
Abstract
The aim of this study was to see whether the scores of the Bayley Infant Neurodevelopmental Screener of 45 high-risk preterm infants (gestational age 26-37 wk) between the ages of 3 and 24 months predicted neurodevelopmental status at 7 to 10 years of age. Neurodevelopmental status of 45/122 preterm infants, grouped according to their gestational ages of 26 to 29, 30 to 32, and 33 to 37 weeks, were previously evaluated by Bayley Infant Neurodevelopmental Screener. The scores were categorized as low or high-moderate. Verbal and performance scores of Wechsler Intelligence Scale for Children–Revised (WISC-R) of those patients were assessed between 7 and 10 years. The patients with high-moderate-risk scores of Bayley Infant Neurodevelopmental Screener at all times, regardless of their gestational age, had lower performance, verbal, and total scores of WISC-R than those of who had low Bayley Infant Neurodevelopmental Screener risk scores. High-moderate risk score of Bayley Infant Neurodevelopmental Screener at 7 to 10, and 16 to 20 months, of all patients especially showed good prediction for identifying lower verbal and performance scales. For 7 to 10 months, verbal scale: positive predictive value = 92.3%, negative predictive value = 44.4%, sensitivity = 70.58%, and specificity = 80%; performance scale: positive predictive value = 100%, negative predictive value = 30%, sensitivity = 68.18%, and specificity = 100%. For 16 to 20 months, verbal scale: positive predictive value = 90%, negative predictive value = 37.5%, sensitivity = 64.3%, and specificity = 80%; performance scale: positive predictive value = 90%, negative predictive value = 12.5%, sensitivity = 56.3%, and specificity = 50%. Bayley Infant Neurodevelopmental Screener shows good prediction of later verbal and performance scores of Wechsler Intelligence Scale–Revised for Children as early as 7 to 10 months, which gives us the opportunity to start early intervention.
Improved medical care of preterm infants has increased the number of such children surviving to school age. Many disciplines are engaged in studying the neurological development of preterm infants, and these researchers have generated a large body of literature. Some disabilities such as attention deficit and specific learning and speech disorders are subtle until preschool or school ages. Other deficits, however, such as poor vision, hearing defects, cerebral palsy, and significant developmental delay appear earlier. 1 –4 In high-risk clinics instituted to follow the preterms’ neurodevelopment, the infants receive a neurologic examination and developmental assessment for improvement. There is an increased interest in prediction of progress from infancy to early childhood and later ages, especially in high-risk cases. 5,6 Several studies provided predictions and correlations from infancy to preschool ages. For Magyary et al, 7 a 24-month standardized measure of infant development proved to be a useful predictor of school-age intellectual functioning. These authors obtained multiple correlations from 0.58 to 0.68, which they regarded as striking, particularly for general intelligence outcomes, as prediction was based on information gathered during the infants’ first 2 years of life. Bowen et al, using the Griffiths General Quotient, found a weak correlation of 0.47 between 1 and 5 years but a stronger correlation of 0.78 with the same test between 3 and 5 years. 8 Kohlhauser et al 9 followed the developmental and neurologic outcome of a group of very low birth weight infants at 1 and 2 years. Using the Griffiths Mental Developmental Scales, the rate of cognitively normal children remained constant (58% at 1 year and 59% at 2 years), indicating that developmental status at 1 year was predictive for the second year. Using the same cohort, he found a weak correlation between 1 and 5 years but a stronger correlation with the same test between 3 and 5 years of ages. Another study of very low birth weight children found that Bayley Mental Development Index scores and weight at 1 year of age were important predictors of motor and intellectual outcome at 6 years. 10 Dezoete et al 2 studied the prediction of cognitive development of very low birth weight infants at 18 months and 4 years by using Bayley and Stanford-Binet scores, and the results indicated that prediction of cognitive development from infancy to preschool age was possible. 2 Although long-term follow-up studies of neurodevelopmental outcome are infrequent because of increased subject dropout, cost, and extended duration required to complete longitudinal assessments, they have been used increasingly as a benchmark to determine efficacy of medical interventions or the consequences of being born early. 11 The Bayley Infant Neurodevelopmental Screener 11 is a screening test designed to identify infants between the ages of 3 and 24 months who are developmentally delayed or have neurodevelopmental impairments. It consists of 6 item sets: 3 to 4 months, 5 to 6 months, 7 to 10 months, 11 to 15 months, 16 to 20 months, and 21 to 24 months, each with 11 to 13 items that are scored in a binary optimality format (optimal/not optimal). It takes approximately 10 to 15 minutes to administer and allows screening of the posture, tone, quality of movement, developmental status, and basic neurologic intactness by assessing 4 conceptual areas that are based on an early developmental, neuropsychological framework. The Bayley Infant Neurodevelopmental Screener risk scores have acceptable concurrent validity when compared with the Bayley Scales of Infant Development II, that is, a 68% to 96% rate of agreement for high risk status, depending on the item set for the mental developmental index, and 78% to 86% agreement for the psychomotor developmental index. 12 Predictive validity has also been established. 13,14 However, prediction of specific later outcomes has not been investigated adequately. Therefore, the purpose of the current investigation is to determine whether identification during infancy of conceptual groupings of items on the Bayley Infant Neurodevelopmental Screener in 45/122 preterm infants will enhance prediction of 7 to 10 years’ cognitive and motor outcome assessed by verbal performance and total scores of Wechsler Intelligence Scale for Children–Revised (WISC-R).
