
Abstract
Rationale:
Despite guidelines advising passive rewarming for mild accidental hypothermia (AH), patients are frequently admitted to intensive care unit (ICU) for active rewarming using a forced-air warming device. We implemented a new policy at our institution aimed at safely reducing ICU admissions for AH. We analyzed our practice pre- and post-policy intervention and compared our experiences with acute care hospitals in Connecticut.
Methods:
A retrospective chart review was performed on 203 participants with AH identified by primary and secondary discharge codes. Our new policy recommended passive rewarming on the medical floors for mild hypothermia (>32°C) and ICU admission for moderate hypothermia (<32°C). Practices of other Connecticut hospitals were obtained by surveying ICU nurse managers and medical directors.
Results:
Over a 3-year period, prior to rewarming policy change, 64% (n = 92) of patients with AH were admitted to ICU, with a mean ICU length of stay (LOS [SD]) of 2.75 (2.2) days. After the policy change, over a 3-year period, 15% (n = 9) were admitted to ICU (P < .001), with an ICU LOS of 2.11 (0.9) days (P = 0.005). In both groups with AH, altered mental status, infection, and acute alcohol intoxication were the most common diagnoses at presentation. Alcohol intoxication was more prevalent in the post-policy intervention group, pre 17% versus post 46% (P < .001). No complications such as dermal burns or cardiac arrhythmias were noted with forced-air warming device use during either time period. Among the 29 hospitals surveyed, 20 used active rewarming in ICU or intermediate care units and 9 cared for patients on telemetry units. Most hospitals used active external rewarming for core body temperature of <35°C; however, 37% of hospitals performed active rewarming at temperatures >35°Cor lacked a policy.
Conclusions:
Reserving forced-air warming devices for the treatment of moderate-to-severe hypothermia (<32°C) significantly reduced ICU admissions for AH.
Background
Hypothermia can be life-threatening due to cardiovascular instability, acute renal failure, coagulopathy, and electrolyte imbalance and warrants evaluation by a medical professional. Every year approximately 1500 deaths are due to primary hypothermia in the United States. 1 Accidental hypothermia (AH) is defined as an involuntary drop in core body temperature to <35°C. 1,2 Stages of hypothermia as defined by core body temperature and clinical presentation influence resuscitation methods. A common approach to classify hypothermia using core body temperature defines mild hypothermia as 32°C to 35°C, moderate hypothermia as 28°C to 32°C, and severe hypothermia as less than 28°C. 2,3
In mild AH, guidelines in emergency management recommend passive rewarming. 4 Despite this recommendation, we observed these patients with mild hypothermia frequently being admitted to the intensive care unit (ICU) for active external rewarming with a forced-air warming blanket. Concerns about adverse effects associated with the use of forced-air warming blankets such as cardiac arrhythmia, dermal burns, and cardiovascular collapse have restricted its use to monitored settings such as emergency departments (EDs), operating rooms, post-anesthesia care units, and ICU, per our hospital policy. 1,5
To understand the frequency of ICU admissions for mild hypothermia and potential overuse of resources, we surveyed treatment practices for AH at all acute care hospitals in Connecticut. At our institution, we performed a retrospective cohort study and analyzed rewarming methods, in-hospital site of care, and outcomes for patients treated with AH before and after implementation of a guideline-based rewarming policy aimed at safely reducing ICU admission for this condition.
Methods
The study consisted of a multi-hospital survey and a pre–post analysis of an intervention approved by the hospital institutional review board. Intensive care unit nurse managers or medical ICU directors at all acute care hospitals in the state of Connecticut were surveyed over the telephone about rewarming policies, practices, and complications at their institutions associated with active rewarming for the treatment of AH. A retrospective chart review was performed of patients treated at our community hospital with AH identified by primary and secondary discharge codes: International Classification of Diseases, Ninth Revision (ICD-9) codes 991.6 and 780.65 during the pre-intervention period from July 2009 to July 2012 and the post-intervention period from July 2013 to September 2015 and ICD-10 codes R98.0 and T68.XXXA from October 2015 to April 2016.
The inclusion criteria were age 18 years and older with suspected AH seen only in the ED or admitted from the ED to the hospital. Exclusion criteria were intraoperative or postoperative hypothermia, hospice care, and transient hypothermia for which no rewarming treatment was administered. Patient characteristics abstracted from the medical record included core body temperature on admission, admission diagnosis, comorbid conditions, hospital admitting location, method of rewarming, and complications associated with active rewarming.
