
Abstract
Purpose:
To study the effect of hypoalbuminemia on short- and long-term mortality in Cardiac Intensive Care Unit (CICU) patients.
Methods:
We reviewed 12,418 unique CICU patients from 2007 to 2018. Hypoalbuminemia was defined as an admission albumin level <3.5 g/dL. Predictors of hospital mortality were identified using multivariable logistic regression.
Results:
We included 2,680 patients (22%) with a measured admission albumin level. The median age was 68 (39% females). Admission diagnoses included acute coronary syndrome, heart failure, cardiac arrest, and cardiogenic shock. The median albumin level was 3.4 g/dL and 55% of patients had hypoalbuminemia. Hospital mortality occurred in 16%, and patients with hypoalbuminemia had higher hospital mortality (21% vs. 9%, adjusted OR 2.64, 95% CI 2.09-3.34, p < 0.001). Albumin level was inversely associated with hospital mortality (adjusted OR 0.60 per 1 g/dL higher albumin level, 95% CI 0.47-0.75, p <0.001), with a stepwise increase in the hospital mortality at lower albumin levels. Post-discharge mortality was higher in hospital survivors with hypoalbuminemia, and increased as a function of lower albumin levels.
Conclusion:
Hypoalbuminemia is common in CICU patients and associated with higher short- and long-term mortality. Progressively lower serum albumin was incrementally associated with higher hospital and post-discharge mortality.
Introduction
Hypoalbuminemia is common among acutely-ill patients with a prevalence of 21-70% in hospitalized individuals. 1 –3 Albumin is the most abundant protein in the plasma and is a major transporter of a multitude of compounds in blood. 4 As a negative acute-phase reactant, the synthesis of albumin can be influenced by numerous acute and chronic disease processes, allowing serum albumin levels to provide prognostic insights into the effects of illness on protein metabolism. Hypoalbuminemia can be observed in acute illness as a result of increased capillary leak or decreased synthesis due to inflammation, underlying malnutrition, or hepatic synthetic dysfunction. 5 Furthermore, a low albumin level has been proposed as a potential biomarker of frailty, which itself is associated with worse outcomes in hospitalized and critically ill patients. 6,7
Hypoalbuminemia has been consistently associated with a higher risk of mortality across various populations of acutely ill patients. Among patients admitted for septic shock, those with hypoalbuminemia have a higher risk of mortality. 5,6 Similar findings have been observed in other critically ill populations, including those with kidney dysfunction, cerebrovascular events, and malignancy. 3,4,8 –11 Likewise, hypoalbuminemia has been associated with reduced survival in patients with cardiovascular disease, including acute and chronic heart failure (HF) and acute coronary syndromes (ACS). 12 –16 In patients with ACS, hypoalbuminemia has been associated with higher in-hospital and post-discharge mortality. 4,17 Further, hypoalbuminemia has been shown to be associated with increased risk of HF, in the setting of a prior myocardial infarction. 18
The contemporary cardiac intensive care unit (CICU) has evolved to include a heterogeneous mix of patients with acute and chronic cardiac disease and extensive non-cardiac comorbidities. 19 In this complex CICU care environment, it would be useful to identify readily-available biomarkers that can predict outcomes, and serum albumin has the potential to fill this need. No studies to date have examined the association between serum albumin or hypoalbuminemia and mortality in CICU patients. To bridge this knowledge gap, we hypothesized that hypoalbuminemia and the serum albumin level would predict hospital and post-discharge mortality in a CICU population.
Methods
Study Population
This study was approved by the Institutional Review Board of Mayo Clinic as posing minimal risk to patients and was conducted under a waiver of informed consent (IRB # 16-000722). We retrospectively analyzed a database of consecutive unique adult (aged ≥18 years) patients admitted to the CICU at Mayo Clinic Hospital St. Mary’s Campus whose entire CICU admission occurred between January 1, 2007 and April 30, 2018, and included only those patients with an available admission albumin level. 19 We only analyzed data from the first CICU admission during the study period to avoid mortality bias associated with CICU readmissions. According to Minnesota state law statute 144.295, patients must provide authorization in order to be included in observational research studies; patients who did not have Minnesota Research Authorization were excluded from the database.
Data Sources
Demographic, vital signs, laboratory, and other clinical outcome data were extracted electronically from the medical record, including procedures and therapies performed during the CICU and hospital stay. The admission values of all vital signs, clinical measurements, and laboratory values were used, defined as either the first value recorded after CICU admission or the value recorded closest to CICU admission. Hypoalbuminemia was defined as an admission albumin level < 3.5 g/dL, based on the accepted normal range for serum albumin. 1 The Acute Physiology and Chronic Health Evaluation (APACHE)-III score, APACHE-IV predicted hospital mortality, and Day 1 Sequential Organ Failure Assessment (SOFA) score were calculated for all patients using data from the first 24 hours of CICU admission, with missing variables imputed as normal; the mean and maximum values of all daily SOFA scores while the patient remained in the CICU were recorded. 20 –24 The Charlson Comorbidity Index (CCI) and individual comorbidities were determined based on a previously validated electronic algorithm. 25 Admission diagnoses were defined as all International Classification of Diseases (ICD)-9 and ICD-10 diagnosis codes recorded on the day of CICU admission plus 1 day before or after; these diagnoses were not mutually exclusive, and the primary discharge diagnosis could not be determined.
