
Abstract
The aim of this study is to identify clinical or electroencephalographic (EEG) features associated with refractoriness to the initial antiepileptic drug in typical benign childhood epilepsy with centrotemporal spikes. A total of 87 children with typical benign childhood epilepsy with centrotemporal spikes were retrospectively reviewed in the analyses. The patients were subdivided into 2 groups: patients whose seizures were controlled with monotherapy and patients requiring 2 medications. Sixty-three children achieved seizure freedom with monotherapy, whereas 24 received 2 medications for seizure control. Diffusing foci at the follow-up EEG and delayed treatment (duration >1 year) are 2 main risk factors associated with more refractory cases (P < .001). Delayed diagnosis (37.1%) and nonadherence to treatment (57.2%) contributed to delayed treatment. Our findings suggested that diffusing foci on EEG and delayed treatment are associated with more frequent seizures and refractoriness in benign childhood epilepsy with centrotemporal spikes. Diagnostic delays and nonadherence hindered timely care, which may represent opportunities for improved intervention.
Keywords
Children with benign childhood epilepsy with centrotemporal spikes usually have favorable long-term prognosis. 1 The label “benign” is applied to this most common child epilepsy syndrome that was formerly considered a defining feature implying age-related resolution, few seizures, pharmacoresponsiveness, and rare neurocognitive comorbidities. When treated, they respond well to antiepileptic medication, even those who initially suffer from frequent and troublesome seizures, with almost all patients achieving long-term remission by midadolescence. 1
Benign childhood epilepsy with centrotemporal spikes is not pharmacologically specific. No antiepileptic medication reaches the highest levels (level A or B) of effectiveness for children with benign childhood epilepsy with centrotemporal spikes. 2 Our recent study suggested that low-dosage monotherapies with levetiracetam or valproate were equally effective in controlling typical benign childhood epilepsy with centrotemporal spikes. 3 However, there are children with this type of epilepsy who present with multiple seizures despite the prophylaxis with one antiepileptic drug. 4 Up to 20% children with benign childhood epilepsy with centrotemporal spikes 5 respond poorly to the initial treatment and may require a second antiepileptic medication for controlling recurrent seizures. How often a second antiepileptic medication is needed in children with typical childhood epilepsy with centrotemporal spikes and the clinical and electrophysiological factors associated with refractoriness to the initial treatment in benign childhood epilepsy with centrotemporal spikes are questions that have been little studied.
The objective of this study is to identify children with typical benign childhood epilepsy with centrotemporal spikes who may have the suboptimal seizure control with the initial treatment and to investigate the clinical and electrophysiological features that might influence the first drug response in childhood epilepsy with centrotemporal spikes.
Methods
Patients
This was a retrospective, uncontrolled, case-comparison cohort study of preselected subjects from the Epilepsy Clinic of the Department of Neurology, West China Hospital of Sichuan University, between June 2010 and May 2013. The inclusion criteria were as follows: (1) newly diagnosed benign childhood epilepsy with centrotemporal spikes according to the current clinical and EEG criteria adopted by the International League Against Epilepsy (ILAE) 6 ; (2) the presence of the specific EEG characteristics at any time before or during the study and an age-typical EEG background rhythm; (3) typical seizures that were hemifacial, characterized by hemifacial clonic manifestations that were sometimes preceded by unilateral paresthesia involving the tongue, lips, gums, and cheek and jerks that were often associated with lateral tonic deviations of the mouth involving the lips and tongue, resulting in drooling due to sialorrhea with or without secondary generalization; (4) no other neurologic, psychiatric, or somatic disorders; (5) no evidence of structural brain damage based on magnetic resonance imaging (MRI); (6) normal neurologic and mental status; (7) at least 2 seizures within 6 months prior to the initiation of treatment; and (8) regular visits to our clinic for at least 24 months. The exclusion criteria were as follows: (1) variants like atypical benign partial epilepsy, Landau-Kleffner syndrome, and continuous spikes and waves during sleep; (2) previous treatment with antiepileptic drugs prior to visiting our clinic or refusal to receive drug treatment; (3) incomplete statistical information; (4) failure to return for follow-up; and (5) cessation of drug treatment without permission. The local research ethics committee approved this study, and written informed consent was obtained from the parents or caregivers. Children so identified with benign childhood epilepsy with centrotemporal spikes were then divided into 2 groups: group 1, those in whom seizure control was attained with the use of the first antiepileptic drug, and group 2, those in whom 2 medications were ultimately required for seizure control. A second medication was added only if seizures persisted despite compliance with adequate amounts of the initial medication selected, with both medications continued for ongoing seizure control. The mainly used initial antiepileptic drugs were valproic acid, oxcarbazepine, lamotrigine, and levetiracetam. Treatment started with 5 mg/kg/d valproic acid, 10 mg/kg/d oxcarbazepine, 10 mg/kg/d levetiracetam, and 1 mg/kg/d lamotrigine. All cases titrate gradually with weekly increments of the same amount. Individualization of the minimal effective maintenance doses is crucial in efficacy, safety, and tolerability in children with epilepsy. 7 Considering the adverse effects of antiepileptic drugs in children, the suggested daily dosage of valproic acid ranges from 15 to 40 mg/kg/d, lamotrigine 1 to 5 mg/kg/d, oxcarbazepine 30 to 45 mg/kg/d, and levetiracetam 20 to 40 mg/kg/d. 8 A second medication was added only if seizures persisted despite compliance with adequate amounts of the initial medication selected, with both medications continued for ongoing seizure control. Compliance was ascertained by parents’ monitoring reports and regular visits to our clinic.
