
Abstract
In children with benign childhood epilepsy with centrotemporal spikes, centrotemporal spikes may cause language dysfunction via disruption of underlying functional neuroanatomy. Fifteen patients with benign childhood epilepsy with centrotemporal spikes and 15 healthy controls completed 3 functional magnetic resonance imaging (MRI) language paradigms; standardized cognitive and language assessments were also performed. For all paradigms, children with benign childhood epilepsy with centrotemporal spikes showed specific regional differences in activation compared to controls. Children with benign childhood epilepsy with centrotemporal spikes also differed from controls on neuropsychological testing. They did not differ in general intelligence, but children with benign childhood epilepsy with centrotemporal spikes scored significantly lower than controls on tests of language, visuomotor integration, and processing speed. These results extend previous findings of lower language and cognitive skills in patients with benign childhood epilepsy with centrotemporal spikes, and suggest epilepsy-related remodeling of language networks that may underlie these observed differences.
Keywords
About 15% of all children with epilepsy have benign childhood epilepsy with centrotemporal spikes. This epilepsy syndrome is characterized by relatively infrequent brief, simple partial, hemifacial motor seizures with somatosensory symptoms; secondary generalization to tonic-clonic seizures is common. The electroencephalogram (EEG) typically shows blunt, high-voltage, centrotemporal spikes often followed by slow waves activated by sleep and that may spread or shift in lateralization. 1 Benign childhood epilepsy with centrotemporal spikes is traditionally assumed to have a relatively benign course with likely cessation of seizures by adulthood, regardless of seizure frequency.2–6
Despite this “benign” prognosis for seizures, recent studies have documented lower levels of cognitive skills in children with benign childhood epilepsy with centrotemporal spikes.7–11 In particular, language deficits have been shown to persist even when children were in remission.12,13 Furthermore, one recent study reported that language deficits may appear as a precursor to the diagnosis of benign childhood epilepsy with centrotemporal spikes. 14 In addition to the effects on cognitive performance, a few studies conducted more specific analyses focusing on the effects of epileptiform discharges on cognitive functioning.15–17 These studies related the lateralization of centrotemporal spikes to particular profiles of cognitive deficits, and their results suggest that it may not only be seizures but also the epileptiform discharges that disrupt typical cortical networks supporting language and other neurocognitive abilities. Some children with benign childhood epilepsy with centrotemporal spikes exhibit normal cognitive and language functions, but as in other epilepsy syndromes, different neurophysiologic compensatory strategies may underlie the maintenance of these functions. 18 Thus, despite its “benign” character, many children with benign childhood epilepsy with centrotemporal spikes may suffer long-term cognitive consequences.
The motivation for this study was the hypothesis that patients with benign childhood epilepsy with centrotemporal spikes will show performance on neuropsychological testing of language functions that is lower than that of controls and that these differences are associated with atypical language distribution as documented by a battery of 3 functional magnetic resonance imaging (functional MRI) tasks designed to evaluate left, bilateral, and right language circuits respectively. 19
Methods
All study procedures were approved by Cincinnati Children’s Hospital Medical Center Institutional Review Board.
Participants
Fifteen patients with clinical presentation consistent with benign childhood epilepsy with centrotemporal spikes (ages 6-13, mean age 8.7, 2 females) were recruited from the New Onset Seizure Clinic at Cincinnati Children’s Hospital Medical Center. These children had a history of 1 to 4 seizures at time of participation and displayed an EEG pattern consistent with typical benign childhood epilepsy with centrotemporal spikes; 5 were taking antiepileptic medications (3 carbamazepine, 1 gabapentin, and 1 levetiracetam). Patient data are included in Table 1. Fifteen healthy children (ages 7-14, mean age 9.2; 6 females) participated in the study (Table 1). All patients and controls were right-handed (based on parent report), native speakers of English with no history of neuropsychological or learning disorders (also based on parent report). Informed consent was obtained from a parent/guardian for all participants, including child assent from participants aged 11 years and older, using consent/assent forms approved by Cincinnati Children’s Hospital Medical Center Institutional Review Board.
Clinical Characteristics of Children With Benign Childhood Epilepsy With Centrotemporal Spikes.
