
Abstract
Cancer continues to be a leading cause of death despite a broader understanding of its biology and the development of novel therapies. Nonetheless, with an increasing survival of this population, intensivists must be aware of the associated emergencies, both old and new. Oncologic emergencies can be seen as an initial presentation of the disease or precipitated by its treatment. In this review, we present key oncologic emergencies that may be encountered in daily practice, complications associated with innovative therapies, and treatment-related adverse events.
Keywords
Introduction
Despite the development of numerous and innovative therapies, cancer remains a leading cause of death in the United States and the second leading cause of death globally. In 2015, cancer was responsible for nearly 8.8 million deaths worldwide as per the World Health Organization. In 2017, approximately 1.6 million people were expected to be diagnosed with cancer in the United States alone. 1 Nonetheless, the evolution of cancer care over the past several decades has led to a decline in mortality rates by 1.5% per year, from 1991 to 2015, with a total decrease of 26%, resulting in about 2.4 million fewer deaths. 2
Patients with cancer account for 14% to 22% of all intensive care unit (ICU) admissions. 3,4 Therefore, intensivists must be knowledgeable of the unique emergencies associated with cancer care. Commonly encountered cancer-related emergencies may arise as a result of the underlying cancer, which can be the initial presentation of the disease, occur during the disease course, or can be precipitated during treatment. Many of the most common cancer-related emergencies are highlighted in Table 1. Due to the scope of this review, however, we will focus on the etiology, pathophysiology, and management of selected key oncologic emergencies. These include febrile neutropenia, hyperleukocytosis, tumor lysis syndrome (TLS), cardiac tamponade, and pulmonary hemorrhage as well as unique complications associated with emerging cancer therapies such as chimeric antigen receptor-T (CAR-T)-cell and immunotherapy-related adverse events.
Common Cancer-Related Emergencies.a
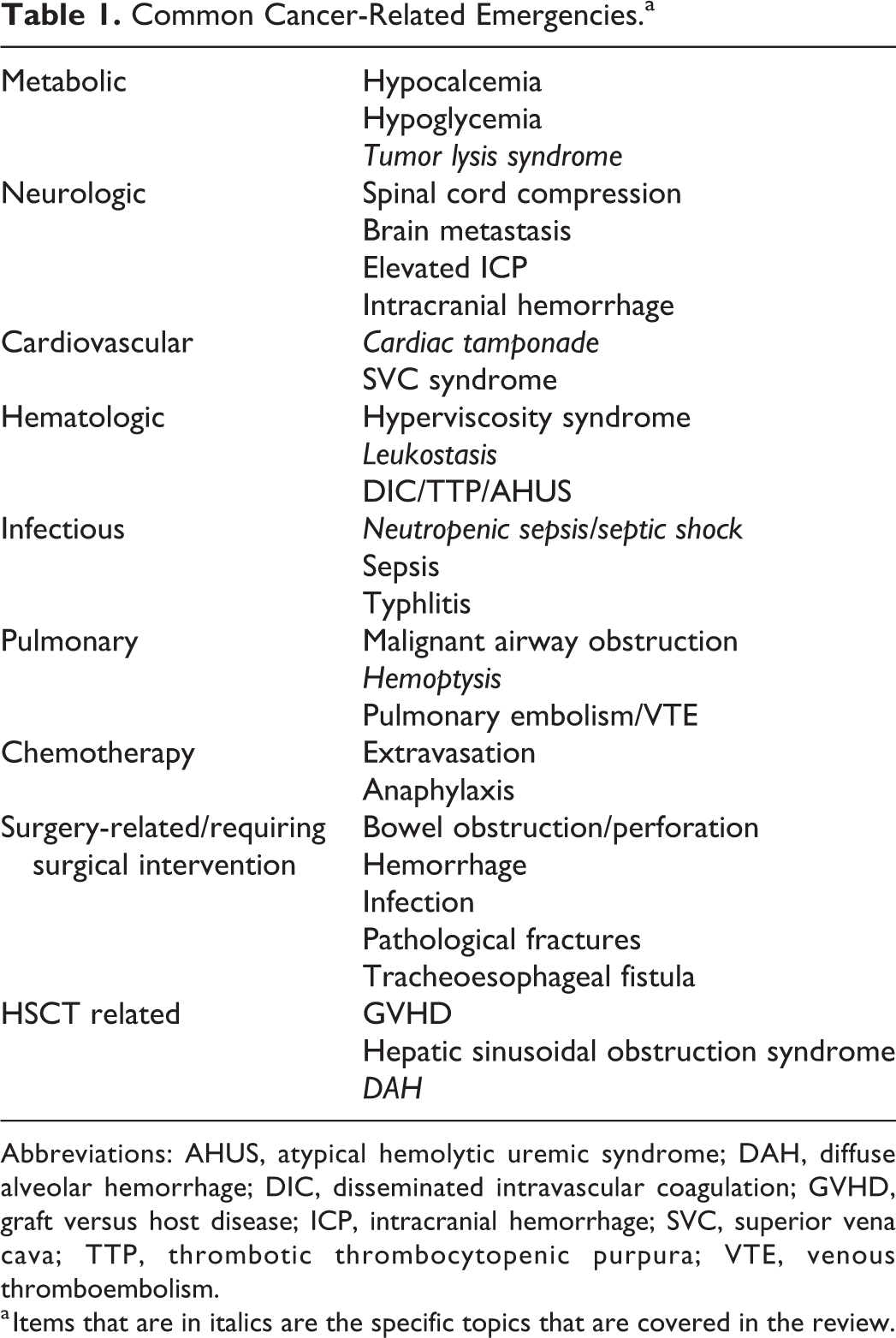
Abbreviations: AHUS, atypical hemolytic uremic syndrome; DAH, diffuse alveolar hemorrhage; DIC, disseminated intravascular coagulation; GVHD, graft versus host disease; ICP, intracranial hemorrhage; SVC, superior vena cava; TTP, thrombotic thrombocytopenic purpura; VTE, venous thromboembolism.
a Items that are in italics are the specific topics that are covered in the review.
