
Abstract
Background:
Morbidly obese patients with respiratory failure who do not improve on conventional mechanical ventilation (CMV) often undergo rescue therapy with extracorporeal membrane oxygenation (ECMO). We describe our experience with high-frequency percussive ventilation (HFPV) as a rescue modality.
Methods:
In a retrospective analysis from 2009 to 2016, 12 morbidly obese patients underwent HFPV after failing to wean from CMV. Data were collected regarding demographics, cause of respiratory failure, ventilation settings, and hospital course outcomes. Our end point data were pre- and post-HFPV partial pressure of arterial oxygen and PaO2 to fraction of inspired oxygen (PF) ratios measured at initiation, 2, and 24 hours.
Results:
Twelve morbidly obese patients required HFPV for respiratory failure. Causes of respiratory failure overlapped and included cardiogenic pulmonary edema (n = 8), pneumonia (n = 5), septic shock (n = 5), and asthma (n = 1). After HFPV initiation, mean fraction of inspired oxygen FiO2 was tapered from 98% to 82% and 66% at 2 and 24 hours, respectively. Mean PaO2 increased from 60.9 mm Hg before HFPV to 175.1 mm Hg (P < .05) at initiation of HFPV, then sustained at 129.5 mm Hg (P < .05) and 88.1 mm Hg (P < .005) at 2 and 24 hours, respectively. Mean PF ratio improved from 66.1 before HFPV to 180.3 (P < .05), 181.0 (P < .05) and 148.9 (P < .0005) at initiation, 2, and 24 hours, respectively. The improvement in mean PaO2 and PF ratios was durable at 24 hours whether or not the patient was returned to CMV (n = 10) or remained on HFPV (n = 2). Survival to discharge was 66.7%.
Conclusion:
In our cohort of morbidly obese patients, HFPV was successfully utilized as a rescue therapy precluding the need for ECMO. Despite our small sample size, HFPV should be considered as a rescue therapy in morbidly obese patients failing CMV prior to the initiation of ECMO. Our retrospective analysis supports consideration for HFPV as another form of rescue therapy for obese patients with refractory hypoxemia and respiratory failure who are not improving with CMV.
Keywords
Introduction
Obesity is known to be associated with pulmonary dysfunction. Increasing body mass index (BMI) has been correlated with reduced forced expiratory volume in 1 second, forced vital capacity, total lung capacity, functional residual capacity, and expiratory reserve volume. 1 –4 This is primarily due to the weight of the abdominal contents and chest wall increasing mechanical load on diaphragm excursion and thoracic compliance. 1,5,6 Because of these physiological changes, obese patients are predisposed to respiratory failure from acute insults, along with greater morbidity and increased duration of conventional mechanical ventilation (CMV). 5,7,8
Current salvage modalities that exist in patients who fail CMV and other nonventilatory techniques (neuromuscular blockade, tailored positive end-expiratory pressure [PEEP], prone positioning [PP] and recruitment maneuvers, and inhaled nitric oxide) are nontraditional ventilatory modes and extracorporeal membrane oxygenation (ECMO). 9,10 Although these modes and ECMO can be effective, they are not without significant practical difficulties when utilized in morbidly obese patients.
Nonconventional ventilator modes in the setting of severe hypoxemic respiratory failure include high-frequency ventilation (HFV). The HFV delivers at least 150 cycles per minute or more of subphysiologic tidal volumes. There are 3 main types—jet, oscillatory, and percussive ventilation. High-frequency oscillatory ventilation (HFOV) oscillates the lung at a constant mean airway pressure, thus allowing for maintenance of alveolar recruitment while avoiding low end-expiratory pressure and high peak pressures. 11 In contrast, high-frequency percussive ventilation (HFPV) is a pneumatically powered, pressure-limited, flow-regulated and time-cycled ventilation modality that delivers a sequence of high-frequency (200-900 cycles per minute) percussions with subphysiological small tidal volumes in a consecutive stepwise stacking pattern, leading to the formation of low-frequency (up to 30 cycles per minute), convective, pressure-limited breathing cycles. The HFPV is nearly instantaneously adapting to the changes in the lung compliance and airway resistance while creating autocephalad countercurrent flow of air, facilitating removal of intrapulmonary secretions and displacement of trapped gas. Improvement in oxygen exchange with alveolar recruitment occurs while maintaining low peak airway pressures in comparison to CMV, thus also reducing the risk of barotrauma. 12 –15 In this manuscript, we review our experience with HFPV in morbidly obese patients failing CMV.