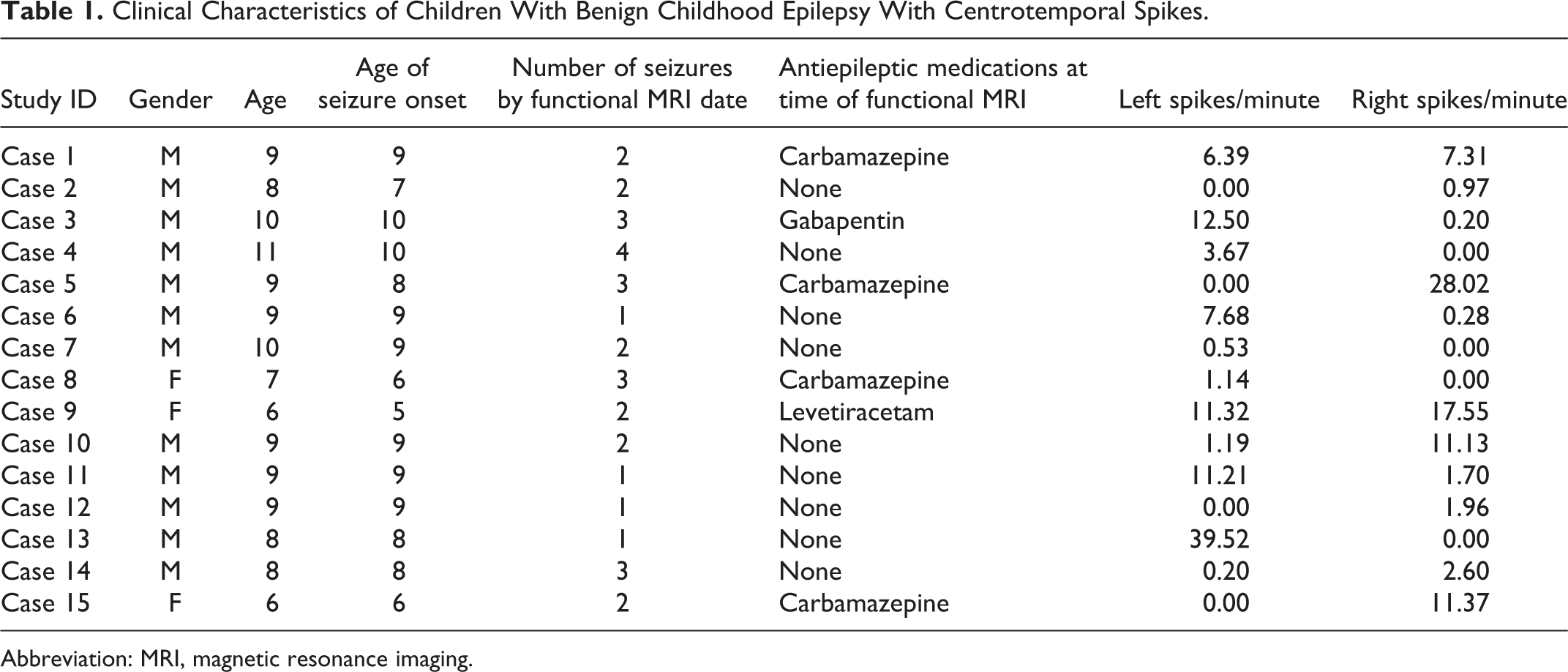
Abbreviation: MRI, magnetic resonance imaging.
Electroencephalographic Evaluation—Benign Childhood Epilepsy With Centrotemporal Spikes
Clinical routine EEG recordings were reviewed by 2 epileptologists (authors DM and JPS). Frequency and lateralization of epileptiform discharges (centrotemporal spikes) was determined based on each patient’s last available clinical EEG recording (duration range 25-47 minutes). Although sleep state was not taken into consideration in the present analysis, all patients exhibited centrotemporal spikes during wakefulness. Nine of the 15 patients slept for some part of their EEG recording (1.2-13.0 minutes), and 8 of these 9 exhibited centrotemporal spikes during sleep. Centrotemporal spikes were counted by visual analysis and noted as originating from left or right centrotemporal regions. Counts from the 2 reviewers did not differ by more than 10% for any patient, and the mean of the 2 counts was used for analysis. Seven patients showed a preponderance of left-sided spikes (at least 87% left), 6 patients showed a preponderance of right-sided spikes (at least 61% right), and 1 patient showed a symmetric (47% left vs 53% right) distribution (Table 1). Frequency of spikes ranged from 0.97/min to 39.5/min (mean 9.0/min).
Neuropsychological Evaluation
Children with benign childhood epilepsy with centrotemporal spikes and controls were administered the Wechsler Abbreviated Scale of Intelligence 20 to measure general intelligence. Language skill assessments included the phonological awareness and rapid naming subtests of the Comprehensive Test of Phonological Processing, 21 and core subtests of the Clinical Evaluation of Language Fundamentals. 22 Nonlanguage testing was included to assess visuospatial skill and general speed of processing: the Developmental Test of Visuomotor Integration 23 and symbol search and coding subtests. 24 Not all participants completed all testing; the numbers of patients and controls for whom scores were obtained are included in Table 2.
Neuropsychological and Behavioral Scores, and Functional MRI Lateralization Indices for Children With Benign Childhood Epilepsy With Centrotemporal Spikes (BECTS) and Controls.
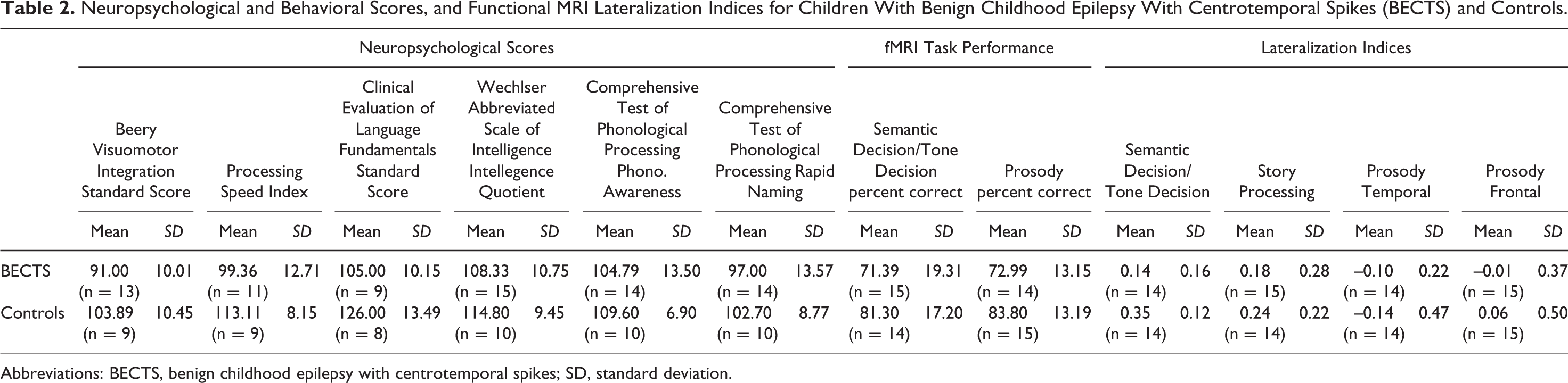
Abbreviations: BECTS, benign childhood epilepsy with centrotemporal spikes; SD, standard deviation.