White Blood Cells—Too Few or Too Many
Febrile Neutropenia
Neutropenia is defined as an absolute neutrophil count (ANC) of less than 1500/µL, while severe neutropenia is defined as an ANC of <500/µL. 5 Neutropenia can occur due to the adverse effects of cytotoxic chemotherapy, tumor-infiltrating bone marrow, or direct interference with hematopoiesis as seen in some hematologic malignancies. 5 Febrile neutropenia is defined as a single oral temperature of ≥38.3°C (101°F) sustained over a 1-hour period in a neutropenic patient. 6 The major risk factors for neutropenic complications include the rate of ANC decline, recent chemotherapy, current immunosuppression, elevated liver enzymes prior to treatment, reduced glomerular filtration rate, and cardiovascular comorbidities. 7 Cytotoxic drugs that have the highest risk of inducing neutropenia include anthracyclines, taxanes, topoisomerase inhibitors, platinum, gemcitabine, vinorelbine, and certain alkylators such as cyclophosphamide and ifosfamide. 7
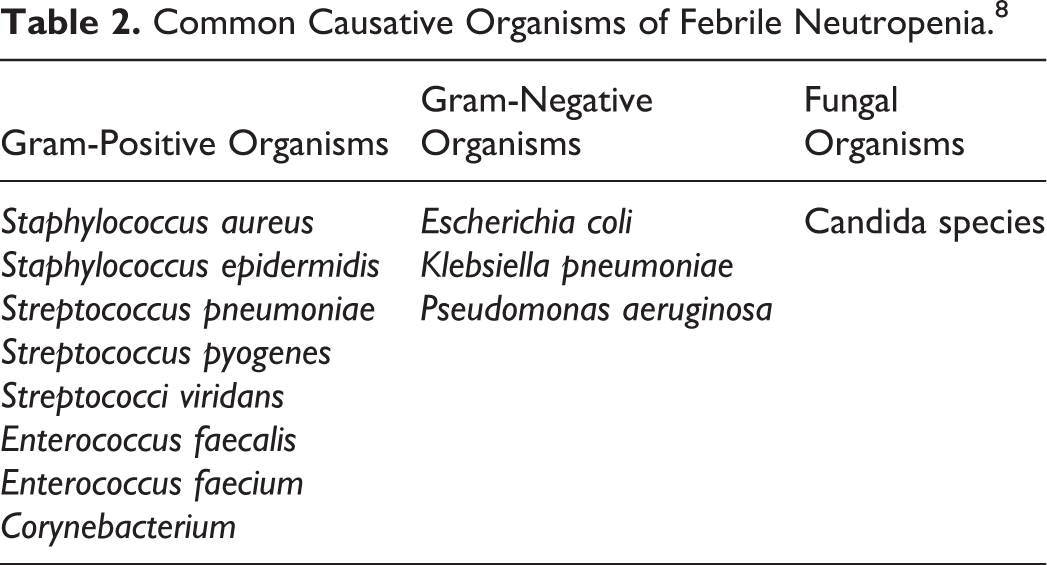
The causative organism is identified only in a minority of patients, and in the rest, it is thought to be due to a variety of organisms. The common causative organisms are listed in Table 2. Patients with febrile neutropenia are at high risk for rapid deterioration; thus, identifying the source of the infection should be aggressively pursued. 3 Common sites of infection in decreasing order include the gastrointestinal tract, blood, skin, lung, and urinary tract. 9 Empiric antibiotic therapy is the mainstay of management and is selected based on clinical status, duration of fever, medical comorbidities, and other factors (Figure 1). Patients with fever >48 hours should be hospitalized for intravenous (IV) antibiotics that should continue until the ANC is >500/µL or depending on the identified source of infection. 6 Addition of an antifungal agent should be considered when fever persists despite 4 to 7 days of broad-spectrum antibiotics without an identified causative organism. 6 When central line-associated bloodstream infection is the confirmed source of infection, the decision to remove the catheter depends on the isolated organism. Recommendations for infections due to Staphylococcus aureus, Pseudomonas aeruginosa, fungi, or mycobacterial species include catheter removal and antibiotic treatment for at least 2 weeks. 7 However, if coagulase-negative Staphylococcus is identified, the catheter can generally remain. 7
Common Causative Organisms of Febrile Neutropenia. 8
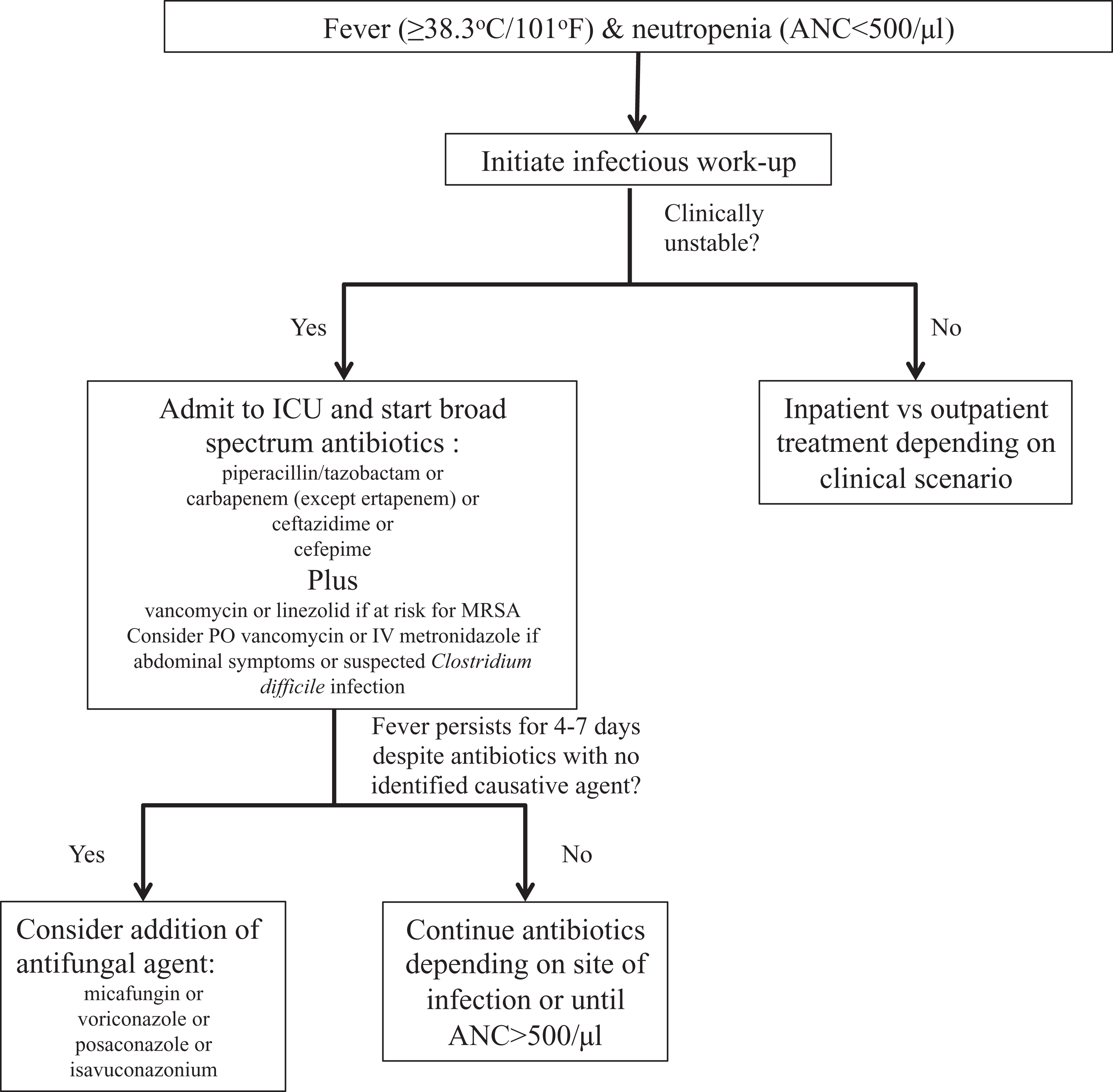
Initial management of febrile neutropenia. 6
The role of granulocyte–colony stimulating factor (G-CSF) is limited once neutropenia occurs and has shown more benefit if given immediately after receipt of chemotherapy. The American Society of Clinical Oncology (ASCO) recommends against the routine use of a CSF unless there is a high risk for infection-associated complications. 10 A course of G-CSF is reasonable until the ANC rises above 1500/µL in high-risk patients who remain febrile after the initiation of antibiotics. High-risk patients include those with expected prolonged (>10 days) or severe neutropenia (<100/µL), age >65 years, pneumonia, sepsis, invasive fungal infection, or hospitalization at the time fever develops. 11
Leukostasis
Leukostasis or symptomatic hyperleukocytosis is an extreme form of leukocytosis that is defined by a white blood cell (WBC) count >100 000/µL. Due to the high quantity, WBCs can clump together, inhibiting efficient microvascular flow leading to end-organ damage with secondary tissue hypoxia and hemorrhage. 12 Patients with hematologic malignancies, most commonly acute myeloid leukemia (AML) and acute lymphoid leukemia (ALL), are at highest risk. However, it can also be seen with chronic myeloid leukemia during blast crisis. 12 The total WBC count is a prognostic factor with commonly accepted cutoffs of 50 000/µL for AML and 400 000/µL for ALL, since blast cells are much larger than lymphocytes. 13
Two possible pathophysiologic mechanisms have been proposed. The first focuses on hyperviscosity that largely depends on cellular deformability and the volume of cell fraction in the blood. Blast cells are less pliable than leukocytes, and thus, the increased cell fraction amplifies the overall viscosity of the blood leading to “sludging” and impaired flow in the microvasculature. 12 An alternative mechanism suggests that endothelial cells are activated by blast cells which secrete inflammatory cytokines leading to an adhesive interaction between them and thus precipitating leukostasis. 12
The diagnosis is made based on the cell counts and peripheral smear along with clinical signs and symptoms of end-organ hypoxemia or hemorrhage. An X-ray or computed tomography (CT) of chest usually shows bilateral interstitial or alveolar infiltrates. Computed tomography or magnetic resonance imaging of the brain may reveal intracranial hemorrhage. 14 Of note, patients with leukostasis are at high risk for concomitant TLS, which is discussed in the next section. 15
Initial management for at-risk patients includes aggressive hydration with calcium- and potassium-free fluids with close monitoring for the development of TLS. Definitive treatment focuses on chemotherapy to decrease tumor load. 15 In cases of very high WBC counts (>200 000 to 300 000/µL) or in symptomatic patients, leukapheresis is the treatment of choice, although there is little evidence on mortality reduction. 16 Leukapheresis is commonly performed through a central venous catheter but can also be done through bilateral antecubital peripheral veins if adequate bore catheters can be placed. A single leukapheresis session can deplete the blood of 20% to 50% of its total WBCs; the remaining blood is then reinfused into the patient. 17 In asymptomatic patients with AML in whom induction chemotherapy cannot be started immediately, cytoreduction with hydroxyurea is suggested. 18 In patients where there is severe anemia, and impending congestive cardiac failure, exchange transfusion may be considered. Partial exchange helps in correcting hyperleukocytosis and severe anemia without increasing the viscosity and fluid overload, which are the main drawbacks of whole blood transfusion and hydration, respectively. 15 Figure 2 depicts a flowchart detailing management strategies in case of leukostasis.