Active rewarming was ordered at the discretion of the treating physician and was performed using a Bair Hugger blanket (model 505; 3M Health Care, Little Canada, MN). Passive rewarming was accomplished by removal of wet clothes, application of warm blankets, provision of warm drinks, and raising ambient temperature.
In May 2013, a change in rewarming policy was implemented at our institution. The new policy included guidelines for the use of forced-air warming systems for patients with hypothermia. A persistent core body temperature of <32°C, which was unresponsive to active rewarming in the ED, mandated admission to the ICU for ongoing active rewarming. For a temperature >32°C, patients received passive rewarming and were admitted to medical/surgical floors or telemetry. The policy continued to allow forced-air warming blanket use in the ED, post-anesthesia care unit, and ICU. All patients receiving active rewarming had continuous temperature monitoring via a rectal or esophageal probe. In cases of severe AH, active external rewarming was initiated, and these patients were evaluated on a case-by-case basis for transfer to a tertiary center with extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass (CPB) capabilities.
Descriptive statistics (means and frequencies) were calculated for all patient characteristics. Chi-square analyses were used to compare categorical variables (characteristics, comorbidities, and hypothermia class), and t tests compared continuous variables (age, temperature, and ICU length of stay [LOS]) in the pre- and post-policy change groups.
Results