Functional MRI Tasks
Semantic decision/tone decision
This is a child-friendly version of the task originally introduced by Binder et al. 25 In this task, participants heard single-word animal names, 1 presented every 5 seconds. Participants were instructed to make a button-press response if the item had target semantic properties, specifically, that the animal has 4 legs. This stimulus was alternated with a tone decision task where participants responded with a button-press to a target sequence of tones. Each condition was repeated 5 times with stimuli (either tones or words) presented every 5 seconds with 8 stimuli per block, resulting in a 40-second interval for each block. This task was completed in 6 minutes 40 seconds. Performance data from button-press responses were recorded.
Story processing
26,27 This task used a 30-second alternating block design in which a different story, read by an adult female speaker, was presented during each active period. Each story, designed by a speech-language pathologist to be appropriate for children aged 5 years and older, contained 10 sentences with a variety of syntactic constructions. During the control epochs, 1-second duration tones were presented at random frequencies (400-2500 Hz) and intervals (1-3 s), to control for sublexical auditory processing. Six blocks of control stimuli and 5 blocks of active were presented for a total scan time of 5 minutes 30 seconds.
Prosody discrimination
In this task, participants were presented with audiovisual sentence stimuli and indicated with a button press whether the sentence is a statement or question. The sentences did not include interrogative words, so the decision regarding whether the sentence is a question or statement was based on prosody alone. Thirty sentences of each type were presented in blocks of 5 with each block 55 seconds in duration, with 11-second instruction periods between blocks. Prosody discrimination alternated with a control semantic judgment task, where participants indicated whether the sentence discussed a person. This control task includes the same sentence materials as the active task, again arranged into blocks of 5 sentences. The order of presentation was counterbalanced so that identical sentence stimuli were used once in the prosody discrimination task and once in the semantic task. This task was completed in 13 minutes 12 seconds.
Functional MRI Methods
The 3 functional MRI paradigms were included in the scan session for each participant. Six children with benign childhood epilepsy with centrotemporal spikes and 3 control participants were scanned on a 3 T Bruker Biospec 30/60 MRI scanner (functional MRI parameters: TR/TE = 2000/38 ms, FOV 25.6 × 25.6 cm, matrix 64 × 64, slice thickness = 5 mm, resulting in a voxel size of 4 × 4 × 5 mm, 25 axial slices; for story processing TR = 3000 ms). Remaining participants were scanned on a 3 T Philips Achieva MRI scanner with the same parameters (except slice thickness was reduced to 4 mm, 28 slices were acquired). For prosody discrimination, we used a sparse acquisition functional MRI sequence where 6-second periods of scanner quiescence alternate with periods of 6-second image acquisitions. Presentation of auditory sentence stimuli takes place during quiet periods. When functional image data are collected after each stimulus, it is at the peak of the hemodynamic response to the preceding stimulus (see Schmithorst and Holland 28 for details). Magnetic resonance imaging data analysis was performed using routines written in Interactive Data Language (ITT Visual Information Solutions, Boulder, CO). The echo planar images were corrected for Nyquist ghosts and geometric distortion using the multiecho reference method. To correct for motion, each echo planar image data set was coregistered to the image volume, 29 which minimized a cost function based on variation in image intensity over the entire data set. 30 After spatial normalization into Talairach space, a general linear model and paired t test were implemented to identify voxels activated by each task for each participant. Random-effects analysis was performed to determine significant group activations in the Talairach space. Group activations for patients and controls and comparisons between groups were thresholded at z > 7 with cluster size > 30 and corrected via Monte Carlo simulation for a significance level of P <.05. (Single-group activations for prosody discrimination did not reach significance at this corrected level and were thresholded at z > 6.25 with cluster size 20.) No significant differences were observed between data collected on the 2 MRI scanners when the data from both were directly contrasted for signal distribution and intensity.
Lateralization index
Lateralization indices were calculated in functionally defined regions of interest. These were defined for each task, based on areas of activation in the composite maps of the control group combined as a union with areas of activation in the patient group for each task. These regions of interest were projected onto both hemispheres for purposes of laterality calculation. Voxels with z scores greater than or equal to the median z score (resulting from the task > baseline contrast in each task) within a region of interest for each individual participant were used in the calculation of the lateralization index for that individual. Voxels above this median z score threshold were counted, and a lateralization index was defined as the difference in the number of activated voxels, summed independently for the left and right regions of interest, divided by the sum of active voxels in the left plus the right regions of interest. This procedure yields lateralization indices ranging from –1 (right) to 1 (left) 31 ; we consider a lateralization index with a value greater than 0.1 or less than –0.1 as clearly defined lateralization.32–34 Conversely, the lateralization of an individual is considered bilateral if it falls between –0.1 and 0.1.
Results
Neuropsychological/Behavioral Results
Intelligence test scores in children with benign childhood epilepsy with centrotemporal spikes were within the average range for Full-Scale Intelligence (range 93-124, mean 108), and did not differ from controls (range 99-128, mean 114; P = .14). However, children with benign childhood epilepsy with centrotemporal spikes, as a group, scored lower than controls on the Clinical Evaluation of Language Fundamentals, t(15) = 3.65, P = .002; the Developmental Test of Visuomotor Integration, t(20) = 2.92, P = .009; and Symbol Search and Coding subtests (measuring processing speed index), t(18) = 2.8, P = .012. Most children with benign childhood epilepsy with centrotemporal spikes performed in the average range on these tests, though 2 patients had standard scores lower than 80 on the Developmental Test of Visuomotor Integration. In addition, although the groups did not significantly differ on Comprehensive Test of Phonological Processing subtest scores, 2 children with benign childhood epilepsy with centrotemporal spikes had standard scores of 85 or below on the phonological awareness subtests, and 3 had standard scores of 85 or lower on the rapid naming subtests (the lowest score on either subtest among controls was 94). Mean scores are included in Table 2.
