
Abstract
Scorpion envenomation is a life-threatening health problem in tropical and subtropical regions, particularly among children. The aim of this study was to describe the epidemiologic characteristics, clinical profile, and prognosis of neurologic complications among children with scorpionism in Upper Egypt. In this retrospective study, the neurologic complications of scorpionism in 2 university hospitals were analyzed from the points of epidemiologic and clinical picture and outcomes. The neurologic manifestations were found at a high percentage (85%). Irritability was the main manifestation (83.4%), followed by sweating (81.5%), hyperthermia (33.6%), and priapism (48.2% of males). Moreover, convulsion and coma were found in 14.7% and 11% of children, respectively. Neurologic manifestations were common in children with scorpionism and they correlated with poor outcome. Identification of epidemiologic and clinical features of central nervous system complications of scorpionism in children provide important data, helping in development of management policies aiming at preventive control of scorpionism and decrease its mortality.
Envenomation by scorpion stings is a major public health problem in numerous tropical countries because of its frequent incidence and potential severity, especially among children, who experience the most severe cases. There are approximately 1900 known scorpion species in the world, and only about 30 are recognized to be potentially dangerous for humans. 1 -3 Previous literature on scorpion taxonomy recognizes 16 scorpion families, and all scorpions hazardous to humans belong to the Buthidae family, but among this family, the species belonging to the genera Androctonus and Leiurus are considered the most significant to humans, causing a large number of envenomations in Africa and Middle East. 3 -6 “Leirus Quinquestriatus, known as the Egyptian scorpion, or ‘Death stalker,’ has been isolated from upper Egypt.” 3 Scorpion venom shows variability by subspecies and has a complex structure composed of neurotoxic proteins, salts, acidic proteins, and organic compounds, thereby having neurologic, cardiovascular, hematologic, and renal side effects, in addition to its local effects. 4 Medically significant scorpion stings are characterized by intense local pain without local tissue injury. Systemic effects occur in a smaller proportion of scorpion stings depending on scorpion species involved. 1,2,4,5 Envenomation severity depends on the scorpion species, its size, the amount of venom inoculated, the victim’s body mass, and the patient’s sensitivity to poison. Additionally, climatic situations, heat and dryness, are also significant risk factors. 2 Early diagnosis, time interval between the sting and the antivenin injection, together with maintenance of the victim’s vital functions, all can interfere in the patient’s outcome. 5 Most of the symptoms of scorpionism are due to either the release of catecholamines from the adrenal medulla or the release of acetylcholine from postganglionic parasympathetic neurons. The adrenergic signs occur at a low venom dose, while cholinergic signs occur at high venom dose concentrations. Furthermore, the adrenergic phase tended to be more dependent on the venom dose than the cholinergic phase. However, dual manifestations of the adrenergic and cholinergic signs are possible because of varying organ system sensitivities to these neurotransmitters. Catecholamine-induced multiple-organ failure among scorpion-envenomed children has been reported by many investigators. Cardiorespiratory manifestations, mainly cardiogenic shock and pulmonary edema, are more frequent in children. 3 -6 Moreover, the presence of neurologic manifestations, mainly coma and convulsion, are also signs of a severe form of scorpion envenomation associated with a poor prognosis. 7
Epidemiologic data of scorpionism are important not only to improve our understanding of the condition but also to allow a rational approach in planning health services. The early diagnosis of neurologic and other systemic complications would be valuable because earlier identification of patients at highest risk would allow for proper planning for the first aid and intervention strategies targeted to those population groups. Despite the medical importance regarding neurologic complications of scorpionism and the increasing number of registers in many studies, the epidemiologic and clinical data on neurologic manifestations of scorpionism in children are limited. In addition, the frequency of these central nervous system complications among the Egyptian children with scorpion envenomation is currently unknown. Therefore, we conducted this work to evaluate some epidemiologic characteristics, clinical data of neurologic complications, and prognostic factors secondary to scorpionism among our studied populations.
Patients and Methods
This was a 2-year retrospective study of the medical records of children diagnosed with scorpionism who were admitted in 2 university hospitals, South Valley University and Assiut University, from May 2013 to May 2015 after approval from Qena Faculty of Medicine Ethical Committee.
