
Abstract
Background:
Children are most vulnerable to tubercular meningitis. Neuroimaging is an important initial investigation in tubercular meningitis.
Objective:
This study was done to describe the clinical profile, neuroimaging changes, and clinical outcome in children with tubercular meningitis.
Methodology:
This was an observational cohort study on children with tubercular meningitis, between January 2012 and June 2018. Tubercular meningitis was diagnosed on the basis of clinical criteria, cerebrospinal fluid analysis, neuroimaging, and response to antitubercular drug treatment. Preferably magnetic resonance imaging (MRI) with contrast was done.
Result:
Out of 79 pediatric patients, 17 patients were lost during follow-up; thus, a total of 62 patients were studied. Mean age at presentation was 7.040 (±3.99 SD) year, 51.6% children were male. Rural children were more affected. Twenty eight (45.2 patients had contact with a person with tuberculosis. Only 3 (4.8%) patients presented within 10 days of duration of illness. Most of the cases (67.7%) were in stage 2 at the time of diagnosis. The most common clinical feature was fever, seizure, and signs of meningeal irritation (all present in 12.9%). In neuroimaging most common findings were tuberculoma (50%), hydrocephalus (54.8%), and basal meningeal enhancement (33.8%). Regarding outcome, 6 (9.67%) patients expired and 47 (75%) patients had sequelae. The most common complications were hydrocephalus (30.64%) and intellectual disability (12.9 ). Hydrocephalus was the most common neuroimaging finding among the patients who expired (33%).
Conclusion:
Hydrocephalus is the most common neuroimaging finding. Normal neuroimaging is associated with good outcome whereas all the patients who died had abnormal neuroimaging.
Tuberculosis (TB) is the second most common cause of infectious disease resulting in mortality worldwide, after HIV/AIDS. 1 Approximately 5% to 10% of all patients with tuberculosis have central nervous system involvement. 2 Tubercular meningitis is the most severe and life-threatening form of tuberculosis in children. 3,4 Its peak incidence is in young children less than 4-5 years old although it may occur at any age. 5 Children are most vulnerable and are frequently affected by tubercular meningitis because of their poor immune response to contain the Mycobacterium tuberculosis bacteria within the lungs. 6
Natural history and clinical manifestations of tuberculosis are different in children and in adults, with a higher incidence of disseminated forms and a higher risk to progression to severe forms being reported to occur in children. 7 Despite advances in its management and control around the world, eradication of this disease continues to be elusive, and it still poses a high risk of death, which is estimated to vary from 15% to 32%. 5,8,9 Neurologic sequelae are noted in more than half of the affected patients. 5,6
Neuroimaging is an important initial investigation in tubercular meningitis. This study was done to describe the clinical and neuroimaging changes of tubercular meningitis patients and also to determine the role of neuroimaging in the diagnosis of tubercular meningitis. It also focused the association between radiologic changes and clinical outcome in a developing country like Bangladesh where the tuberculosis burden is high.
Methodology
This was an observational cohort study on patients with pediatric tubercular meningitis where study subjects were prospectively followed up. It was conducted between January 2012 and June 2018. All patients who attended a tertiary center with tubercular meningitis were recruited. Tubercular meningitis was diagnosed on clinical criteria, cerebrospinal fluid analysis (pleocytosis, high protein, low glucose), neuroimaging (tuberculoma, basilar enhancement, calcification, hydrocephalus, etc) along with other relevant investigations. In the neuroimaging study, magnetic resonance imaging (MRI) was preferred when affordable. Magnetic resonance angiography, magnetic resonance venography, and magnetic resonance spectroscopy was done in selected cases. Evaluation was done by an expert neuroradiologist.
Severity of meningitis was graded at the time of admission according to British Medical Research Council criteria: stage 1 for Glasgow Coma Scale score 15 with meningeal signs only, stage 2 for Glasgow Coma Scale score 11-14 or 15 with focal neurologic signs, and stage 3 for Glasgow Coma Scale score ≤10. 10 The advanced stages were defined as stages 2 and 3.