For semantic decision/tone decision and prosody discrimination, where in-scanner responses were recorded, children with benign childhood epilepsy with centrotemporal spikes performed less accurately than age-matched controls, though these differences did not reach significance. Mean accuracy on semantic decision/tone decision for the controls was 84%, whereas for children with benign childhood epilepsy with centrotemporal spikes it was 73% (P = .15); for prosody discrimination accuracy for the controls was 81%, for children with benign childhood epilepsy with centrotemporal spikes it was 71% (P = .15). These levels of performance are fairly consistent with the results of previous studies in healthy adults and epilepsy patients that used a similar semantic decision task.35–37
Functional MRI Results—Group Comparisons
Semantic decision/tone decision
In our healthy controls, significant regions of activations were found in the left inferior/middle frontal gyrus, extending into insula (Brodmann area 44/6/13), cingulate cortex (Brodmann area 32), and left supramarginal gyrus (Brodmann area 40), typical for this task (Figure 1a). Children with benign childhood epilepsy with centrotemporal spikes as a group, however, showed no significant regions of activation in the composite maps. When compared to control participants, they showed significantly increased activation in the right middle temporal gyrus/fusiform gyrus (Brodmann area 20/21) but had lower levels of activation in left frontal (Brodmann area 46/9), left supramarginal (Brodmann area 40), and cingulate regions (Brodmann area 23) (Figure 1b).
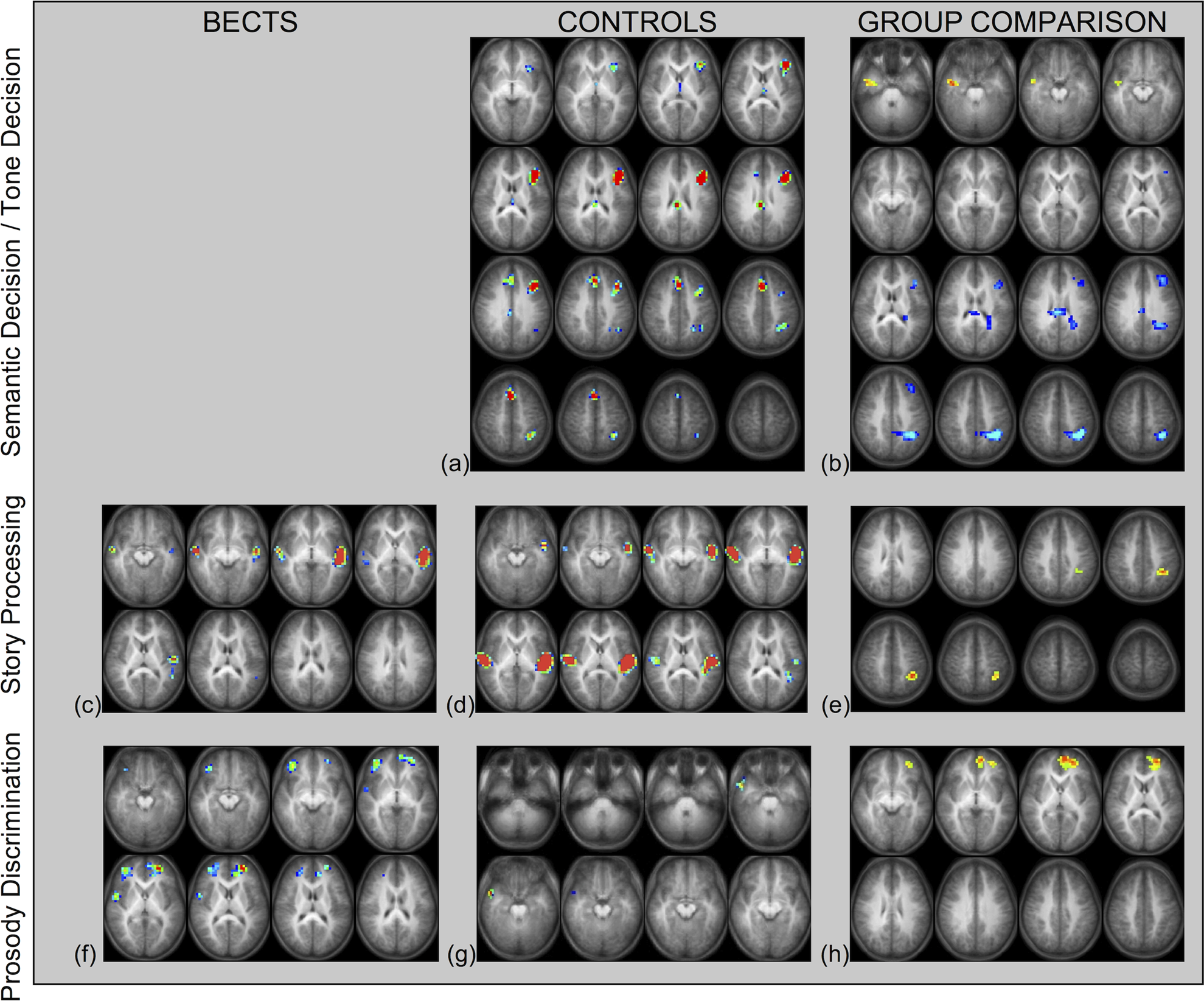
Top row: (1a) Group activation map for 14 control participants during semantic decision/tone decision task (group map is not included for children with benign childhood epilepsy with centrotemporal spikes because they did not show significant regions of activation in the group analysis). (1b) Group contrast map showing areas of increased activation for 14 children with benign childhood epilepsy with centrotemporal spikes indicated by hot colors, 14 controls by cool colors. Both z = 7, cluster size 30, P < .01, corrected. Middle row: (1c) Group activation map for 15 control participants during the story processing task. (1d) Group activation map for 15 children with benign childhood epilepsy with centrotemporal spikes during the story processing task. (1e) Group contrast map showing areas of increased activation for 15 children with benign childhood epilepsy with centrotemporal spikes. All z = 7, cluster size 30, P < .01, corrected. Bottom row: (1f) Group activation map for 14 control participants during the prosody discrimination task, z = 6.25, uncorrected, cluster size 20. (1g) Group activation map for 14 children with benign childhood epilepsy with centrotemporal spikes during the prosody discrimination task. (1h) Group contrast map showing areas of increased activation for 14 children with benign childhood epilepsy with centrotemporal spikes, z = 7, cluster size 30, P < .01 corrected. BECTS = benign childhood epilepsy with centrotemporal spikes.
