
Abstract
Juvenile neuronal ceroid lipofuscinosis (JNCL; CLN3 disease) is a rare autosomal recessive neurodegenerative lysosomal storage disorder characterized by childhood-onset progressive visual loss, epilepsy, and cognitive decline. Although behavioral and emotional symptoms are frequently reported, manic episodes remain rarely characterized within a structured diagnostic framework. We present a 16-year-old girl with progressive visual impairment and epilepsy who developed a manic episode with psychotic features meeting Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, including decreased need for sleep, increased goal-directed activity, hypersexuality, pressured speech, and hallucinations. Genetic testing using whole exome sequencing identified a homozygous likely pathogenic variant in CLN3 (c.898C>T), which was also identified in her affected sibling, further supporting the diagnosis of JNCL. The patient showed significant clinical improvement with antipsychotic treatment and multidisciplinary follow-up. This report delineates the neuropsychiatric spectrum associated with CLN3 disease and supports the need for systematic mood symptom monitoring in affected adolescents. These findings should be interpreted as hypothesis-generating, and further studies are needed to clarify the underlying mechanisms.
Neuronal ceroid lipofuscinoses (NCLs) are a group of lysosomal storage disorders and an important cause of pediatric neurodegeneration. 1 In the late 1960s, NCL disease was classified into 4 groups according to age of onset: infantile, late-infantile, juvenile, and adult. The NCLs comprise a group of 13 genetically defined subtypes. 2 With the exception of CLN4, which is inherited in an autosomal dominant manner, the remaining subtypes follow an autosomal recessive inheritance pattern. 1 Each subtype is caused by mutations in different genes encoding proteins associated with the endo-lysosomal system.3,4 NCLs are characteristically marked by intracellular accumulation of lipopigments, resulting in neuronal degeneration and retinal atrophy. 5
Ceroid-lipofuscinosis, neuronal 3 (CLN3), is also known as Batten disease or juvenile NCL. 6 The CLN3 protein has been implicated in a variety of metabolic and inflammatory processes, including the regulation of intracellular pH, arginine transport, cell motility, membrane trafficking, and apoptosis. 7 CLN3 disease typically follows a more protracted clinical course compared with other NCL subtypes. 8 Initial symptoms typically emerge between the ages of 4 and 10 years, most commonly presenting as rapidly progressive vision loss, followed by behavioral disturbances, cognitive decline, and epileptic seizures. Recent large-scale natural history analyses further indicate that these neurobehavioral and cognitive symptoms typically emerge at a mean age of approximately 8-9 years, shortly after the onset of visual impairment. 9
Consistent with this clinical progression, neuropsychiatric manifestations are increasingly recognized as a core component of the disease spectrum. 9 Anxiety and cognitive impairment are among the most commonly reported symptoms, whereas depression, aggression, speech and language impairments, and psychotic features may also be present.10,11 Behavioral disturbances in CLN3 disease may not simply reflect primary psychiatric conditions but instead may arise from developmentally mediated processes associated with severe cognitive decline and underlying neurobiological dysfunction. 12 However, the precise neurobiological mechanisms underlying these manifestations remain incompletely understood. 13
In a study conducted in Finland involving 27 patients diagnosed with JNCL, the most frequently observed psychiatric symptoms were reported to be social problems, thought disorders, attention deficits, somatic complaints, aggressive behavior, as well as sleep and speech disturbances. Psychiatric symptoms were found to be more pronounced in female patients compared with males, and the most commonly used psychotropic medications were reported to be the antidepressant citalopram and the antipsychotic risperidone. 14
In addition to these neuropsychiatric features, the disease is characterized by a progressive clinical course, and life expectancy is generally limited, with most patients surviving only into their 30s. 15 Despite this growing body of evidence, manic episodes remain rarely characterized within a structured diagnostic framework in patients with JNCL, highlighting the need for further case-based documentation to better define bipolar-spectrum manifestations in CLN3 disease.