Methods
Local institutional review board waived approval for this study. Informed consent was waived due to the observational retrospective design of the study. Electronic medical records were searched using the term “HFPV” from November 2009 to December 2016. In all, 60 patients requiring HFPV for respiratory failure were identified, with 12 being morbidly obese (BMI > 35 kg/m2). The HFPV was initiated in these patients after prolonged status of PaO2 to FiO2 ratio (PF) ratio <100 or if they did not show improvement on CMV despite paralysis and sedation, at the discretion of the intensive care unit team. The HFPV was delivered via volumetric diffusive respirator 4 (Percussionare Corp, Sandpoint, Idaho). Basic initial settings include high-frequency rate of 500 to 600 percussions per minute, convective rate of 15 breaths per minute, the lowest pulsatile flow rate leading to the rise of the chest, continuous positive airway pressure of 10 to 15 cm H2O, FiO2 titrated down to avoid hyperoxia, and inspiratory to expiratory ratio of 1:1 on both convective and percussive rate. Humidification is provided by humidifier (MR 850; Fisher & Paykel, Auckland, New Zealand) set up at 39°C.
Data collected encompassed demographics (age, sex, height, weight, BMI, and cause of respiratory failure), progression of oxygenation, and hospital course, including clinical outcomes such as success of weaning from mechanical ventilation and overall survival. Respiratory support data included pre-HFPV and HFPV ventilation settings, PaO2, and PF ratios at initiation, 2, and 24 hours. Hospital course data include days on HFPV, post-HFPV patient course, and survival to discharge. Primary end point data were pre- and post-HFPV PaO2 and PF ratios collected at initiation, 2, and 24 hours.
Statistical Analysis
Clinical data are presented as mean. Student paired t test was used to analyze PaO2 and PF ratio progressions on HFPV, where a P value <.05 was considered statistically significant. Outcomes were plotted on linear diagrams with standard deviations and confidence intervals (CI; Figures 1 and 2). Ventilation FiO2 settings were compared as means in the analysis of oxygenation progression.
