
Abstract
Insomnia is prevalent in pediatrics, particularly in those with neurodevelopmental disorders. Gabapentin has shown promise in treating insomnia in adults. The purpose of our study was to review our experience with using gabapentin to treat insomnia in children. We identified 23 children, seen by the authors in our Pediatric Sleep Clinic from January 2009 to March 2012. The mean age was 7.2 years and 70% were male. The majority (87%) had been given diagnoses of neurodevelopmental or neuropsychiatric disorders. All parents received education in sleep behavioral interventions. The majority of children (70%) had both sleep-onset and sleep maintenance insomnia. The average starting dose of gabapentin was 5 mg/kg every bedtime and the maximal dose was 15 mg/kg every bedtime. At follow-up, improved sleep was noted in 78% of children. Adverse effects were noted in 6 children.
Insomnia in a pediatric population is defined as difficulty in initiating or maintaining sleep that is viewed as a problem by the child or caregiver. Insomnia may be primary or secondary to another condition (psychiatric, neurologic, medical, drug, or alcohol related). The associated impairment in daytime functioning, frequency, chronicity, and severity in either the child or the child’s family helps characterize the clinical significance. 1 Insomnia is prevalent and challenging to treat in pediatrics, particularly in those with neurodevelopmental disorders. Children with neurologic injury or genetic, psychiatric, and behavioral syndromes are especially susceptible to certain types of insomnia. 2 There are no sleep medications approved by the United States Food and Drug Administration (FDA) for a pediatric indication and there have been very few studies published on pharmacologic interventions for childhood insomnia refractory to behavioral interventions. 3
Gabapentin was approved for treatment of partial seizures by the Food and Drug Administration in 1993. Gabapentin, originally designed as a precursor of γ-aminobutyric acid (GABA) that easily enters the brain, has been known to increase brain synaptic γ-aminobutyric acid. 4 However, its precise pharmacologic mechanism in humans remains unknown. Gabapentin is an attractive agent given its favorable side effect profile, strong safety record, and limited adverse effects, such as somnolence. Numerous off-label uses have also been extended for various clinical trials, expanding gabapentin’s applicable uses. It has been approved for the treatment of neuropathic pain and restless legs syndrome in addition to its original purpose as an anticonvulsant medication. 5 In a recent open-label study in adults, it was found to improve sleep quality in patients with primary insomnia, as it increases slow-wave sleep and sleep efficiency; it also decreases wake after sleep onset (WASO) and spontaneous arousal. 6 Studies on cognitive effects of gabapentin reveal minimal impact. 7 The purpose of this manuscript is to report on the use of gabapentin for sleep in children with insomnia.
Case Summary
A 4-year-old boy with autism spectrum disorder presented with difficulty maintaining sleep. His bedtime was at 8:30 pm throughout the week, and he took 20 to 30 minutes to fall asleep. He would then wake up between 2 and 5
His parents previously had tried supplemental melatonin for night wakings without success. He was not currently on melatonin. He was on no other concurrent psychotropic medications.
His parents were counseled on sleep hygiene techniques and other behavioral modifications. The patient was also started on gabapentin 5 mg/kg. This initial dose was titrated to 15 mg/kg over a 3-week period. They returned for follow-up 3 months after the initial consultation. At that visit, his parents reported that he was now sleeping through the night and no longer had any night awakenings. He was waking up at 6
Methods
Approval was obtained through the institutional review board at Vanderbilt University to review the electronic medical records of children with insomnia (onset and/or maintenance) treated with gabapentin. Twenty-nine children, seen by the authors in our Pediatric Sleep Clinic from January 2009 to March 2012, were identified, with follow-up data available in 23 children (Table 1). Gabapentin was given 30 to 45 minutes before bedtime. All patients received a comprehensive sleep history and neurologic exam. Age, gender, diagnosis, type of insomnia, behavioral sleep intervention, and medications were recorded. The initial starting dose and final dose of gabapentin were recorded, along with clinical response, side effects, and discontinuation (where applicable).