Study Subjects
Assiut University and South Valley University hospitals are tertiary referral centers in Upper Egypt receiving patients from primary and secondary health centers. Children with scorpionism (<18 years) presented to our Emergency Units, where preliminary assessment and management were provided. Diagnosis depended on positive history of scorpion sting. The guidelines of our hospitals are to hospitalize all children with scorpionism for observation. All patients in our study were admitted. On admission, all patients received scorpion antivenin (if not given at their local medical service) together with antihistamine and corticosteroid. Patients with no systemic manifestations were sent to the intermediate care unit for observation for at least 24 hours. Children with severe envenomation were transferred to the intensive care unit. Inotropic medications and mechanical ventilation were decided if the patient was indicated.
Methods
Patients’ medical files were retrospectively reviewed for their clinical and demographic data, including the age, sex, vital signs (heart rate, respiratory rate, systolic and diastolic blood pressure), body temperature, and Glasgow Coma Scale (GCS) score. Glasgow Coma Scale scores ≤14 were considered having disturbed consciousness level, whereas those with Glasgow Coma Scale scores ≤12 were considered to have coma. The presence of shock (defined as systolic blood pressure 2 standard deviations below normal), pulmonary edema, and respiratory distress were recorded. Other data included characteristics of the stings and the time elapsed between sting and admission to the hospital. Neurologic manifestations, such as the presence of coma, convulsions, priapism, and the presence of any autonomic manifestations, were also investigated. Using Abroug’s clinical severity classification, 8 we grouped our patients into class I, local signs, including local pain, erythema, and paresthesia restricted to the sting area; class II, shivering, fever, excessive sweating, nausea, vomiting, diarrhea, hypertension, and priapism; and class III, cardiovascular, respiratory, or neurologic complications such as a disturbed conscious level and convulsions.
Laboratory investigations of the patients were reviewed for complete blood count, blood urea nitrogen, liver function tests, creatine phosphokinase, lactate dehydrogenase, arterial blood gases, and serum electrolytes, including sodium, potassium, and calcium.