Evaluation of Possible Factors That Might Influence the Response to the First Antiepileptic Medication
An assortment of information was extracted and contrasted between the 2 groups, including gender, family history, febrile seizures, age of onset, interval duration of seizures prior to treatment initiation, and type of seizures experienced (simple partial, complex partial, secondary generalized tonic-clonic seizures). All cases received 24-hour video EEG at diagnosis and overnight video EEG during the follow-up. The following EEG parameters were evaluated: spike localization, spike index (number of spikes/min), focal specific discharges, and occasional sharp waves diffusing to one or both hemispheres, being present during I-II slow sleep stages and during wakefulness any time during the study period. The Chinese version of the Child Behavior Checklist 9 was filled out by the parents of patients to assess behavioral conditions at baseline.
Statistical Analysis
Statistical analyses were performed using commercially available SPSS 19.0 (SPSS, Chicago, IL). Continuous variables were expressed as means ± standard deviations. Pearson chi-square test or Fisher exact test was used, as appropriate, for analysis of between-group differences in discrete variables, and analysis of variance with a Bonferroni post hoc test was used for continuous variables. Logistic regression analysis was used for multivariate analysis to identify factors associated with the necessity of 2 antiepileptic drugs. Significance was set at P <.05 in analysis.
Results
A total of 87 subjects (49 male, 38 female), mean age 9.8 ± 2.1 years, were diagnosed with typical benign childhood epilepsy with centrotemporal spikes and included in this study. None of these patients’ condition evolved into atypical benign partial epilepsy during the follow-up. The ages of seizure onset ranged from 4.0 to 12.0 years, and the mean peak frequency occurred at 7.7 ± 2.1 years. Only 2 of 87 (2.3%) patients had seizure before age 3 years, and 31 of 87 (35.6%) had seizures before age 6 years (Table 1). Of the 87 subjects included in the study, 63 (72.4%) required a single medication (Group 1) and 24 (27.6%) required 2 medications (Group 2).
Demographic and Clinical Factors Associated With the Need for the Second Medication.

Abbreviation: CFT, centrofrontotemporal; CPS, complex partial seizure; CPS-GTCS, complex partial seizure secondary with generalized tonic-clonic seizure; CPT, centroparietotemporal; CT, centrotemporal; IQ, Intelligence Quotient; LTG, lamotrigine; LEV, levetiracetam; OXC, oxcarbazepine; SD, standard deviation; SPS, simple partial seizure; VPA, valproic acid.
The differences between the 2 groups observed regarding gender, age, age of onset, family history, febrile seizures, and seizure types were not found to be statistically significantly different (Table 1).
Multivariate analysis was also performed. The first drug choice (P < .001, odds ratio = 24.454), delayed treatment (P < .001, odds ratio = 33.784), diffusing spike foci (P < .001, odds ratio = 15.331), and living in rural areas (P = .001, odds ratio = 11.853) are associated with the necessity of 2 antiepileptic drugs.