Subject Description and Response to Gabapentin
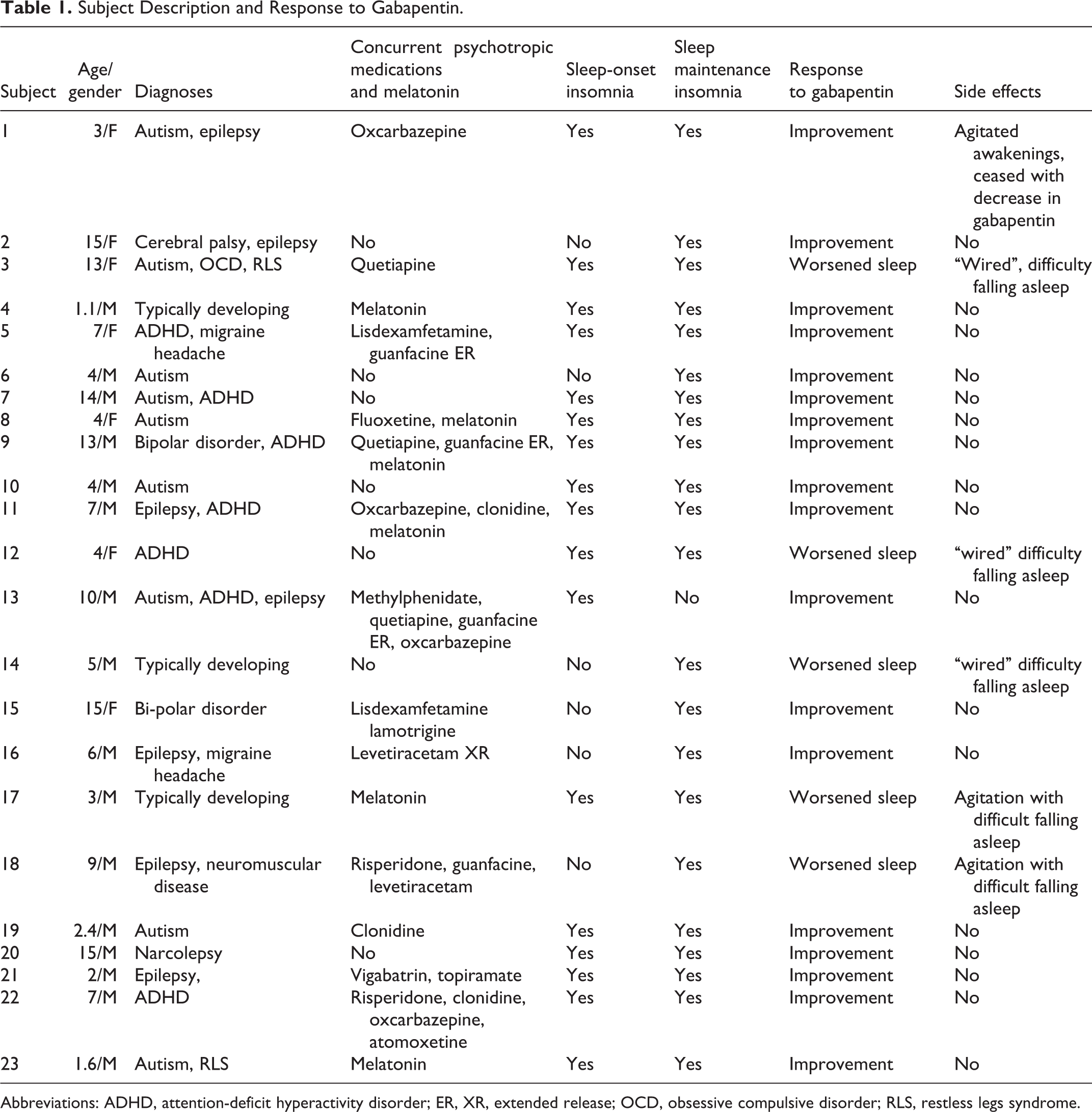
Abbreviations: ADHD, attention-deficit hyperactivity disorder; ER, XR, extended release; OCD, obsessive compulsive disorder; RLS, restless legs syndrome.
Results
Participants
We limited our analysis to the 23 children who had follow-up data. The mean age was 7.2 years and 70% were male. The majority (87%) had been given diagnoses of neurodevelopmental or neuropsychiatric disorders (autism spectrum disorder, with other diagnoses including attention-deficit hyperactivity disorder, epilepsy, and bipolar disorder). The majority of children (70%) had both sleep-onset and sleep maintenance insomnia. Only 1 child had sleep-onset insomnia alone and 6 children had sleep maintenance insomnia alone. Follow-up visits occurred approximately every 3 to 6 months.
Gabapentin Response and Adverse Effects
The average starting dose of gabapentin was 5 mg/kg every bedtime (range 3-7.5 mg/kg) and the maximal dose was 15 mg/kg every bedtime (range 6-15 mg/kg). Gabapentin was given 30 minutes to 45 minutes before bedtime. At follow-up, improved sleep was noted in 78% of children. Adverse effects were noted in 6 of the children. One subject had onset of agitated awakenings on increasing gabapentin to 15 mg/kg; the dose was then decreased to 10 mg/kg and these events resolved at the lower dose, while improvements in sleep continued. Five subjects (with both sleep-onset and sleep maintenance insomnia) were described as being “wired” and having increased difficulty falling asleep upon initiation of gabapentin (within the first week). Use of gabapentin was discontinued with resolution of symptoms.
