
Abstract
We reviewed neurologic complications after renal transplantation in children over a 20-year period. Neurologic complications were classified as early (within 3 months) and delayed (beyond 3 months). Of 115 children, 10 (8.7%) had complications. Early complications were found in 4.35% of patients: seizures in 4 (posterior reversible leukoencephalopathy syndrome due to immunosuppressant toxicity [2], sepsis/presumed meningitis [1], and indeterminate [1]) and headaches in 1. One patient with seizures received levetiracetam for 6 months and 1 with headaches received amitriptyline prophylaxis. Late complications were noted in 4.35% of patients: seizures in 3 (posterior reversible leukoencephalopathy syndrome due to hypertension [2], hypertensive encephalopathy [1]), headaches in 2, and tremors in 1. Two patients with seizures were treated with anti-epilepsy medications; 1 with migraine received cyproheptadine prophylaxis. Neurologic complications develop in children after renal transplantation. Seizures due to posterior reversible leukoencephalopathy syndrome were the commonest complication. Early detection and appropriate management of these complications is important.
Keywords
Kidney transplantation is the most effective renal replacement for patients with end-stage renal failure. The kidney is the most frequently transplanted organ worldwide. Advances in the field of organ transplantation and improvements in surgical techniques and perioperative care have reduced the mortality and morbidity of transplantation. 1 The 1-year patient survival rate after renal transplantation in adults is close to 100%, with an estimated 85% to 95% graft survival rate. 2 Patient and graft survival rates of pediatric renal transplant recipients are also excellent. 3,4 Neurologic complications in transplant recipients are an important cause of morbidity and mortality. 1,5 Neurologic complications could be seen in up to 30% of recipients after renal transplantation in adults. 6 –10 Neurologic complications can develop secondary to the transplantation itself, because of immunosuppressant medications used to prevent transplant rejection or because of the inherent disorders that led to transplantation, as well as a combination of all the above factors. 5
The range of indications for renal transplantation in pediatric patients differs from that in adults, and therefore a different spectrum of complications would be expected. There are only a few studies where the authors looked into the spectrum of neurologic complications in pediatric renal transplant recipients. 11 –14 In this study, we reviewed the neurologic complications noted following renal transplant in pediatric patients from a single tertiary care center in the United States.
Methods
The study was approved by the Cleveland Clinic Institutional Review Board. All patients (age ≤21 years at the time of renal transplantation) who underwent transplants at the Department of Pediatric Nephrology, and Transplant Surgery, Cleveland Clinic, Ohio, and maintained in the pediatric renal transplant database over a 20-year period (1990-2010) were included in the analysis. The charts were reviewed retrospectively and the following data were recorded: demographics, indication for renal transplantation, spectrum of neurologic complications after renal transplantation, the time of onset of each complication, diagnostic workup, treatment, and follow-up. Depending on the nature of the neurologic complications, the following investigations were done: serum chemistry panel, serum trough level of the immunosuppressive agents, blood counts, and coagulation profile. Electroencephalography (EEG), computed axial tomography (CT), or magnetic resonance imaging (MRI) of the brain was performed when clinically indicated. We defined neurologic complications as those based on history and neurologic examination, and/or investigations performed after renal transplantation. All patients who presented with neurologic complications either in the inpatient or outpatient settings were evaluated by a pediatric neurologist.
Statistical Analyses
We divided neurologic complications after renal transplantation into 2 subgroups: (A) early (within 3 months of transplantation) and (B) delayed (> 3 months after transplantation). Descriptive statistics regarding age, sex, neurologic complications, and mortality were calculated for each group.