The background rhythms were normal in all patients. Regarding EEG findings, 11 of 63 (17.5%) patients in group 1 had bilateral spike foci, whereas 8 of 25 (33.3%) patients in group 2 did. Of patients in group 1, 12 of 63 (19.0%) had diffusing focal specific discharges and occasional sharp waves to one/both hemispheres, whereas 15 of 24 (62.5%) patients in group 2 had diffusing foci. Presence of diffusing foci at the follow-up EEG pattern when compared with the EEG pattern at diagnosis was a risk factor for poor response to the first antiepileptic drug (P < .001). No significant differences in EEG focus (P = .942) and EEG lateralization (P = .147) were observed between treatment groups.
Regarding the initial antiepileptic drug treatment, for patients in Group 1, 33 of 64 (52.4%) patients took levetiracetam. The levetiracetam dosages ranged from 15.2 to 37.9 mg/kg/d (mean 22.7 ± 4.7 mg/kg/d). Twenty-three of 64 (36.5%) patients took valproic acid. The doses ranged from 9.3 to 27.0 mg/kg/d, and the mean dose was 18.6 ± 5.7 mg/kg/d. Five of 64 (7.9%) patients took oxcarbazepine, with average dose ranging from 13.1 to 19.7 mg/kg/d (mean 15.8 ± 2.4 mg/kg/d). Two of 64 (3.2%) patients took lamotrigine. One took 3.4 mg/kg/d and the other took 2.9 mg/kg/d. Among 24 patients in group 2, 9 (37.5%) took levetiracetam ranging from 33.8 to 33.7 mg/kg/d (mean 35.4 ± 2.5 mg/kg/d), 7 (33.3%) patients took lamotrigine ranging from 3.4 to 5.4 mg/kg/d (mean 4.1 ± 0.7 mg/kg/d), and 6 (25.0%) took oxcarbazepine at doses ranging from 26.7 to 34.2 mg/kg/d (mean 30.2 ± 3.7 mg/kg/d). Only 1 (4.2%) child received valproic acid, at a dose of 31.9 mg/kg/d.