All children were treated with antitubercular drug, mostly isoniazid (INH), rifampicin, pyrazinamide, and ethambutol/streptomycin. The average duration of treatment was 12 months. In some patients, prolonged treatment was given for up to 18 to 24 months. In all children, steroid was given mostly in the form prednisolone (oral) or dexamethasone (intravenous) for 6 to 8 weeks. Informed consent was taken from the parents of all the patients. Approval of the Ethical Committee of the institution (Internal Review Board) was taken to conduct the study.
Data on demographic characteristics such as age, gender, period of evolution of the disease, symptoms and signs at the time of admission, complete blood count, cerebrospinal fluid findings, and Mantoux test were recorded. Treatment and clinical course was recorded, including the drug side effects as well as neurosurgical intervention.
The patients were followed for about 2 weeks to 4 years. In every follow-up, clinical features, routine investigations, and computed tomography (CT)/MRI of the brain were done if needed.
Statistical Analysis
The chi-squared test was used for statistical analysis, and a value of <.05 was considered statistically significant.
Results
Demographic characteristics of tubercular meningitis patients: Over a 6-year period, 62 pediatric patients with tubercular meningitis were followed. The mean patient age at presentation was 7.040 years (standard deviation 3.99). Thirty-two children were male (51.6%) and 30 (48.4%) female. Rural children were more affected than the urban. Twenty-eight (45.2%) children had contact with a person with open case of tuberculosis (Table 1).
Baseline Characteristics of the Studied Children (N = 62).
Clinical Features and Staging
About 46.8% had more than 30 days of clinical presentation before they were attended to in this tertiary center. However, the range of duration of illness was 5 to 71 days. Only 3 children (4.8%) presented in less than 10 days of duration of illness. Most of the children (67.7%) were in stage 2 at the time of diagnosis. Only 8.1% of the patients were diagnosed in stage 1. Fever was the most common feature at admission (96%). Other features were headache (82%), vomiting (49%), and seizure (44%) (Table 2).
Clinical Features of the Studied Children (N = 62).
Note: The clinical findings are rounded off.
Laboratory Findings
More than half of the studied children (64.5%) had normal hemoglobin percentage, and the majority had normal white blood cell count (82.3%). Among the patients who had increased white blood cell count, most showed lymphocytosis (33.9%). The erythrocyte sedimentation rate was increased in 55.6% patients. Cerebrospinal fluid test was done in all children. In 80.6% children, cerebrospinal fluid had increased leukocyte count. Glucose levels were normal in the cerebrospinal fluid at presentation in 67.7% patients. The cerebrospinal fluid protein levels were normal in 9.7% patients. Most of the patients had 100 to 300 mg/dL of protein (41.9%), whereas 3.2% children had very high levels (>500 mg/dL) of protein in the cerebrospinal fluid (Table 3).
Laboratory Findings of the Studied Children (N = 62).
Abbreviations: CSF, cerebrospinal fluid; ESR, erythrocyte sedimentation rate; WBC, white blood cell.
a Normal = 12.0-15.5 g/dL, reduced = <12 g/dL
b White blood cell: normal = 4000-10 000/mm3, abnormal = >10 000/mm3.
c ESR: normal = 0-40, high = >40 mm in the first hour.
d WBC count in CSF: normal = 0-5, increased = >5/HPF.