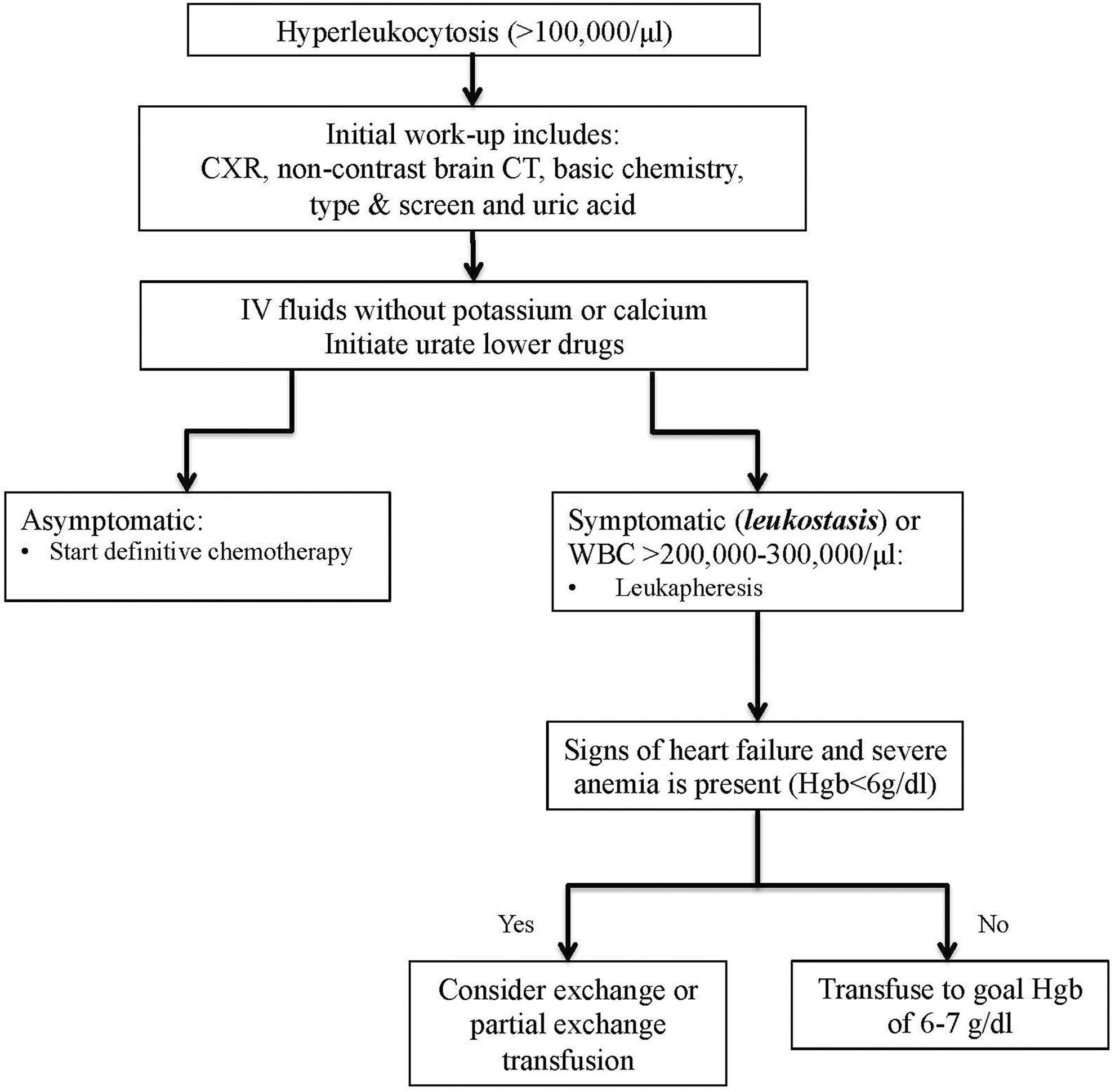
Management of leukostasis.
Too Much Growth
Tumor Lysis Syndrome
Tumor lysis syndrome is a constellation of metabolic abnormalities that occur secondary to the rapid lysis of tumor cells and release of their intracellular contents. It is usually seen upon initiation of cytotoxic chemotherapy but can also occur spontaneously in highly proliferative malignancies due to increased cell turnover. Tumor lysis syndrome is most commonly reported in patients with high-grade non-Hodgkin lymphoma (NHL) and acute leukemias but can also occur during the treatment of large solid tumors (ie, hepatocellular carcinoma, metastatic prostate cancer) that are highly chemosensitive. 19
The pathophysiology is mainly attributed to the release of intracellular components (potassium, phosphate, and uric acid) into the bloodstream. The symptoms of TLS are nonspecific and are largely attributed to the predominant metabolic abnormalities and those related to acute kidney injury (AKI). 20 Hyperkalemia occurs secondary to the release of intracellular potassium during cell lysis. 21 Uric acid is produced by the catabolism of purines by xanthine oxidase. Increased breakdown of nucleic acids produces large amounts of uric acid, which can crystallize in the renal tubules leading to AKI. This is further exacerbated by hyperphosphatemia, which can deposit in the renal tubules as calcium phosphate crystals and thus lead to hypocalcemia. Independent of uric acid precipitation, hyperuricemia by itself can lead to vasoconstriction, decreased renal blood flow, and release of pro-inflammatory mediators due to vascular smooth muscle irritation leading to AKI.