Case
A 16-year-old female patient presented to the child and adolescent psychiatry outpatient clinic with complaints of pressured speech, decreased need for sleep, increased energy levels, recurrent episodes of leaving home without permission, and heightened sexual interest and behaviors. She was the child of a consanguineous marriage and the third of 4 siblings. Motor and cognitive development were reported to be normal until age 8 years, when progressively worsening visual impairment and academic decline emerged. She had been receiving levetiracetam 500 mg twice daily for 3 years because of epileptic seizures.
Clinical history revealed that her sister, who was 3 years older, had experienced learning and attention difficulties beginning at approximately 10 years of age, followed by progressive visual impairment. She also had a history of psychiatric hospitalization due to psychotic symptoms accompanied by a catatonic presentation, based on limited parental report. The 2 male siblings had no reported neurologic or psychiatric conditions. There was no known family history of bipolar disorder or other major psychiatric disorders.
The patient's first psychiatric presentation occurred approximately 6 months prior, with complaints of irritability and restlessness. Over the subsequent months, the patient developed progressively increasing irritability, hypersexuality, reduced sleep duration, increased energy levels, and visual hallucinations. Mental status examination revealed pressured speech and loosened associations. The clinical presentation fulfilled criteria for a manic episode according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), 16 including decreased need for sleep, increased goal-directed activity, and engagement in risky behaviors. The diagnosis was based on comprehensive clinical evaluation by a child and adolescent psychiatrist, without the use of standardized rating scales.