Neuroimaging Findings of Studied Children
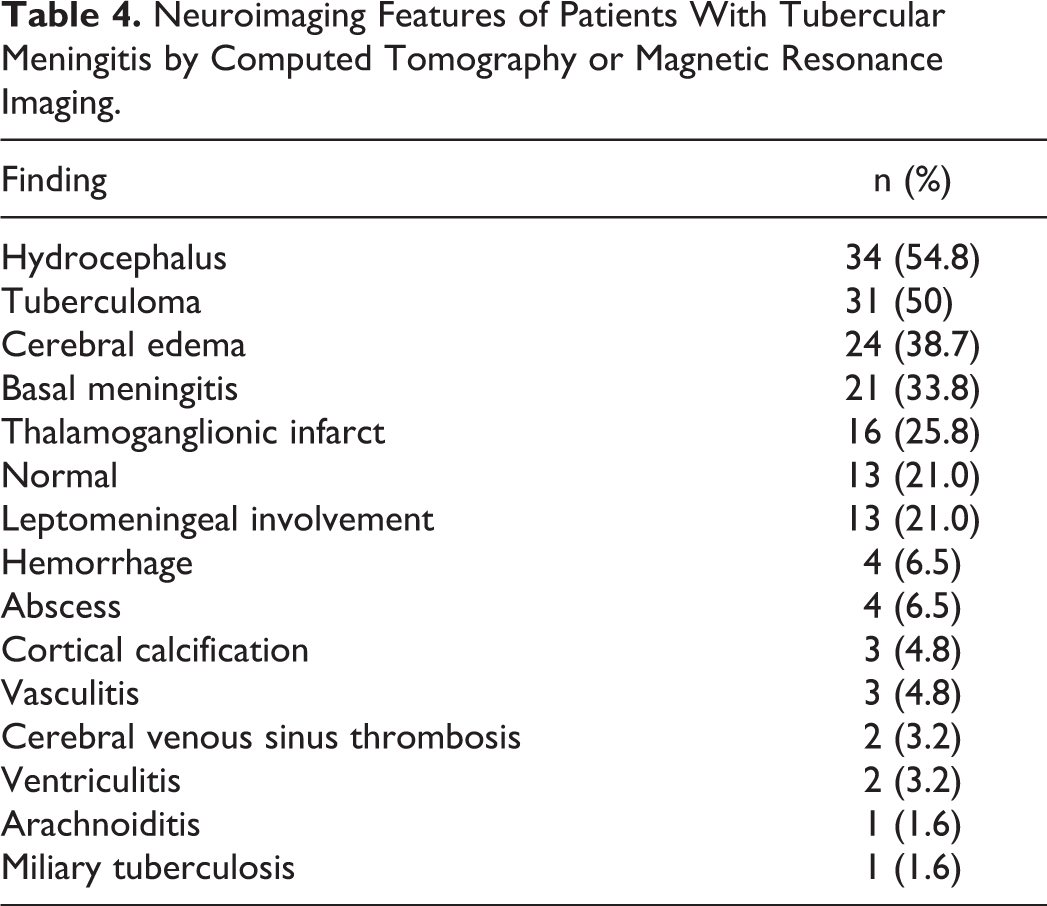
The most common finding was hydrocephalus (Figure 1C) (54.8%). Other findings were tuberculoma (Figure 1E), cerebral edema, basal meningitis (Figure 1D), leptomeningeal enhancement (Figure 1A), cerebral infarction, hemorrhage, calcification, cerebral venous sinus thrombosis, abscess (Figure 1B), ventriculitis, arachnoiditis, and vasculitis (Table 4, Figure 1).