Statistical Analysis
Analysis of data was done using SPSS version 20. Values were recorded as mean and standard deviation. Differences in proportions were compared by the chi-square test. P values <.05 were considered significant.
Results
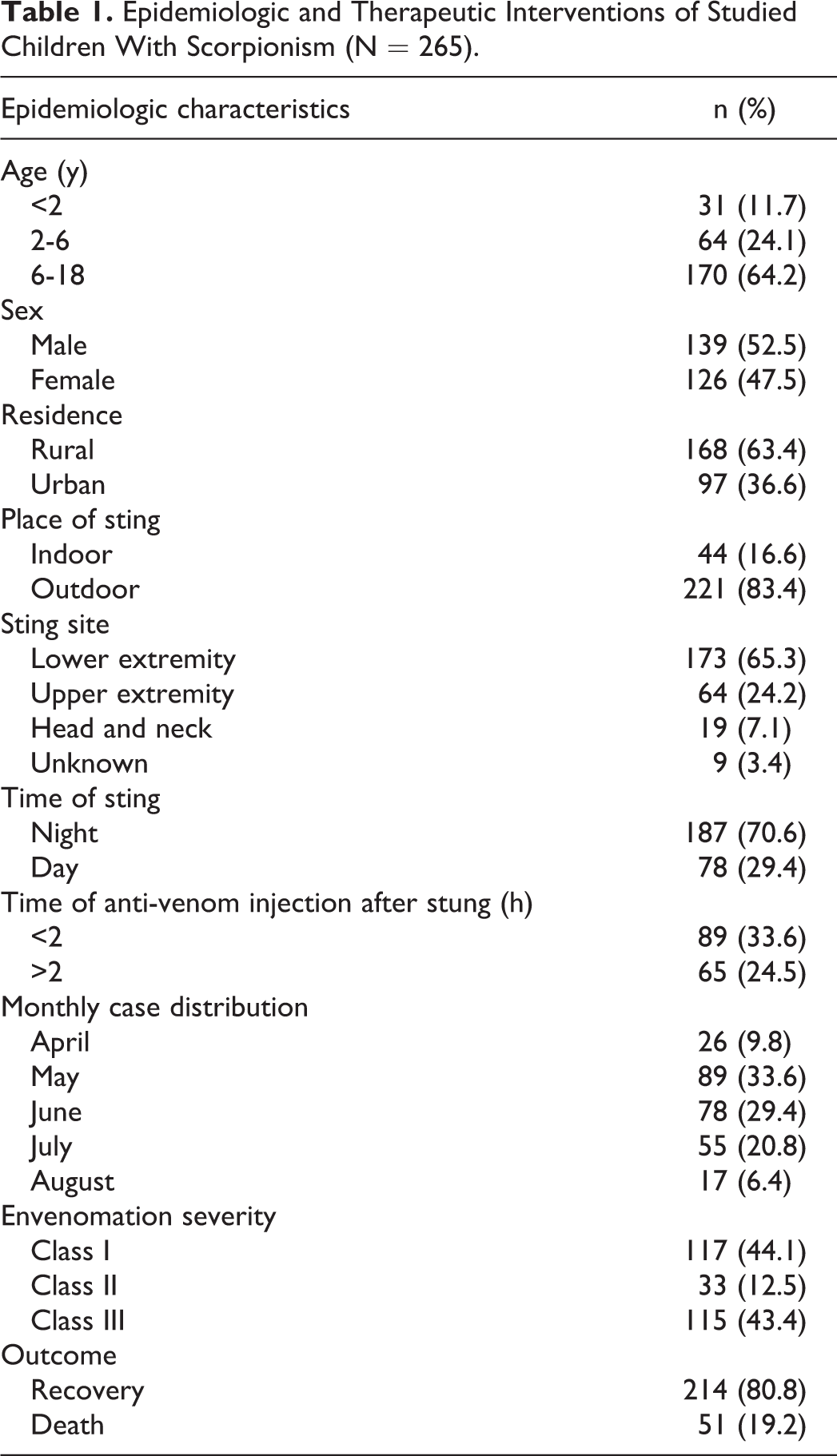
A total of 265 children with scorpionism were recruited during the 24-month period. Of the victims, 52.5% (n = 139) were boys and 47.5% (n = 126) were girls, with a mean age of 7.8 ± 5.2 (range from 1 to 16 years). Table 1 demonstrates the demographic and therapeutic interventions of the studied children with scorpion envenomation. It was observed that 64.2% of the participants were aged more than 6 years, 63.4% lived in rural areas, and the majority (83.4%) were exposed to the sting outdoors and at night (70.6%). Regarding the sting site, 65.3% of the patients were stung at lower extremities, whereas 24.2% were stung at upper extremities. As for the time of antivenom injection after being stung, more than half (57.7%) received it at less than 2 hours. More than two-fifths (44.1% and 43.4%, respectively) suffered from envenomation severity class I and III. Recovery was reported among 80.8% of the studied patients, whereas death was reported among 19.2%. The monthly case distribution of our patients with scorpionism occurred during the hot months from April to August (Table 1).
Epidemiologic and Therapeutic Interventions of Studied Children With Scorpionism (N = 265).
The frequency of neurologic manifestations was depicted in Table 2. It was found at a high percentage (85%). Irritability was the main manifestation (83.4%), followed by hypersweating (81.5%). A disturbed consciousness level (Glasgow Coma Scale score ≤14) was observed in 66 patients (25%); 29 (11%) had coma (Glasgow Coma Scale score ≤12), whereas 39 patients (14.7%) had seizures. Other central nervous system signs were also noted, such as hyperthermia (33.6%), hypothermia (24.5%), miosis (4.5%), and mydriasis (5.7%). Finally, priapism was reported in 67 patients (48.2% of males). Systemic and autonomic manifestation were reported as well: tachycardia (79.2%), hypertension (54%), bradycardia (20.8%), and hypotension (15.8%).
The Frequency of Neurologic and Systemic Manifestation of the Studied Group (N = 265).