Olanzapine was initiated at a dose of 5 mg/d and titrated to 10 mg/d. During follow-up, the patient showed significant clinical improvement, including normalization of sleep patterns, reduction in irritability, and stabilization of energy levels. Her mood was euthymic, and no psychotic symptoms were observed.
Brain magnetic resonance imaging (MRI), performed in 2020, demonstrated prominent perivascular spaces in the bilateral periatrial white matter, accompanied by minimal perivascular gliosis. Electroencephalography (EEG) recordings obtained in April 2024 and January 2025 were within normal limits, with no evidence of epileptiform activity. A representative axial fluid-attenuated inversion recovery MR image demonstrating posterior periventricular gliotic changes is shown in Figure 1.
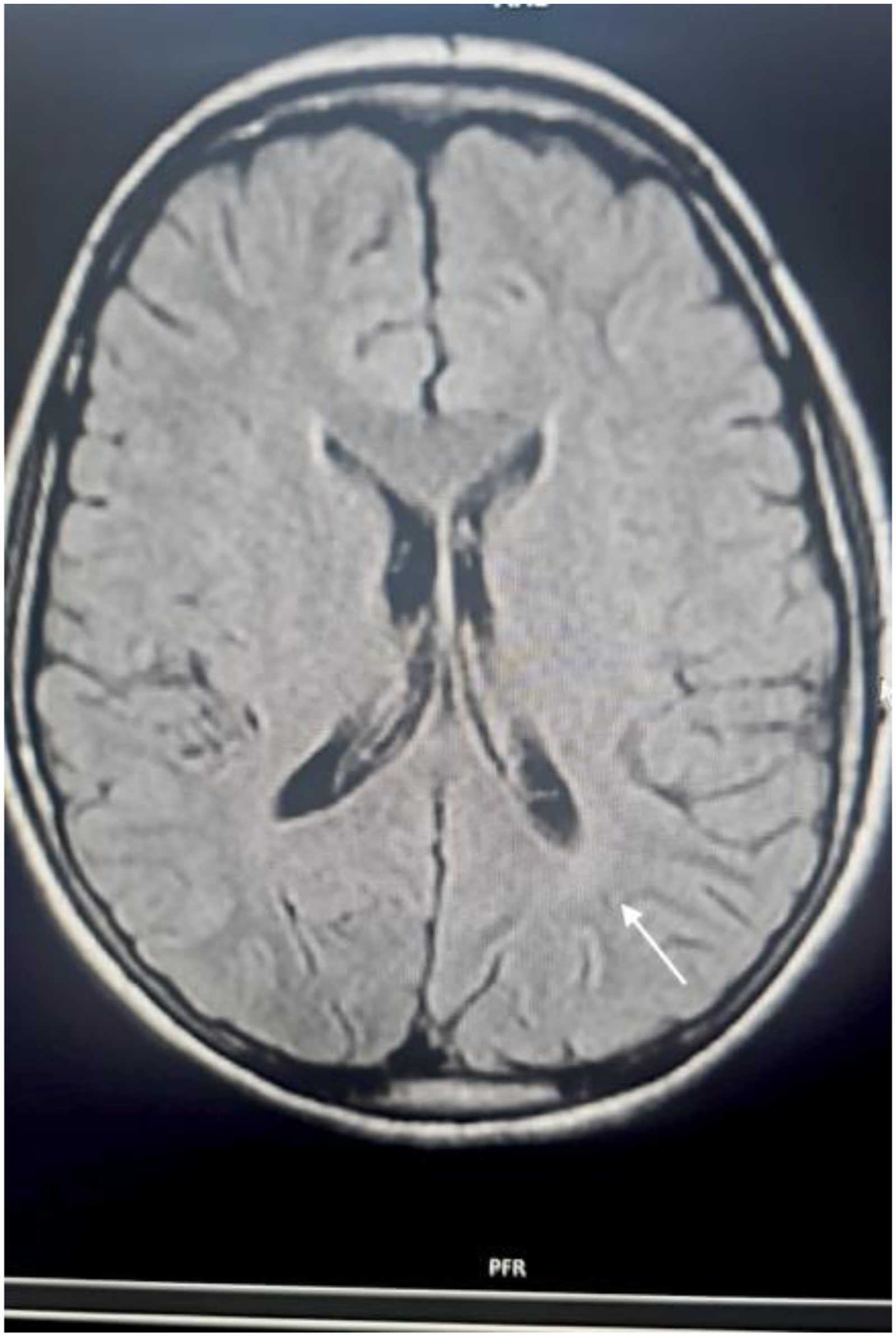
Representative axial fluid-attenuated inversion recovery magnetic resonance image showing posterior periventricular gliotic changes.
Genetic testing was performed using whole exome sequencing as part of the ongoing diagnostic evaluation. The results became available during follow-up and were shared with the psychiatric team. A homozygous likely pathogenic variant in the CLN3 gene (c.898C>T) was identified in the patient. The same variant was also detected in her older sister. Although detailed parental genotype data were not available, these findings are consistent with autosomal recessive inheritance.