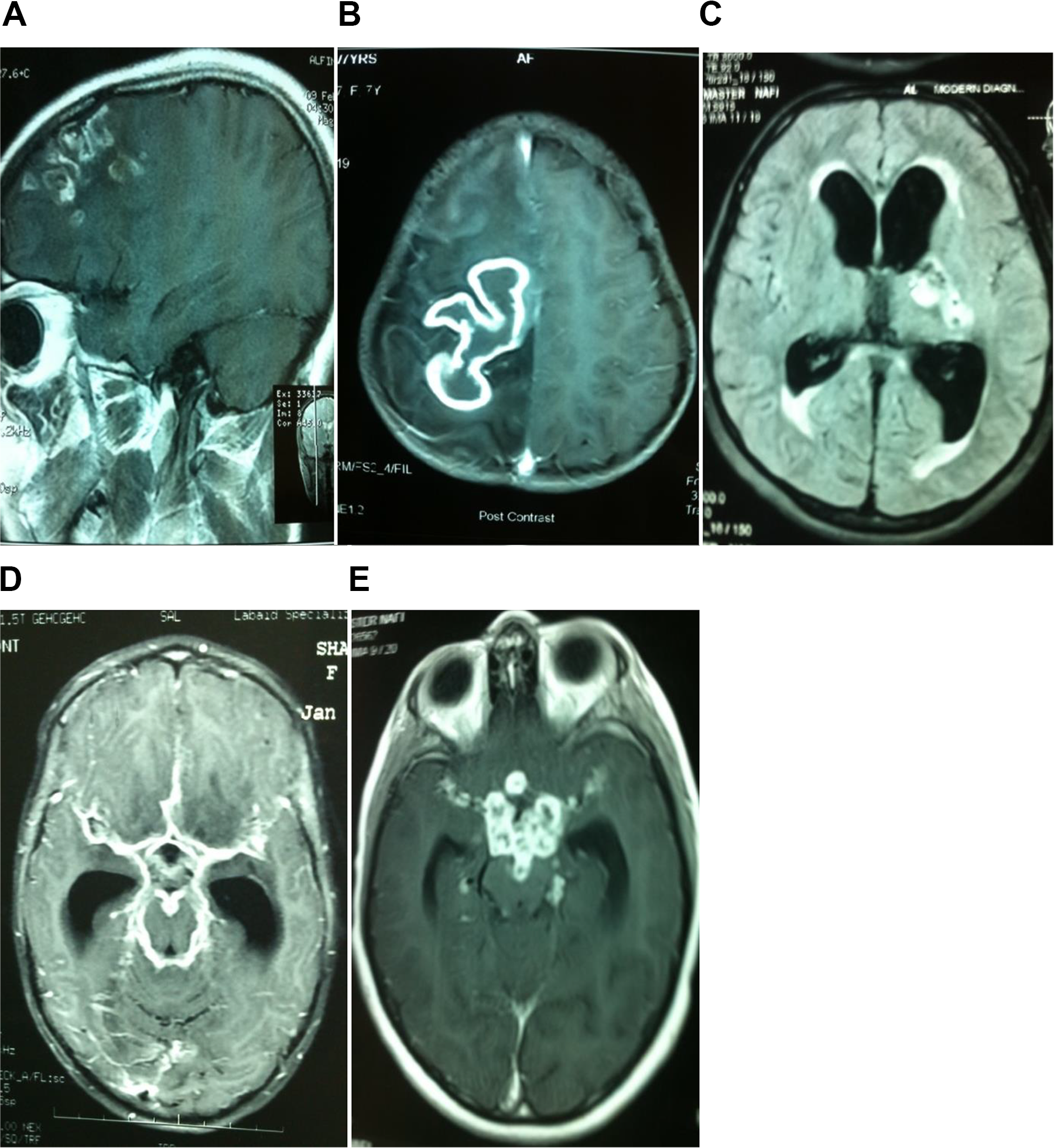
(A) Magnetic resonance imaging (MRI) of brain with contrast (sagittal view) showing gyriform enhancement of frontal lobe with multiple tuberculomas. (B) MRI of brain with contrast showing irregular oval ring-enhancing lesions with perilesional edema in the frontoparietal region suggestive of tubercular brain abscess. (C). MRI of brain with contrast showing enlargement of the lateral ventricle with pressure effect (hydrocephalus) along with tuberculomas in the left capsuloganglionic region. (D) MRI of brain with contrast showing basilar enhancement along with enlargement of the lateral ventricle (hydrocephalus). (E). MRI of brain with contrast showing multiple ring-enhancing lesions.
Neuroimaging Features of Patients With Tubercular Meningitis by Computed Tomography or Magnetic Resonance Imaging.