Statistical Analysis
The primary outcome was all-cause hospital mortality, and the secondary outcomes were CICU and 1-year post-discharge mortality, which was determined based on the electronic review of the medical record. Data are reported as number (%) for categorical variables and median (interquartile range [IQR]) for continuous variables. Groups were compared using the Wilcoxon test for continuous variables and Pearson chi-square test for categorical variables. Correlations between continuous variables were assessed using Pearson r coefficients from linear regression. Logistic regression was used to calculate the unadjusted odds ratio (OR) and 95% confidence interval (CI) values for hospital mortality. The optimal cut-off for albumin level as a predictor of hospital mortality was determined from the receiver-operator characteristic curve based on the highest value of Youden’s J index (sensitivity + specificity − 1). Multivariable analysis was performed to determine adjusted OR values for hospital mortality using stepwise forward variable selection (p < 0.25 to enter, p > 0.1 to leave the model) followed by logistic regression, with candidate variables including demographics, comorbidities, illness severity, and CICU therapies and complications; only variables present in > 75% of patients were included as candidate variables. Kaplan-Meier survival analysis was used to compare 1-year post-discharge survival among patients surviving to hospital discharge (hospital survivors), with groups compared using the log-rank test. Cox proportional-hazards analysis was used to determine whether predictors of hospital mortality were associated with post-discharge mortality up to 1 year among hospital survivors. Two-tailed P values < 0.05 were considered statistically significant. Statistical analyses were performed using JMP version 13.0 Pro (SAS Institute, Cary, NC).
Results
Study Population and Baseline Characteristics
Among the 15,947 adult patients admitted to the CICU over the study period, 3,529 were excluded (2,472 readmissions, 1,047 without Minnesota Research Authorization, 10 without available ICD-9/10 diagnosis codes), leaving 12,418 unique CICU patients eligible for inclusion (Supplemental Figure 1). Admission albumin levels were available in 2,680 (21.6%) patients who comprised the final study population and the remaining 9,738 (78.4%) patients were excluded (Supplemental Figure 1); included patients with a measured albumin level differed substantially from excluded patients without a measured albumin level, with higher illness severity, more comorbidities, and worse outcomes (Supplemental Table 1). The median age of the final study population was 68 (IQR 57, 78), 1,031 (39%) patients were females, and 2,412 (90%) patients were White. The baseline characteristics of the study population are shown in Table 1. The median albumin level was 3.4 (IQR 2.9, 3.8) g/dL.