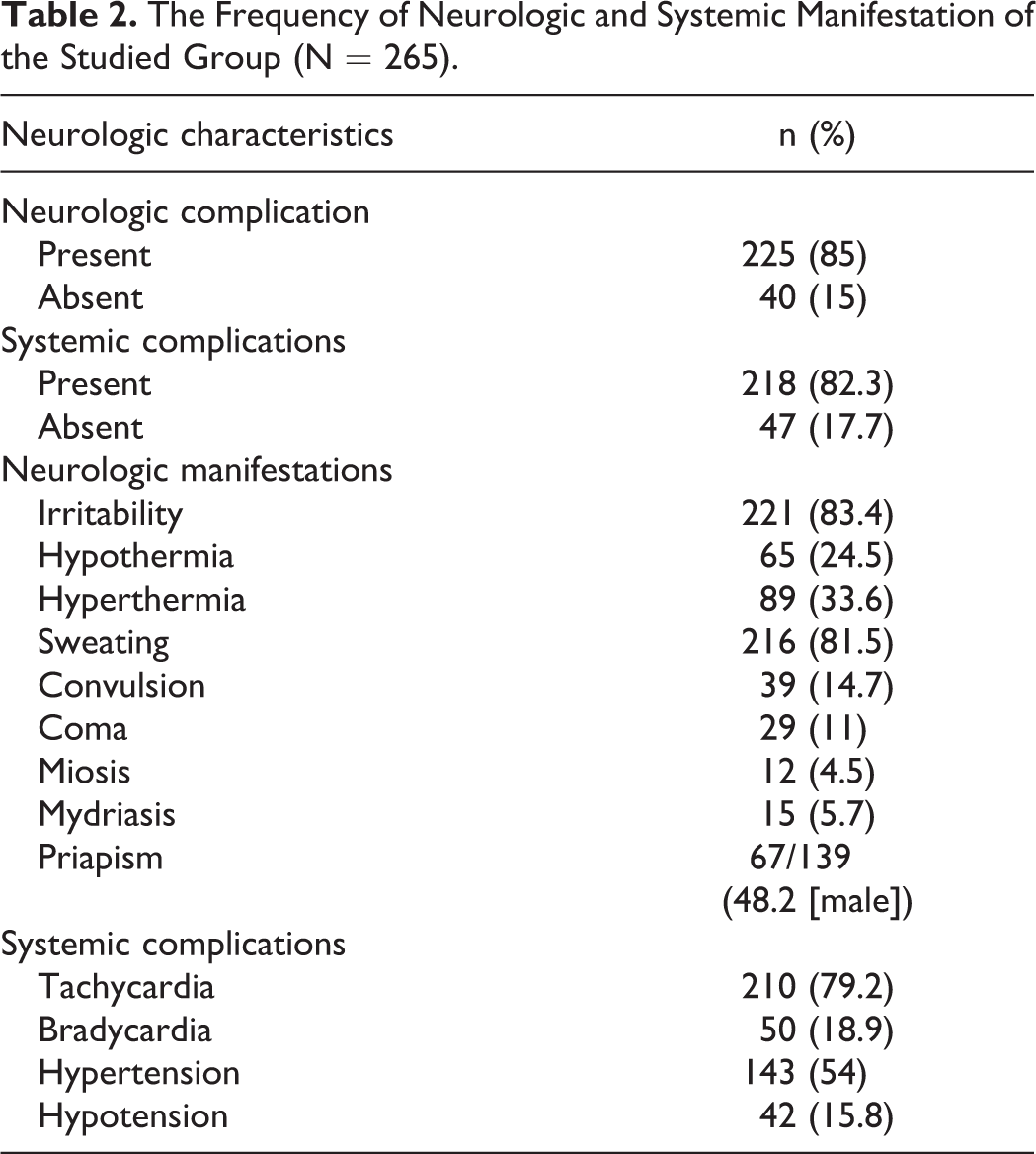
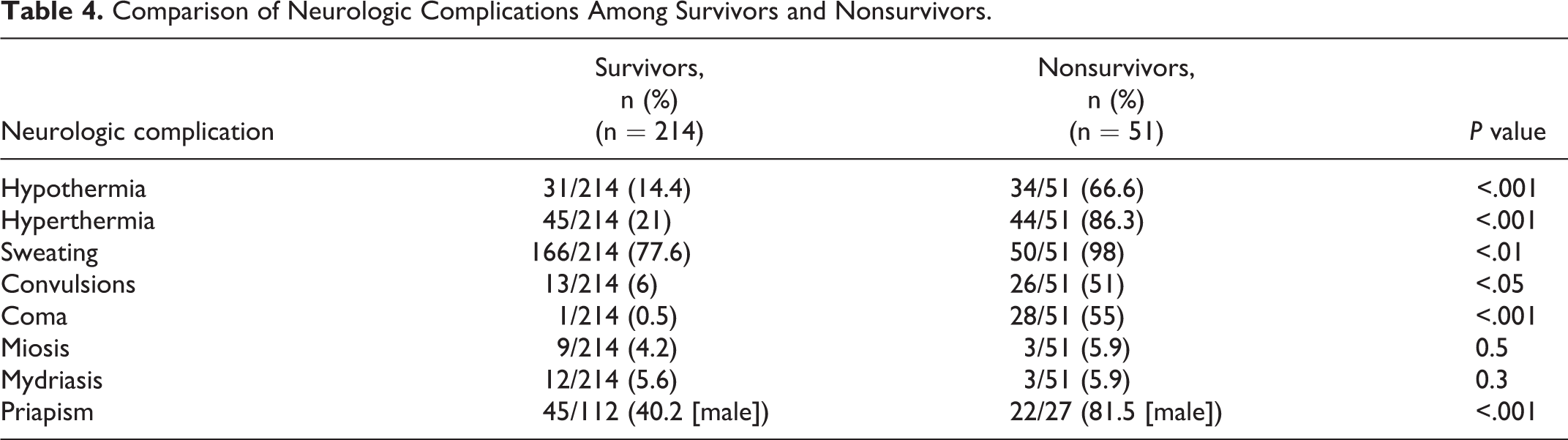
Table 3 indicates a statistically significant relation between the epidemiologic characteristics of survivors and nonsurvivors at all categories of age. In reverse, there is no significant relation between sex and district when comparing the survivors and nonsurvivors in the sample. Moreover, a statistically significant difference was found at the time of antivenom injection for both less than and more than 2 hours and class III envenomation severity. In addition, a statistically significant difference was noted in all forms of organ failure and therapeutic interventions among the studied survivors and nonsurvivors, including heart failure, pulmonary edema, gastrointestinal failure, renal failure, hematological failure, blood glucose levels, inotropic support, and mechanical ventilatory support. As illustrated in Table 4, a statistically significant difference was found in all aspects of neurologic complications except miosis and mydriasis between the studied survivors and nonsurvivors, including hypothermia (P < .001), hyperthermia (P < .01), sweating (P < .05), convulsions (P < .001), coma (P < .001), and priapism (P < .001).