In group 2 patients, 15 of 24 (62.5%) used valproic acid with an average dose of 13.1 ± 5.4 mg/kg/d as an add-on therapy (ranging from 5.6 to 23.3 mg/kg/d). In addition, 6 of 24 (25.0%) used levetiracetam with an average dose of 13.7 ± 5.0 mg/kg/d as add-on therapy (ranging from 4.8 to 22.1 mg/kg/d). Three of 24 (12.5%) patients used oxcarbazepine at an average dose of 13.1 ± 3.0 mg/kg/d (ranging from 10.2 to 16.2 mg/kg/d). The demographic and clinical data and details of add-on therapy of group 2 were summarized in Table 2.
Demographic and Clinical Data of BECTS Children Requiring the Second Antiepileptic Drug for Seizure Control.
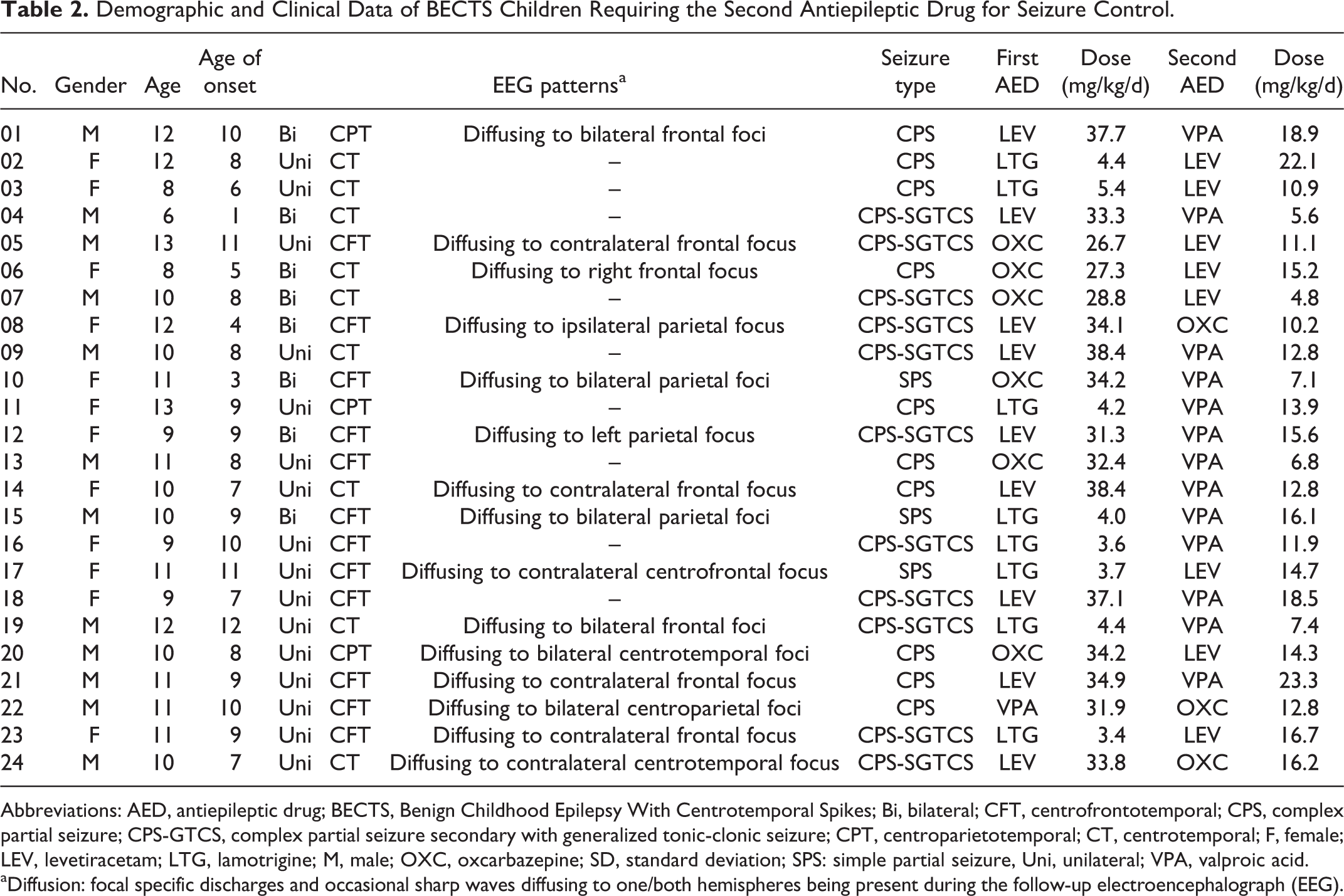
Abbreviations: AED, antiepileptic drug; BECTS, Benign Childhood Epilepsy With Centrotemporal Spikes; Bi, bilateral; CFT, centrofrontotemporal; CPS, complex partial seizure; CPS-GTCS, complex partial seizure secondary with generalized tonic-clonic seizure; CPT, centroparietotemporal; CT, centrotemporal; F, female; LEV, levetiracetam; LTG, lamotrigine; M, male; OXC, oxcarbazepine; SD, standard deviation; SPS: simple partial seizure, Uni, unilateral; VPA, valproic acid.
aDiffusion: focal specific discharges and occasional sharp waves diffusing to one/both hemispheres being present during the follow-up electroencephalograph (EEG).
A total of 35 of 87 (40.2%) patients had at least 1 year’s delay of treatment. In group 2, 9 of 24 (37.5%) had more than 6 months’ delay and 12 of 24 (50.0%) had more than 2 years’ delay. In contrast, 14 of 63 (22.2%) patients in group 1 had delay in treatment. We reviewed the medical records and inquired from parents or caregivers about the reasons for treatment delay. The main reasons contributing to treatment delay were delays in diagnosis and nonadherence to antiepileptic medications (Table 3).
Factors Contributing to Delayed Treatment.