Story processing
This task typically engages transverse temporal gyrus and planum temporale, with a larger intensity and extent of activation in the left hemisphere (Brodmann area 21/22/41/42). This typical pattern of activation was observed in our control group and in children with benign childhood epilepsy with centrotemporal spikes (Figure 1c/d). The main observed difference between the groups was an increase in left supramarginal gyrus (Brodmann area 40) for children with benign childhood epilepsy with centrotemporal spikes relative to healthy controls (Figure 2e).
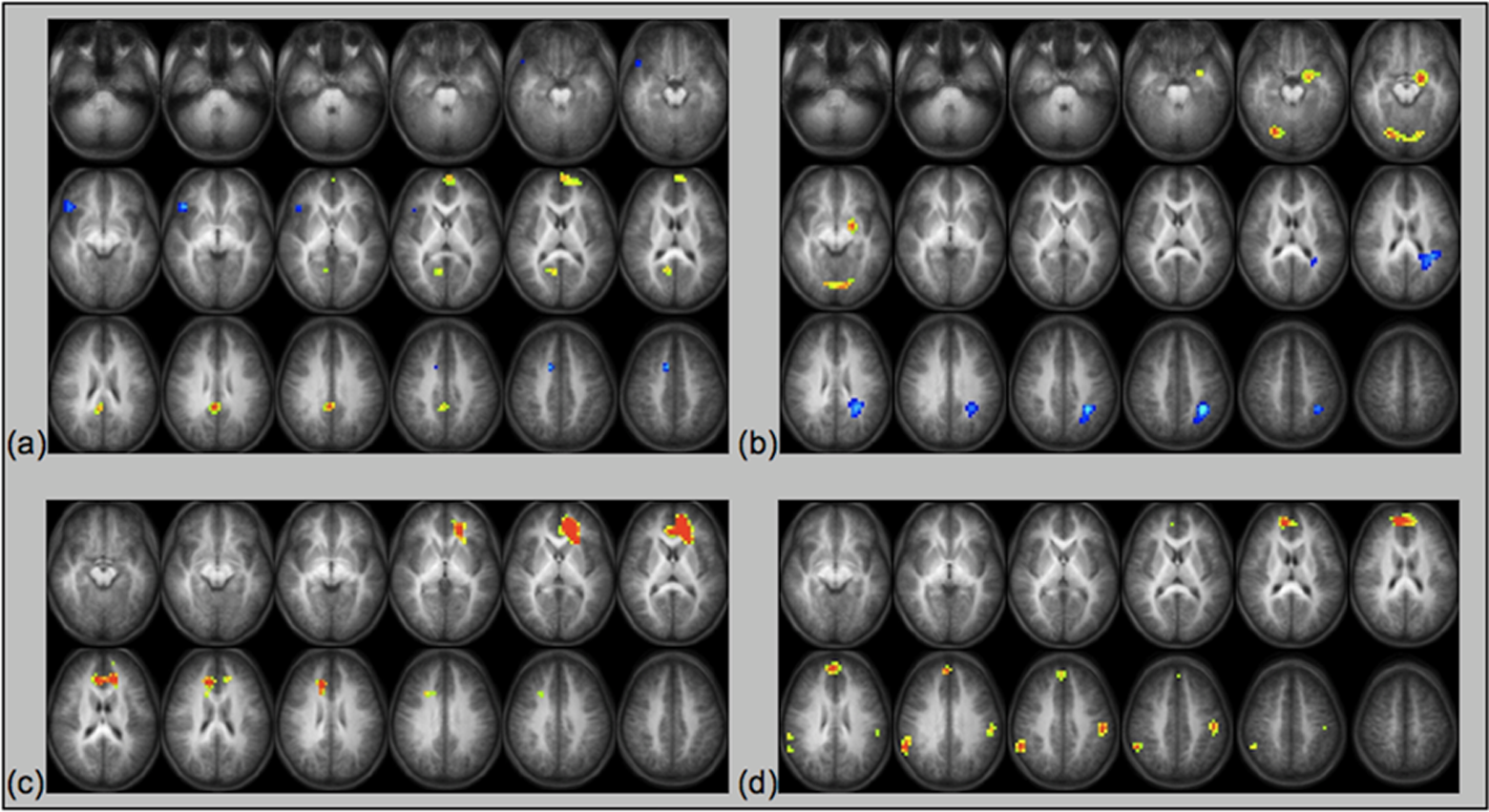
Regions of significant correlation with semantic decision performance during the semantic decision/tone decision task for (a) controls and (b) children with benign childhood epilepsy with centrotemporal spikes, z = 6.75, cluster size 30, P < .001, corrected. Regions of significant correlation with prosody discrimination performance during the prosody discrimination task for (c) controls and (d) children with benign childhood epilepsy with centrotemporal spikes, z > 8, cluster size 30, P < .05, corrected. BECTS = benign childhood epilepsy with centrotemporal spikes.