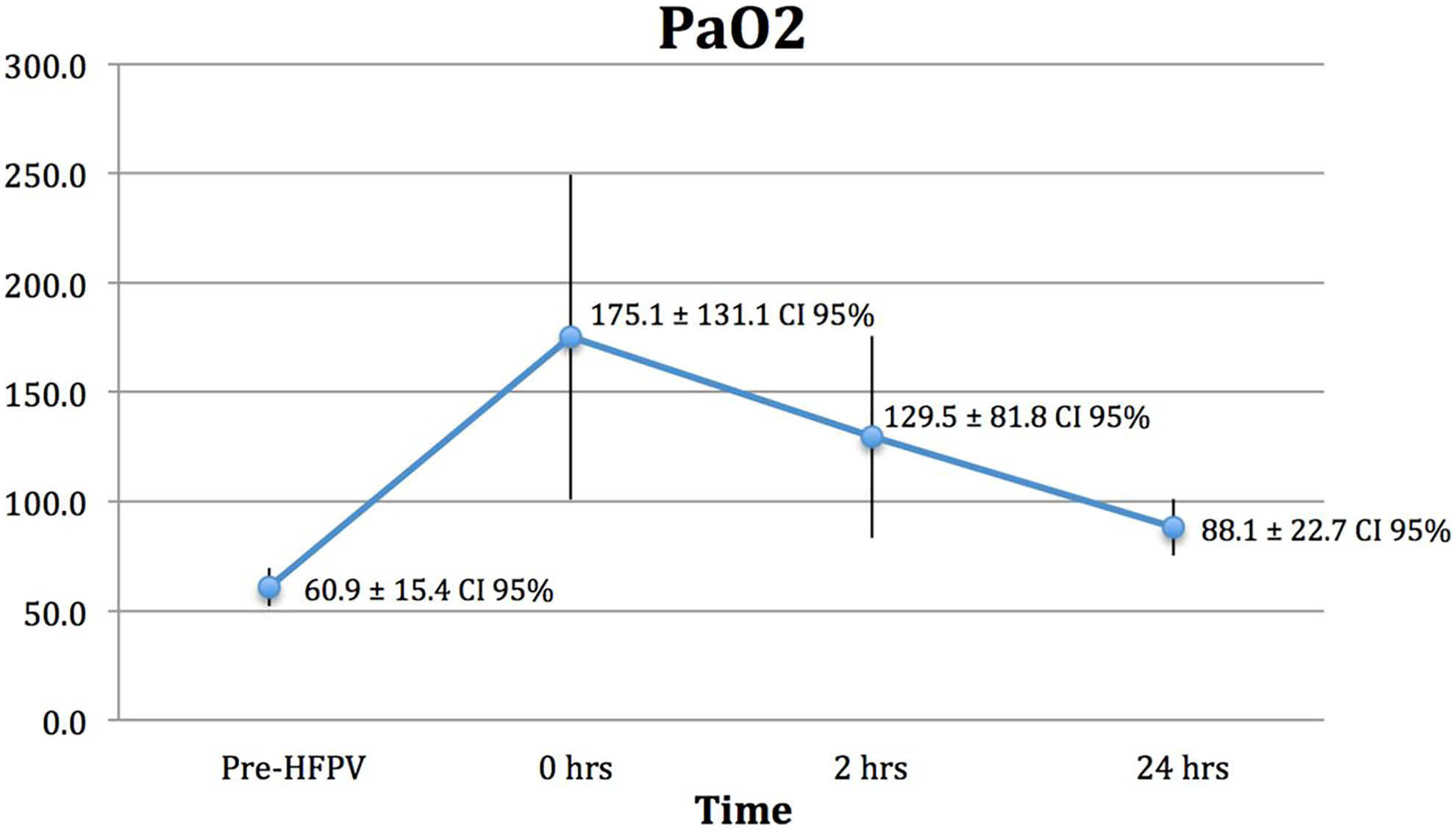
PaO2 prior to initiation of HFPV, beginning of HFPV, and 2 and 24 hours after HFPV initiation. HFPV indicates high-frequency percussive ventilation; PaO2, partial pressure of arterial oxygen.
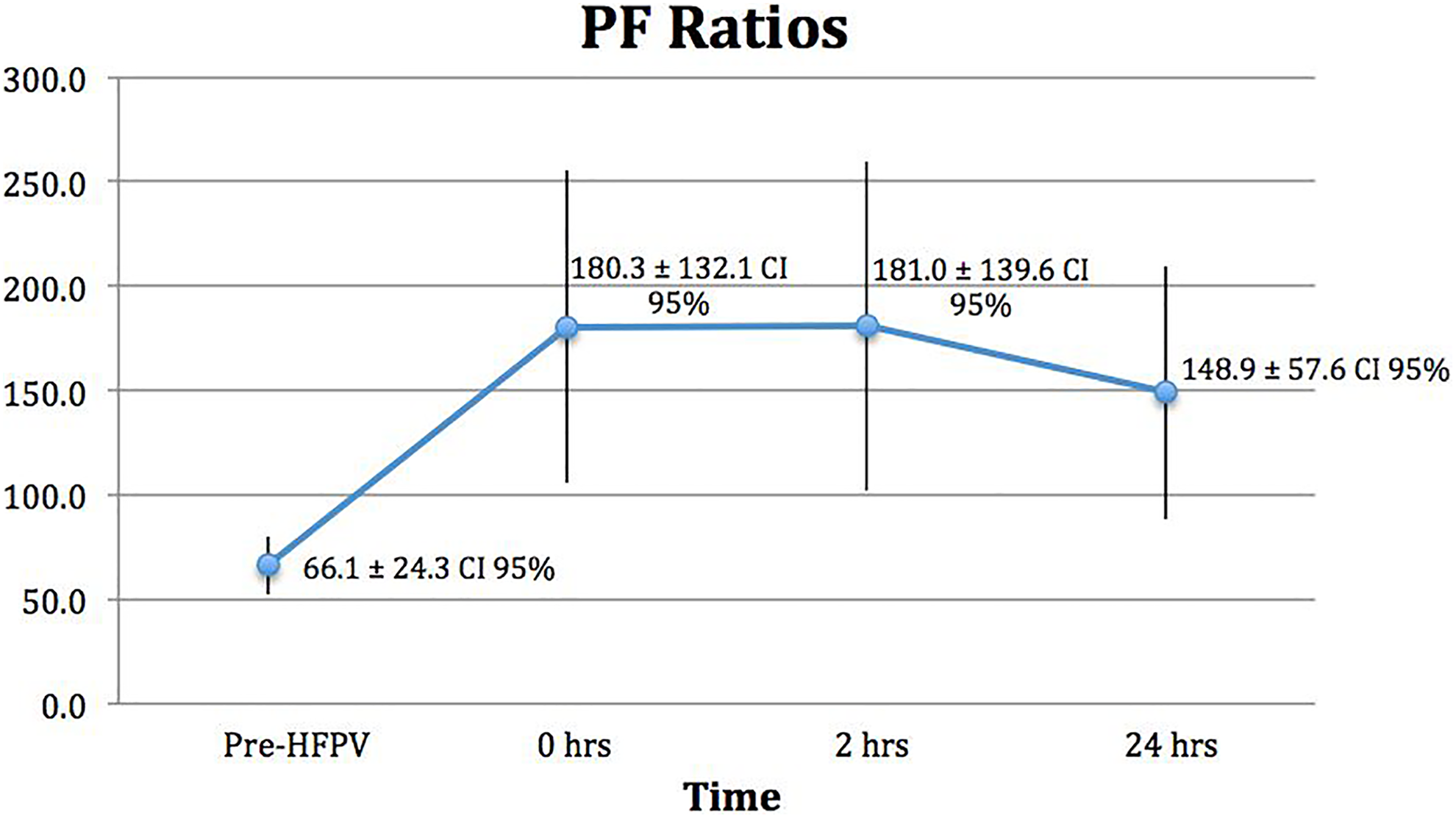
PF ratios prior to initiation of HFPV, beginning of HFPV, and 2 and 24 hours after HFPV initiation. HFPV indicates high-frequency percussive ventilation; PF ratio, partial pressure of arterial oxygen to fractional inspiration of oxygen ratio.
Results
Twelve morbidly obese patients were identified with mean BMI of 42.9, ranging between 36 and 55 kg/m2. Mean patient age was 56, ranging between 28 and 85 years. Causes of respiratory failure overlapped and included cardiogenic pulmonary edema (n = 8), pneumonia (n = 5), septic shock (n = 5), and asthma (n = 1). Demographics and causes of respiratory failure are listed in Table 1.
Demographics.
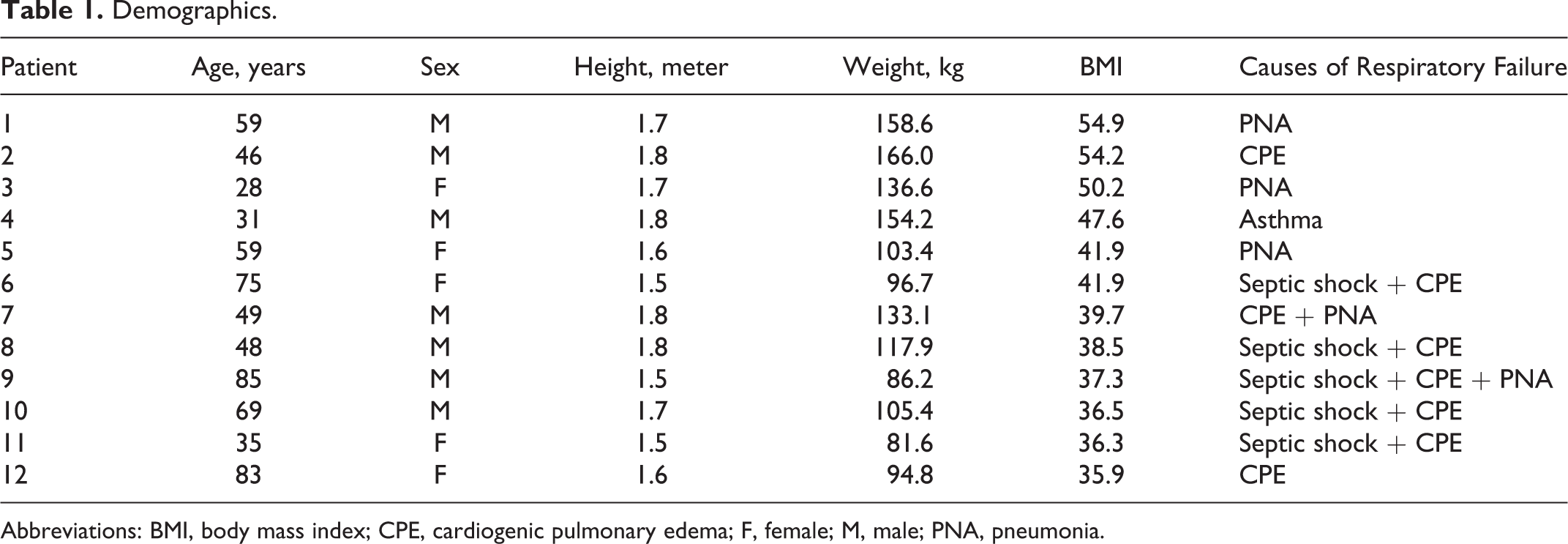
Abbreviations: BMI, body mass index; CPE, cardiogenic pulmonary edema; F, female; M, male; PNA, pneumonia.