Results
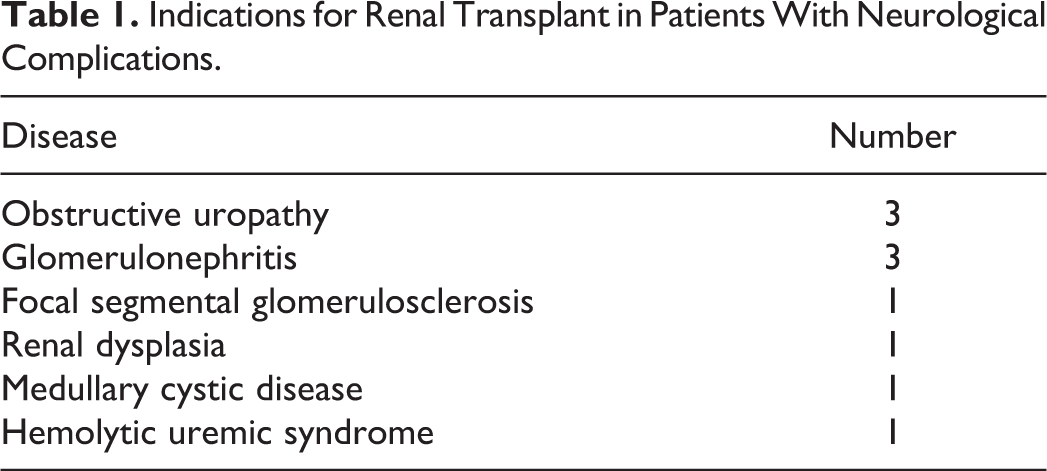
We reviewed the records of 115 patients in our pediatric renal transplantation database. We found 10 patients (8.7%) with neurologic complications; 5 were females. The mean age at the time of renal transplantation was 15.3 ± 3.6 years (range = 9 months to 21 years). Indications for renal transplantation in patients who had neurologic complications included a spectrum of disorders (Table 1). Two common indications were obstructive uropathy (3/10) and glomerulonephritis (3/10).
Indications for Renal Transplant in Patients With Neurological Complications.
Characteristics of Group A
Clinical
Five patients (5/115, 4.35%) had neurologic complications within 3 months of renal transplant (Table 2). Their mean age at the time of transplantation was 14.6 ± 2.6 years (range 10-16 years), 3 were males. The most common neurologic complication in this group was seizure, noted in 4 patients (4/115, 3.6%). The seizures were generalized tonic-clonic in all except 1. Among the patients with seizures: 2 had posterior reversible leukoencephalopathy syndrome because of the toxic level of tacrolimus in one (trough level 23.5 ng/mL in the patient, normal 5-20 ng/mL, Figure 1) and to toxic level of cyclosporine in one (trough level 520 ng/mL the patient, normal 100-400 ng/mL), one had septicemia and presumed central nervous system infection, and in another the cause was indeterminate. One patient developed headaches (1/115, 0.9%). The headaches eventually became chronic daily headaches. Neurologic examination was nonfocal in all of them.