Patients and Methods
Forty-five of 122 patients who were evaluated by Bayley Infant Neurodevelopmental Screener in the original study could be reached and were given the WISC-R. The rest, 77 patients, were not in the postal addresses they had registered.
In this study, we used data from a previously reported follow-up study of preterm infants, 15 in which the study group consisted of 122 preterm infants either born in or referred to the Gazi University Hospital neonatal intensive care unit. Within the scope of the previous study, the patients were divided into 3 groups according to their gestational age: group 1, 26 to 29 weeks; group 2, 30 to 32 weeks; group 3, 33 to 37 weeks.
Groups 1 and 2 both are regarded as high-risk groups. Medical factors such as mean birth weight, gender, birth place and type, number of multiple pregnancies, days of hospitalization and oxygen therapy, use of antenatal steroids, and occurrence of sepsis for each patient were evaluated. A pediatric neurologist made the neurodevelopmental examination and administered the Bayley Infant Neurodevelopmental Screener at each visit of the patients whose corrected ages were used from 3 months to 24 months. Those patients were followed up at our pediatric neurology outpatient clinic under a program to monitor developmental outcome.
Within the scope of this second study, as mentioned above, 45 patients between the ages of 7 and 10 years could be reached. They were assessed by a pediatric neurologist and a psychologist. Parents attended voluntarily and were informed that the information collected and the feedback they provided to staff could be published.
The reevaluated socioeconomic status of the family and the educational statuses of the mothers were given in Table 1. In terms of monthly income and education level, no statistically significant difference was found between the families (P > .05).
Patient Characteristics and Medical Risk Factors.
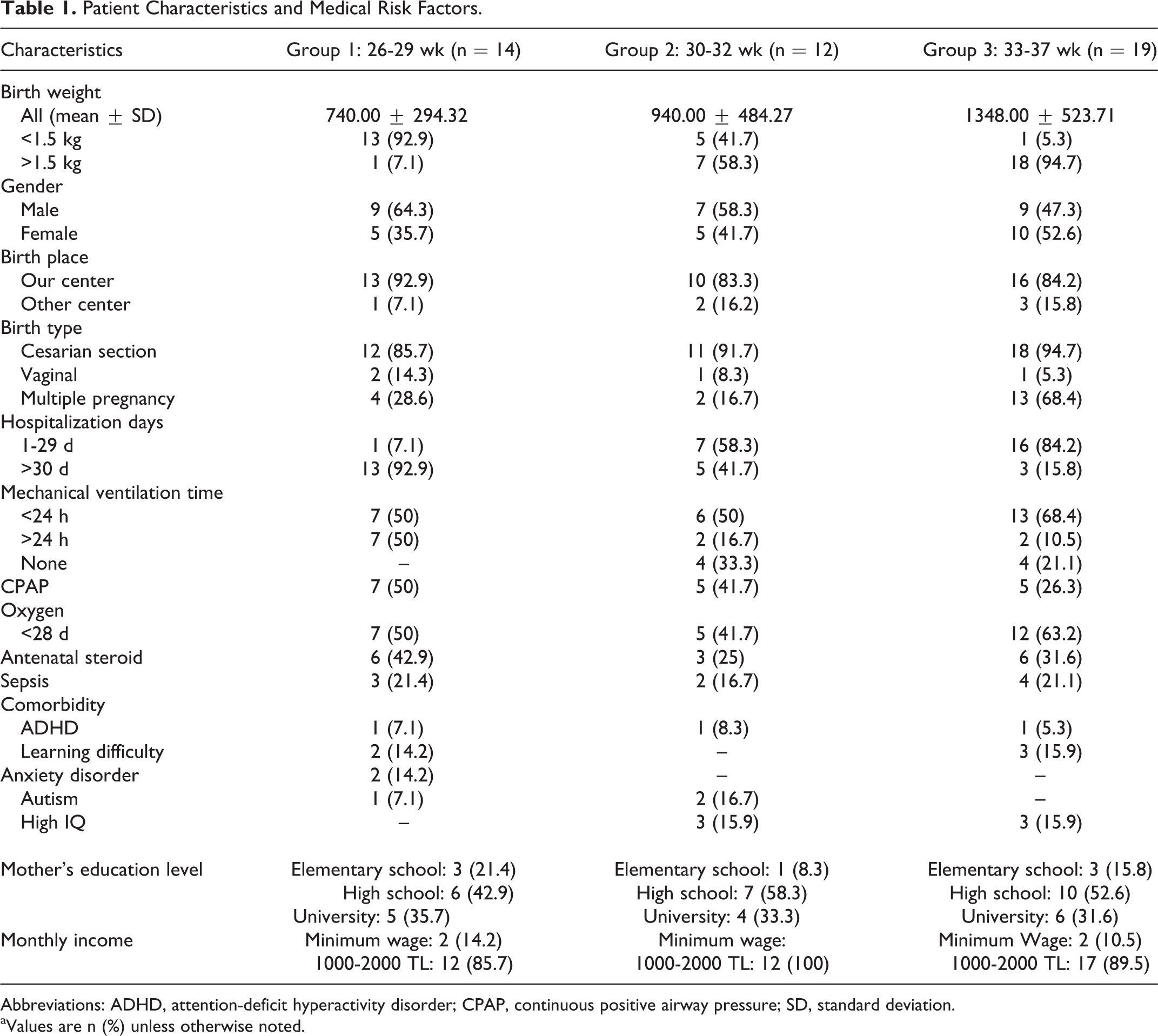
Abbreviations: ADHD, attention-deficit hyperactivity disorder; CPAP, continuous positive airway pressure; SD, standard deviation.
aValues are n (%) unless otherwise noted.
Measures
Demographic information and the Bayley Infant Neurodevelopmental Screener scores of the 45 patients were extracted from the previous study’s records. 15
Bayley Infant Neurodevelopmental Screener Assessment