Baseline Characteristics of Overall Study Population Including Patients With Hypoalbuminemia (≤3.5 g/dL) and Normal Albumin Levels (>3.5 g/dL).
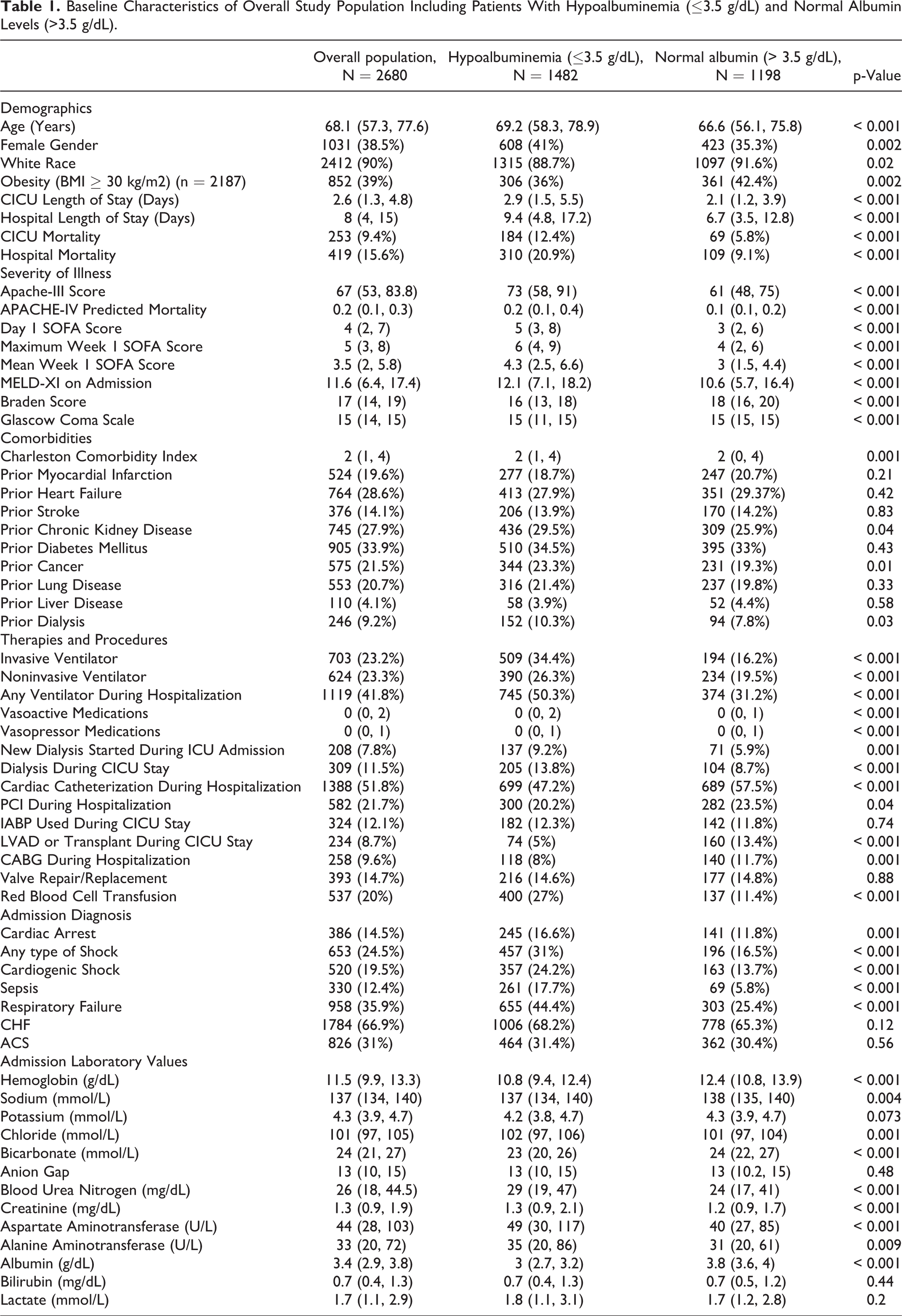
Hypoalbuminemia (admission albumin level < 3.5 g/dL) was present in 1,482 (55%) patients. Patients with hypoalbuminemia differed substantially from patients without hypoalbuminemia (Table 1), with older age, greater prevalence of non-White race, more comorbidities, greater illness severity, more vital sign and laboratory abnormalities, more critical care diagnoses and greater need for critical care therapies (all p < 0.01). Patients with and without ACS or HF had a similar prevalence of hypoalbuminemia (p > 0.1), although patients with concomitant ACS and HF had a higher prevalence of hypoalbuminemia (64%). Among the 81.6% of patients with available data for BMI, 39% were classified as obese (BMI ≥ 30 kg/m2). Patients with hypoalbuminemia were less likely to be obese (36.0% vs 42.4%, p = 0.002). Admission albumin levels were directly correlated with admission Braden skin score (r = 0.36) and admission hemoglobin (r = 0.33), and inversely correlated with APACHE-III/IV (r = 0.31-0.32) and Day 1 SOFA scores (r = 0.32); all p < 0.001. Weaker (r ≥ 0.1) but significant (p < 0.01) inverse correlations were observed between admission albumin levels and CCI, transaminases, bilirubin, BUN and creatinine.
Hospital Mortality
A total of 419 (16%) patients died in the hospital, including 253 (9%) who died during the CICU stay. Patients who died during hospitalization had lower median admission albumin levels (3.0 vs. 3.4 g/dL, p < 0.001). Patients with hypoalbuminemia had higher CICU (12% vs. 6%, unadjusted OR 2.32, 95% CI 1.74-3.09, p < 0.001) and hospital (21% vs. 9%, unadjusted OR 2.64, 95% CI 2.09-3.34, p < 0.001) mortality. A higher admission albumin level was associated with lower hospital mortality (unadjusted OR 0.36 per 1 g/dL, 95% CI 0.30-0.43, p < 0.001). Admission albumin had an AUC value of 0.67 with an optimal cut-off of 3.1 g/dL for discrimination of hospital mortality. Hospital mortality increased progressively with declining albumin level (Figure 1), without a clear inflection point. Similar findings were observed in patients with an admission diagnosis of ACS or HF (Figure 1), although the association between albumin and hospital mortality appeared stronger in ACS patients (unadjusted OR 0.29 per 1 g/dL, 95% CI 0.21-0.41, p < 0.001) than in HF patients (unadjusted OR 0.42 per 1 g/dL, 95% CI 0.34-0.53, p < 0.001). Notably, ACS patients with hypoalbuminemia were less likely to receive coronary angiography, PCI, or CABG (all p < 0.001). A similar optimal albumin cut-off for predicting hospital mortality of 3.1 g/dL was found in patients with and without cardiogenic shock or cardiac arrest, and for patients with pulmonary hypertension. Hypoalbuminemia and low albumin levels were associated with unadjusted hospital mortality risk in both obese and non-obese patients, but the OR effect size was greater in non-obese patients.
