literature, 2 -4 were normal.
These cases are noteworthy as they demonstrate that alternating hemiplegia of childhood may manifest by bath-induced bouts and also as they represent the first example of a family with affected monozygotic twins and the first cases of neonatal onset of bath-induced alternating hemiplegia of childhood. The current clinical manifestations consist of cognitive impairment with no epileptic episodes.
Footnotes
GI, PP, and LP followed the twins since their first referral to our institutions in Italy. They wrote the initial observations (as reported in Epilepsy Research and European Journal of Paediatric Neurology), recorded and commented on all their standard electroencephalograms, and drafted and redrafted all the versions of the present manuscript. MC followed the twins by obtaining and commenting on all their standard and video-electroencephalograms. She drafted and redrafted the neurophysiology sections in the present and previous manuscripts. MP was called as a consultant during one of his lectures at our department to see and give his expert opinion on this set of twins. He saw and commented on all the electroencephalographic recordings and followed-up on the case (from the United States). He drafted and redrafted the present (and previous) studies and edited all versions for language. AP was called as consultant regarding the diagnosis of alternating hemiplegia in childhood as coordinator of the Italian guidelines on alternating hemiplegia in childhood for the Superior Institute of Health. She contributed to the diagnosis, followed the twins after age 4 years, and drafted and redrafted the present manuscript. MR followed the twins clinically, conceived and made the first draft, and drafted and redrafted the present and previous manuscripts, coordinating the group of coauthors in Italy and United States.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.
This study was reviewed and approved by the Ethic Committee at the University Hospital Policlinico-Vittorio Emanuele in Catania, Italy, during the years 2006, 2008, and 2011.