The Bayley Infant Neurodevelopmental Screener identifies infants between 3 and 24 months who are developmentally delayed or have neurologic impairment by assessing 4 a priori conceptual areas of ability 1 : basic neurologic functions/intactness (posture, muscle tone, movement, asymmetries, abnormal indicators), 2 expressive functions (gross motor, fine motor, oral motor/verbal), 3 receptive functions (visual, auditory, verbal), 4 cognitive processes (object permanence, goal directedness, imitative abilities, problem solving). It consists of 11 to 13 items for different age levels, and each item is scored as optimal or nonoptimal, based on a priori decision rules. The numbers of optimal responses for a given item set are added to provide a summary score, the sum of items failed places the infant in a range of low, moderate, and high risk for developmental delay. Because of the low number of patients in each gestational age group evaluated for the corrected age, patients with low risk scores were pooled in 1 group, and the ones with high- and moderate-risk scores were pooled in the other group for statistical evaluations. At the corrected age of 7 to 10 months, patients at 26 to 29 weeks’ gestational age had significantly lower total means of Bayley Infant Neurodevelopmental Screener scores when compared to those of the other 2 groups at 30 to 32 and 33 to 37 weeks’ gestational age. During this period the scores of the items defining the expressive and cognitive functions of the patients at 26 to 29 weeks’ gestational age were lower than those of the patients at 30 to 32 weeks’ gestational age and 33 to 37 weeks’ gestational age (P < .05). At 16 to 20 months, the mean scores of the items of expressive functions were significantly lower in patients of the 26 to 29 weeks’ gestational age compared to those of the patients of 33 to 37 weeks’ gestational age (P < .05).
WISC-R Assessment
The Total, Verbal, and Performance IQ scores were selected for comparison with the high-moderate and low risk Bayley Infant Neurodevelopmental Screener scores for the ages at which a considerable difference was found between the patients grouped by their gestational ages in the previous study. We used 5 verbal subscales (similarities, information, arithmetic comprehension, and digit span) and 5 performance subscales (picture arrangement, picture completion, block design, object assembly, coding) and then calculated the Verbal, Performance, and Total IQ; children scoring below 90 were regarded as abnormal.