Prosody discrimination
This task typically engages right frontal and temporal regions, and our group of control participants showed a peak region of activation in the right temporal pole (Brodmann area 38/21, Figure 1g). Children with benign childhood epilepsy with centrotemporal spikes, as a group, had a different pattern of activation (Figure 1f) involving dorsolateral prefrontal cortex bilaterally (Brodmann area 9/10), anterior cingulate (Brodmann area 32), and right superior temporal gyrus (Brodmann area 22). When comparing groups, children with benign childhood epilepsy with centrotemporal spikes showed greater activation in left dorsolateral prefrontal cortex (Figure 1 h; Brodmann area 10).
Functional MRI Results: Correlations With Behavioral Data
Semantic decision/tone decision
In our group of healthy controls, there were 2 regions of significant positive correlation with performance on the semantic decision part of semantic decision/tone decision: left anterior prefrontal cortex (Brodmann area 10) and precuneus/posterior cingulate cortex (Brodmann area 7/31). Right inferior frontal gyrus (Brodmann area 45/47) showed a negative correlation with semantic decision performance (Figure 2a). Children with benign childhood epilepsy with centrotemporal spikes, in contrast, showed increases in activation in the left parahippocampal gyrus (Brodmann area 34) and lingual gyrus (Brodmann area 19) bilaterally associated with better performance. A region in the left intraparietal sulcus/supramarginal gyrus (Brodmann area 40) showed a negative correlation (Figure 2b).
Prosody discrimination task
Both controls and children with benign childhood epilepsy with centrotemporal spikes showed increases in activation in medial frontal and anterior cingulate cortex (Brodmann area 39/10/32) associated with better performance on the prosody discrimination part of the task (Figure 2c/d). However, only children with benign childhood epilepsy with centrotemporal spikes showed parietal regions bilaterally that were associated with better performance (supramarginal gyrus, Brodmann area 40, more anterior and extending into postcentral gyrus on the left).
Table 3 includes a list of regions of significant group contrast and Talairach coordinates of these areas of activation, group differences, and significant correlation.
Locations of Group Activation Regions and Activation Differences Between Children With Benign Childhood Epilepsy With Centrotemporal Spikes and Controls.
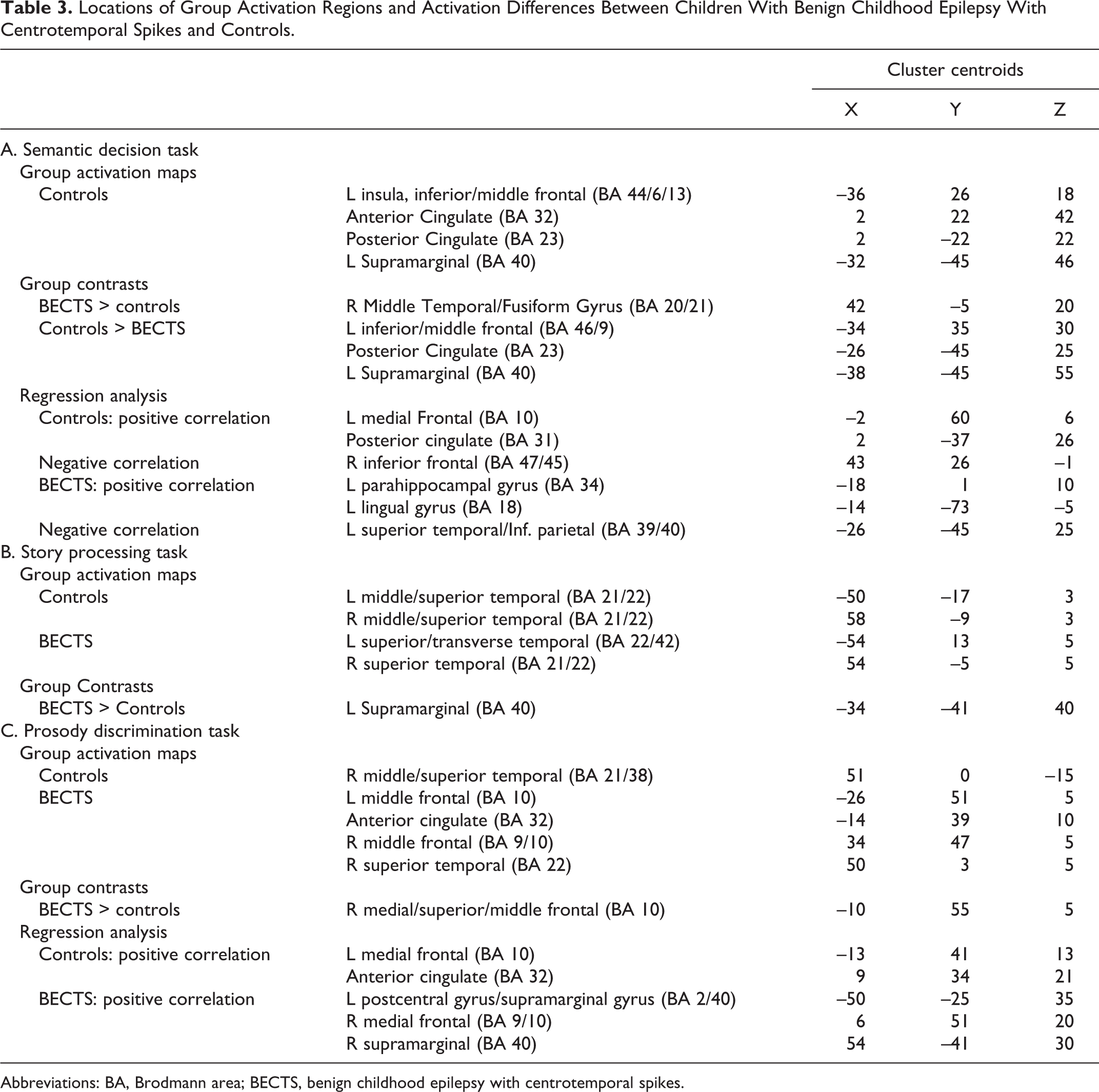
Abbreviations: BA, Brodmann area; BECTS, benign childhood epilepsy with centrotemporal spikes.