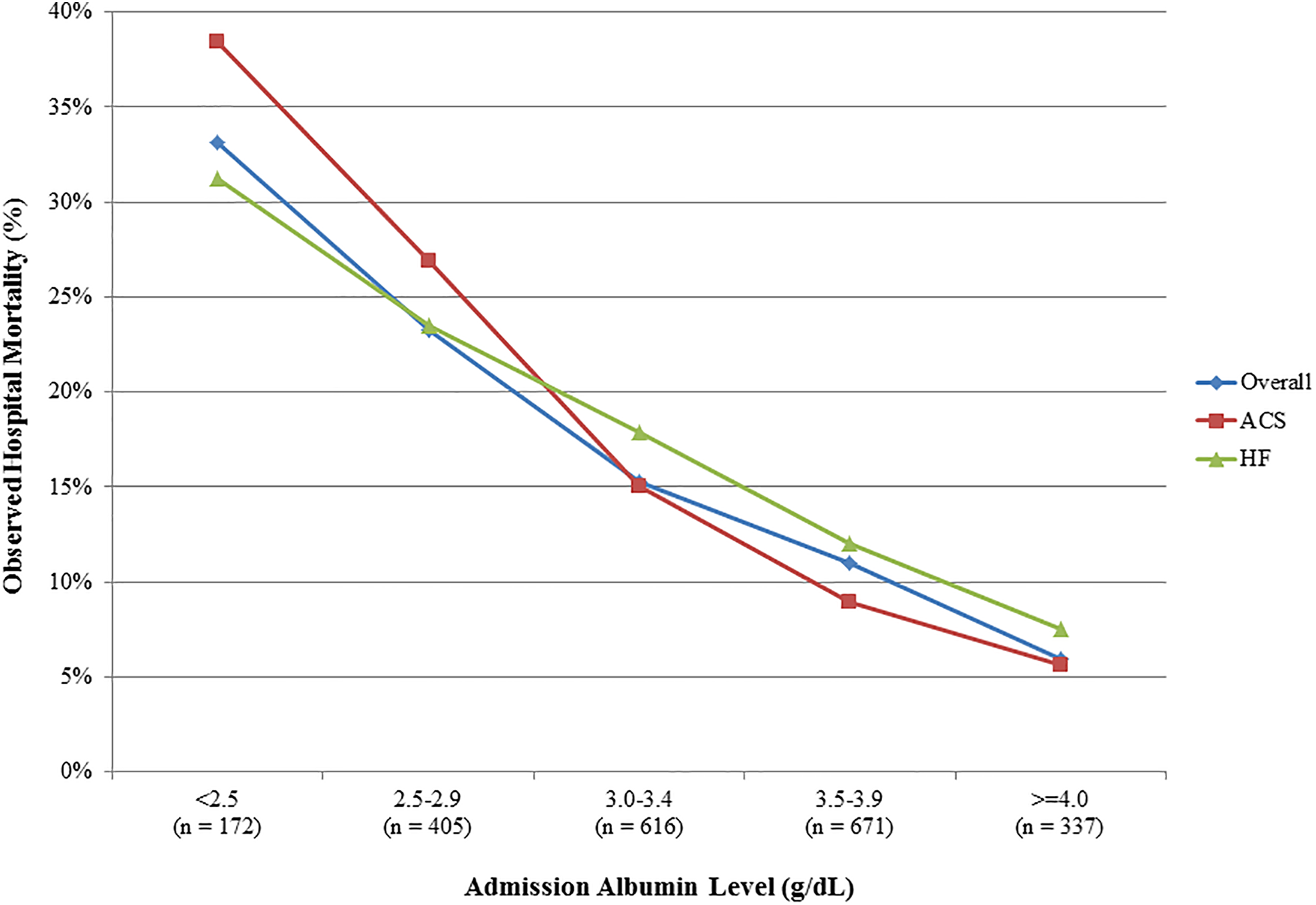
Hospital mortality stratified by albumin levels in the overall study population and patients with ACS and HF.
After multivariable adjustment (Table 2), admission albumin level remained inversely associated with hospital mortality (adjusted OR 0.60 per 1 g/dL, 95% CI 0.47-0.75, p < 0.001). After a similar adjustment, hypoalbuminemia remained associated with higher hospital mortality (adjusted OR 1.52, 95% CI 1.14-2.04, p = 0.002). Before and after multivariable adjustment, a stepwise increase in the risk of hospital mortality with decreasing albumin levels were observed compared with an albumin level ≥ 4 g/dL, particularly for admission albumin levels < 3.0 g/dL (Figure 2). After multivariable adjustment, higher albumin levels were associated with lower hospital mortality in non-obese patients (adjusted OR 0.50, 95% CI 0.36-0.70, p < 0.001), but not obese patients (adjusted OR 0.78, 95% CI 0.51 -1.19, p = 0.25).