Early (<3 Months) Neurologic Complications Following Renal Transplantation (Group A).
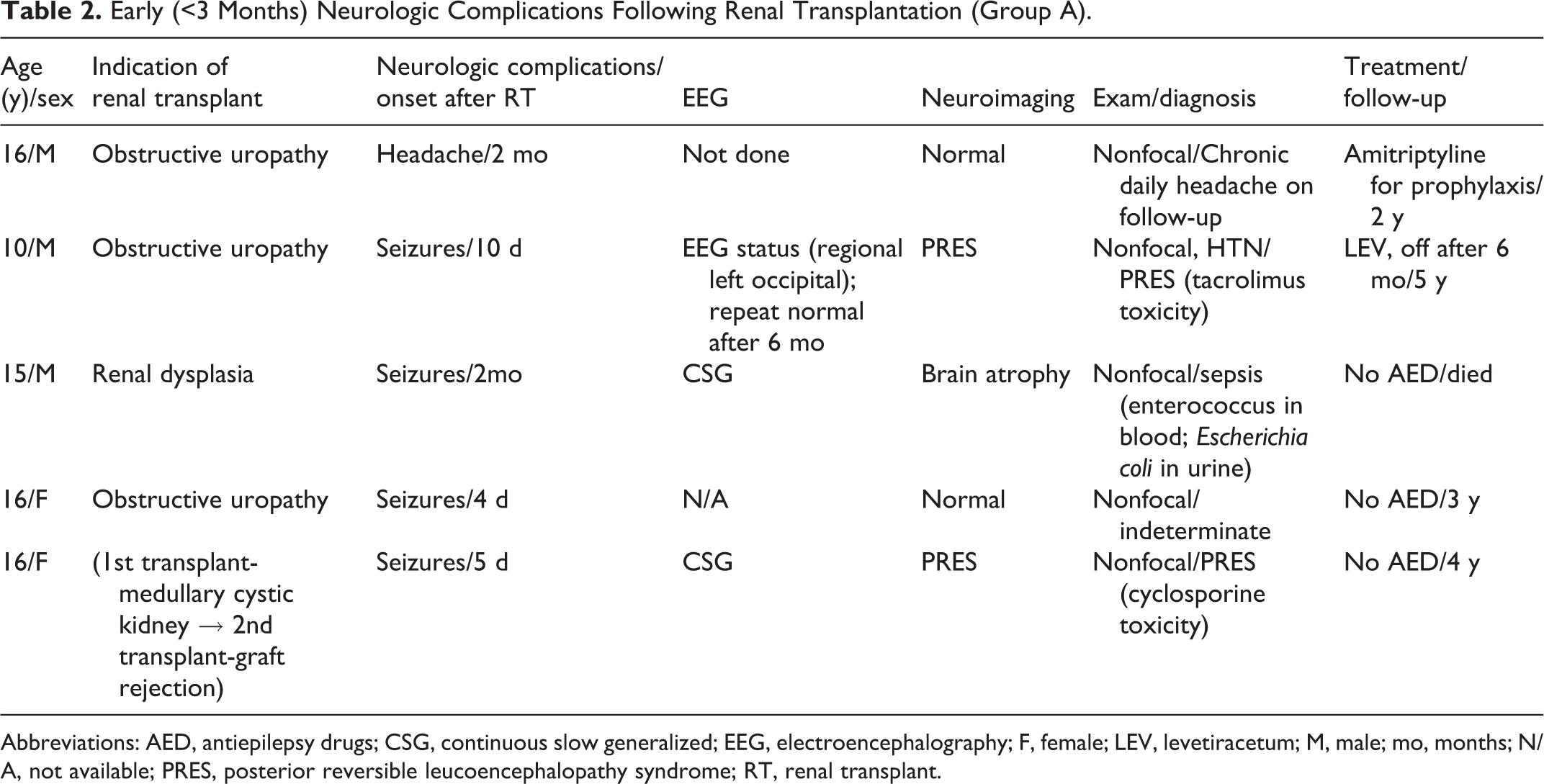
Abbreviations: AED, antiepilepsy drugs; CSG, continuous slow generalized; EEG, electroencephalography; F, female; LEV, levetiracetum; M, male; mo, months; N/A, not available; PRES, posterior reversible leucoencephalopathy syndrome; RT, renal transplant.
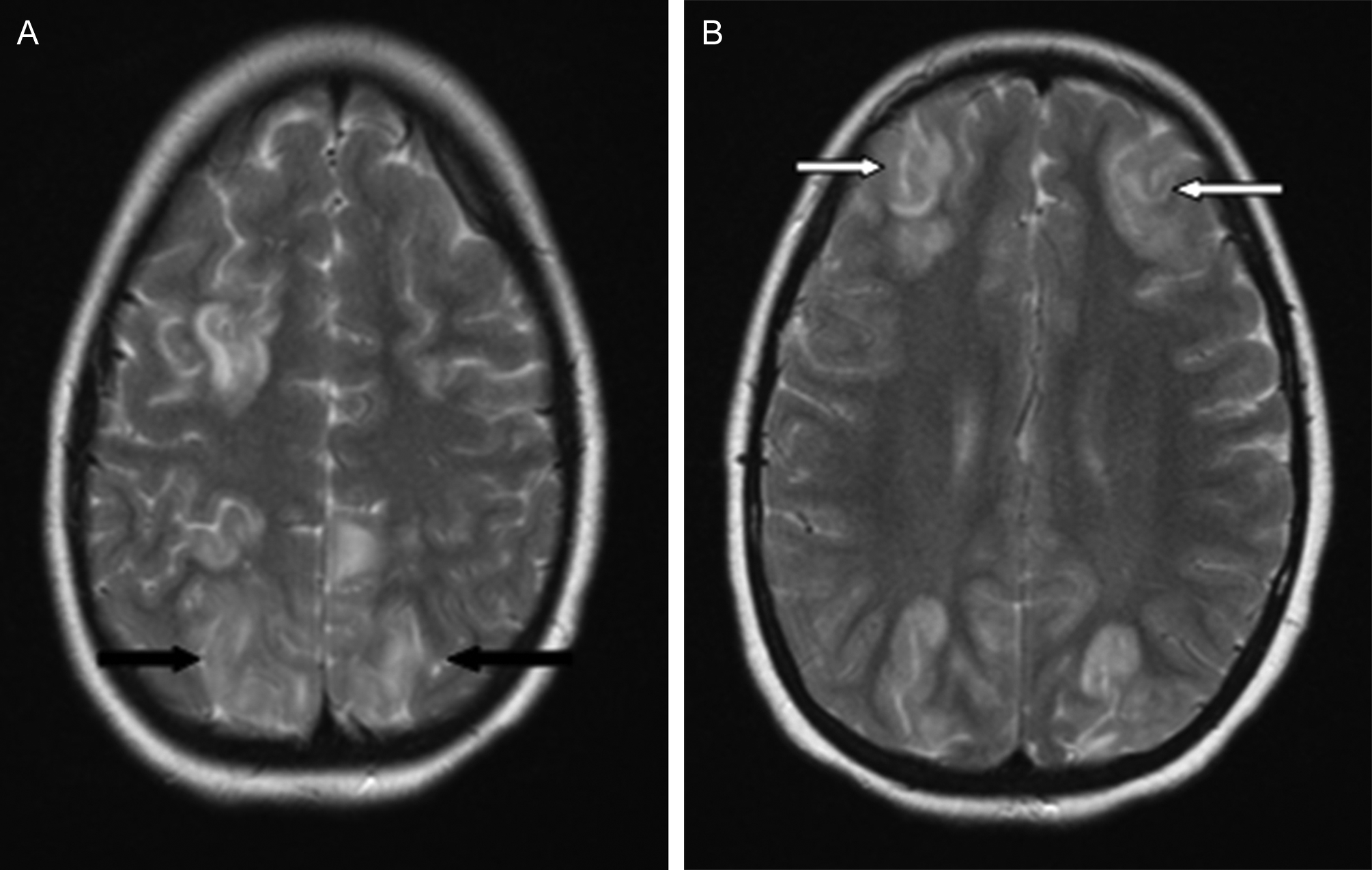
MRI brain. Axial T2-weighted images showing bilateral parieto-occipital (A, black arrows) and bifrontal (B, white arrows) hyperintensities suggestive of posterior reversible leukoencephalopathy syndrome in a patient with tacrolimus toxicity in the early neurologic complication group.
Investigations
In this group, neuroimaging (CT/MRI brain) was abnormal in 3 of 5 patients. The neuroimaging abnormalities included posterior reversible leukoencephalopathy syndrome (2) and brain atrophy (1). Electroencephalogram was available in 3 patients. Electroencephalographic findings were generalized background slowing in 2, and left occipital seizures in 1 patient with posterior reversible leukoencephalopathy syndrome. Spinal fluid analysis could not be performed in the patient with septicemia because of severe illness.
Follow-Up