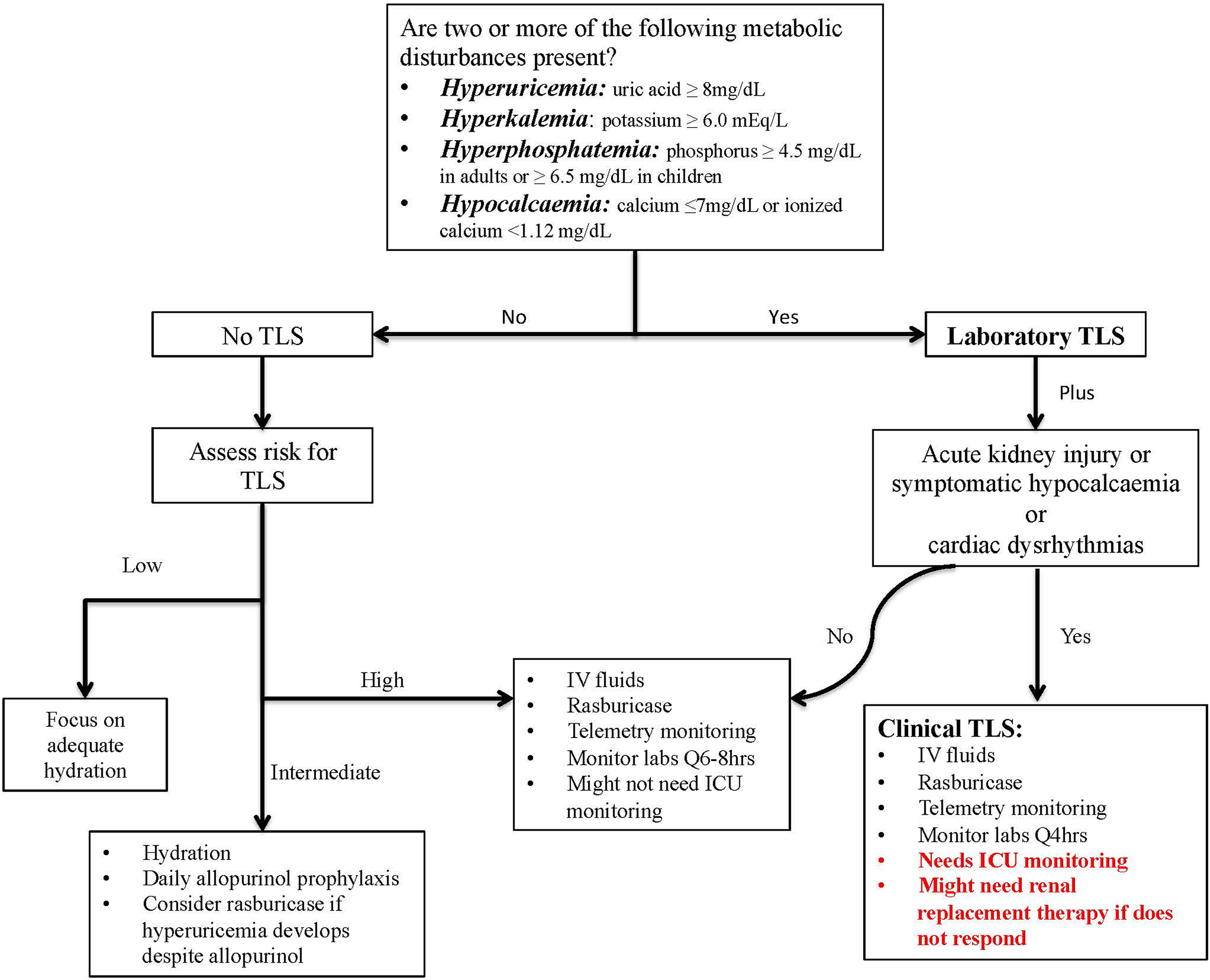
There are both clinical and laboratory criteria for the diagnosis of TLS according to the classification system of Cairo and Bishop. 22 Laboratory TLS is the presence of 2 or more metabolic abnormalities including hyperuricemia, hyperkalemia, hyperphosphatemia, or hypocalcaemia (Figure 3) occurring within 3 days prior to or 7 days after the initiation of treatment assuming that adequate hydration and a hypouricemic agent are given. 22 Clinical TLS is defined as the presence of laboratory TLS along with AKI (increase in creatinine of 0.3 mg/dL from baseline, or when no baseline is available, a single value ≥1.5 times the upper limit of normal for the patient’s age and sex), symptomatic hyperkalemia, or hypocalcemia such as cardiac dysrhythmias, sudden death, tetany, paraesthesia, or seizure. 22 The American Society of Clinical Oncology stratifies patients into high, intermediate, and low risk of developing TLS based on the type of cancer, leukocyte count, and rapidity of proliferation with the expected response to chemotherapy. 23
Management of tumor lysis syndrome.
In each of the risk groups, the coexisting metabolic abnormalities are treated accordingly, and a summary of the ASCO guidelines is shown in Table 3. 23 Management of TLS as outlined in Figure 3 starts with risk stratification and initiation of interventions focused on preventing clinical TLS as it is associated with morbidity and mortality. In patients who are at high risk for TLS or with established TLS, aggressive hydration is provided along with rasburicase for the initial management of hyperuricemia (Figure 3). 23 Rasburicase, a recombinant form of urate oxidase metabolizes insoluble uric acid to allantoin, may be considered if hyperuricemia develops despite allopurinol therapy or as an initial management in pediatric patients. Rasburicase is known to be active ex vivo; as such, blood samples should be sent on ice in order to avoid a falsely normal level in the presence of true hyperuricemia. To decrease the risk of calciphylaxis, it is recommended to use aluminium hydroxide or sevelamer in place of calcium-based phosphate binders. 20
Management of Electrolyte Abnormalities in TLS.
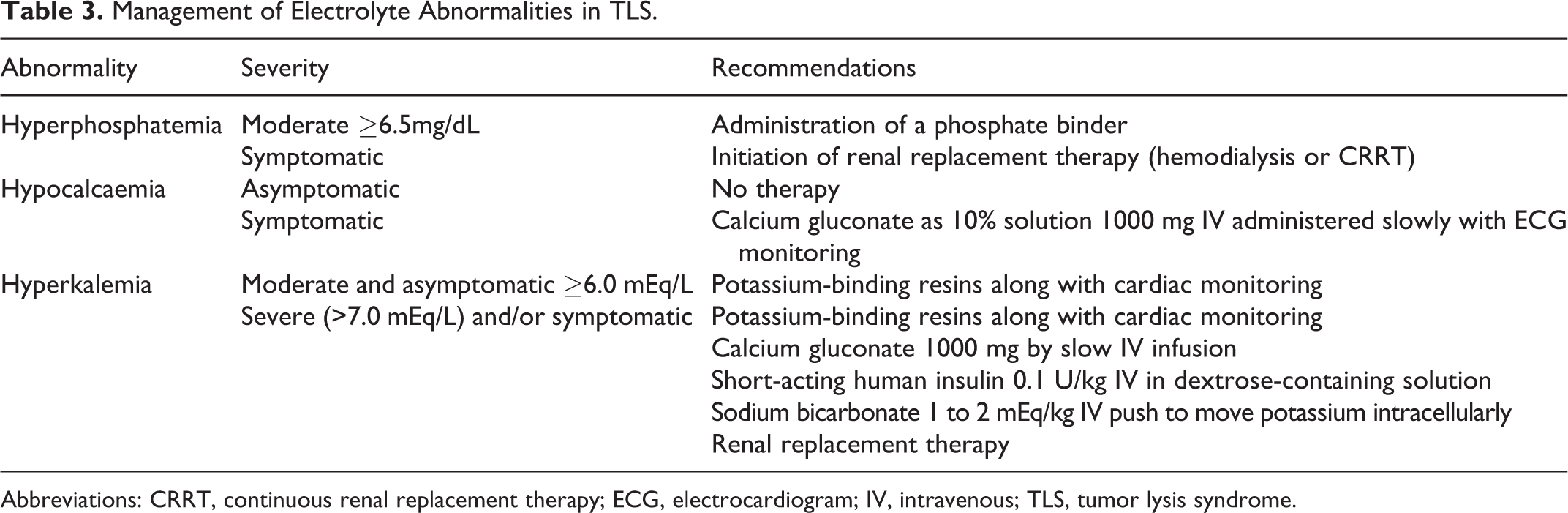
Abbreviations: CRRT, continuous renal replacement therapy; ECG, electrocardiogram; IV, intravenous; TLS, tumor lysis syndrome.