Pre-HFPV CMV included pressure-regulated volume control, assist control/volume control, and pressure control. The CMV mean FiO2 was 95%, mean PEEP was 15.8 cm H2O, mean PaO2 of 60.9 mm Hg, and a mean PF ratio of 66.1, indicating severe respiratory failure (Table 2).
Respiratory Support Data.
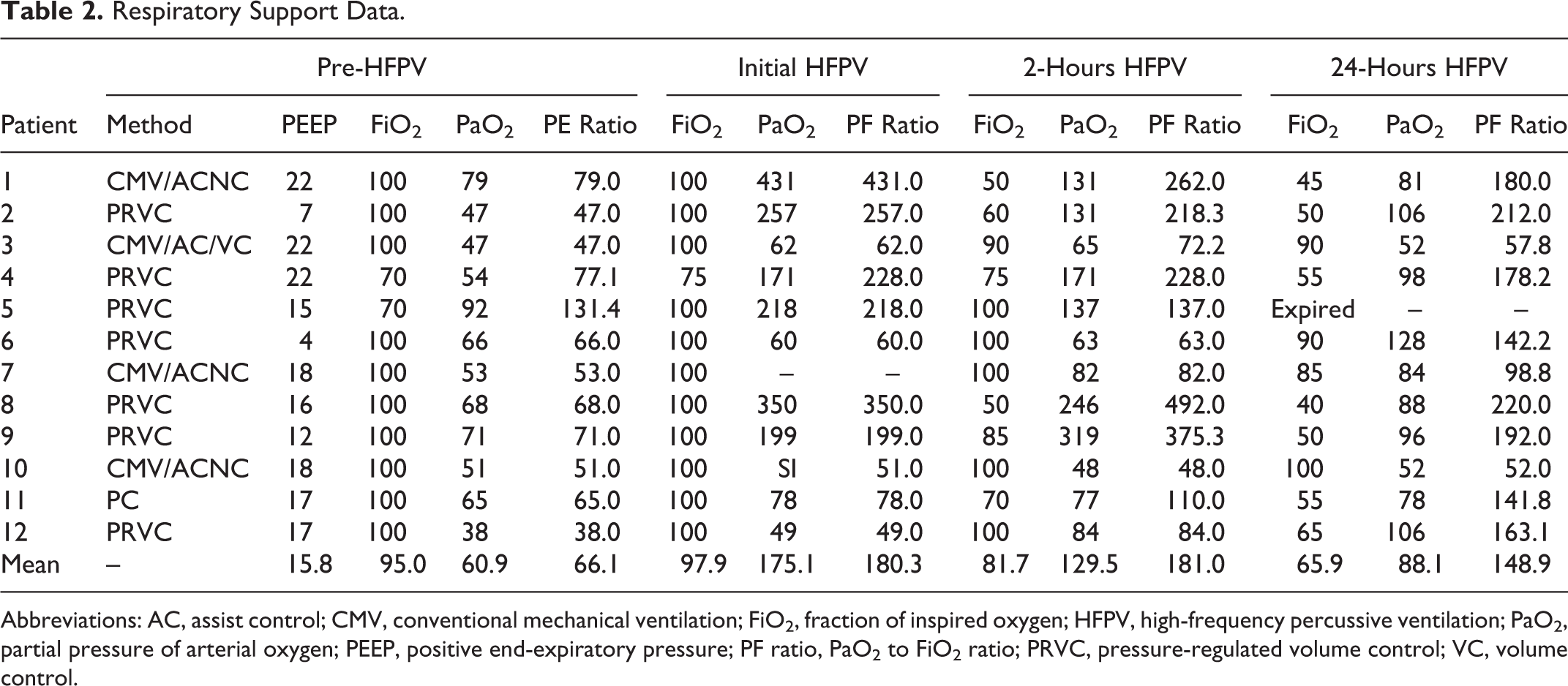
Abbreviations: AC, assist control; CMV, conventional mechanical ventilation; FiO2, fraction of inspired oxygen; HFPV, high-frequency percussive ventilation; PaO2, partial pressure of arterial oxygen; PEEP, positive end-expiratory pressure; PF ratio, PaO2 to FiO2 ratio; PRVC, pressure-regulated volume control; VC, volume control.