Predictors of Hospital Mortality on Multivariable Regression.a
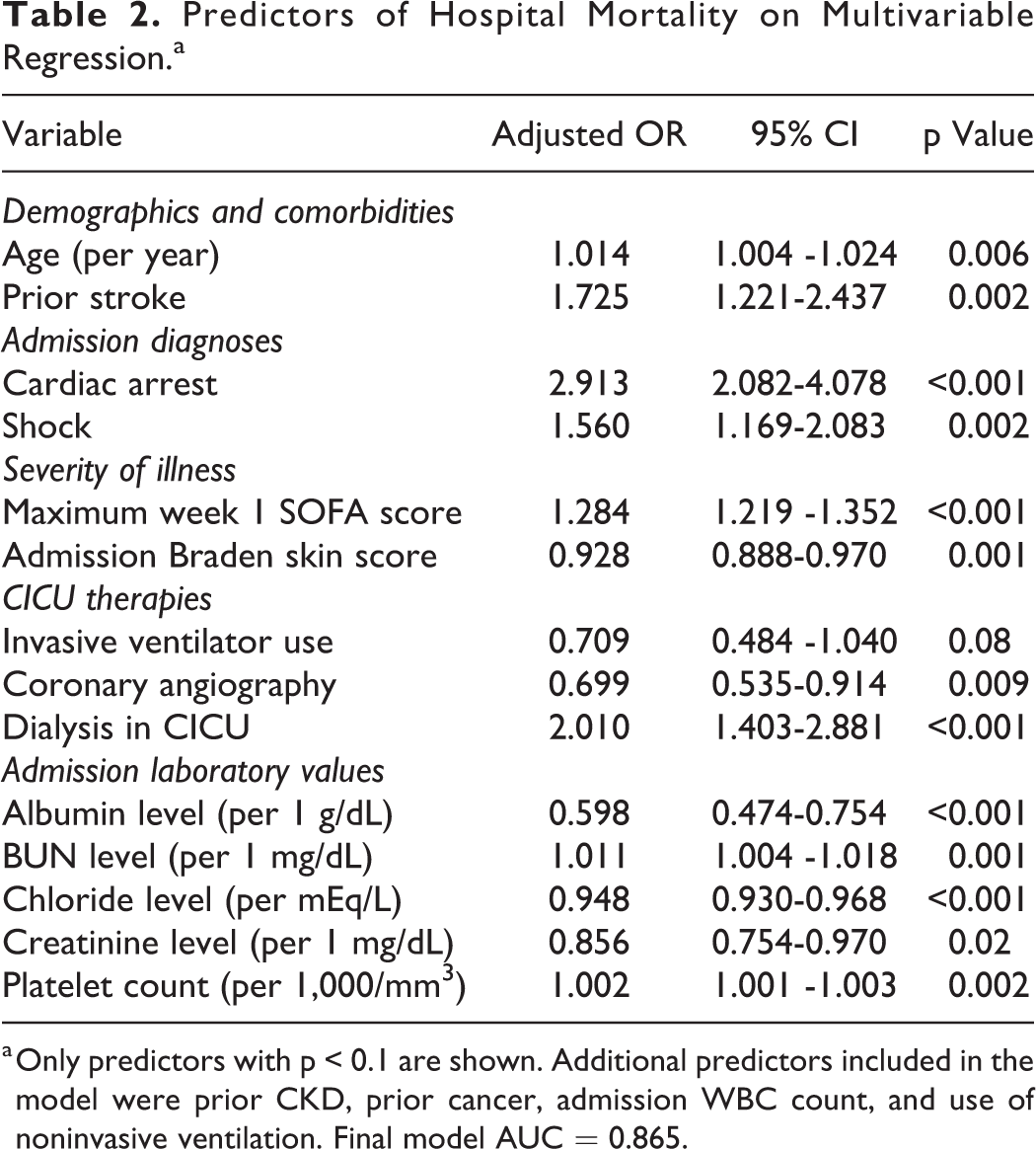
a Only predictors with p < 0.1 are shown. Additional predictors included in the model were prior CKD, prior cancer, admission WBC count, and use of noninvasive ventilation. Final model AUC = 0.865.