Statistical Analysis
Statistical analysis was performed using the Statistical Program for Social Sciences software (SPSS 13.0, SPSS Inc, Chicago, IL). The numerical values of IQ scores were expressed as means ± standard deviations. The mean and standard deviation of total WISC-R scores of the low-risk and high-medium-risk groups of each gestational age were compared using analysis of variance and post hoc analysis (Bonferroni); P values <.05 were considered to be statistically significant. The positive and negative predictive values and the sensitivity and specificity were calculated for the 7 to 10 and 16 to 20 months Bayley Infant Neurodevelopmental Screener and the Total, Verbal, and Performance IQ scores of the WISC-R.
Results
The study included 45 infants, 14 of whom were between a gestational age of 26 and 29 weeks, 12 between 30 and 32 weeks, and 19 between 33 and 37 weeks. The patient characteristics and medical risk factors are presented in Table 1. Results of assessment of the WISC-R scores of the patients between the ages of 7 and 10 years who had low- and high-medium-risk Bayley Infant Neurodevelopmental Screener scores at ages 7 to 10 and 16 to 20 months are given in Table 2. In terms of the gestational ages, the lowest WISC-R scores were of patients with gestational ages 26 to 29 weeks (Table 2). When the subscales of the WISC-R were evaluated, the patients assessed at the ages of 7 to 10 months and gestational age 26 to 29 weeks with low-risk Bayley Infant Neurodevelopmental Screener scores had higher scores of Verbal IQ subdomains (arithmetic, comprehension, and digit span) than those with high-medium-risk Bayley Infant Neurodevelopmental Screener scores. The same group of patients who were assessed at the ages of 16 to 20 months with low-risk Bayley Infant Neurodevelopmental Screener scores had higher Performance IQ subdomains (information, digit span, block design, and coding) than those with high-medium-risk Bayley Infant Neurodevelopmental Screener scores. Patients in the 30 to 32 and 33 to 37 weeks gestational age groups with low-risk Bayley Infant Neurodevelopmental Screener score results at 7 to 10 months had higher scores in the Verbal IQ subdomain (digit span) than those with high-medium-risk Bayley Infant Neurodevelopmental Screener scores. The same 2 groups having low-risk Bayley Infant Neurodevelopmental Screener scores at the ages of 16 to 20 months had both higher Verbal IQ subdomain scores (digit span) and Performance IQ subdomain scores (block design, coding) than those having high-medium Bayley Infant Neurodevelopmental Screener scores (Table 3). Positive and negative predictive values, sensitivity and specificity of low-risk and high-medium-risk Bayley Infant Neurodevelopmental Screener scores at 7 to 10 and 16 to 20 months, and WISC-R Verbal, Performance, and Total IQ scores at 7 to 10 years of age are shown in Tables 3 and 4. All the patients who had high-moderate-risk scores of the Bayley Infant Neurodevelopmental Screener at all times regardless of their gestational age had lower Performance, Verbal, and Total IQ scores of WISC-R than those who had low-risk scores. High-moderate-risk scores of the Bayley Infant Neurodevelopmental Screener at 7 to 10 and 16 to 20 months of all patients showed good prediction, especially for identifying lower Verbal and Performance IQ scores. For 7 to 10 months, Verbal IQ: positive predictive value = 92.3%, negative predictive value = 44.4%, sensitivity = 70.58%, and specificity = 80%; Performance IQ: positive predictive value = 100%, negative predictive value = 30%, sensitivity = 68.18%, and specificity = 100%. For 16 to 20 months, Verbal IQ: positive predictive value = 90%, negative predictive value = 37.5%, sensitivity = 64.3%, and specificity = 80%; Performance IQ: positive predictive value = 90%, negative predictive value = 12.5%, sensitivity = 56.3%, and specificity = 50%. The socioeconomic status and the environmental factors of all patients and the incidence of major medical risk factors are given in Table 1. There is no significant difference between the groups (P > .5).
WISC-R Scores at 7-10 Years of the Patients Who Had High-Medium-Risk and Low-Risk Bayley Infant Neurodevelopmental Screener Scores at the Ages of 7-10 and 16-20 Months.