The HFPV FiO2 settings were initially approximated to that of previous oxygenation support, with a mean FiO2 of 97.9%. Mean PaO2 drastically increased from 60.9 to 175.1 mm Hg at initiation (±131.1, CI: 94.8%, P < .05). FiO2 was gradually decreased thereafter to avoid hyperoxia. Mean FiO2 of 81.7% at 2 hours resulted in mean PaO2 of 129.5 mm Hg (±81.8, CI: 60.4%, P < .05). Tapering mean FiO2 to 65.9% at 24 hours resulted in mean PaO2 88.1 mm Hg (±22.7, CI: 19.8%, P < .005). Overall, mean PF ratio improved from 66.1 pre-HFPV to 180.3 at HFPV initiation (±132.1, CI: 94.7%, P < .05), 181.0 at 2 hours (±139.6, CI: 98.9%, P < .005), and 148.9 at 24 hours (±57.6, CI: 60.9%, P < .0005; Figures 1 and 2).
The overall survival rate was 66.7% (Table 3). Six patients were switched back to CMV and eventually weaned from ventilation completely. Three patients improved on HFPV in respect to oxygenation and converted to CMV but concomitantly received tracheostomies due to failure to liberate from ventilator. Patient 3 with a tracheostomy ultimately developed renal failure, hypotension, and expired due to cardiac arrest. Patient 5 showed significant improvement on HFPV, but unfortunately expired from pulmonary embolism. Patient 7 showed mild improvement on HFPV, converted back to CMV, and failed to wean resulting in expiration. Patient 10 was the only one who did not show improvement on HFPV and expired due to multisystem organ failure from sepsis.
Patient Hospital Course.
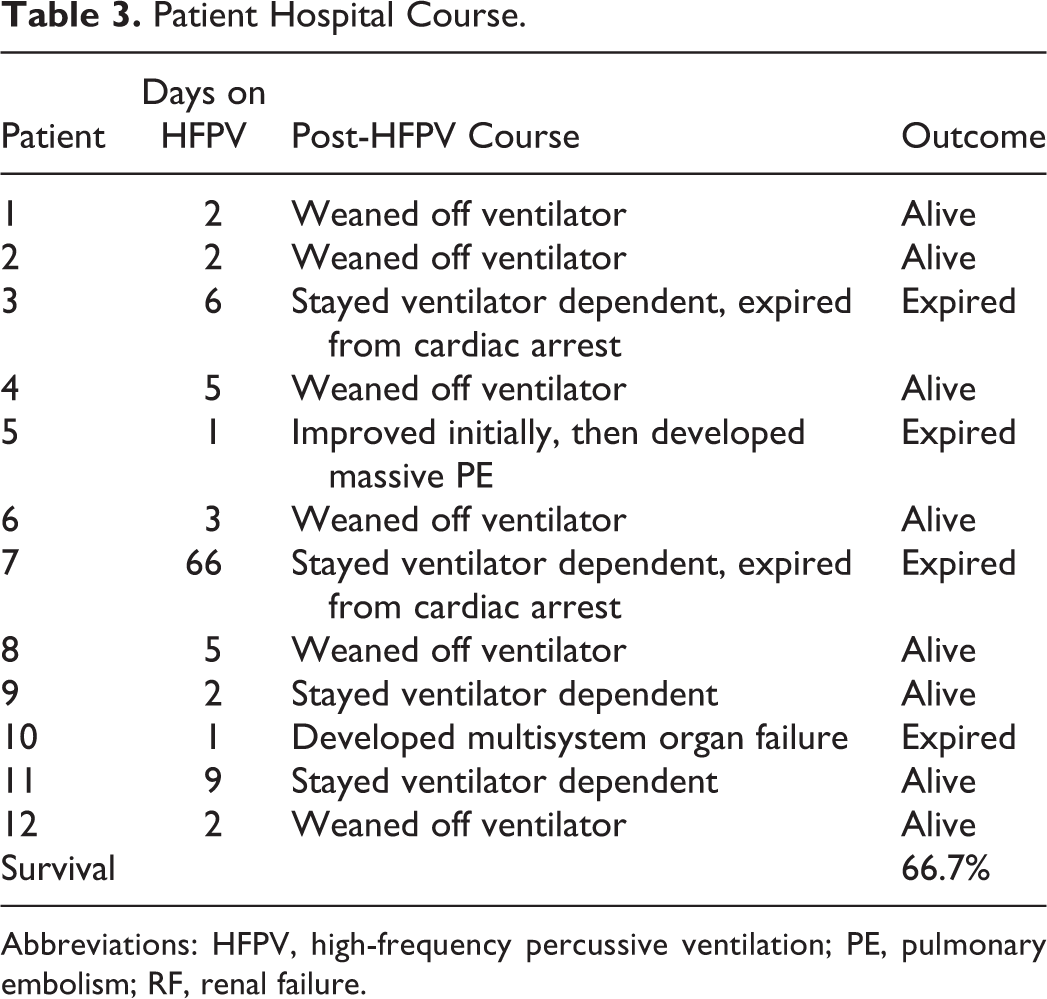
Abbreviations: HFPV, high-frequency percussive ventilation; PE, pulmonary embolism; RF, renal failure.
Discussion
This study is the first descriptive analysis of the applicability of HFPV as a rescue therapy for morbidly obese patients who failed CMV. With the use of HFPV, we noticed significant improvement in PaO2 and PF ratios within 2 hours after conversion from CMV and that maintained for 24 hours in majority of patients. Gradual decrease in PaO2 and PF ratios from HFPV initiation to 24 hours is a result of curbing FiO2 to avoid over oxygenation, not because of continually decreasing respiratory function.
The HFPV was shown to improve gas exchange at lower peak-inflating pressures 16 –18 and low-tidal volume CMV. 16 The mechanism by which HFPV carries out gas exchange is suggested by various theories, including direct bulk flow, longitudinal dispersion of gas molecules at terminal airways and alveoli, Pendelluft air flow between neighboring lung regions thereby increasing dead space ventilation, laminar flow, cardiogenic mixing, and molecular diffusion. 19