The mean follow-up period was 2.8 ± 1.8 years (range 2 months to 5 years). One patient died because of septicemia from Enterobacter species and Escherichia coli. Neurologic examination remained normal on follow-up in the remaining patients. One patient (with electrographic seizures) was treated with levetiracetam, which was tapered and stopped after 6 months without any seizure recurrence. The patient who eventually developed chronic daily headaches did well with amitriptyline prophylaxis.
Characteristics of Group B
Clinical
We found 5 patients (4.35%) in this group; 3 were females (Table 3). Their mean age at the time of renal transplantation was 16 ± 4.6 years (range 9-21 years). The following complications were noted in this group: seizures (3, 2.7%), headaches (2, 1.8%), and tremors (1, 0.9%). Two patients had both seizures and headaches. Neurologic examination was nonfocal in all. Among the patients with seizures, 2 had posterior reversible leukoencephalopathy syndrome due to hypertension (normal immunosuppressant drug levels) and 1 had hypertensive encephalopathy. Seizures were generalized in all of them. The etiology of headaches was migraine without aura in both the patients with headaches. Headaches developed independently after the onset of seizures in those 2 patients. The tremors were postural and were attributed to tacrolimus.
Delayed (>3 Months) Neurologic Complications Following Renal Transplantation (Group B).