Because of increased appetite, cross-titration to risperidone 2 mg/d was performed, and quetiapine 50 mg/d was added for sleep disturbances. The patient continues to receive regular psychiatric follow-up within a multidisciplinary care framework, including pediatric neurology, pediatric cardiology, ophthalmology, physical therapy, and rehabilitation services. The clinical course is summarized in Figure 2.
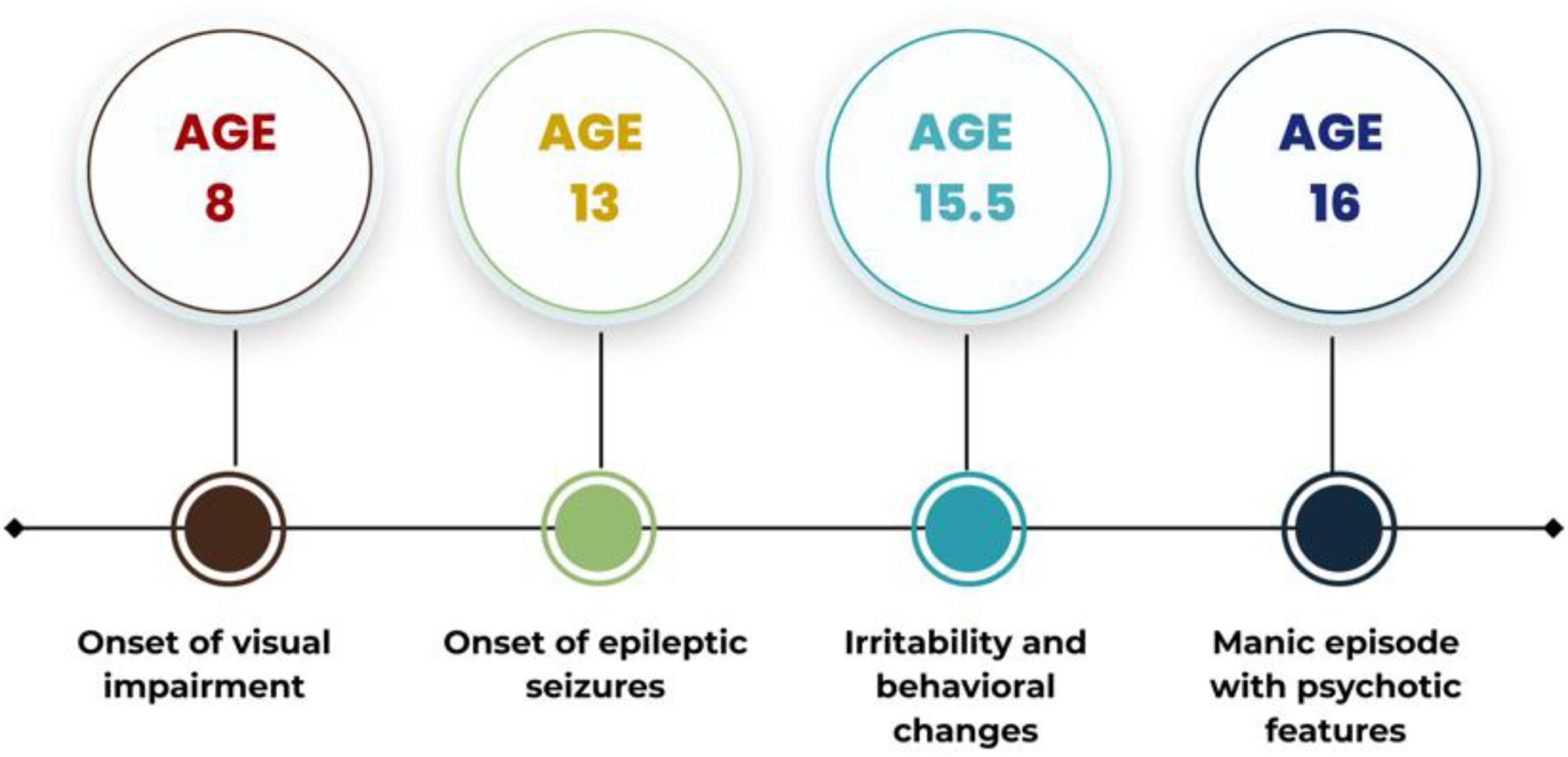
Timeline of clinical course.
Discussion
Neuropsychiatric manifestations are increasingly recognized as part of the clinical spectrum of CLN3 disease, including behavioral disturbances, mood symptoms, and psychotic features. However, well-characterized manic episodes fulfilling DSM-5 criteria remain rarely described. This case suggests that CLN3-associated neurodegeneration may present with symptoms consistent with a manic episode within the bipolar spectrum and highlights the importance of systematic psychiatric assessment and longitudinal monitoring in patients with JNCL.
The symptoms and clinical course of bipolar disorder can vary significantly among individuals, and their underlying pathologic mechanisms remain incompletely understood. Traditionally, psychiatric illnesses have been conceptualized as complex, polygenic conditions with multifactorial etiologies. Although single-gene mutations are relatively rare, their mechanisms are often well-characterized, offering valuable insights into the shared pathophysiological pathways between neurologic and psychiatric disorders.
Differential Diagnostic Considerations
The differential diagnosis in this case required careful consideration. Behavioral dysregulation in CLN3 disease may arise from multiple factors, including neurodegeneration-related psychiatric symptoms, epilepsy-related behavioral changes, and antiepileptic drug–induced psychiatric effects.