Neurologic Outcome of Studied Children
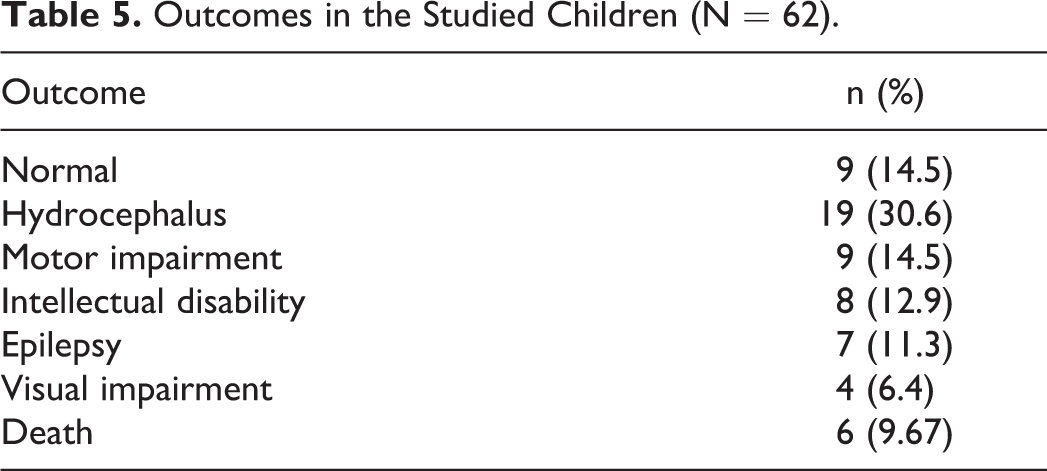
In this period, only 9 (14.5%) children had no sequelae; however, 6 (9.67%) children died within this period. Most of the patients (47) developed sequelae. Most cases developed hydrocephalus during follow-up. Other complications were motor impairment in the form of paresis and involuntary movement. Visual impairment, intellectual disability, and epilepsy were also noted (Table 5).
Outcomes in the Studied Children (N = 62).
Association of Neuroimaging Finding and Outcome of Studied Children
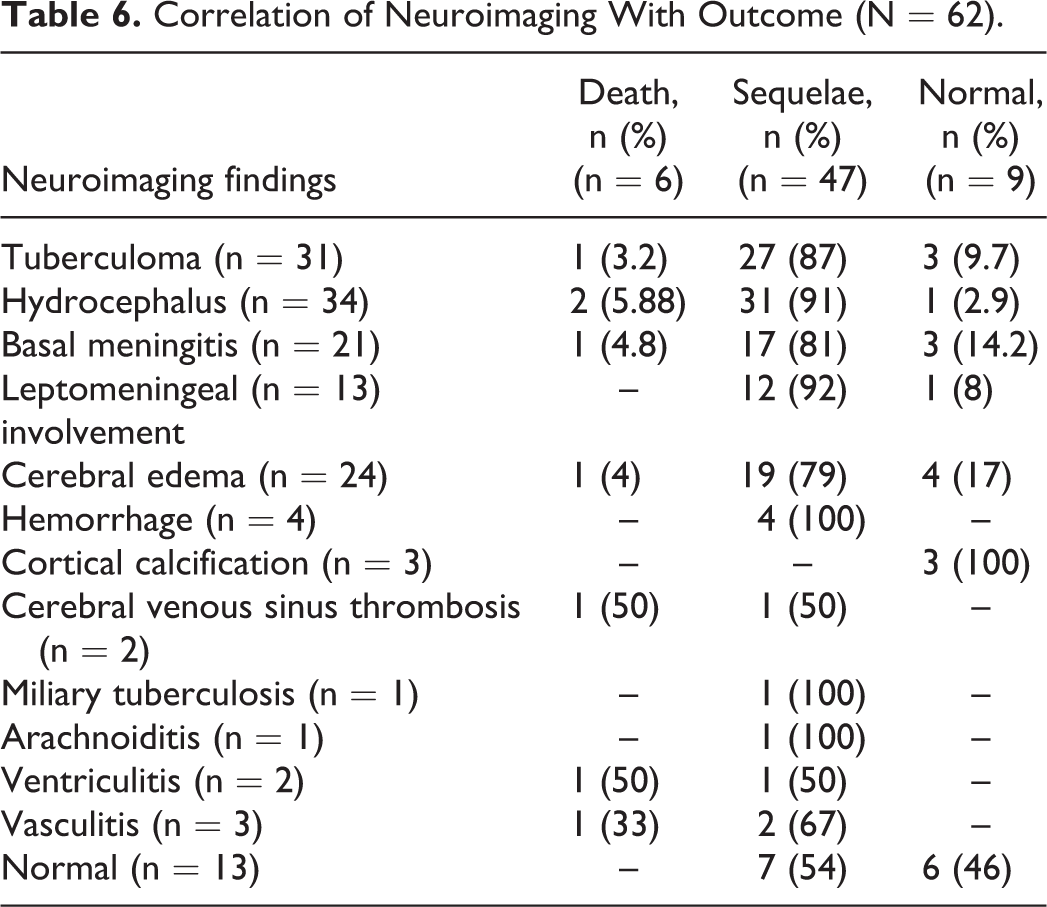
Of the 6 children who died, the neuroimaging features were tuberculoma, hydrocephalus, basal meningitis, cerebral edema, and cerebral venous sinus thrombosis. Patients who had sequelae had hydrocephalus (49%), tuberculoma (43%), cerebral edema (30%), and basal meningitis (27%) (Table 6, Figure 2).
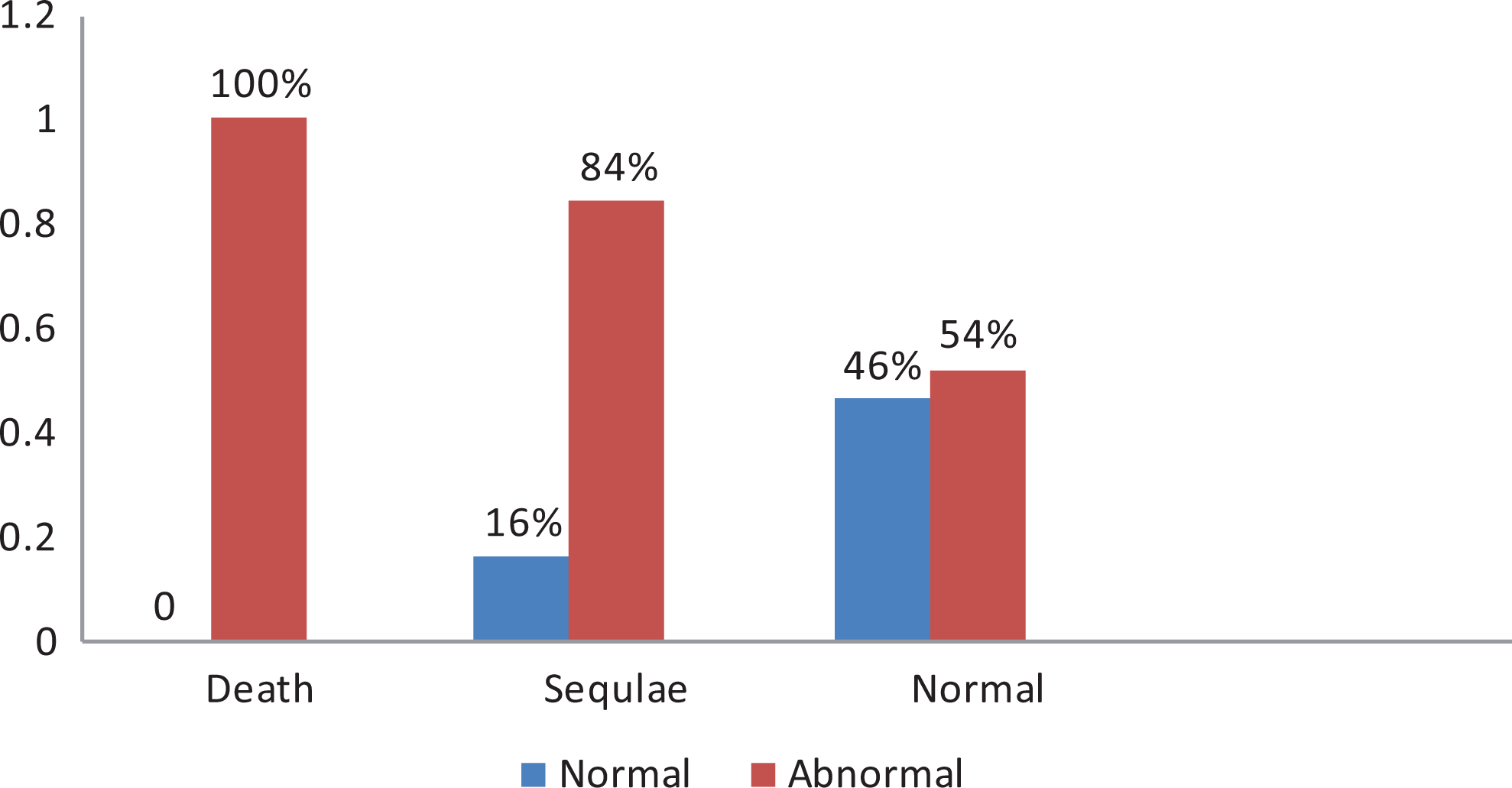
Relationship of neuroimaging with outcome of children with tubercular meningitis (N-62).
Correlation of Neuroimaging With Outcome (N = 62).
Discussion
Tubercular meningitis is the most severe form of extrapulmonary disease highly predominant in children. 10,11 In this study, 62 children with tubercular meningitis was included, out of which 51.6% were male. This is similar to the study by Miftode et al, where male children were more affected (61%). 