Too Much Fluid in the Wrong Places
Malignant Pericardial Effusion and Cardiac Tamponade
The pericardial sac is easily distensible and can potentially accommodate up to 2 L of fluid if the accumulation occurs slowly. 24 However, tamponade physiology may arise with as little as 100 mL of fluid if the accumulation is acute. 25 As the intrapericardial pressure increases, it prevents the distension of cardiac chambers but to a higher degree on the right ventricle since it is a thin-walled structure. Venous return is thus hampered resulting in compromised filling; diastolic pressures begin to equalize with subsequent reduction in cardiac output resulting in tamponade. The classic presentation of Beck’s triad—hypotension, elevated jugular venous pressure (JVP), and muffled heart sounds—may not be seen when accumulation is gradual, and patients may present with only chest discomfort or dyspnea. 26 Pericardial effusion in patients with cancer is due to metastasis, direct extension of a local tumor, or cancer therapy. Metastatic disease occurs most commonly from noncontiguous breast or lung cancer and melanoma, while primary neoplasms of the pericardium are extremely rare. 27
Diagnosis of pericardial effusion occurs through clinical examination plus either echocardiography or CT scan. 27 Clinical presentation can be nonspecific and includes tachycardia, hypotension, peripheral edema, pulsus paradoxus, elevated JVP, and muffled heart sounds. Chest X-ray (CXR) may show a water bottle appearance of the cardiac silhouette. Electrocardiogram findings can include low voltage and electrical alternans as the heart pendulates within the distended fluid-filled sac. 27 Echocardiography confirms the diagnosis of pericardial effusion and, if present, tamponade physiology. Echocardiographic signs of tamponade physiology include early diastolic right ventricular collapse, late diastolic atrial collapse with a dilated IVC, and no respiratory variation. 28
The mainstay of emergent treatment is pericardiocentesis. This may be performed under ultrasound guidance or via the blind subxiphoid approach, which is more prone to complications. A catheter can also be placed in the pericardial space if recurrence is anticipated. If the effusion is due to lung adenocarcinoma, it is highly likely to recur and a pericardial window or pericardiectomy should be considered. 29 Of the various treatment strategies, prolonged catheter drainage has been shown to have a clear advantage. A systematic review has shown that once a catheter is placed, the rates of reaccumulation are similar with or without the use of sclerosing agents. 30 After drainage, patients should be closely monitored due to the risk of paradoxical hemodynamic instability (PHI). 31 The exact physiology of PHI remains unclear but portends a grave prognosis with risk factors including tamponade, large effusion, and evidence of malignant pericardial process. 32 Pulmonary edema is another uncommon complication but can present immediately after drainage of pericardial fluid. The risk can be minimized by draining the fluid slowly in cases of large pericardial effusion. There are limited data supporting routine diuretics immediately after drainage if hemodynamically tolerated. 33 However, diuresis should be employed in patients who are at high risk for developing pulmonary edema, if hemodynamically feasible.
Pulmonary Hemorrhage
Massive hemoptysis is the expectoration of a large amount of blood due to a rapid rate of bleeding, but the precise volumes remain controversial. Thresholds from 100 mL up to 1000 mL over 24 hours have been proposed, but no single definition is universally accepted. 34 Hemoptysis has multiple causes which are categorized under parenchymal diseases, airway diseases, vascular diseases, coagulation disorders, and miscellaneous (Table 4). In patients with cancer, massive bleeding is generally due to direct infiltration of the tumor cells into the main blood vessels or due to massive tumor necrosis. 35 Additionally, tumors in the lung have abundant and irregular vasculature. Asphyxia due to the flooding of the airways rather than exsanguination is usually the cause of death and is commonly accompanied by cardiovascular collapse. 36
Select Causes of Hemoptysis.
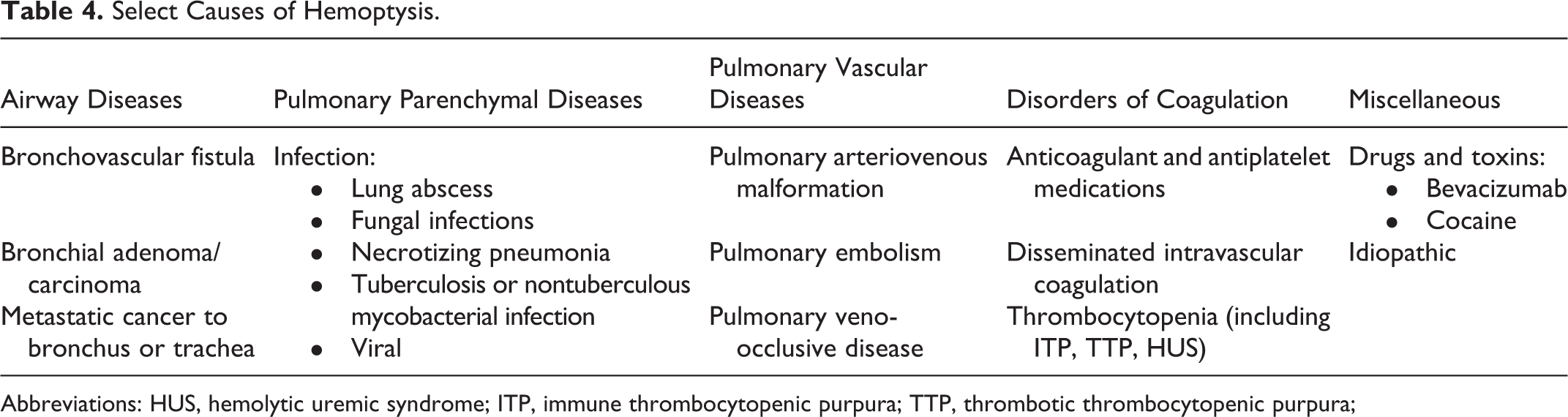
Abbreviations: HUS, hemolytic uremic syndrome; ITP, immune thrombocytopenic purpura; TTP, thrombotic thrombocytopenic purpura;
Patients with hemoptysis should be managed based on the rate and severity of bleeding (massive or nonmassive) and the clinical condition. 36 In addition to maintaining a patent airway and ensuring adequate gas exchange, adequate resuscitation is commonly necessary before any diagnostic investigation. 35 However, occasionally diagnostic bronchoscopy is required in order to temporarily control bleeding, which may include placement of a bronchial blocker, and allow for resuscitation. Ideally, once hemodynamic stability is achieved, patients should be placed in a lateral decubitus position with the bleeding origin in the dependent location. Cough suppression or paralysis can also be used to avoid recurrent bleeding once initial hemostasis is achieved. An initial CXR may help to localize the bleeding site; however, bronchoscopy will provide maximal information if any active bleeding site is detected. 37 Computed tomography angiography may yield additional information regarding the source of active bleeding. 38 Surgical exploration remains the treatment of choice only in selected cases, such as pulmonary artery rupture and other bleeding refractory to nonsurgical therapies. 35 Endovascular embolization has an 85% success in controlling hemoptysis and is considered the most effective and minimally invasive procedure for managing massive and recurrent hemoptysis in almost all other cases. 38 Paraplegia, vascular perforation, and hemorrhage are some of the complications associated with embolization. Early interventional pulmonary involvement is strongly encouraged if expertise is readily available to potentially control bleeding from central or peripheral lesions. This may be achieved with an endobronchial blocker to temporarily occlude and tamponade the culprit bronchus as a supportive measure or until therapeutic intent is achieved. Additionally, central endoluminal lesions can be controlled with topical vasoconstriction, thermal, or direct cautery. 39 Independent predictors of mortality in patients with massive hemoptysis include chronic alcoholism, neoplasm, mechanical ventilation, multilobar infiltrates, and pulmonary vascular involvement. 40
Conversely, diffuse alveolar hemorrhage (DAH) encompasses a variety of disorders in which significant bleeding occurs in the lungs, but not always with overt hemoptysis. Causes of DAH include underlying autoimmune disorders, infection, toxins, drug reactions, coagulopathy, or malignancy. It is characterized by damage to the pulmonary microvasculature. In patients with cancer, it is most commonly seen in hematologic malignancies or after hematopoietic stem cell transplantation (HSCT). Risk factors associated with DAH in HSCT patients include older age, myeloablative conditioning, and severe acute GVHD. 41 It typically presents within the first month following HSCT; however, cases have been described beyond that. The pathophysiology of DAH post HSCT is not clear but is thought to be related to extensive inflammation secondary to uncontrolled cytokine release.