Neurodegenerative disorders are known to be associated with behavioral and mood disturbances, including disinhibition and affective dysregulation. However, the presence of core manic symptoms, including decreased need for sleep, increased goal-directed activity, and hypersexuality, supports a manic episode within the bipolar spectrum rather than nonspecific behavioral changes.
Levetiracetam is known to be associated with behavioral adverse effects, including irritability and agitation. 17 Although these adverse effects most commonly occur within the first months of treatment, delayed-onset psychiatric symptoms have also been reported. 18 However, the patient had been receiving a stable dose of levetiracetam for several years without recent dose adjustments, and repeated EEG recordings were within normal limits. These findings reduce the likelihood of medication-related or seizure-related behavioral changes, supporting a bipolar-spectrum manic episode. Although spontaneous remission cannot be entirely excluded, the temporal association between antipsychotic treatment and clinical improvement suggests a treatment-related effect.
Neurobiological Considerations
Recent studies suggest that inflammatory processes may play a significant role in the pathophysiology of mood disorders. 19 A study by Privitera et al 20 identified an association between heterozygous variants in the CLN6 and ZNF92 genes and an increased risk of bipolar disorder. These findings suggest that even heterozygous variants in NCL-related genes may influence psychiatric phenotypes. Furthermore, experimental studies have suggested a possible molecular interaction between CLN6 and CLN3, both of which are membrane-bound proteins; however, it remains unclear whether this interaction is direct.21,22 Taken together, these observations raise the possibility of shared underlying biological pathways, although such interpretations remain speculative and should be approached with caution. Importantly, despite increasing recognition of psychiatric symptoms in CLN3 disease, reports of manic episodes remain limited, supporting the relevance of the present case in expanding the clinical spectrum.
In this context, a recent study examining neurodevelopmental and psychiatric disorders in individuals with JNCL identified attention-deficit hyperactivity disorder as the most common single diagnosis. 23 It should also be borne in mind that some symptoms attributed to attention-deficit hyperactivity disorder may overlap with early affective manifestations, including impulsivity, irritability, and increased activity levels. In a progressive neurodegenerative disorder such as JNCL, where behavioral dysregulation is common, distinguishing neurodevelopmental symptoms from emerging mood-related features may be particularly challenging, especially in the early stages of the disease.
Another consideration is that many patients with JNCL are treated from a young age with antiepileptic drugs and antipsychotics to control seizures and behavioral symptoms, which may influence the clinical expression of mood-related phenomena. Such treatments may mask or attenuate manic symptomatology, potentially contributing to the limited reporting of manic features in this population. Taken together, these considerations point to a gap in the characterization of mood symptoms in JNCL and highlight the need for more systematic and longitudinal investigation.
Conclusion
In patients with CLN3 disease, a multidisciplinary approach involving psychiatry, neurology, ophthalmology, and rehabilitation is essential for optimal care. Early recognition and careful characterization of psychiatric symptoms may improve quality of life and reduce caregiver burden. More broadly, this case highlights the importance of systematically evaluating psychiatric manifestations within neurogenetic and neurodegenerative disorders, as these conditions may present with clinically recognizable neuropsychiatric syndromes, including bipolar-spectrum features.
Limitations
This report has several limitations. Detailed genetic variant annotation, including the full HGVS protein-level description and ACMG classification criteria, was not available. Parental genotype data were also unavailable, limiting segregation analysis. In addition, longitudinal neuropsychological assessments and biomarker data were not available. Therefore, the findings should be interpreted as associative rather than causal. Further studies are needed to better characterize the relationship between CLN3-related neurodegeneration and bipolar-spectrum manifestations.
Footnotes
Acknowledgements
We thank the patient and her family for their cooperation throughout the clinical evaluation and publication process.
Ethical Considerations
Written informed consent for the publication of anonymized clinical data were obtained from the patient's family. The clinical evaluation and initial management of the patient were conducted at a previous institution where the corresponding author was employed at the time.
Author Contributions
ES contributed to patient evaluation, case conceptualization, and manuscript drafting. DNT contributed to literature review and manuscript revision. All authors approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available because of the sensitive nature of the clinical information and the possibility of identifying the individual case.