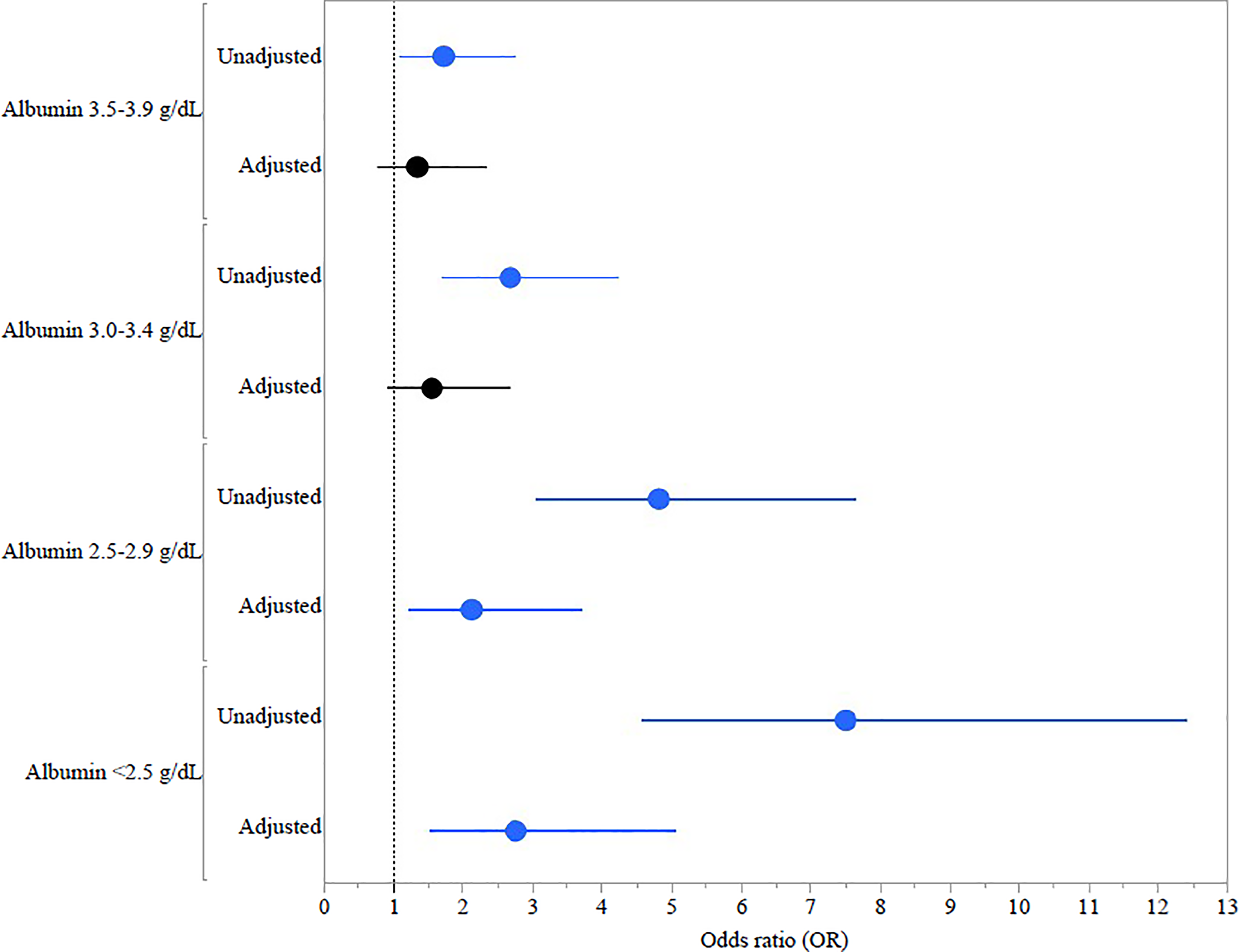
Multivariate analysis demonstrating adjusted and unadjusted odds ratio of hospital mortality stratified by albumin levels.
Post-Discharge Survival
During 1 year of follow-up, a total of 538 (24%) hospital survivors died and 278 (12%) were lost to follow-up at 1-year. Overall Kaplan-Meier 1-year survival was lower for patients with a measured albumin level than for patients without a measured albumin level (62.1% vs. 79.5%, p < 0.001 by log-rank; Supplemental Figure 2). Hospital survivors with hypoalbuminemia had lower 1-year survival by Kaplan-Meier analysis (Figure 3A; p < 0.001 by log-rank). A stepwise decrease in 1-year survival was observed as a function of decreasing albumin level by Kaplan-Meier analysis in hospital survivors (Figure 3B, p < 0.001 by log-rank), as in the overall population (Supplemental Figure 3). Hospital survivors with admission hypoalbuminemia were at increased risk of post-discharge mortality on Cox proportional-hazards analysis (adjusted HR 1.71, 95% CI 1.41-2.08, p < 0.001). A higher admission albumin level was associated with lower post-discharge mortality among hospital survivors on Cox proportional-hazards analysis (adjusted HR 0.56 per 1 g/dL, 95% CI 0.47-0.66, p < 0.001).