Comparison of Epidemiologic and Therapeutic Interventions Among Survivors and Nonsurvivors.
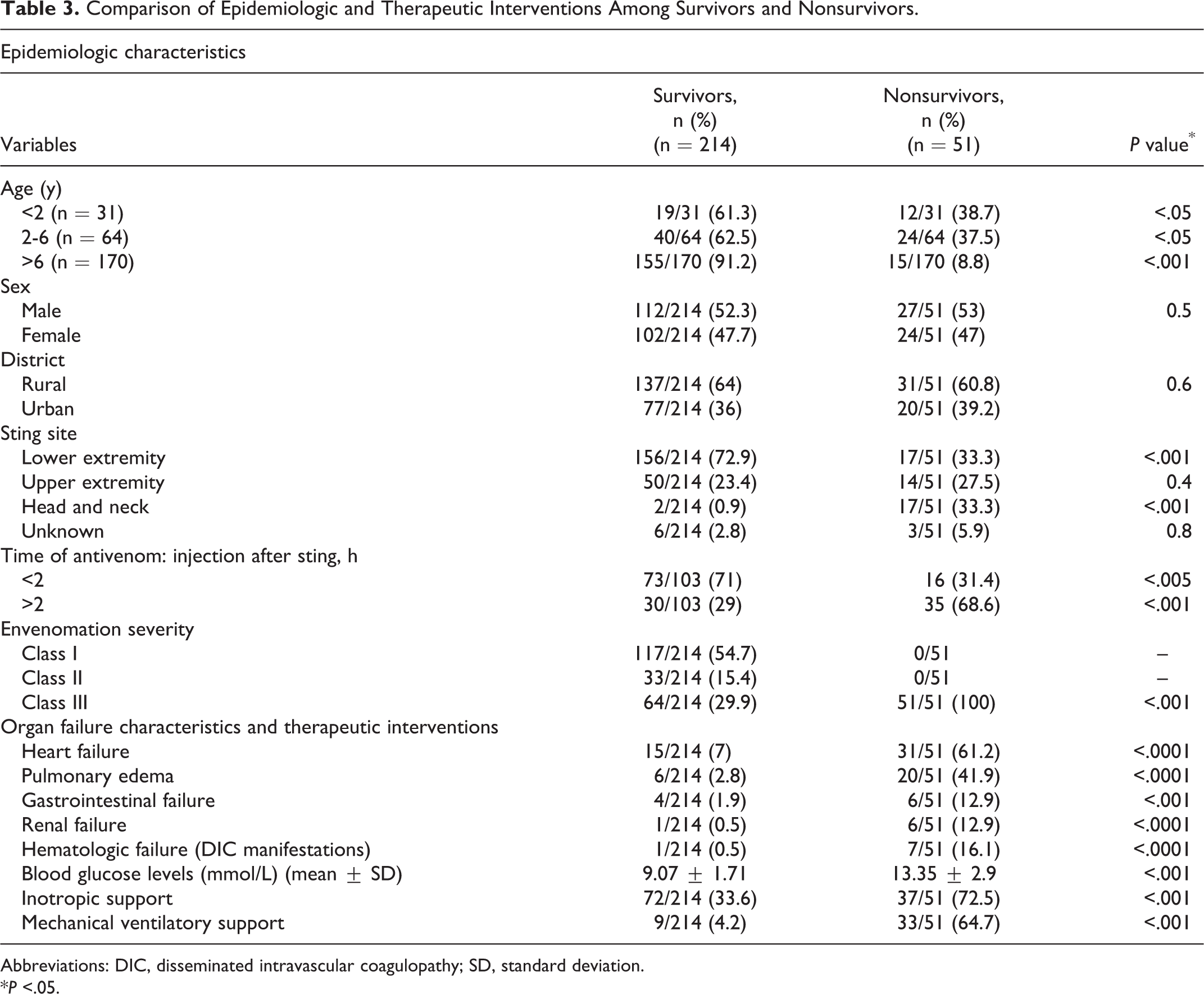
Abbreviations: DIC, disseminated intravascular coagulopathy; SD, standard deviation.
*P <.05.
Comparison of Neurologic Complications Among Survivors and Nonsurvivors.
Discussion
The epidemiology of the neurologic manifestations in children with scorpionism is poorly discussed in literature. However, scorpionism is a common medical, public health problem and a life-threatening hazard in many areas of the world including Egypt. 2 Scorpionism is a life-threatening emergency in children. 2,9 Children potentially are at a greater risk of organ damage and developing fatal conditions such as severe cardiac, respiratory, and neurologic complications after scorpionism. 9 In the present study, it was observed that neurologic manifestations were present at a high percentage (85%) (Table 2). Neurologic manifestations of scorpionism are considered as an indicator of the severity of scorpion sting. These signs are observed in nearly two-thirds of hospitalized patients. The presence of neurologic manifestations, mainly coma and convulsion, are also signs of a severe form of scorpion envenomation associated with a poor prognosis. 7
Our findings agree with those of Bahloul et al, 7 who reported 78% of scorpionism patients had neurologic complications due to scorpion envenomation. The mean age of patients was 14.7 years, ranging from 0.5 to 90 years. Six hundred eighty-five patients (72%) were younger than 16 years. Patients presented with impaired consciousness (21.9%), coma (15.4%), convulsions (5.9%), priapism (72.2%), hyperthermia (42.3%), miosis (4.5%), and mydriasis (1.7%). Brain edema had the poorest outcome in this study. The majority of victims’ neurologic complications were secondary to brain anoxia caused by pulmonary edema and cardiovascular failure. 7 In another study, 10 scorpionism was recorded in 302 patients, and 78.5% of them were younger than 18 years. Neurologic evaluation revealed noticeable autonomic manifestations, mainly sinus tachycardia (78.1%), vomiting (70.5%), and hyperthermia (53.2%). Other neuropsychiatric manifestations included agitation and restlessness (17.7%) and disturbance of consciousness (8.0%). Similar results were observed in a study in Saudi Arabia 11 that found neurologic complications had the most morbidity and are major causes of mortality in scorpion envenomation.