Twenty-nine acute care hospitals in Connecticut were surveyed between July 2009 and September 2011. Twenty (69%) of these hospitals admitted patients for active rewarming to ICU or intermediate care units and 9 hospitals treated their patients on telemetry units. Most hospitals had a policy for starting active rewarming based on a core body temperature <35°C, but 30% of centers employed active rewarming for temperatures >35°C and 2 hospitals lacked a protocol for ordering active rewarming based on core body temperature. All respondents recalled low rates of complications (<1%) with forced-air warming blankets and no health-care providers recalled patients experiencing thermal injuries.
During the 3-year period prior to a rewarming policy change, 144 patients treated at our hospital met the inclusion criteria for AH. The mean (SD) patient age was 72 (18) years, and the most common admitting diagnoses were altered mental status, infection, hypoglycemia, and alcohol intoxication (Table 1). The mean admission temperature recorded was 33.7°C (1.4°C). The majority of patients, 64% (n = 92), were admitted to the ICU, with a mean ICU LOS of 2.75 (2.2) days. Among the patients admitted to the ICU, 86% (n = 79) had mild hypothermia and received active rewarming with forced-air warming blankets. A minority of patients, 14% (n = 13), had moderate hypothermia (Table 2). No patients met criteria for severe AH. Active rewarming was initiated in the ED in 96% (n = 88) of the patients who were admitted to the ICU.
Patient Characteristics.
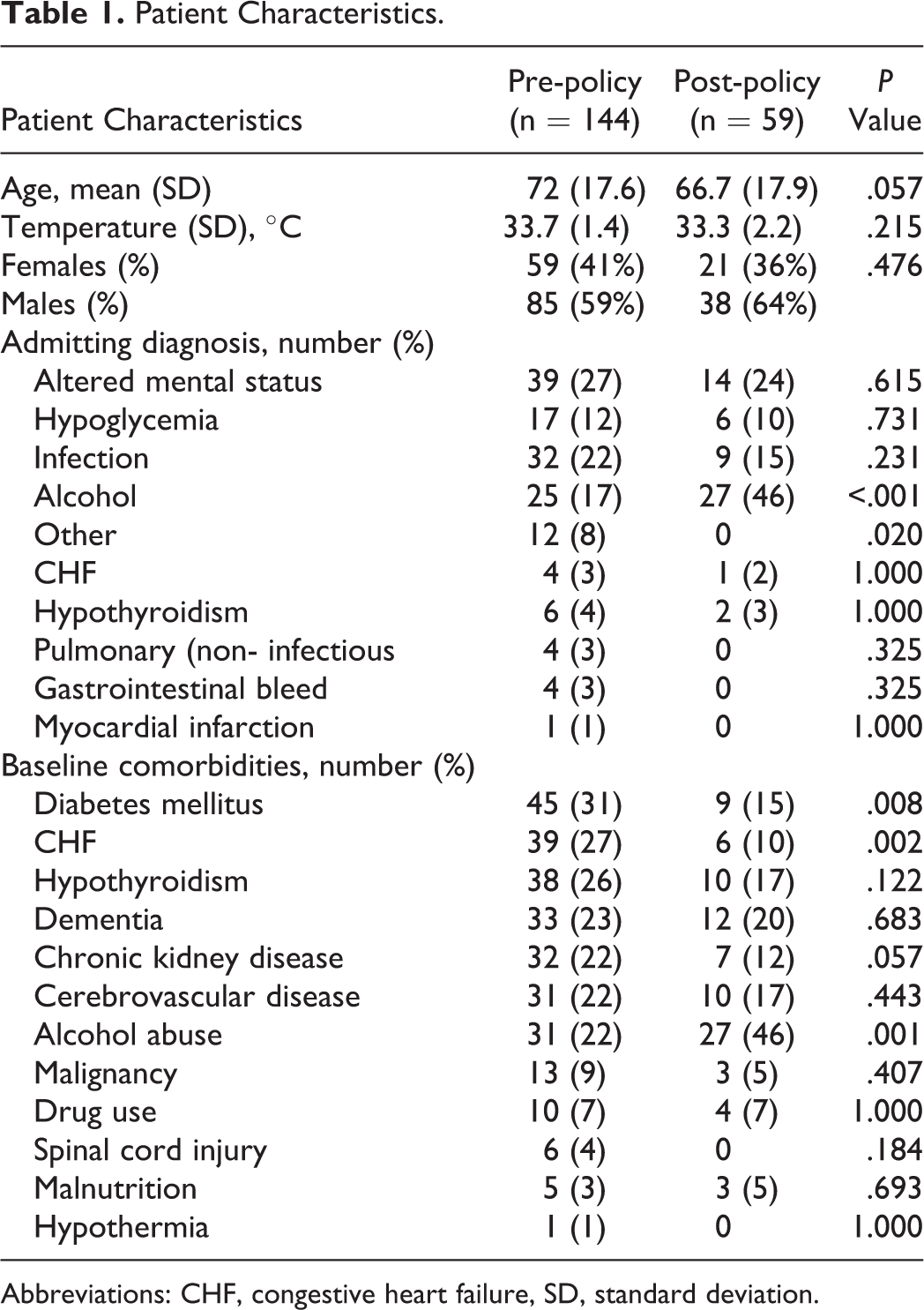
Abbreviations: CHF, congestive heart failure, SD, standard deviation.
Patients Admitted to ICU.
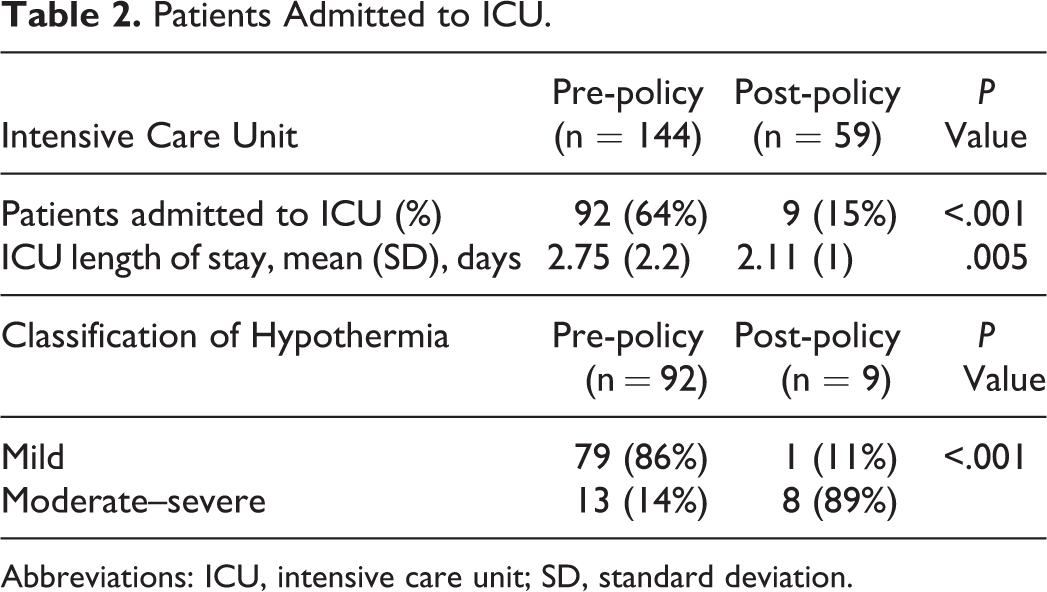
Abbreviations: ICU, intensive care unit; SD, standard deviation.