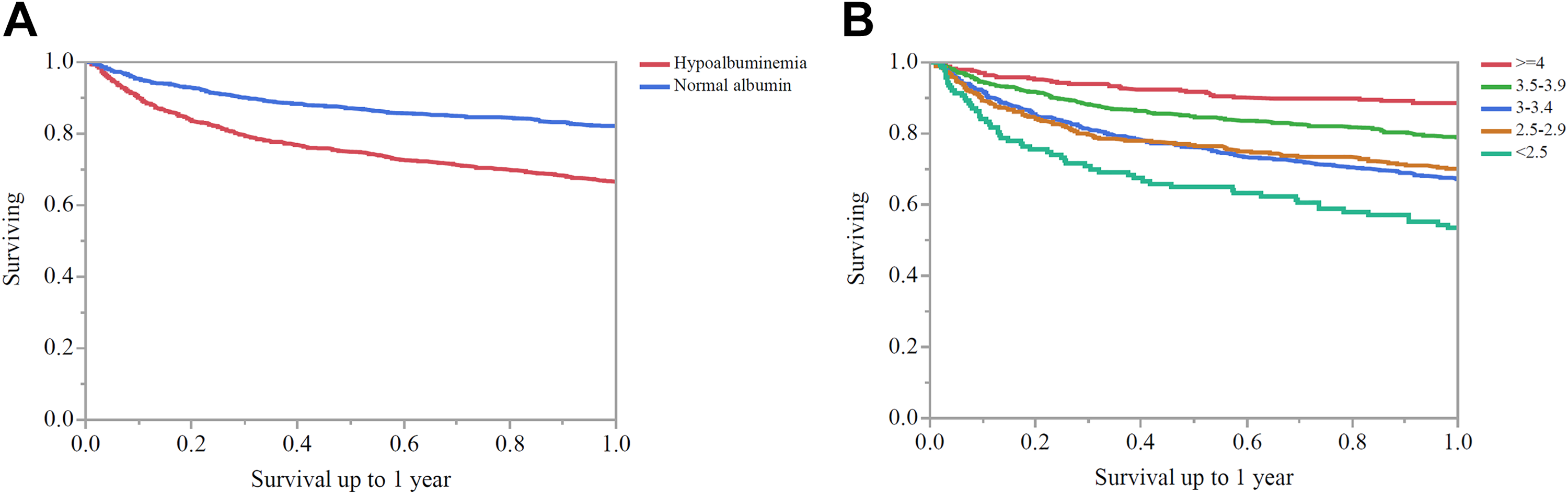
Kaplan-Meier curve demonstrating 1-year survival in patients with normal albumin compared to hypoalbuminemia. P < 0.001 by log-rank. Figure 3B. Kaplan-Meier curve demonstrating 1-year survival in patients stratified by serum albumin level. P < 0.001 by log-rank.
Discussion
The findings of this study exemplify the importance of a biomarker-based prediction of outcome using albumin levels in the critically ill population specific to the CICU. Hypoalbuminemia identifies patients that have higher illness severity, more comorbidities, greater acute critical care needs, and have higher mortality in the hospital and post-discharge setting. This study illustrates that hypoalbuminemia can be used as a prognostic factor in patients admitted to the CICU, including those patients surviving hospitalization. Low albumin levels remained associated with higher short-term and long-term mortality even after adjusting for established prognostic variables, emphasizing the independent association of hypoalbuminemia with adverse outcomes. This study adds to our prior work emphasizing the important prognostic value of commonly-obtained laboratory tests and simple bedside assessment in CICU patients, creating a foundation for biomarker-based risk assessment in CICU patients. 19,26,27
To our knowledge, this is the first large study to examine the association between hypoalbuminemia with hospital and post-discharge mortality in unselected CICU patients, although multiple studies have identified hypoalbuminemia as a predictor of mortality and morbidity in other ICU populations. 1 –3,5,6,28 Patients in a medical ICU, including septic shock patients, with hypoalbuminemia (albumin < 3.5 g/dL) were found to have higher APACHE and SOFA scores and increased 30-day all-cause mortality. 29,30 Indeed, albumin is included in the APACHE-III/IV scoring systems for prediction of hospital mortality in critically-ill patients, although only severe hypoalbuminemia (albumin level < 2.5 g/dL) contributes to risk prediction. 31
Hypoalbuminemia is an independent risk factor for adverse outcomes in patients hospitalized for HF and ACS, who comprise the majority of CICU patients. Hypoalbuminemia (particularly albumin levels below 3-3.2 g/dL) is strongly associated with higher hospital and 1-year mortality in patients with acute decompensated HF (ADHF). 14,32,33 Hypoalbuminemia and anemia are independent risk factors in patients admitted for ADHF. 33 Hemoglobin was not a significant predictor of mortality in our study, despite the strong association between albumin and mortality and the observed correlation between albumin and hemoglobin. 27
Hypoalbuminemia has been consistently associated with increased mortality and morbidity in ACS populations. 12 –16,34 A study of 7,192 patients with ACS found that a serum albumin level ≤ 3.5 g/dL was an independent risk factor for the development of new-onset HF and in-hospital mortality. 15 In 8,750 patients with acute myocardial infarction, admission albumin levels were found to be an independent predictor of long-term all-cause mortality. 4 We found that lower albumin levels were strongly associated with higher mortality in CICU patients with ACS, an effect partially explained by the lower use of coronary angiography, PCI, and CABG in ACS patients with hypoalbuminemia.