Polysomnography
Twelve subjects had polysomnography before initiating gabapentin. No subjects had polysomnography after starting gabapentin. Two subjects out of the 12 were diagnosed with sleep-disordered breathing based on their polysomnography (apnea-hypopnea indices of 3.8 and 2 events/h). One patient underwent adenotonsillectomy and 1 patient was treated by medical intervention (nasal steroids and montelukast inhibitors), respectively. One patient presented to the clinic already having a diagnosis of residual obstructive sleep apnea after adenotonsillectomy being treated with continuous positive airway pressure. Despite clinical improvement in sleep apnea, the 3 patients continued to experience insomnia on follow-up and were subsequently started on gabapentin and reported improvement in insomnia. Eight subjects had full 21-lead electroencephalography either before or after initiating gabapentin (ordered by epileptologist). Periods of sleep were not obtained on the electroencephalography.
Previous Medications, Coexisting Medications, and Sleep Behavioral Interventions
Sixteen subjects had used melatonin as an initial medication intervention; all but 1 had sleep maintenance insomnia with or without sleep-onset insomnia. Although 5 showed an improvement in sleep-onset insomnia, improvement in sleep maintenance insomnia was not reported with melatonin treatment. Two subjects had used clonidine and 2 other subjects had used amitriptyline to treat their insomnia without improvement. At the time of gabapentin initiation, 13 children were concurrently taking psychotropic medications and 5 children were concurrently taking melatonin (Table 1).
All parents received education in sleep behavioral interventions in the clinic setting by the first author. Sleep behavioral interventions included sleep hygiene techniques (maintaining a regular bedtime and wake time, establishing a bedtime routine, avoiding stimulating activities before bed) and, when appropriate, relaxation techniques along with cognitive restructuring (eg, eliminating negative thoughts).
Discussion
Gabapentin has previously been shown to be an effective treatment for adults with primary insomnia but to our knowledge its use as a treatment for insomnia in children has not been reviewed. In this case series, gabapentin was found to be a safe and a well-tolerated treatment for sleep-onset and sleep maintenance insomnia in the majority of children, including those with neurodevelopmental or neuropsychiatric disorders. A strength of our series is that tolerability was documented in children across a wide age range, diagnoses, and in the presence of multiple psychotropic medications. Another strength is that it mirrors the clinical population treated by many pediatric providers (eg, children with coexisting psychiatric and behavioral conditions who require psychotropic medications). One important feature of gabapentin in this population is that it has minimal drug interactions. 8
The retrospective chart review design of our study does not allow us to assess efficacy. However, in combination with sleep behavioral interventions, 78% of children showed improvement in sleep (as reported by parents). Furthermore, this beneficial response was noted at gabapentin doses of 3 to 15 mg/kg orally every bedtime, much less than the recommended dose to treat epileptic seizures (40 mg/kg divided 3 times daily).
Few studies have evaluated pharmacologic interventions for childhood insomnia refractory to behavioral interventions 3 and even fewer have included children with neurodevelopmental or neuropsychiatric disorders. For children with chronic and severe sleep problems that are neurologically based or are due to structural damage, the addition of adjunct pharmacotherapy often proves necessary to enhance the quality of the child’s sleep. 9 Melatonin has been demonstrated to be effective for the treatment of sleep-onset insomnia in children with autism spectrum disorder, although it has not been shown to be effective in sleep maintenance insomnia (meta-analysis). 10 It also has minimal side effects, including in a large series of 107 children. 11 Gabapentin appears to have a similar side effect profile to melatonin, although it may have the added benefit of also treating sleep maintenance insomnia, although larger controlled trials will be needed to establish its efficacy.
Few and minor adverse effects were reported. The main adverse effect was children feeling “wired” that led to a worsening in sleep-onset insomnia, which resolved when gabapentin was discontinued. When this side effect occurred, it happened within 1 week of starting gabapentin, which was beneficial to patient care in that parents can be counseled about this side effect prior to initiation.
Our study has several limitations. First, the nature of our study (retrospective and not placebo controlled), the small sample size, the heterogeneous sample, and the presence of confounding variables (eg, concurrent medications, variability of dose) does not allow us to attribute the reported improvement in sleep to the efficacy of gabapentin alone. However, when gabapentin was added to psychotropic medications and/or melatonin, it was because the child was continuing to experience sleep difficulties while taking these medications. Therefore, we believe that the observation of improved sleep with administration of gabapentin, even in cases where the child was taking other psychotropic medications, is still meaningful.
Second, we relied on parental report of clinical response to gabapentin via clinical chart review. The use of validated measures of sleep would have strengthened parental observations.
Future prospective randomized blinded placebo clinical trials of gabapentin in children with insomnia appear warranted. These studies will need to carefully control for dose, concurrent medications, account for the effects of behavioral sleep interventions, and use validated measures of sleep, including questionnaires, actigraphy, or polysomnography.
Footnotes
Acknowledgments
Erica Kesse assisted with the formatting of the manuscript, including the table. This work was performed at Vanderbilt University Medical Center and presented in abstract form at the annual meeting of the Associated Professional Sleep Societies SLEEP 2012.
Author Contributions
AR wrote the first draft of the manuscript and BAM supervised the submission of the manuscript. BAM also reviewed the manuscript and made editing suggestions related to content and readability.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Vanderbilt Institutional Review Board approved this study.