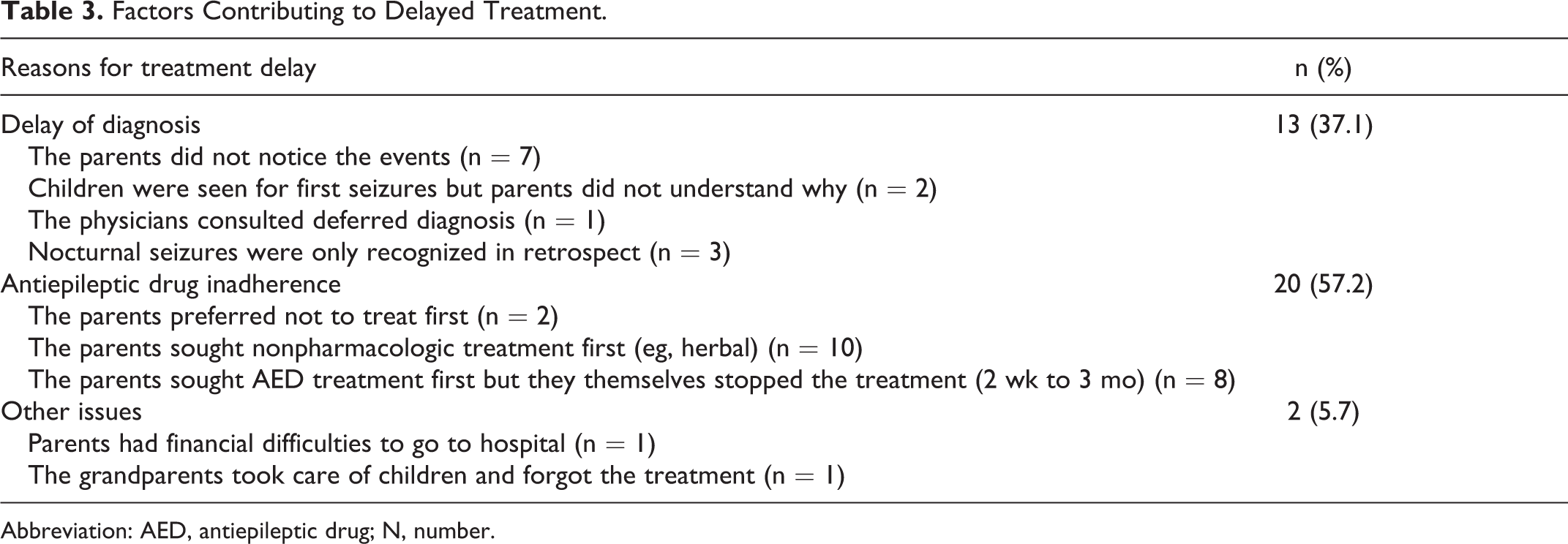
Abbreviation: AED, antiepileptic drug; N, number.
All parents completed the Child Behavior Checklist and all children participated in WISC-IV testing at baseline. The scores with the Child Behavior Checklist in children requiring a second drug were higher (34.13 vs 28.24), but the difference were not statistically significant (P = .087). But children with monotherapies performed better in full-scale IQ (99.16 vs 91.33, P = .007) and performance IQ (97.92 vs 90.08, P = .012).
Discussion
For children with typical benign childhood epilepsy with centrotemporal spikes, low-dosage antiepileptic monotherapy is sufficient to control seizures. 3 In the present study, all the patients in our study reached seizure freedom for at least 12 months. We found that a small portion of (27.1%) children suffering from benign childhood epilepsy with centrotemporal spikes require a second antiepileptic drug as add-on therapy to attain seizure freedom. Diffusing foci on the EEG pattern during the follow-up and delay of treatment may be the risk factors associated with refractoriness to the initial medical treatment in children with benign childhood epilepsy with centrotemporal spikes.
Limited data are available on the utility of polytherapy with antiepileptic drugs in benign childhood epilepsy with centrotemporal spikes. Previous literature has demonstrated that early onset of seizures is associated with poor response to the initial treatment; seizure onset before age 3 years was a crucial risk factor. 10 -12 We did not find age of onset to be a risk factor, and this inconsistency may be explained by the age difference of the study population. In our study, only 2 children (2.3%) had seizures before age 3. We divided our sample into 3 age groups according to age of onset (Table 1). We included 31 of 87 children having seizures under the age of 6 but we did not identify it as a risk factor.
We found that children with diffusing foci on EEG pattern were more likely to be refractory to the first medication. The epileptic foci in benign childhood epilepsy with centrotemporal spikes are not confined to rolandic areas and diffuses between bilateral hemispheres in 17% to 24.7% of patients. 13,14 In the present study, 31% of the patients presented diffusing foci during the follow-up EEG monitoring. We did not find any correlation between the EEG lateralization and the response of the initial antiepileptic drug (P = .142) despite one recent study finding that children with unilateral discharges responded better to the monotherapies with antiepileptic drug. 15 The classical EEG presentation of benign childhood epilepsy with centrotemporal spikes is normal background, high-voltage diphasic spikes, or sharp waves in rolandic areas with or without aftercoming slow waves. 16 Atypical EEG patterns such as slow spike-wave focus, synchronous foci, or generalized 3-Hz spike-wave discharges 17 were related to severe evolutions of benign childhood epilepsy, with centrotemporal spikes into severe epileptic syndromes such as Landau-Kleffner syndrome and continuous spike waves during slow sleep. 18 The reasons that some children develop diffusing foci on EEG are not yet understood. It may be explained by the hypothesis that the children with diffusing foci may suffer from more widely distributed epileptic activity throughout the bilateral hemispheres. 16 Varying epileptic focus in benign childhood epilepsy with centrotemporal spikes may suggest a more widespread neuronal network involved in epileptic discharges, which may be difficult to interfere with.