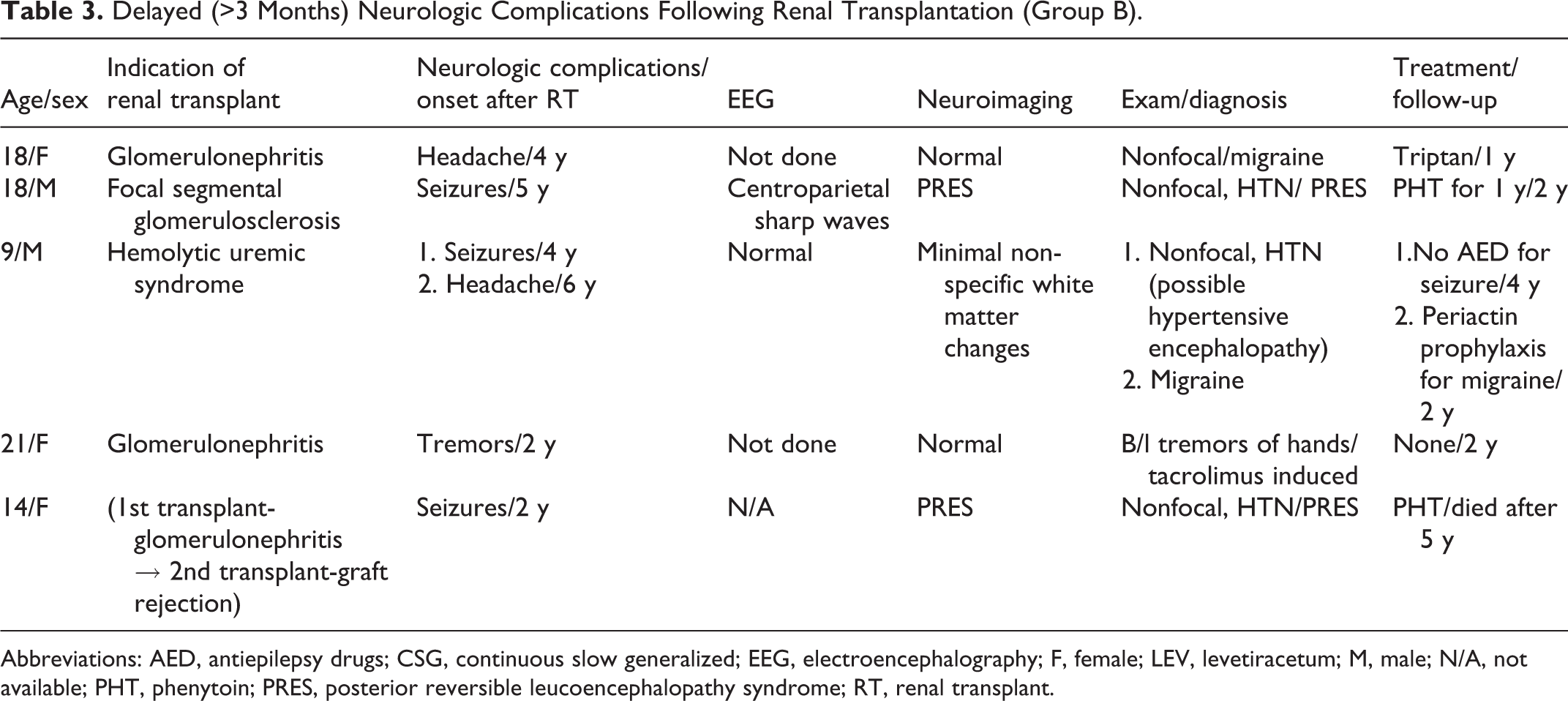
Abbreviations: AED, antiepilepsy drugs; CSG, continuous slow generalized; EEG, electroencephalography; F, female; LEV, levetiracetum; M, male; N/A, not available; PHT, phenytoin; PRES, posterior reversible leucoencephalopathy syndrome; RT, renal transplant.
Investigations
Neuroimaging abnormalities were noted in 3 of 5 patients: posterior reversible leukoencephalopathy syndrome in 2 and nonspecific white matter changes in the patient with hypertensive encephalopathy. Electroencephalogram was available for 2 patients: one had centroparietal sharp waves whereas the other was normal.
Follow-Up
On follow-up over a mean of 2.8 ± 1.6 years (range 1 to 5 years), 1 patient died due to nonneurologic complication. Neurologic examination was unchanged in all patients at the time of last follow-up. Two patients with seizures were started on phenytoin, but it was tapered and stopped in one after 1 year. One patient with migraine was on cyproheptadine prophylaxis while the other was on sumatriptan for breakthrough headaches.
Both Groups Combined
Overall, combining the 2 groups we noted the most common neurologic complication following renal transplantation was seizures (7/115, 6.1%) followed by headaches (3/115, 2.7%) and tremors (1/115, 0.9%). Death occurred in 1 patient in each group.