12 Rural people were more affected with tubercular meningitis in this study group. It is to be noted that 46.8% had more than 30 days of clinical presentation before they were attended to in this tertiary center. The vast majority of these patients were admitted in a critical condition (stage 2, 67.7%), whereas only 8.1% patients presented in stage 1. This finding matches with the previous reports of other groups. 12,13 The late presentation was most probably due to the limited specialized services and delayed referral to the tertiary centers in developing countries. Moreover, the majority of the patients were from a rural background, where there is limited health care facility and travel times to the service providers are longer.
Fever, headache, vomiting, seizure, signs of meningeal irritation were the major clinical features at the time of admission which is similar to the previous studies in the developing country. 14 Contact history of TB was positive in 45.2% cases. This figure has been reported between 33% and 69% in various studies. 13,15 This emphasizes the importance of eliciting contact history and family screening for TB in suspected cases of tubercular meningitis.
Anemia was found in 35.5% of the children. This could be an indicator of the long duration of clinical illness. In the cerebrospinal fluid, 91.3% showed elevated protein, out of which 41.9% had protein levels of 100 to 300 mg/dL, which is similar to previous studies where most patients (88.9%) had 40 to 400 mg/dL of protein. 14
Most of the patients had some form of abnormalities in the neuroimaging, the most common being hydrocephalus (54.8%), tuberculoma, and cerebral edema. Meningeal enhancement was most commonly observed over the basal cisterns and cerebral cortex. Infarction was most common in the basal ganglion followed by the cortex. MRI contrast picked up abnormalities relatively well. Thus, previous studies had indicated MRI as a superior diagnostic imaging modality. 16 -18
The most common neuroimaging finding in this study was hydrocephalus. More than half (54.8%) had hydrocephalus out of which 70% had communicating hydrocephalus. The proportion with hydrocephalus was within the range reported by other authors (58%-71%). 19 -21 According to Bonefe et al, hydrocephalus may be the first clinical manifestation of tubercular meningitis and it may precede the obliteration of basilar cisterns by several weeks. 22 Communicating hydrocephalus, which is considered the most common complication of tuberculous meningitis, is usually caused by the obstruction of cerebrospinal fluid flow in the basal cisterns. 23 -25 In some cases, the hydrocephalus may be noncommunicating, resulting from obstruction due to tuberculoma or rarely tuberculous abscess.