Fifty-four percent of our series had hypertension. Hypertensive encephalopathy is one of the most important predisposing factors for neurologic deterioration in patients with scorpionism. Forty-five to 70% of scorpionism victims have raised blood pressure ranging from 140/90 to 200-230/130-160 mm Hg reported within 30 minutes to 8 hours of the sting. 12 If untreated, the hypertensive effect is long lasting, and when the arterial blood pressure is excessive (sometimes exceeding the cerebral autoregulatory plateau), it leads to cerebral damage (edema and ischemia). Hyperreninemia and sympathetic stimulation results in rapid and significant rise in the level of epinephrine, norepinephrine, endothelin, and atrial natriuretic peptide as a result of sting by Buthidae species. 12 -15 Accumulation of angiotensin II accelerates the myocardial injury and oxygen demand. Alpha-receptors stimulation plays an important part in the pathogenesis of hypertension and pulmonary edema due to scorpion sting. 7,12 -15
The neurologic abnormalities in children with scorpionism can be explained by a direct action of the scorpion venom on the central nervous system. Scorpions’ venom is a mixture of numerous low-molecular-weight proteins, neurotoxins, nucleotides, amino acids, oligopeptides, cardiotoxins, nephrotoxin, hemolytic toxins, phosphodiesterase, phospholipase, hyaluronidase, and acetylcholine esterase. Several toxins in the venom of a single species of scorpion can produce potent synergic effects in the victim. 12,16,17 Although the wide range of clinical effects of scorpion venom reflects its multicomponent character, the most significant mechanism of action is at the level of excitable membranes and leads to its characterization as a neurotoxin. 18 Neurotoxins of scorpion venom are more lethal than those of snake venom. 12 The main molecular targets of scorpion neurotoxins are the voltage-gated sodium channels and potassium channels, including calcium-activated potassium channels. This explained why scorpion neurotoxins act mainly on the excitable cells of nerves and muscles. 12,17 Sodium and potassium channel toxins of scorpions’ venom mediate synergistic effects responsible for powerful and persistent depolarization of autonomic nerves with massive release of autonomic neuromuscular neurotransmitter, evoking an “autonomic storm.” 12 Systemic intoxication reflects overstimulation of the central nervous system and the sympathetic and parasympathetic nervous system. 7 Pro-inflammatory cytokines linked to the severely scorpion-envenomed patients are tumor necrosis factor (TNF)-alpha, interleukin (IL)-1 and IL-6, gelatinolytic, caseinolytic and hyaluronidase and metalloproteinase, which cause injury to the central nervous system and cardiovascular system. 16 Previous reports 7,19 have suggested the possibility of the scorpion venom crossing the hematoencephalic barrier in immature children, analogous to the passage of the venom in immature mammals. Furthermore, pulmonary edema and cardiogenic shock observed in severe scorpionism may lead to hypoxemia, with impairment of the neurologic status of these patients. 7
This and other previous studies all have pointed out that the frequency of stings increase in the warmest months of the year throughout the world. In addition, they stated a more frequent occurrence of stings in rural areas. 2,7,10,14,20
Our study demonstrated that delayed medical assistance constituted a negative impact on envenomation prognosis; hence, children who arrived at the hospital more than 2 hours after the accident presented a greater risk of unfavorable evolution as hinted in our findings. Further, 68.6% of nonsurvivors take the antivenom after more than 2 hours. In contrast, 86% of survivors were admitted to hospital and injected with the antivenom before 2 hours of the sting. Our results stand in line with other studies. 2,4,7,10,14,20
There are limitations to our study. The most important is that this was a retrospective chart review study, our data being limited to what was recorded on the patient records.
Footnotes
Author Contributions
KS, MAA, MGA, AEA, KAA, and MDA designed the study, followed the patients’ files and drafted the manuscript. AAE, GMH, and AME performed analyzed the data and the performed the revision process. All authors were involved in the critical analysis of the final version of the manuscript. All authors approved the manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Ethical Committee of Qena Faculty of Medicine, South Valley University, Egypt, approved the study. The work has been carried out in accordance with the code of Ethics of the World Medical Association (Declaration of Helsinki).