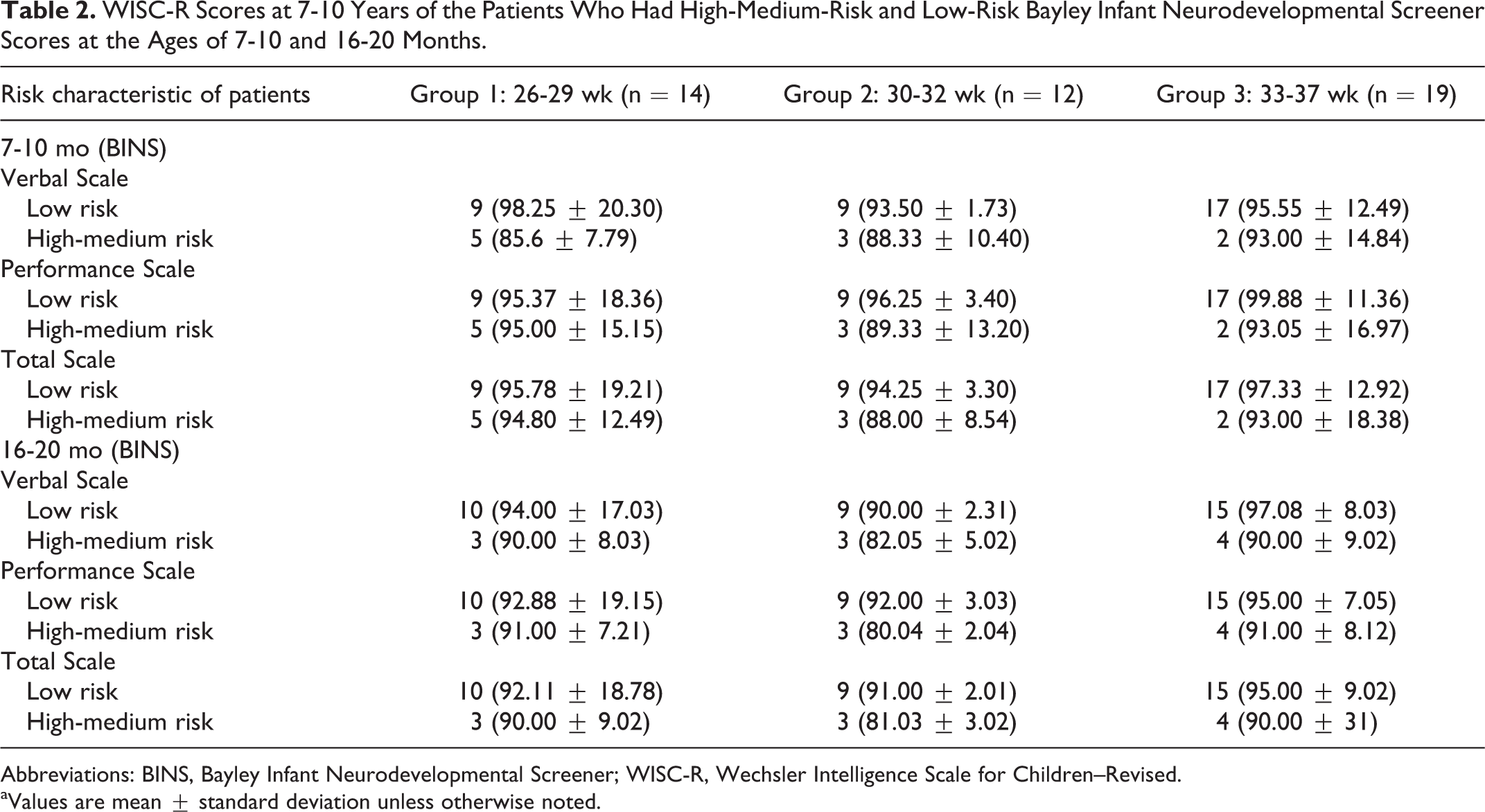
Abbreviations: BINS, Bayley Infant Neurodevelopmental Screener; WISC-R, Wechsler Intelligence Scale for Children–Revised.
aValues are mean ± standard deviation unless otherwise noted.