Diffuse alveolar hemorrhage typically presents as dyspnea, nonproductive cough, acute hypoxic respiratory failure with diffuse lung infiltrates, and drop in hemoglobin. The diagnosis is typically made through bronchoscopy demonstrating bloody bronchoalveolar lavage that does not clear with repeated lavages or becomes progressively bloodier. Confirming the diagnosis requires a biopsy where an accumulation of erythrocytes, fibrin, or hemosiderin-laden macrophages can be seen in the alveolar space. 42
Treatment is primarily supportive with correction of any coagulopathies and mechanical ventilation while treating the underlying condition leading to DAH. In addition, since extensive inflammation is thought to be the underlying cause, corticosteroids are commonly utilized. Although dosing is not clear, pulse methylprednisolone (500-2000 mg/d) for the first 5 days followed by prednisone 1 mg/kg/d with gradual tapering has been used. When DAH is suspected to be due to medications or bleeding disorders, anticoagulant reversal or administration of the appropriate blood products is indicated. There are no adequate clinical trials showing efficacy and safety of recombinant factor VIIa use in pulmonary hemorrhage, but it has been used off-label in the pediatric population. 43 Extracorporeal membrane oxygenation remains an option in refractory hypoxic respiratory failure secondary to DAH but is challenging given the need for anticoagulation in the context of active hemorrhage. 44 There is no evidence available for use of antifibrinolytics in DAH currently, although such agents can be considered in extreme cases. Recipients of antifibrinolytics have a higher risk of systemic thromboses if given IV. There are several case reports of inhaled delivery; however, dosing and delivery remain a challenge. 45
Too Much Stress—All Revved Up
Chimeric Antigen Receptor-T-Cell Complications and Toxicity
Chimeric antigen receptor-T cells are a novel therapy that harnesses the immune system to target and kill cancer cells. Normally, when T cells encounter exogenous/foreign antigens, it leads to T-cell proliferation and attack on the antigen-carrying cells to kill them. CAR-T-cell therapy utilizes a patient’s own T cells which are collected and genetically reprogrammed to target and kill cancer cells that express a selected antigen. 46 Currently, CAR-T-cell therapy remains in its early stages with multiple ongoing trials, and notable responses for complete remission are reported to be 70% to 90% in short-term follow-up. 47 In 2017, the Food and Drug Administration (FDA) approved the first CAR-T-cell therapy, tisagenlecleucel (KYMRIAH), for relapsed/refractory B-cell ALL in children and young adults. Soon thereafter, the FDA also approved axicabtagene ciloleucel (YESCARTA) for relapsed/refractory diffuse large B-cell lymphoma. There are several other ongoing trials to evaluate CAR-T-cell efficacy in other malignancies including chronic lymphocytic leukemia, NHL, mesothelioma, ovarian cancer, breast cancer, neuroblastoma, and sarcoma. The FDA has required that hospitals and health-care professionals involved with patients who receive tisagenlecleucel or axicabtagene ciloleucel complete Risk Evaluation and Mitigation Strategies programs. These programs aim to certify providers by requiring training and education regarding the particular side effects and risks of these therapies.
CAR-T-cell therapy is associated with a variety of specific and unique toxicities; the 2 we will highlight are cytokine release syndrome (CRS) and neurotoxicity, either of which may require ICU admission. Several cytokines including interferon γ, tumor necrosis factor α, interleukin-6 (IL-6), IL-10, granulocyte–macrophage CSF, soluble glycoprotein 130, soluble IL-6 receptor, and monocyte chemoattractant protein 1 have been implicated in causing toxicity with significant increase in their respective levels. 48 Patients with high pretreatment disease burden and those who received high doses of CAR-T cells were at increased risk for more severe CRS. 49
Cytokine release syndrome
Patients with CRS initially develop constitutional symptoms, but this syndrome can progress rapidly to multiple organ system dysfunction. It is difficult to differentiate from septic shock and macrophage activation syndrome/hemophagocytic lymphohistiocytosis, which can by itself be a complication of CAR-T-cell therapy. Concomitant antimicrobials are generally employed while awaiting sepsis workup results.
Procalcitonin is a biomarker that has gained popularity in determining presence of bacterial sepsis, but its role in CRS has not been established. Certain biomarkers including rapidly measurable C-reactive protein levels were thought to estimate the severity of the CRS toxicity as it correlated well with IL-6 levels. 48 However, the utility of any specific biomarkers to predict the severity of CRS remains unknown and results should be used as an adjunct to management, which is primarily based on clinical symptomatology.
In addition to understanding the general management principles of CRS, intensivists should also be familiar with the specific CAR-T-cell product being used since each varies in symptoms and severity of CRS, timing of symptoms, and individual reaction to each product. Table 5 lists symptoms and signs in patients with CRS. Treatment of CRS is guided by its toxicity grading as detailed in Table 6. 50 Cytokine release syndrome treatment primarily focuses on supportive ICU care and pharmacologic treatments that may be targeted (tocilizumab) or generalized (corticosteroids). It is not fully clear to what extent immunosuppression interferes with expansion of CAR-T cells, which is necessary for effective tumor control. As such, the goal of pharmacologic treatment is to control life-threatening symptoms.
Signs and Symptoms Associated With CRS.
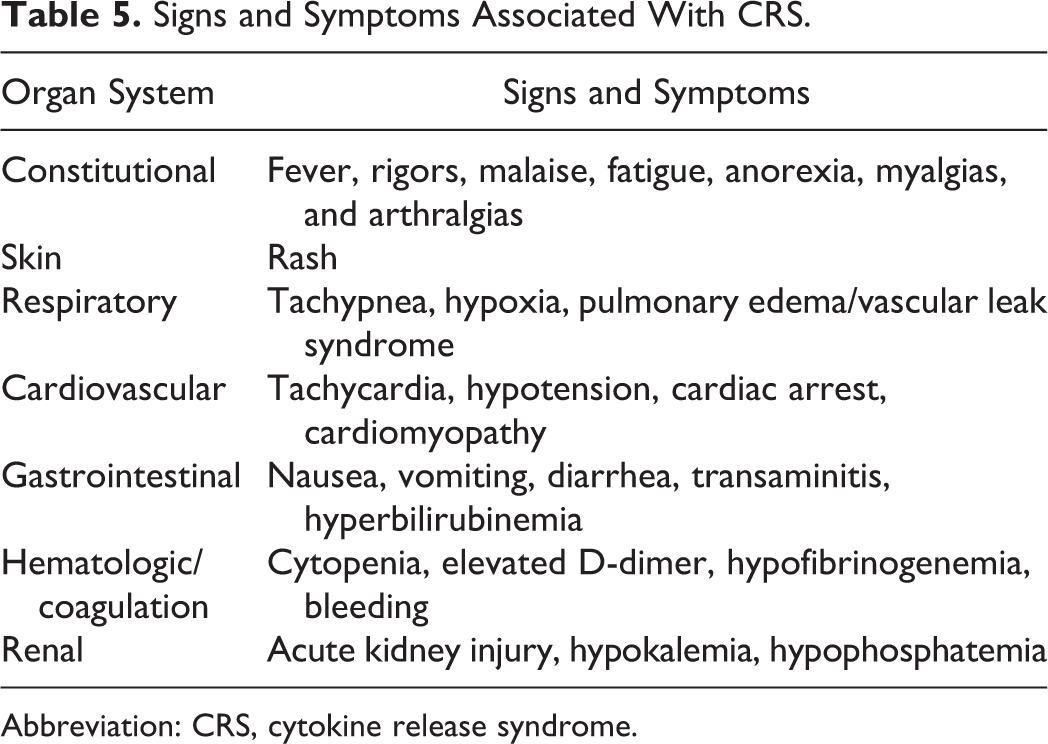
Abbreviation: CRS, cytokine release syndrome.
Grading of CRS.