Majority of patients (87.5%) in group 2 failed to receive timely treatment. Because of its benign nature and good outcome, the delay of treatment in benign childhood epilepsy with centrotemporal spikes received little attention in previous studies. 10 -12 We further analyzed the reasons for delay of treatment and found that they were mainly social. One contributing factor is the challenge of timely and accurate diagnosis at the onset of seizure, which accounted for 37.1% children who had delayed treatment in our study. Rare seizures and typically nocturnal nature make the characterization of benign childhood epilepsy with centrotemporal spikes mainly based on parents’ report. 19 Parents, most of whom lack the basic knowledge of epilepsy, often did not recognize subtle events and therefore did not realize it as being of concern. Furthermore, some physicians and pediatricians failed to recognize seizures and make different diagnosis. Physician knowledge, particularly among nonneurologists, of the range of seizure types and impact of epilepsy is a specific area for medical education. 20 Epilepsy care is less than optimal in most settings in Sichuan, where our academic center is located. 21 In this context, the correct diagnoses were deferred in certain cases by the physicians who first saw the patients. Epilepsy in numerous patients who experience an even lower frequency of seizures may progress to chronic epilepsy without timely treatment. The misrecognition or even ignorance of parents and some physicians reflect the need for public education as well as the training of local physicians.
Another factor that may influence timely treatment is antiepileptic medication nonadherence. In our findings, 57.2% of children did not comply well with the prescription at the onset of epilepsy and failed to receive timely treatment. Nonadherence is a common and underrecognized problem for children with newly diagnosed epilepsy. Our prior study revealed that appropriate treatment is not always guaranteed in certain areas in Sichuan, and some uninformed patients prefer herbal medicine to appropriate treatment program, 22 which holds true for some children’s parents in the current cohort (28.6%). Recent findings revealed that early adherence is critical to seizure outcomes in children with newly diagnosed epilepsy. 23,24 Pediatric antiepileptic medication nonadherence in the first 6 months of treatment is related to lower rates of long-term seizure freedom. 24 Hence, considering these negative influences of nonadherence, education about epilepsy is the cornerstone of optimal management. 21 Parents should be educated about the characteristics of childhood epilepsy and information about the right and appropriate treatment programs should be made available to them.
The current study results should be interpreted within the context of several limitations. First, given the retrospective nature and small number of individuals requiring second medications, this observation requires prospective validation in a larger sample. Also, although every effort was made to document reported seizures using chart review and directly asking the parents, it is possible that parents did not report seizures that occurred between clinic visits. Furthermore, serum drug level data may be more reliable than weight-based dosage, but these data were not available. Third, we had only neuropsychological tests at baseline, so we could not evaluate the impact of the second drug’s efffect on IQ and behavior.
In conclusion, these observations provide insights into variable pharmacologic responsiveness in benign childhood epilepsy with centrotemporal spikes. For patients who have frequent seizures despite prophylaxis with the first antiepileptic drug, a second medication may be needed as an add-on therapy. Children with diffusing foci on EEG patterns deserve more attention and are more likely to require the add-on antiepileptic drug. Delay of appropriate intervention for children with benign childhood epilepsy with centrotemporal spikes is another risk factor for resistance to the first antiepileptic drug in benign childhood epilepsy with centrotemporal spikes. The diagnostic yield of community-based pediatricians and neurologists should be standardized to minimize diagnostic delay and thus facilitate timely intervention.
Footnotes
Acknowledgments
We thank all the children who took part in this study as well as their parents.
Author Contributions
FX conducted the research, interpreted data, and wrote the first draft. DA revised the manuscript for content. SC and JR were involved in planning the research and had revised the manuscript for content. DZ made critical corrections to the manuscript and obtained funding.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (Grant nos. 810420108014, 81371529, and 81301206).
Ethical Approval
The local research ethics committee approved this study, and written informed consent was obtained from the parents or caregivers (20110818).