Potential causes of hypoalbuminemia in the critically ill populations include a systemic inflammatory response leading to capillary leak as well as albumin catabolism to facilitate increased inflammatory protein anabolism; liver dysfunction or malnutrition leading to decreased albumin synthesis; and hemodilution from volume overload. 5 –7,35 –37 The current investigation confirms that hypoalbuminemia is associated with mortality even after adjusting for the higher illness severity and greater comorbidities in patients with hypoalbuminemia. Furthermore, we observed that a lower albumin level correlated with higher overall illness severity and other proposed markers of frailty (i.e., hemoglobin and Braden skin score). This implies that the albumin level may be used as a biomarker that integrates the overall level of acute and chronic illness in CICU patients, explaining its strong and independent association with mortality. The weaker association between albumin levels and mortality among obese patients might suggest different underlying pathophysiology of hypoalbuminemia in obese patients, who may have secondary sarcopenia and expanded extracellular volume.
The present analysis does not allow us to determine whether low albumin levels are directly harmful or whether hypoalbuminemia is simply a marker of a high-risk patient. The multitude of pathophysiologic processes that affect albumin levels all could contribute to worse clinical outcomes. Patients who are frail often have hypoalbuminemia, and albumin has been proposed as a potential frailty biomarker. 38,39 Consistent with this hypothesis, Braden skin scores (a proposed frailty marker) were worse among hypoalbuminemic patients and albumin levels correlated most strongly with the Braden skin score. 26 Our study adds to the growing body of evidence that hypoalbuminemia can serve as an adverse prognostic marker in CICU patients, even after accounting for known mortality risk factors. It remains uncertain whether interventions designed to increase albumin levels (such as nutritional supplementation) have the potential to improve outcomes in CICU patients with hypoalbuminemia. Notably, intravenous hyperoncotic albumin supplementation to target an albumin level ≥ 3 g/dL in hypoalbuminemic patients with sepsis or septic shock failed to produce an improvement in clinical outcomes. 40
Limitations
This study has a number of relevant limitations that apply similarly to other retrospective cohort analyses, particularly the potential for additional unmeasured confounding variables to have influenced the results. Patients with a measured albumin level were a selected group that differed from other patients, having greater illness severity and higher mortality (data not shown). Furthermore, the CICU population at Mayo Clinic may differ from other populations in terms of baseline demographics and case mix. 41 We focused on admission laboratory values to predict mortality and were not able to determine whether changes in these variables during hospitalization influenced mortality risk, and we could not confirm the timing of the albumin level measurement relative to CICU admission. Our post-discharge mortality analysis should be considered exploratory, as the use of electronic health records to determine patient death may underestimate post-discharge mortality by potentially failing to capture patients dying in other health systems. We did not have data available to determine the cause of death, preventing us from providing specific insights about the mechanisms that could have linked hypoalbuminemia with mortality risk.
Conclusions
Hypoalbuminemia is common in CICU patients and correlates with frailty, anemia, and overall illness severity. Patients with hypoalbuminemia had higher short and long-term mortality after adjusting for illness severity and comorbidities. Further study will be required to define the mechanisms by which hypoalbuminemia is associated with mortality, and whether therapeutic interventions targeting patients with hypoalbuminemia can improve outcomes.
Supplemental Material
Supplemental Material, Hypoalbuminemia_CICU_Supplemental_Figure_1 - Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients
Supplemental Material, Hypoalbuminemia_CICU_Supplemental_Figure_1 for Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients by Mitchell Padkins, Thomas Breen, Nandan Anavekar, Gregory Barsness, Kianoush Kashani and Jacob C. Jentzer in Journal of Intensive Care Medicine
Supplemental Material
Supplemental Material, Hypoalbuminemia_CICU_Supplemental_Figure_2 - Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients
Supplemental Material, Hypoalbuminemia_CICU_Supplemental_Figure_2 for Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients by Mitchell Padkins, Thomas Breen, Nandan Anavekar, Gregory Barsness, Kianoush Kashani and Jacob C. Jentzer in Journal of Intensive Care Medicine
Supplemental Material
Supplemental Material, Hypoalbuminemia_CICU_Supplemental_Figure_3 - Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients
Supplemental Material, Hypoalbuminemia_CICU_Supplemental_Figure_3 for Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients by Mitchell Padkins, Thomas Breen, Nandan Anavekar, Gregory Barsness, Kianoush Kashani and Jacob C. Jentzer in Journal of Intensive Care Medicine
Supplemental Material
Supplemental_Table_1. - Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients
Supplemental_Table_1. for Association Between Albumin Level and Mortality Among Cardiac Intensive Care Unit Patients by Mitchell Padkins, Thomas Breen, Nandan Anavekar, Gregory Barsness, Kianoush Kashani and Jacob C. Jentzer in Journal of Intensive Care Medicine
Footnotes
Acknowledgments
The authors would like to acknowledge the dedicated physicians, nurses, and allied health staff comprising the multidisciplinary team that cares for our CICU patients each day.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.