Functional MRI Results: Lateralization Index
Lateralization indices were calculated in selected task-specific regions of interest. For the semantic decision/tone decision task, this included an inferior frontal region of interest; for the story processing task, a superior temporal region of interest; and for the prosody task, 2 regions of interest were selected, one in the temporal pole, and a second in middle frontal gyrus.
Mean lateralization indices for children with benign childhood epilepsy with centrotemporal spikes and controls are listed in Table 2. Children with benign childhood epilepsy with centrotemporal spikes showed a significantly more bilateral pattern of activation in the semantic decision/tone decision task, t(26) = 3.93, P < .001. There was no significant difference in lateralization in story processing (P = .55) or prosody discrimination tasks (P = .68 for frontal, P = .75 for temporal region of interest), though children with benign childhood epilepsy with centrotemporal spikes had slightly more bilateral activation overall. Frequency of right or left centrotemporal spikes in the EEG evaluation of children with benign childhood epilepsy with centrotemporal spikes also did not predict lateralization index in any task (all P > .22).
Discussion
Children with benign childhood epilepsy with centrotemporal spikes showed lower language and cognitive skills when compared to healthy controls and they had different patterns of functional MRI activation during language processing, which may reflect shifts in functional architecture. These results support the presence of a link between functional reorganization of the neural architecture for language, and language and cognitive function in patients with benign childhood epilepsy with centrotemporal spikes.
Neuropsychological/Behavioral Data
Our neuropsychological findings support previous studies that have detected language difficulties in children with benign childhood epilepsy with centrotemporal spikes.7,12,16,38–42 The subtle difficulties in language processing and visuospatial skills noted in our study were not associated with particular lateralization of centrotemporal spikes or seizure history. The relatively mild degree of these difficulties suggests that these patients have been able to develop adequate language functions despite changes in the underlying neural architecture. However, they are not performing at the level of their healthy peers. Furthermore, lower levels of visuospatial skill and processing speed suggest that specific cognitive domains other than language may be affected in some children with benign childhood epilepsy with centrotemporal spikes.
Scores in both groups were higher than average. This finding may be, at least in part, attributed to the relatively high socioeconomic status in both groups. We did not collect data on socioeconomic status in this initial study. However, median income data by zip code from the 2000 United States Census indicates above-average income for families in both groups (for controls and patients, mean annual household income was 56 300 and 46 800 annually, respectively; P = .11).
Functional MRI Data
Semantic decision/tone decision
In adults, semantic decision tasks are known to activate a left-lateralized network involved in language processing, including left inferior frontal and prefrontal cortex, and left superior and middle temporal regions.25,43–47 We found a similar left-lateralized pattern of activation using this type of task. Our results in healthy children confirm this pattern: areas of activation included left inferior/middle frontal gyrus and left temporoparietal cortex. This functional MRI task was selected to highlight left-hemisphere–dominant semantic language networks and, therefore, detect potential anomalies in the typical network architecture resulting from benign childhood epilepsy with centrotemporal spikes. Children with benign childhood epilepsy with centrotemporal spikes, as a group, did not show as consistent activation of the left hemisphere during this task as healthy controls did. Relative to controls, they showed an increase in activation in the right hemisphere and decreases in left hemisphere regions typically engaged for the task (Figure 1b), suggesting that they may rely on an atypically bilateral network to support semantic processing, which is similar to patients with other types of epilepsy.48,49 These participants may use right hemispheric language areas to attempt to improve their performance. 35 However, when directly correlating activation with performance on this task, it was the striatum and visual regions that were associated with better performance in children with benign childhood epilepsy with centrotemporal spikes. In controls, better performance was associated with increases in cingulate cortex and decreases in right frontal activation. The different results suggest that the 2 groups may be using different strategies to perform the task: for controls, better task performance relies on regions associated with attention and response monitoring, not on regions supporting processing linguistic stimuli. Children with benign childhood epilepsy with centrotemporal spikes may be drawing on additional resources to process the stimuli: engaging visual cortex associated with visual imagery (because the decision task relies on visual properties of the animal named). The striatum has also been implicated in semantic processing. 50
Story processing task
When listening to an aurally presented story, a naturalistic speech task, multiple aspects of language processing are engaged, including speech perception, word recognition, and syntactic processing. Because of the complexity of auditory input that comprises natural speech processing, listening to speech sounds relative to nonspeech sounds engages bilateral primary and secondary auditory processing regions when observed with functional MRI.51,52 Specifically, bilateral superior and middle temporal regions are active.26,27,53,54 Children with benign childhood epilepsy with centrotemporal spikes showed increased activation in a more posterior part of left superior temporal cortex, indicating that their locus of activation during the task was shifted away from the centrotemporal region where centrotemporal spikes originate. Furthermore, we have shown recently (Figure 1c in Karunanayaka et al., 2007) that whereas the typical pattern of brain activation with this task is bilateral and fairly symmetric, when individual cortical components that participate in story processing were delineated with independent component analysis, the clearly lateralized components were the left frontal and left temporoparietal language areas. 53 Certainly, when these regions primarily involved in the story processing network are affected (as in patients with benign childhood epilepsy with centrotemporal spikes), there may be a shift of the posterior language area that shows here as a separate region of differing activation between healthy controls and children with benign childhood epilepsy with centrotemporal spikes.