The ANOVA Results of the WISC-R Scores of Patients With High-Medium-Risk Versus Low-Risk BINS Scores.*
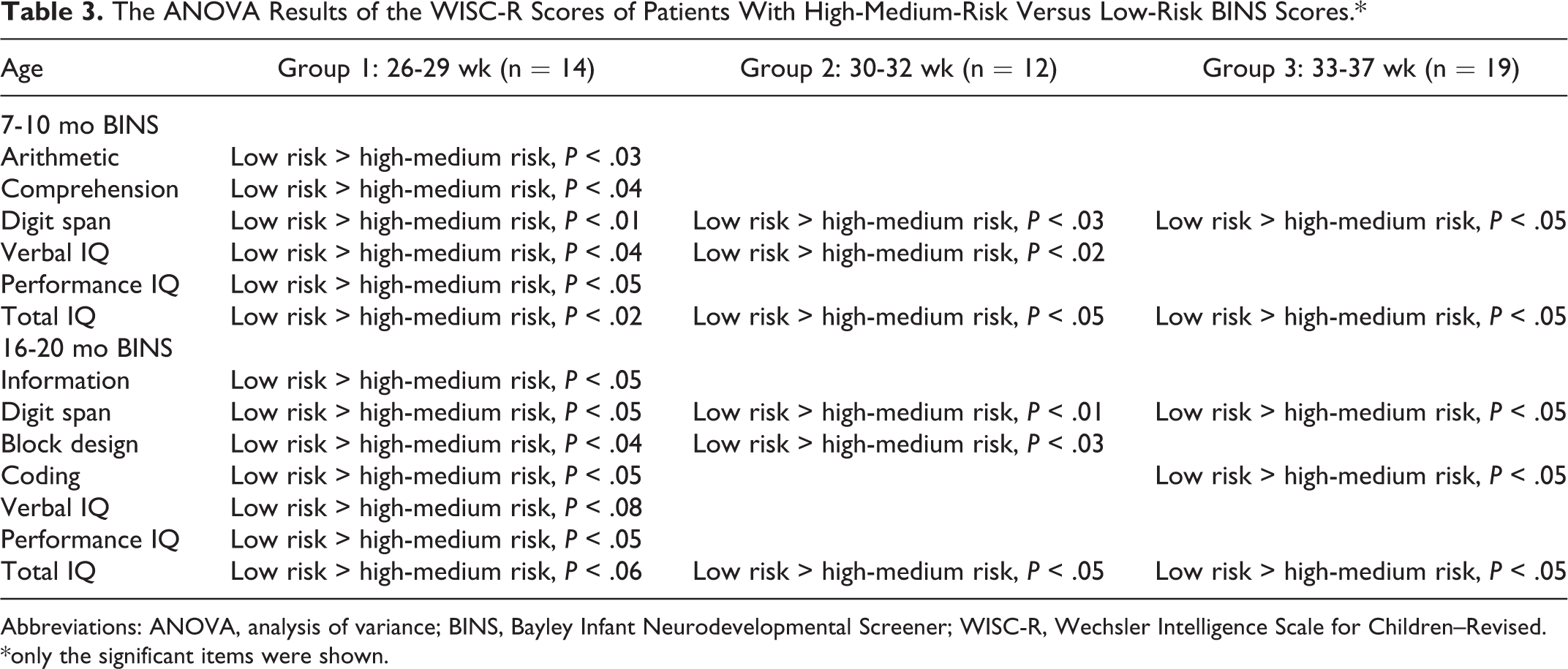
Abbreviations: ANOVA, analysis of variance; BINS, Bayley Infant Neurodevelopmental Screener; WISC-R, Wechsler Intelligence Scale for Children–Revised.
*only the significant items were shown.
Seven to 10 Months Sensitivity, Specificity, and Positive Predictive Value of BINS High-Medium/Low-Risk Status and 7-10 Years WISC-R Scores.
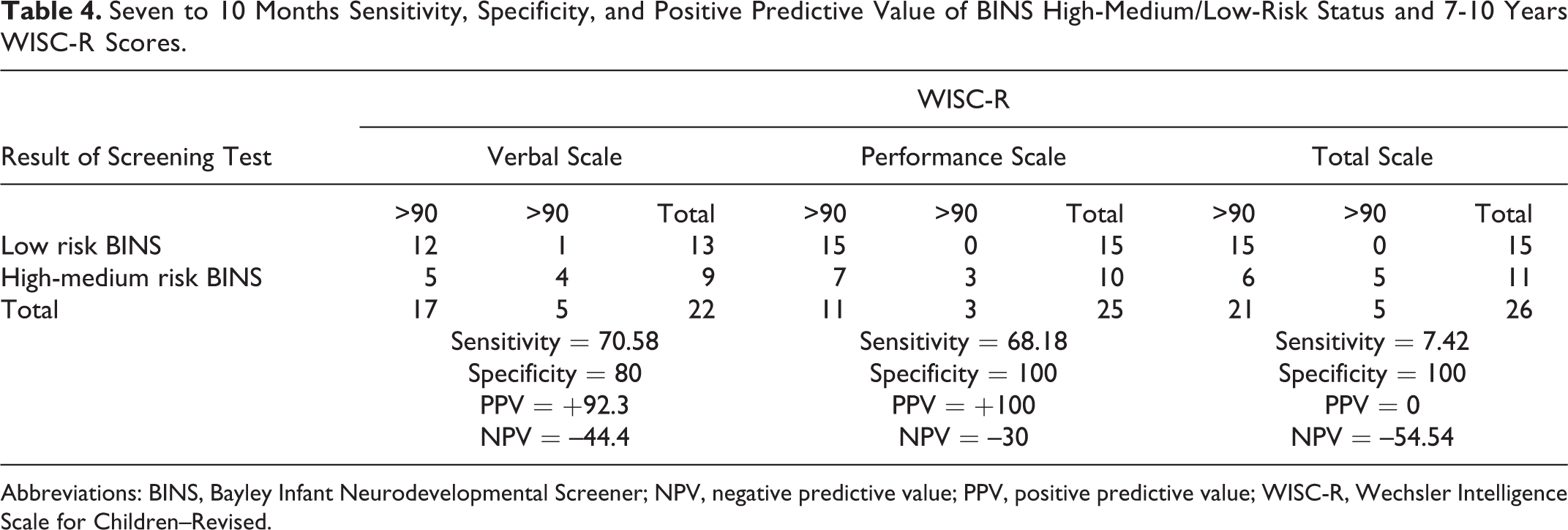
Abbreviations: BINS, Bayley Infant Neurodevelopmental Screener; NPV, negative predictive value; PPV, positive predictive value; WISC-R, Wechsler Intelligence Scale for Children–Revised.