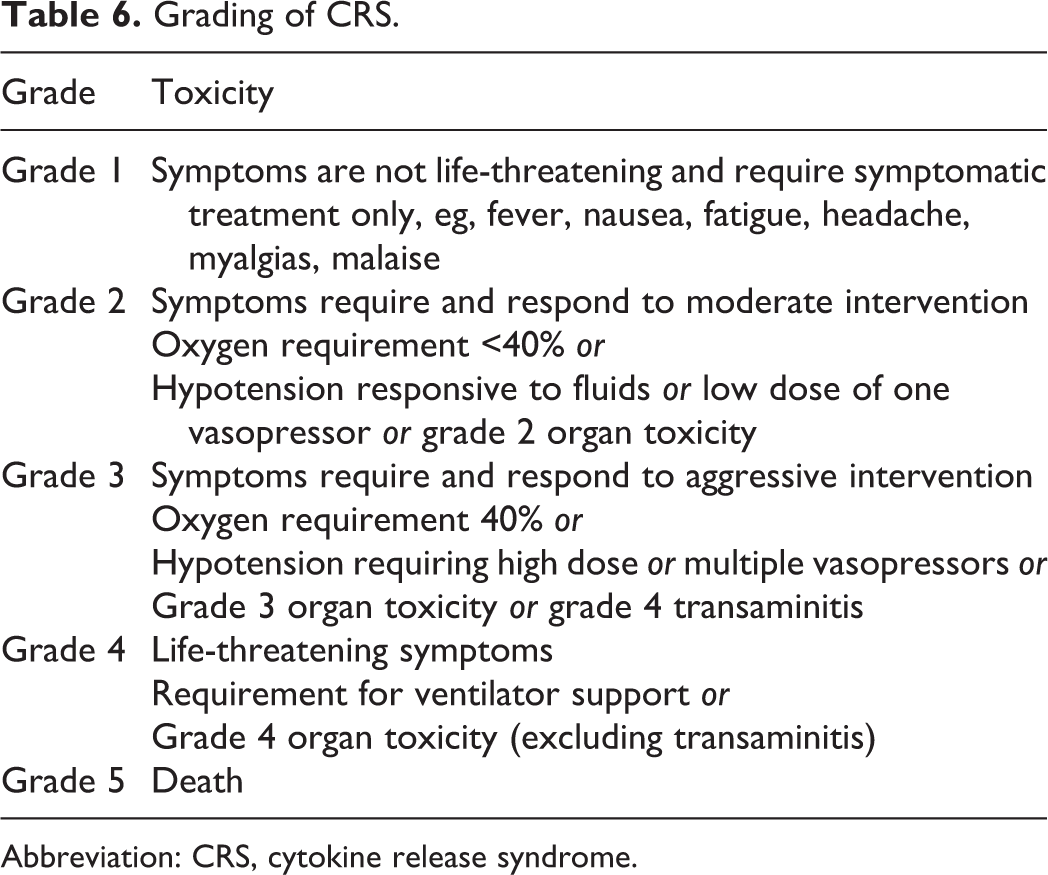
Abbreviation: CRS, cytokine release syndrome.
Tocilizumab is a monoclonal antibody which competitively binds to the IL-6 receptor and thus can mitigate toxicity. Tocilizumab administration in general is employed for grade 3 to grade 4 CRS but is variable depending on the specific CAR-T-cell product given and can be used from grade 1 to grade 4 CRS. A single dose of 8 mg/kg IV is given for patients >30 kg and can be repeated if there is no response within 6 hours. Clinical symptoms and signs are used to initiate tocilizumab as cytokine levels are generally not available immediately. Since tocilizumab is thought to be unlikely to affect T-cell expansion, it is usually used as first-line therapy. Steroids are used as second-line therapy for patients who do not respond or have an inadequate response to tocilizumab as it could alter the effectiveness of the CAR-T cells. 51
Neurotoxicity
The complete pathophysiology of neurotoxicity remains unclear but is thought to be due to vascular instability with increased blood–brain barrier permeability leading to elevated concentrations of cytokines in the CSF. 52 Some of the risk factors associated with neurotoxicity are higher CAR-T-cell dose, severity of disease burden, and lymphodepletion prior to CAR-T-cell therapy. 52 It is thought to be a separate phenomenon with variable and unusual presentations but is almost invariably associated with CRS. 52
Presenting symptoms vary widely from a simple headache to confusion, delirium, hallucinations, aphasia, blinking, staring, tremors or life-threatening seizures, and brain herniation. Management of neurotoxicity includes close vigilance for early development or progression and prompt treatment with corticosteroids, most commonly dexamethasone. There is a suggested association of tocilizumab with worsening neurotoxicity when used for CRS; hence, there is no role for tocilizumab in isolated neurotoxicity currently. The mainstay of treatment involves steroids, generally dexamethasone, with the dose depending on the CAR-T-cell construct and the severity of symptoms. A grading severity scale is currently being developed for neurotoxicity.
Immune Checkpoint Blockade–Related Adverse Events
Immune checkpoint blockade is rapidly becoming a mainstay of cancer treatment both as salvage therapy and as initial therapy, showing a remarkable benefit in the treatment of a wide range of cancer types. 53 Immune checkpoint inhibitors (ICPis) are monoclonal antibodies that liberate the host’s immune response in order to attack cancer cells. This is done by blocking intrinsic downregulators of immunity such as cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death 1 (PD-1) or its ligand PD-L1. 53 As such, these immunotherapies expose patients to a wide array of new immune-related adverse effects (irAEs) that have the potential to affect any organ system and can lead to catastrophic events with prolonged morbidity or in some cases death.
The exact mechanism underlying irAEs is unknown, but it is believed to be related to how these downregulators of immunity (CTLA-4, PD-1, PD-L1) maintain immunologic homeostasis and how that is disrupted by the administration of ICPis. 53 Proposed mechanisms include increasing levels of inflammatory cytokines (similar to CRS), nonspecifically increasing T-cell activity against a variety of antigens, increasing levels of preexisting autoantibodies, and enhanced complement-mediated inflammation. 53
Due to their far-reaching effects, it is difficult to devise a protocol to detect all of the possible irAEs. Instead, the workup is dictated by the organ system involved, for example, if the skin is involved, thorough examination of the skin including the mucosal membranes is essential and a punch biopsy should be performed. Some of the possible presenting signs and symptoms along with suggested diagnostic tests are listed in Table 7. No matter which organ system is involved, it is always important to rule out and empirically treat for possible infections until the workup comes back negative.
Sign, Symptoms, and Workup of Immune-Related Adverse Events.