Discussion
Few authors have systemically investigated neurologic complications in pediatric patients after renal transplantation. 11 –14 In our series of 115 pediatric renal transplant recipients, 10 (8.7%) had neurologic complications. The incidence of neurologic complications after renal transplantation is variable and ranges from 8% to 30% in adults. The exact incidence in the pediatric age group is difficult to determine as most of the studies are case reports and small series. The authors of one study reported severe central nervous system complications in 7 of 36 (19%) children after renal transplantation. 11
Seizures are one of the most common severe neurologic complications after renal transplantation. 15 –18 Various etiologies of seizures after renal transplantation include metabolic derangements (electrolyte disturbances like hyponatremia, hypocalcemia and hypomagnesemia, and hepatic and renal derangements), sudden elevation of blood pressure, treatment with immunosuppressive agents (cyclosporine, tacrolimus), hypoxic-ischemic injury, cerebral structural lesions (ischemic or hemorrhagic strokes), and central nervous system infections. 1,2,15 –18 Seizures were the most common neurologic complication noted in our series (7/115, 6.1%). In children, the incidence of seizures after renal transplantation varies from 17% to 20% in 2 studies; one of which was in the precyclosporine era 19 and the other was in the pretacrolimus era. 13 The reduced incidence of seizures in our study could be related to advances in the field of organ transplantation and improvements in surgical techniques and perioperative care. None of our patients had a seizure before renal transplant, indicating that seizures most likely developed as a complication after the transplantation rather than a preexisting condition as noted in some children in the prior studies. 13,19 According to the existing literature, the majority of the seizures are noted in the first 2 months after renal transplantation. 13 In our study, seizures developed both within and beyond the 3-month period after renal transplantation, though they were more common in the early group (4 vs 3). The most common seizure type was generalized tonic-clonic, which is comparable to the existing literature. In our cohort, etiology of seizures was posterior reversible leukoencephalopathy syndrome (n = 4), presumed central nervous system infection (n = 1), hypertensive encephalopathy (n = 1), and indeterminate (n = 1). In previous studies, the causative factors leading to seizures in children were hypertension (most common), graft rejection, infection, and immunosuppressive medications. Most of our patients had good response to antiepilepsy medications and did not have seizure recurrence as noted in prior studies, too. 13,19 Of the 7 patients with seizures, 3 were started on antiepilepsy medications. The antiepilepsy medications were tapered and stopped in all except one. One patient died as a result of septicemia and presumed central nervous system infection in the immediate posttransplant period whereas another died as a result of nonneurologic complications several years after renal transplantation.
Posterior reversible leukoencephalopathy syndrome is a clinicoradiological entity. The characteristic symptoms include acute onset of neurologic dysfunction in the form of seizures, headaches, and visual disturbances. 20 Common causes include sudden rise of blood pressure, eclampsia, renal failure, or use of immunosuppressive agents. The pathogenesis of posterior leukoencephalopathy syndrome is not fully understood but is believed to be due to a breakdown in cerebral autoregulation that results in leakage of fluid into the interstitium. The characteristic radiologic findings are bilateral grey and white matter edema predominantly in the posterior regions of the cerebral hemispheres. 21 The immunosuppressive agents used after transplantation are often associated with this complication, the reported incidence ranges from 1% to 6%. 22 In our series, 4 patients had posterior reversible leukoencephalopathy syndrome (3.6%), which is comparable to the existing literature. In children, however, the true incidence of posterior reversible leukoencephalopathy syndrome after renal transplantation is unknown. We have observed that in the early group, posterior reversible leukoencephalopathy syndrome was due to immunosuppressant toxicity, and in the delayed group it was due to sudden elevation of blood pressure from some other etiology.
Headache is a recognized neurologic complication of organ transplantation. In a study of 83 adult consecutive kidney transplant patients who underwent neurologic examination and a detailed headache history, 44.5% had headache. 23 The incidence of headaches in children after renal transplantation is not well described but noted in 6% of patients after pediatric liver transplantation. 24,25 Headaches after organ transplantation present as new-onset headaches or worsening of a primary headache disorder like migraine. 26 Immunosuppressive agents like cyclosporine and tacrolimus with their vasoactive properties are thought to play a role in the development of headaches; the exact mechanisms by which they induce or exacerbate headaches, however, are unknown. 27 Though post-transplant headaches are considered a minor complication, they can have a significant negative effect on quality of life. 28 There is a report of development of pseudotumor cerebri with impairment of vision in 2 children 5 years after renal transplantation. 29 In addition to primary headache disorders, intracranial pathologies like posterior reversible leukoencephalopathy syndrome, stroke (arterial/venous, ischemic/hemorrhagic), meningitis/encephalitis, brain abscess, and brain tumors can lead to headache after renal transplantation. 5 In our series, we found 3 patients (2.7%) who had headaches, manifesting mainly in the delayed subgroup. This finding is comparable with one previously reported. 23 The cause of headaches was attributed to migraine without aura in 2 and chronic daily headaches in 1, which is similar to the study by Maggioni et al 23 in which they have found migraine without aura and episodic tension-type headaches as the most common causes. Immunosuppressant-related headaches are very rare. Two of our patients did well with headache-prophylaxis medications whereas another received headache-abortive medication only. None of our patients had underlying serious intracranial pathology leading to headaches.