Discussion
There is increased interest in prediction of outcome from infancy to early childhood and older ages of preterm and low birth weight infants, as the survival rates of this population as young as 23 weeks’ gestational age have increased, resulting in more of these infants surviving to school life. This fact raised concerns that there might be a higher incidence of later neurodevelopmental disability in this population with respect to their term normal birthweight peers. Preterm children have specific areas of deficit; the most commonly expected outcome after preterm birth is cerebral palsy of variable severity occurring in 8% to 10% of very low birth weight infants. 16 Severe handicaps may have a suppressor effect on all aspects of development and thus validate a global measure of delay; however, children with later high prevalence but low severity dysfunctions such as attention-deficit hyperactivity (ADHD) disorders, learning disabilities, low IQ, behavioral problems, and neuropsychological deficits (executive function, visual motor integration) may display much more variability in their initial assessment results as well as in later outcome. The neurodevelopmental outcome is increasingly used as a benchmark to follow the efficacy of medical interventions or the consequences of being born early. Unfortunately, long-term follow-up studies are not extensively done, because of increased subject dropout and cost along with the long-standing bias that data merging from those studies are not as precise as biochemical or radiographic measurements. However, long-term follow-up is absolutely critical in order to identify possible negative effects of prematurity, some medical intervention, or a standard of care that might have an effect on the baby that are not obvious during the first years of life. The best example to show the need of extended follow-up for identification of a later problem was clearly demonstrated in the use of postnatal steroids for the treatment of chronic lung disease of the preterm baby, where there was an immediate positive effect, but negative consequences that became obvious later. 17 Although major disabilities found nearly in 15% to 20% of those born with very low birth weight and 20% to 25% in those born with extremely low birth weight are mostly identified early in infancy, high-prevalence/low-severity dysfunctions found in 50% to 70% of very preterms become more overt as the child grows older, further emphasizing the need for long-term follow-up. 1,3,4 At present, there are no good predictors of those more subtle problems that can be identified during childhood. What complicates the matter further is that it is also very difficult to say whether developmental problems found during infancy are transient because of the negative effects of prematurity and expectations that the baby may catch up, or if they reflect the emergence of a more permanent deficit. 18 In this respect, very well organized long-term follow-up programs should be established after the baby is discharged from the neonatal intensive care unit. For monitoring the neurodevelopmental profile of children until 2 years, there are many developmental screening tests and assessments 19,20 ; however, prediction or continuity from infant screening tests to later outcome has not been an area intensively studied. Hack et al in their study had indicated that attainment of a subnormal Mental Development Index on the Bayley Scales of Infant Development II at 20 months’ gestational age was not predictive of subnormal cognitive function at school age, although it was better for children who have neurosensory impairments. However, it might be a marker of future risk of problems in academic, motor, and social functioning and for increased need for special education. 21 Leonard et al 14 had investigated the relationship of Bayley Infant Neurodevelopmental Screener scores at 6 months of age to later development at 1 year of age as measured by the Bayley Scales of Infant Development II and had proposed that Bayley Infant Neurodevelopmental Screener at 6 months of age might reflect subtle aspects of behavioral organization and attention span that could be identified at 1 year of age. Aylward et al 22 administered Bayley Infant Neurodevelopmental Screener at 6, 12, and 24 months and Bayley-II or McCarthy scales at 36 months and showed that stability and continuity in time do exist in high-risk babies with respect to specific subdomains of function. He showed that the functional subdomains begin to extract at 6 months but separate out more clearly by 12 months; around 24 months, the distinction between verbal expressive and cognitive/verbal receptive factors becomes quite obvious. Thus, pursuing those functional subdomains throughout infancy, especially verbal, cognitive, and motor abilities, could yield more precise prediction than tracking global measures, and later outcomes are defined better. In our previous study we had used Bayley Infant Neurodevelopmental Screener to assess the neurodevelopmental outcome during the first 2 years of life. At 7 to 10 months, the scores of the items defining the expressive and cognitive functions of the patients at 26 to 29 weeks’ gestational age were found to be lower than those of the patients at 30 to 32 and 33 to 37 weeks’ gestational age. 15 The 7 to 10 months item set of Bayley Infant Neurodevelopmental Screener is mainly directed to investigate the intentionality or purposeful activity with expressive functions—gross motor items being predominant. Two items, “lifts the inverted cup [cognitive process, involving exploration and goal directedness]” and “responds to spoken request [Receptive Functions–Verbal]” are used to differentiate those with medical complications. 