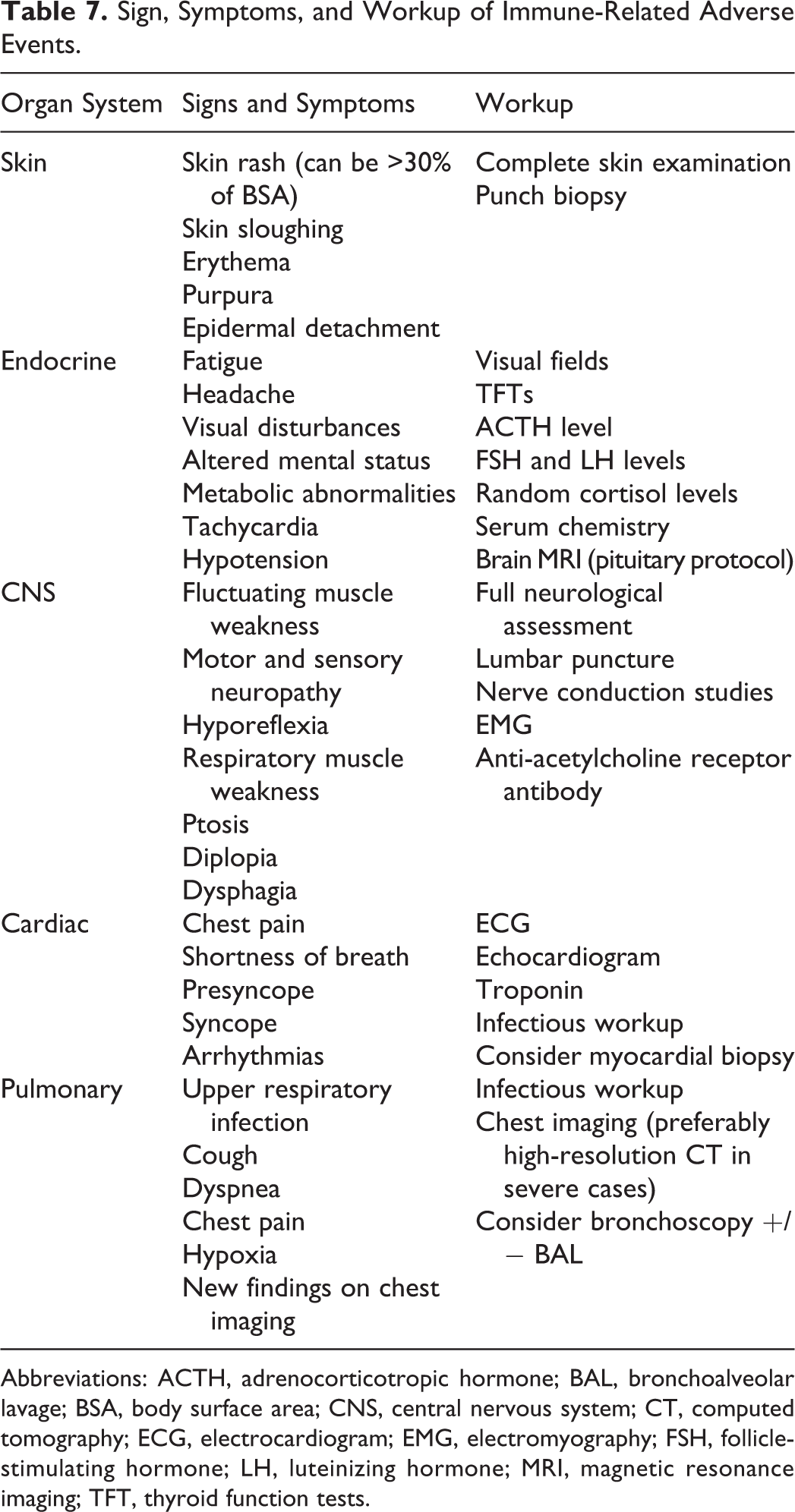
Abbreviations: ACTH, adrenocorticotropic hormone; BAL, bronchoalveolar lavage; BSA, body surface area; CNS, central nervous system; CT, computed tomography; ECG, electrocardiogram; EMG, electromyography; FSH, follicle-stimulating hormone; LH, luteinizing hormone; MRI, magnetic resonance imaging; TFT, thyroid function tests.
As seen in Figure 4, irAEs can affect multiple organ systems. Pertinent critical care manifestations include Stevens-Johnson syndrome, toxic epidermal necrolysis, hypophysitis (most commonly associated with anti-CTLA-4 therapy), 54 multiple hormonal deficiencies related to the function of the anterior pituitary gland, severe hypoadrenalism with severe electrolyte abnormalities, 55 myasthenia gravis, Guillain-Barré syndrome leading to respiratory failure, 56 arrhythmias (including third-degree atrioventricular block), and cardiomyopathies which are associated with high morbidity and mortality if treatment is not initiated early. 57 Immune-related pneumonitis has also been reported and can lead to hypoxic respiratory failure and acute respiratory distress syndrome. 55
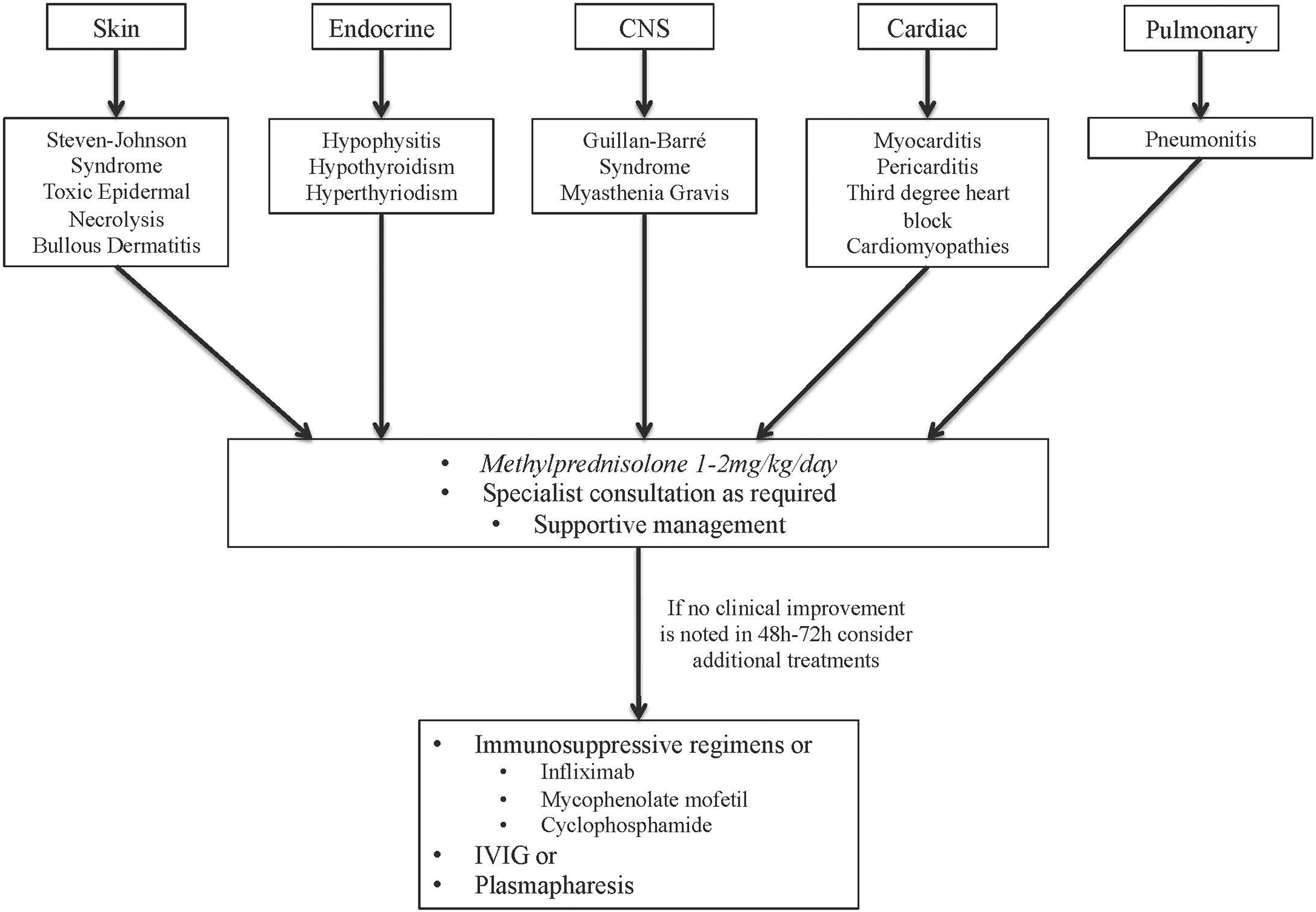
Immune-related adverse events caused by immune checkpoint inhibitors.
In addition to discontinuing the offending agent, the mainstay of treatment for all irAEs is high-dose steroids with consideration of additional immunosuppressive agents such as infliximab, mycophenolate mofetil, cyclophosphamide, IV immunoglobulin, or plasmapheresis in cases refractory to steroids. 55 Figure 4 highlights some of the more catastrophic irAEs and their management. Recent evidence suggests that there is no difference in clinical outcomes between patients who require treatment for irAEs and those who do not. 53 Additionally, retrospective data suggest that irAEs associated with one class of inhibitor may not necessarily occur during subsequent treatment with another agent.
Conclusion
Despite overall improved cancer care, classic oncologic emergencies continue to occur and many require ICU management. Cancer therapies have evolved with more focused tumor targeting; however, complications and side effects are not necessarily limited and unique emergencies have been identified. Although overall survival from cancer has improved, patients are commonly admitted to the ICU at some point during their clinical course. Therefore, it is crucial for intensivists to have a working knowledge of the common oncologic emergencies and novel therapy–related complications as they are more likely to be seen in everyday critical care practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Anesthesiology & Critical Care Medicine, MSK Cancer Center Support Grant/Core Grant (P30 CA008748).