For the 3 years following the institution of the rewarming policy, 59 patients met the inclusion criteria for the study. The mean (SD) patient age was 67 (18) years (Table 1). Acute alcohol intoxication was a more prevalent admitting diagnosis in the post-policy intervention group, pre 17% versus post 46% (P < .001). The mean temperature (33.3°C [2.2°C]) recorded was similar to that of the pre-policy change group; however, only 15% (n = 9) were admitted to the ICU for active rewarming (P < .001). Mean ICU LOS was reduced 23% to 2.11 (0.9) days (P = .005). The majority of patients, 89% (n = 8), treated with forced-air warming blankets in ICU had moderate (n = 5) or severe (n = 3) hypothermia and 1 patient (11%) had mild hypothermia. This patient had septic shock and received active rewarming therapy in ICU at the discretion of the treating physician. Baseline comorbid conditions between the 2 groups were similar, with the exception of more diabetes mellitus and congestive heart failure in the pre-policy group and more alcoholism in the post-policy group (Table 1). No complications such as dermal burns or cardiac arrhythmias were noted with forced-air warming blanket use during the study period.
Discussion
Introduction of a guideline-based policy limiting forced-air warming blanket use to those with moderate and severe hypothermia (<32°C) was followed by a 10-fold decrease in ICU admission and a 23% reduction in ICU LOS. Prior to 2013, our policy recommended active rewarming in the ED or ICU, based on core body temperature alone (<35°C) and regardless of clinical stability. This practice was shared by the majority of acute care hospitals within the state of Connecticut. The change in our rewarming policy was guided by evidence for the safety of passive rewarming in mild hypothermia. 1,5
Optimal treatment for moderate AH involves cardiac monitoring and active external rewarming. 1 Atrial fibrillation is common in moderate hypothermia 6 ; however, the risk of malignant cardiac arrhythmia and cardiac arrest is substantially higher with severe hypothermia. 4 Patients with severe AH who are unconscious with cardiac and/or hemodynamic instability should be managed in a hospital with ECMO or CPB capabilities. 1
The change in active rewarming policy was associated with a shift in the profile of the patients treated. Pre-policy intervention, patients had baseline comorbidities such as congestive heart failure, diabetes mellitus, and hypothyroidism compared with more alcoholism in the post-policy intervention. Nearly half of all patients cared for with AH were acutely intoxicated with alcohol, a substantial increase from 17% pre-policy intervention. Alcohol intoxication is known to cause peripheral vasodilation, volume loss, impaired judgment, stupor, or coma and has been reported as a common risk factor for AH 7 and fatalities related to hypothermia. 8
No complications of dermal burns were observed at our institution or reported by centers around Connecticut with the use of forced-air warming blankets. Thermal burn injuries have been described in anesthesiology literature due to misuse of forced-air warming blankets. This practice is known as “hosing” 9 and involves detaching the hose from the blanket and blowing air directly onto a patient’s skin and is clearly warned against by the manufacturer in the operator manual.
Certain methodological limitations of our study are worth noting. The surveys to understand rewarming practices at hospitals across the state were done over the telephone with ICU nurse managers and medical directors and were subject to recall bias. The remainder of the study was a retrospective single-center analysis. Our results largely reflect the safety of active external rewarming in mild-to-moderate AH, as our study population only had 3 patients with severe AH. Although we are confident the more stringent policy implementation led to improved resource utilization by directly influencing site of care, our results are not generalizable to all patients presenting with AH. After the change in policy, the number of cases with primary or secondary discharge diagnoses of AH decreased by 59%. The possible reasons may have been social or environmental factors as well as a direct result of guidelines recommending de-escalation of warming therapy.
In summary, use of passive rewarming for mild hypothermia and limiting forced-air warming blankets for moderate or severe hypothermia were followed by a significant decrease in ICU admissions and reduced ICU LOS without compromising patient safety. No complications such as dermal burns or cardiac arrhythmias were recorded with forced-air warming blanket use during the last 6 years at our hospital. A trial of active rewarming in a non-high dependency unit is needed to evaluate its safety in this setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.