The second common neuroimaging finding was tuberculoma. Tuberculoma is the most common parenchymal lesion in CNS tuberculosis, which could be found in any portion of the intracranial space. The lesion may be solitary or multiple and may be seen with or without meningitis. Histologically, the mature tuberculoma is composed of a necrotic caseous center surrounded by a capsule that contains fibroblasts, epithelioid cells, Langhans giant cells, and lymphocytes. 26 In this study, tuberculoma were seen in 50% patients. Multiple tuberculomas were present in 73% of the patients, and supracortical sites were the most common (66%). This matches with previous studies, where about half of the patients had tuberculomas, mostly multiple. 19,27,28 Here, tuberculomas either showed a hypointense core with rim enhancement or were nodular, with diffuse enhancement. Four (6.45%) patients had cerebral abscess. In follow-up CT or MR studies, resolution of tuberculoma is an indicator of treatment response. We found paradoxical enlargement of a preexisting tuberculoma in 1 patient receiving adequate treatment. However, healed tuberculomas were found in 3 cases as calcified foci on nonenhanced CT.
Leptomeningeal enhancement was seen in 20.9% children, and basal meningeal involvement was present in 33.8% cases. Common locations were interpedicular fossa, prepontine cistern, sylvian fissure, and quadrigeminal cistern. Infarction was detected in 25.8% of the cases on admission, which matches with related studies where infarct ranges from 20% to 41%. 29,30 The most common site of infarct in this study was the thalamoganglionic region (74%). This is may be due to involvement of branches of the middle cerebral artery due to inflammation at the basal cisterns where the middle cerebral arteries pass through. 31
In this study, one case of miliary tuberculosis was found in a patient with a known case of contact and pulmonary involvement. The lesions were located mostly at the corticomedullary junction. In MRI the lesions were small, 2-3 mm in diameter, hypointense in T2-weighted MRI. Meanwhile, cerebral venous sinus thrombosis was found in 2 cases, both of whom presented with severe headache, vomiting, and signs of meningeal irritation.
In this study, the mortality rate of the children was 9.67%. This coincides with similar study done in India where the mortality rate was 10%. 32 This high mortality rate may be explained by delayed presentation to the center and also advanced stage of the disease (stage 2 and 3). Also, both the studies were done in tertiary care centers, where more complicated patients are sent. Although 14.5% completely recovered without any sequelae. About three-fourths of the children developed disability in this study, which is higher than that found by Mohan et al (57%). The most common sequelae the patients developed during the course of the treatment and follow-up were hydrocephalus (30.64%), motor impairment (14.5%), intellectual disability (12.9%), epilepsy (11.3%), and visual impairment (6.4%). Among the patients who died, none had normal neuroimaging findings; rather, most had 2 or more neuroimaging abnormalities, mostly hydrocephalus, tubercle, cerebral venous sinus thrombosis, cerebral edema, etc. This was consistent with other studies where poor outcome was associated with hydrocephalus, tubercle, and cerebral infarct. 33
Limitations
This study had a small cohort of 62. A larger study is needed for drawing an inference. Moreover, it has been carried out in a setup of tertiary care center, which does not reflect the scenario of the whole country. Long-term follow-up is very important for prediction of outcome, but here all the patients were not followed up for a long period.
Conclusion
Fever, headache, and signs of meningeal irritation were the most common combination of clinical features in this study. Most of the children presented to this center after 30 days of illness. Hydrocephalus is the most common neuroimaging finding. Normal neuroimaging is associated with good outcome while all the patients who died had abnormal neuroimaging. Thus, timely neuroimaging seemed to be a powerful tool for early diagnosis.
Footnotes
Author Contributions
KF substantially contributed to conception and design, script writing. MR critically revised the manuscript for important intellectual content. SA final approved the manuscript. NA contributed to acquisition and analysis of data. BCP contributed to conception of research. SB contributed in script writing and FB in data interpretation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study received IRB approval with IRB reference no 2254.