Prosody discrimination task
Perception and discrimination of linguistic prosody (eg, identifying statements vs questions when the lexical content is the same) has been shown to rely on bilateral or right frontal and temporal mechanisms.55–58 In healthy children and young adults, we found that this task engaged right superior temporal gyrus, and right inferior frontal gyrus extending into middle frontal gyrus. 19 In the present study, our young control group showed a peak area of activation in the right inferior temporal region, whereas children with benign childhood epilepsy with centrotemporal spikes activated bilateral dorsolateral prefrontal cortex. In a group comparison, children with benign childhood epilepsy with centrotemporal spikes showed significantly more activation than control participants in the left middle frontal gyrus. This finding suggests that children with benign childhood epilepsy with centrotemporal spikes, as a group, may rely on an atypically bilateral network for this task as well, though distinguishing the specific roles of temporal and frontal regions requires further study. In both groups, better prosody discrimination skill was associated with increases in frontal anterior cingulate cortex, suggesting a dependence on attentional resources. Children with benign childhood epilepsy with centrotemporal spikes showed additional regions in parietal cortex that were associated with better task performance; the supramarginal gyrus has been associated with language comprehension in a number of contexts59–61 and these results suggest that again, children with benign childhood epilepsy with centrotemporal spikes are relying on additional resources atypical for the task in order to maintain a level of performance that is similar to healthy controls.
A limitation of our study was the relatively small sample of EEG used to estimate centrotemporal spike frequency and lateralization. The reviewed EEG recordings were routine samples obtained as part of clinical care. With this limited sample, we found no clear relationships between centrotemporal spikes and functional MRI measures. We cannot ascertain that the EEG samples reviewed in this study are in fact representative samples for the enrolled patients. In addition, sleep was not recorded for all the patients. Given the fact that epileptiform discharges commonly activate during sleep, the difference in sleep obtained in the routine EEGs may have affected the number of centrotemporal spikes observed. A much more reliable incidence and lateralization of centrotemporal spikes could be obtained using a 24-hour EEG. Another limitation was the relatively small sample of 15 children with benign childhood epilepsy with centrotemporal spikes, 6 of whom were on antiepileptic medications, which does not allow us to separate out the effects of medication on cognitive performance, functional MRI activations, or the effect on centrotemporal spikes. Finally, not all neuropsychological and functional MRI measures were collected on all participants.
Using functional MRI, we have demonstrated that language ability in children with benign childhood epilepsy with centrotemporal spikes is associated with detectable differences in the underlying language networks supporting these skills. These results are consistent with another recent functional MRI and event-related potential studies. Lillywhite et al 62 found a lesser degree of left-lateralization for language function during covert verb generation with visual stimulus presentation in patients with benign childhood epilepsy with centrotemporal spikes compared to controls. Monjauze et al 13 recorded event-related potentials during an auditory verb generation task. They found that patients in remission from benign childhood epilepsy with centrotemporal spikes had atypical (more rightward) lateralization in frontal regions as well as significant language deficits. Our results extend these findings by revealing changes in the language network that underlie various linguistic functions in patients with benign childhood epilepsy with centrotemporal spikes. The present results and other recent neurobehavioral studies suggest that this disorder may not be completely benign, and assessment and/or treatment of patients with benign childhood epilepsy with centrotemporal spikes to prevent or reduce language and cognitive problems could be clinically important. The language weakness associated with benign childhood epilepsy with centrotemporal spikes maybe progressive and long-lasting,12,63 or may precede seizures. 14 If the language difficulties and their consequences are caused by centrotemporal spikes and/or seizures, there is potential for intervention with antiepileptic medications, though some antiepileptic medications may worsen cognitive problems.64–66 So far, studies that have systematically examined medication effects have found mixed results38,64,67,68 and further studies are needed. Siblings of children with benign childhood epilepsy with centrotemporal spikes who do not have seizure have also been shown to have a similar pattern of cognitive impairment. 69 Clarifying the interaction between seizures, centrotemporal spikes and cognitive function in benign childhood epilepsy with centrotemporal spikes will allow for a better understanding of how antiepileptic medication or early behavioral intervention can best be used to ensure the best cognitive outcome in these patients.
Footnotes
Acknowledgments
All work described in this manuscript was conducted at Cincinnati Children’s Hospital Medical Center. Portions of this work were presented as posters at the Organization for Human Brain Mapping Annual Meeting in June 2011, and the American Epilepsy Society Annual Meeting in December 2011.
Author Contributions
JV: drafting of manuscript, study design, data acquisition and analysis. JPS: EEG review, study design, manuscript review. KPE: data analysis, construction of figures and tables, manuscript review. DMH: participant recruiting, data acquisition. DM: participant recruiting, EEG review, manuscript review. TAG: mentorship, manuscript review. AWB: design and interpretation of neuropsychological testing, manuscript review. KP: participant recruiting, data acquisition, manuscript review. SKH: mentorship, study design, manuscript review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board at Cincinnati Children's Hospital Medical Center.