12 At 7 to 10 months of age, nearly 95% of our patients in the 26 to 29 weeks’ gestational age group had failed these 2 items. Likewise, at 16 to 20 months, the mean scores of the items of expressive functions were also found to be significantly lower in patients of the 26 to 29 weeks’ gestational age compared to those of the patients of 33 to 37 weeks’ gestational age. The 16- to 20-month item set, primarily consisting of items of the expressive functions and cognitive process is also helpful to differentiate infants who had severe medical complications. Most of our patients of the 26 to 29 weeks’ gestational age group at the age of 16 to 20 months had also failed those items, indicating the persistent delay of the expressive and cognitive functions. 12 We also wanted to see whether the items of expressive/cognitive functions in which the 2 age groups of patients failed would enhance the prediction of their 7 to 10 years’ cognitive outcome. All patients with 26 to 29 weeks of gestational age having high-medium-risk Bayley Infant Neurodevelopmental Screener scores at 7 to 10 months had worse Verbal IQ subscores (arithmetic, comprehension, and digit span) of the WISC-R than those in the low-risk Bayley Infant Neurodevelopmental Screener group. The same patient group with high-medium-risk Bayley Infant Neurodevelopmental Screener scores at 16 to 20 months had both worse Verbal (information, digit span) and Performance (coding, block design) IQ subscores in the WISC-R than those in the low-risk Bayley Infant Neurodevelopmental Screener group. This high concordance between the Bayley Infant Neurodevelopmental Screener and WISC-R scores defining expressive and cognitive functions suggests that stability and continuity over time exists in high-risk infants with respect to specific subdomains of function, thus enabling the prediction of later cognitive repertoire. An array of cognitive deficits have been reported in those patients who score lower in the Verbal IQ subscale of the WISC-R, including visuomotor problems, attention difficulties, impaired memory, delayed language skills, and executive dysfunction. Consistent with this profile of cognitive impairment, high rates of learning disabilities are cited. 23 In our patient population of 26 to 29 weeks gestational age group, 1 patient had attention-deficit hyperactivity disorder (ADHD), 2 had learning disability, 2 had anxiety disorder, and 1 had autism. In the 30 to 32 weeks’ gestational age group, 1 patient had ADHD and 2 had autism. In the 33 to 37 weeks’ gestational age group, 1 patient had ADHD and 2 had learning disability. All those patients had difficulty in short-term and working memory functions. Thus, our study indicates that early measures of cognitive processes seem to correlate with later various product measures of intelligence. The number of patients we have followed is only one-third of the original study population. That could be taken as a weak point. Our results, nevertheless, indicate that the Bayley Infant Neurodevelopmental Screener is highly useful in identifying infants who are currently at risk and also those whose later functioning may be at risk. If the cost and time factors are taken into consideration, it seems logical to use it for monitoring and to predict later outcome, provided that subdomain scores in addition to total scores are used. Infants at risk for cognitive and expressive deficits in later childhood can thus be identified by better understanding the subdomains that contribute to these deficits. Without doubt, prediction of later outcome will most likely improve with the combined use of brain imaging technique, functional activity of the brain, magnetic resonance spectroscopy, biochemical markers, and serial neurodevelopmental assessments. Identification and understanding of these functional processes would inevitably lead to implementation of early interventions to the target population, with specially designed programs that are particularly useful.
Footnotes
Author Contributions
All the authors, except ASS, made clinical evaluation and follow ups of the patients. ASS made the literature search, all psychological tests, assessments, and statistical analysis. The results and discussion are concluded by all the authors in collaboration. KG and ASS reviewed and developed the study in article format.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.