There have been limited studies describing the use of HFPV in pediatric, 17,18 trauma, 20 acute respiratory distress syndrome (ARDS), 19 cardiac surgery, 21 and burn patients, 16,22,23 with burn inhalational injury cohort being most commonly described. 22,23 There is even less data supporting the use of HFPV as the standard of rescue therapy in patients who fail CMV. 20,21,24 –26
Other alternative therapies described in morbidly obese patients failing CMV are PP, inhaled nitric oxide, HFOV, jet ventilation, and ECMO. 10,27 –32 Each one of these therapies, including HFPV, can lead to improvement of oxygenation, and each has ardent advocates. None of these modes received widespread acceptance, most likely due to limited high-level evidence supporting improved outcomes. It is also important to realize that improved gas exchange doesn’t necessarily leads to reduction in mortality. The PP maintains a predominant role as a rescue therapy in severe hypoxemia. In the article by De Jong et al, the authors reported on the PP in morbidly obese patients with ARDS in comparison to nonobese group. 27 The study not only demonstrated improvement in gas exchange but also showed significantly lower mortality at 90 days in obese cohort when compared to nonobese group. The HFOV has also been used as a rescue therapy for patients who fail CMV. One randomized controlled trial on patients with ARDS indicated no difference between CMV and HFOV, and another showed increased hospital mortality with HFOV. 33,34 The use of ECMO as a rescue therapy has also grown over the past decade, yet it is still reserved for patients who do not respond to CMV and other alternative rescue methods and techniques.
In conclusion, despite the obvious limitations of the study such as small sample size and retrospective nature of the data collection, this study clearly suggests potential rescue role of HFPV in morbidly obese patients failing CMV, adding to the armamentarium of the clinicians dealing with these challenging patients, thereby obviating the need for ECMO. Future studies are needed to clarify the role of HFPV as a rescue modality in comparison to other rescue modes in morbidly obese patients failing CMV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.