Tremor is described as a frequent neurologic complication after organ transplantation as reported in up to 50% of pediatric renal transplant recipients related to tacrolimus by the authors of a small study. 12 In our study, only 1 patient developed tremors several months after renal transplantation on a stable dose of tacrolimus. Her tremors were mild and did not interfere with functioning, so the tacrolimus dose was not modified, a finding also observed in the previous study. 12 The relatively low incidence in our study might be due to the fact that the tremors were too mild to be reported by the patients or their caregivers.
Several other neurologic complications reported after renal transplantation include stroke, encephalopathy, central nervous system infections, cerebellar ataxia, brain tumors, and peripheral neuropathy. 5 Stroke can be ischemic or hemorrhagic and can involve cerebral arteries or venous sinuses, with an incidence of about 8% in renal transplant recipients. 30 They are common in adults as hypertension, hyperlipidemia, and diabetes are frequent comorbidities leading to vascular compromise. In addition, a uremic state is associated with increased atherogenesis, thus increasing the risk of arterial ischemic strokes. 5 In children with longstanding nephrotic syndrome, particularly in patients with the congenital nephritic syndrome of the Finnish type, hyperlipidemia can predispose to premature atherogenesis, thus increasing the likelihood of development of arterial ischemic stroke. 31 None of our patients had stroke. Encephalopathy following renal transplantation could be multifactorial: drug induced (calcineurin inhibitors, steroids), metabolic derangements, uremia, and hypoxia-ischemia. 5 It was not observed in our cohort. Central nervous system infections (meningoencephalitis or brain abscess) in the setting of renal transplantation are mainly caused by opportunistic infections like mycobacteria, cryptococcus, aspergillus, listeria, and toxoplasma. In addition, community-acquired bacterial pathogens are also encountered. 5 One of our patients who had septicemia and developed seizures was too sick to undergo lumbar puncture to confirm meningitis.
Neuropathy after renal transplantation can be due to local compression of the nerve trunks (like femoral nerve) leading to mononeuropathy or due to generalized peripheral neuropathy from long-standing uremia, associated diabetes mellitus, side effects of immunosuppressant medications (calcineurin inhibitors) and Guillain-Barré syndrome. 5 None of our patients had objective clinical findings of neuropathy or reported paresthesias.
There are some limitations to our study. First, it was retrospective in nature and thus carries the limitations inherent to this methodology. Another limitation was lack of uniformity among the indications for renal transplantation and posttransplant treatment regimen in patients spread over a 20-year period.
Conclusions
Neurologic complications can develop in children after renal transplantation. It is of utmost importance that the transplantation team collaborates with pediatric neurologists to ensure prompt and accurate diagnosis of these complications and to institute appropriate management. Seizures were the most common neurologic complication and posterior reversible leukoencephalopathy syndrome was the predominant underlying etiology. These complications can develop in the early as well as delayed period after renal transplantation.
Footnotes
Acknowledgments
The work was done at the Pediatric Neurology Center and Department of Nephrology, Cleveland Clinic, Cleveland, Ohio. The paper was presented as a poster at the Child Neurology Society Annual Meeting in 2012 at Huntington Beach, California.
Author Contributions
PSG, MK, and JC collected and organized the data. PSG wrote the manuscript (including the first draft). DG conceptualized the study. DG and CK verified the results and revised the manuscript at all stages.
Declaration of Conflicting Interests
The authors declared the following potential conflict of interest with respect to the research, authorship, and/or publication of this article: Debabrata Ghosh received a one-time consultation fee of $1500.00 from Merz Inc. in January 2013. No other authors report any conflict of interest pertaining to this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board at the Cleveland Clinic (IRB #: 11-593).